
Dental Caries Status in Postmenopausal Women: Systematic Review and Meta-Analysis

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Review Question
2.2. Eligibility Criteria
2.3. Search Strategy and Information Sources
2.4. Data Extraction
2.5. Data Synthesis and Analysis
2.6. Risk of Bias Assessment
- (A)
- Sample Selection Domain (maximum: 6 points):
- (1)
- Sample representativeness: random sampling (3 points), non-random sampling (2 points), selected groups (1 point), or no description (0 points).
- (2)
- Sample size: justified by calculations or entire population recruitment with ≤20% loss (1 point); otherwise, (0 points).
- (3)
- Menopausal status confirmation: cessation of menstruation (2 point); only by age (1 point); no criteria description (0 points).
- (B)
- Outcome Domain (maximum: 3 points):
- (1)
- Outcome assessment: DMFT index registered with inter- and intra-examiner reliability reported (2 points), partial reliability (1 point), or none (0 points).
- (2)
- Number of observers: Two or more examiners (1 point); otherwise (0 points).
2.7. Grading of Recommendations Assessment, Development, and Evaluation
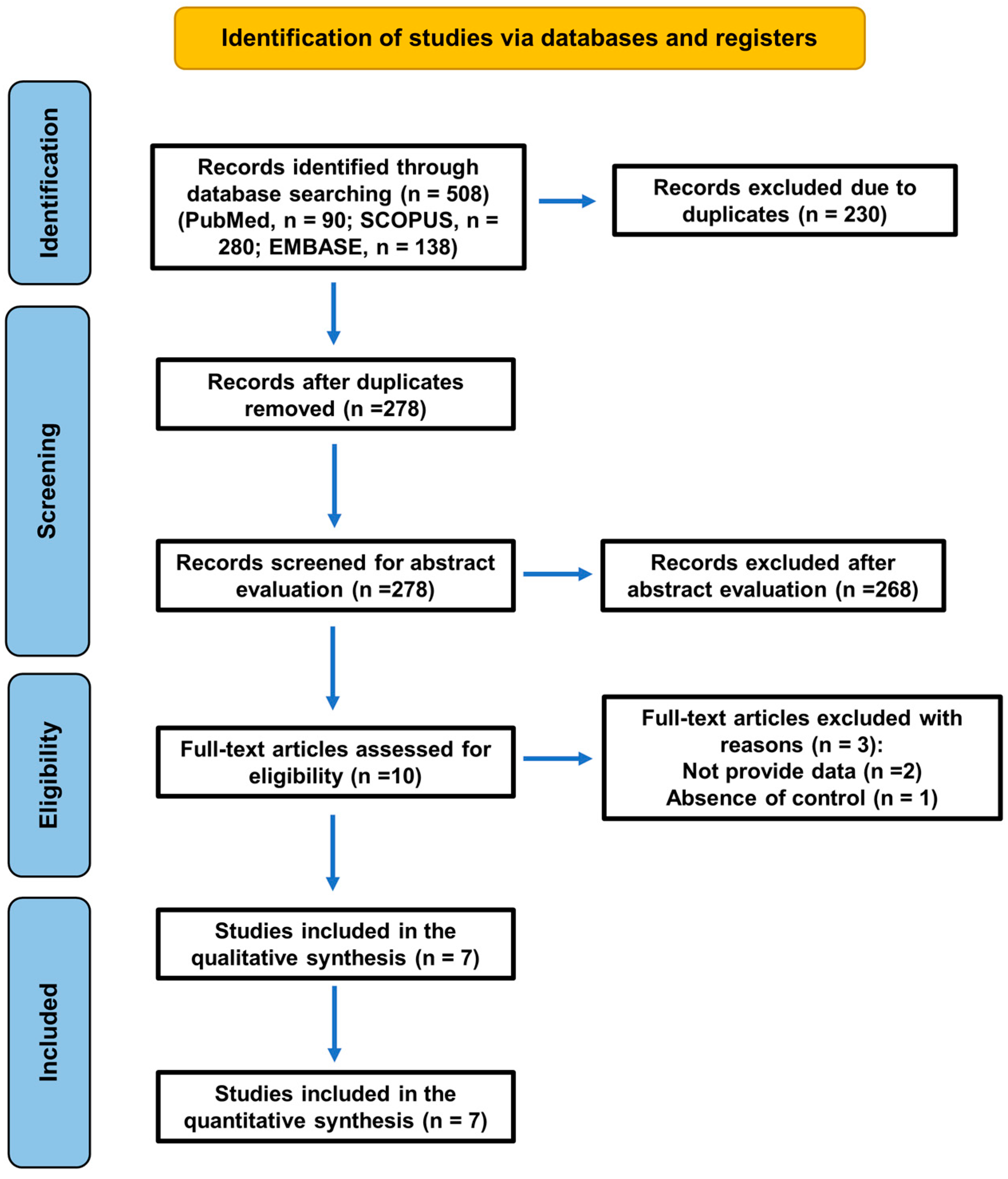
3. Results
3.1. Characteristics of the Included Studies
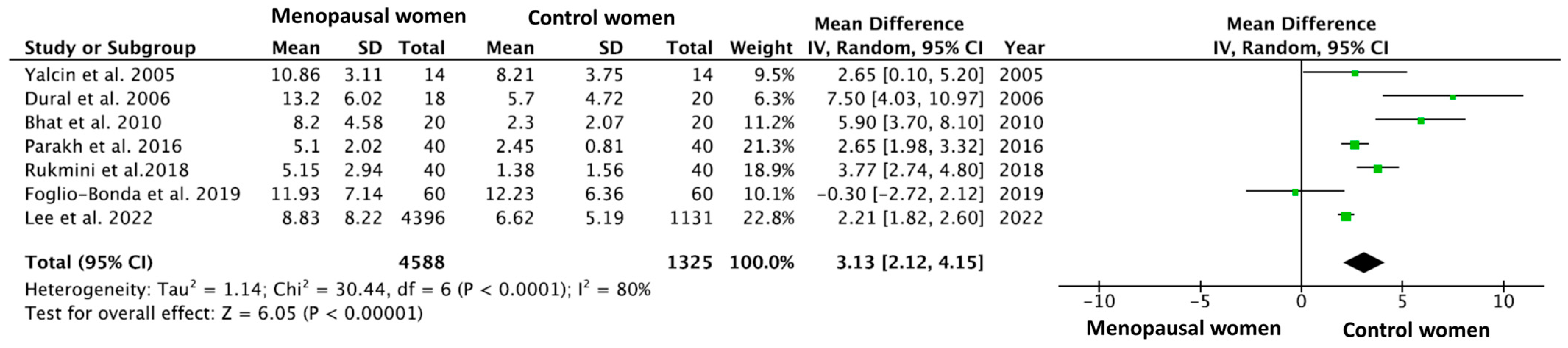
3.2. Meta-Analysis of the Prevalence of Caries Assessed Using the DMFT Index
3.3. Risk of Bias Assessment
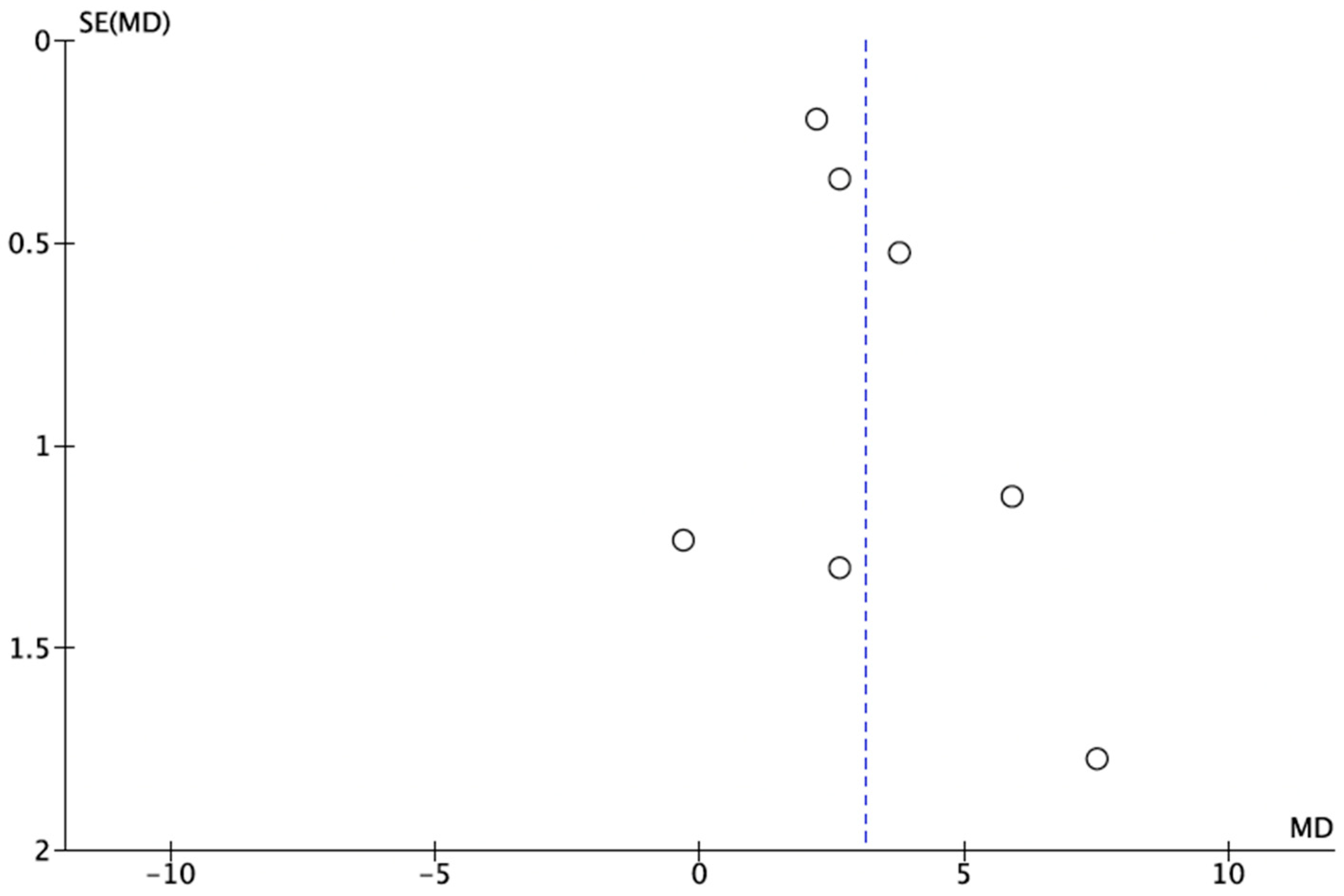
3.4. Publication Bias
3.5. GRADE Evaluation: Level of Certainty
4. Discussion
4.1. Risk of Bias of Included Studies
4.2. The Heterogeneity of the Included Studies
4.3. Menopause as a Risk Factor for Caries and Other Oral Diseases
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DMFT | Decayed, Missing, and Filled Teeth |
| MD | Mean Difference |
| MESH | Medical Subject Headings |
| CI | Confidence Interval |
| GRADE | Grading of Recommendations Assessment, Development, and Evaluation |
| HRT | Hormone Replacement Therapy |
References
- Davis, S.R.; Lambrinoudaki, I.; Lumsden, M.; Mishra, G.D.; Pal, L.; Rees, M.; Santoro, N.; Simoncini, T. Menopause. Nat. Rev. Dis. Primers 2015, 1, 1–19. [Google Scholar] [CrossRef] [PubMed]
- López-López, J.; Castellanos-Cosano, L.; Estrugo-Devesa, A.; Gõmez-Vaquero, C.; Velasco-Ortega, E.; Segura-Egea, J.J. Radiolucent Periapical Lesions and Bone Mineral Density in Post-Menopausal Women. Gerodontology 2015, 32, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Viganò, P. Endometriosis. Nat. Rev. Dis. Primers 2018, 4, 9. [Google Scholar] [CrossRef]
- Friedlander, A.H. The Physiology, Medical Management and Oral Implications of Menopause. J. Am. Dent. Assoc. 2002, 133, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Martín-González, J.; Castellanos-Cosano, L. Endodontic Medicine: Connections between Apical Periodontitis and Systemic Diseases. Int. Endod. J. 2015, 48, 933–951. [Google Scholar] [CrossRef]
- Rockenbach, M.I.; Marinho, S.A.; Veeck, E.B.; Lindemann, L.; Shinkai, R.S. Salivary Flow Rate, PH, and Concentrations of Calcium, Phosphate, and SIgA in Brazilian Pregnant and Non-Pregnant Women. Head Face Med. 2006, 2, 44. [Google Scholar] [CrossRef]
- Mishra, R.; Haider, K.; Rizwan, R.; Monga, S.; Pritam, A.; Singh, P. Assessment of Effect of Menopause on Saliva and Oral Health Status. J. Pharm. Bioallied Sci. 2021, 13 (Suppl. S2), S1535–S1537. [Google Scholar] [CrossRef]
- Featherstone, J.D.B. The science and practice of caries prevention. J. Am. Dent. Assoc. 2000, 131, 887–899. [Google Scholar] [CrossRef]
- MacHiulskiene, V.; Campus, G.; Carvalho, J.C.; Dige, I.; Ekstrand, K.R.; Jablonski-Momeni, A.; Maltz, M.; Manton, D.J.; Martignon, S.; Martinez-Mier, E.A.; et al. Terminology of Dental Caries and Dental Caries Management: Consensus Report of a Workshop Organized by ORCA and Cariology Research Group of IADR. Caries Res. 2020, 54, 7–14. [Google Scholar] [CrossRef]
- WHO. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; Licence: CC BY-NC-SA 3.0 IGO; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Foglio-Bonda, P.L.; Rocchetti, V.; Nardella, A.; Fantinato, M.; Sandhu, K.; Foglio-Bonda, A. Salivary PH and Flow Rate in Menopausal Women. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 918–922. [Google Scholar] [CrossRef]
- Lee, Y.H.; Myong, J.P. Relationship between Bone Mineral Density and Dental Caries in Koreans by Sex and Menopausal State. Int. J. Environ. Res. Public Health 2022, 19, 6917. [Google Scholar] [CrossRef] [PubMed]
- Areal-Quecuty, V.; Cantiga-Silva, C.; Simón-Soro, A.; Cabanillas-Balsera, D.; Martín-González, J.; Saúco-Márquez, J.J.; Segura-Egea, J.J. Apical Periodontitis in Osteoporotic Postmenopausal Women: Systematic Review and Meta-Analysis. Med. Oral Patol. Oral Y Cir. Bucal 2024, 29, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ (Clin. Res. Ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- León-López, M.; Cabanillas-Balsera, D.; Martín-González, J.; Montero-Miralles, P.; Saúco-Márquez, J.J.; Segura-Egea, J.J. Prevalence of Root Canal Treatment Worldwide: A Systematic Review and Meta-Analysis. Int. Endod. J. 2022, 55, 1105–1127. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Rind, D.; Akl, E.A.; Treweek, S.; Mustafa, R.A.; Iorio, A.; Alper, B.S.; Meerpohl, J.J.; Murad, M.H.; Ansari, M.T.; et al. The GRADE Working Group Clarifies the Construct of Certainty of Evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE Guidelines: 1. Introduction-GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE Guidelines: 4. Rating the Quality of Evidence--Study Limitations (Risk of Bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Baum, B.J. Characteristics of Participants in the Oral Physiology Component of the Baltimore Longitudinal Study of Aging. Community Dent. Oral Epidemiol. 1981, 9, 128–134. [Google Scholar] [CrossRef]
- Yalcin, F.; Gurgan, S.; Gul, G. Oral Health in Postmenopausal Turkish Women. Oral Health Prev. Dent. 2006, 4, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Rukmini, J.; Sachan, R.; Sibi, N.; Meghana, A.; Malar, C. Effect of Menopause on Saliva and Dental Health. J. Int. Soc. Prev. Community Dent. 2018, 8, 529. [Google Scholar] [CrossRef] [PubMed]
- Parakh, D.; Garla, B.K.; Dagli, R.; Solanki, J.; Thareja, P.; Vyas, D.; Parakh, D.; Garla, B.K.; Dagli, R.; Solanki, J.; et al. Evaluation of the Effect of Menopause on Saliva and Dental Health. Int. J. Oral Health Dent. 2016, 2, 71–76. [Google Scholar] [CrossRef]
- Bhat, S.; Hegde, S.; Sujatha, D. A Study on Evaluation of the Effect of Menopause on Saliva and Dental Health. J. Adv. Oral Res. 2010, 1, 33–36. [Google Scholar] [CrossRef]
- Dural, S.; Güngör, M.; Dds, H.; Berna, L.; Dds, Ç. Evaluation of the Effect of Menopause on Saliva and Dental Health. Citeseer 2006, 3, 15–18. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.581.6000&rep=rep1&type=pdf (accessed on 23 March 2022).
- Yalcin, F.; Gurgan, S.; Gurgan, T. The Effect of Menopause, Hormone Replacement Therapy (HRT), Alendronate (ALN), and Calcium Supplements on Saliva. J. Contemp. Dent. Pract. 2005, 6, 10–17. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Lukacs, J.R.; Thompson, L.M. Dental Caries Prevalence by Sex in Prehistory: Magnitude and Meaning. In Cambridge Studies in Biological and Evolutionary Anthropology; Irish, J.D., Nelson, G.C., Eds.; Cambridge University Press: Cambridge, UK, 2008; pp. 136–177. [Google Scholar] [CrossRef]
- Wasterlain, S.N.; Hillson, S.; Cunha, E. Dental Caries in a Portuguese Identified Skeletal Sample from the Late 19th and Early 20th Centuries. Am. J. Phys. Anthropol. 2009, 140, 64–79. [Google Scholar] [CrossRef]
- Lukacs, J.R. Fertility and Agriculture Accentuate Sex Differences in Dental Caries Rates. Univ. Chic. J. 2015, 49, 901–914. [Google Scholar] [CrossRef]
- Walter, B.S.; DeWitte, S.N.; Redfern, R.C. Sex Differentials in Caries Frequencies in Medieval London. Arch. Oral Biol. 2016, 63, 32–39. [Google Scholar] [CrossRef]
- Lagerlöf, F.; Oliveby, A. Caries-Protective Factors in Saliva. Adv. Dent. Res. 1994, 8, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Meema, S.; Meema, H.E. Menopausal Bone Loss and Estrogen Replacement. Isr. J. Med. Sci. 1976, 12, 601–606. [Google Scholar] [PubMed]
- Al-Safi, Z.A.; Santoro, N. Menopausal Hormone Therapy and Menopausal Symptoms. Fertil. Steril. 2014, 10, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Ben-Hur, H.; Mor, G.; Blickstein, I.; Likhman, I.; Kohen, F.; Dgani, R.; Insler, V.; Yaffe, P.; Ornoy, A. Localization of Estrogen Receptors in Long Bones and Vertebrae of Human Fetuses. Calcif. Tissue Int. 1993, 53, 91–96. [Google Scholar] [CrossRef]
- Arid, J.; Oliveira, D.B.; Evangelista, S.S.; Vasconcelos, K.R.F.; Dutra, A.L.T.; de Oliveira, S.S.; de Queiroz, A.M.; Nelson-Filho, P.; Vieira, A.R.; Küchler, E.C. Oestrogen Receptor Alpha, Growth Hormone Receptor, and Developmental Defect of Enamel. Int. J. Pediatr. Dent. 2019, 29, 29–35. [Google Scholar] [CrossRef]
- La Rosa, G.R.M.; Loreto, C.; Pedullà, E.; Lombardo, C. Association between Estrogen Receptors Polymorphisms and Temporomandibular Joint Disorders: A Systematic Review. Arch. Oral Biol. 2025, 170, 106130. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Reasons | Excluded Studies |
|---|---|
| Quantitative data not reported | Baum et al., 1981 [22] Mishra et al., 2021 [7] |
| Absence of control group | Yalcin et al., 2006 [23] |
| Author | Reference | Study Design | Subjects | Menopause–Caries Association |
|---|---|---|---|---|
| Lee et al., 2022 | [12] | Cross-sectional | Control—5131 Menopause—4396 | Yes p < 0.05 |
| Foglio-Bonda et al., 2019 | [11] | Cross-sectional | Control—60 Menopause—60 | No p > 0.05 |
| Rukmini et al., 2018 | [24] | Cross-sectional | Control—40 Menopause—60 | Yes p < 0.05 |
| Parakh et al., 2018 | [25] | Cross-sectional | Control—40 Menopause—40 | Yes p < 0.05 |
| Bhat et al., 2010 | [26] | Cross-sectional | Control—20 Menopause—20 | Yes p < 0.05 |
| Dural et al., 2006 | [27] | Cross-sectional | Control—20 Menopause—18 | Yes p < 0.05 |
| Yalcin et al., 2005 | [28] | Cross-sectional | Control—14 Menopause—14 | Yes p < 0.05 |
| Authors | Sample Size | Control Women | Postmenopausal Women | MD (95% C.I.) | p | ||
|---|---|---|---|---|---|---|---|
| DMFT Index | Subjects | DMFT Index | Subjects | ||||
| Lee et al., 2022 [12] | 9527 | 6.62 ± 5.19 | 5131 | 8.83 ± 8.22 | 4396 | 2.21 (1.82–2.6) | <0.05 |
| Foglio-Bonda et al., 2019 [11] | 120 | 12.23 ± 6.36 | 60 | 11.93 ± 7.14 | 60 | −0.3 (−2.72–2.12) | >0.05 |
| Rukmini et al., 2018 [24] | 80 | 1.38 ± 1.56 | 40 | 5.15 ± 2.94 | 40 | 3.77 (2.74–4.8) | <0.05 |
| Parakh et al., 2016 [25] | 80 | 2.45 ± 0.81 | 40 | 5.10 ± 2.02 | 40 | 2.65 (1.98–3.32) | <0.05 |
| Bhat et al., 2010 [26] | 40 | 2.30 ± 2.07 | 20 | 8.20 ± 4.58 | 20 | 5.9 (3.7–8.1) | <0.05 |
| Dural et al., 2006 [27] | 38 | 5.7 ± 4.72 | 20 | 13.2 ± 6.02 | 18 | 7.5 (4.03–10.97) | <0.05 |
| Yalcin et al., 2005 [28] | 28 | 8.21 ± 3.75 | 14 | 10.86 ± 3.11 | 14 | 2.65 (0.1–5.2) | <0.05 |
| Studies | Sample Selection | Outcome | Risk of Bias | |||
|---|---|---|---|---|---|---|
| Representativeness | Sample Size | Menopausal Status | Outcome Assessment | No. of Observers | ||
| Lee et al., 2022 [12] | *** | 0 | ** | * | 0 | Moderate (6) |
| Foglio-Bonda et al., 2019 [11] | * | 0 | 0 | * | 0 | High (2) |
| Rukmini et al., 2018 [24] | * | * | ** | * | 0 | Moderate (5) |
| Parakh et al., 2016 [25] | * | 0 | ** | * | 0 | Moderate (4) |
| Bhat et al., 2010 [26] | * | 0 | ** | * | 0 | Moderate (4) |
| Dural et al., 2006 [27] | * | 0 | ** | * | 0 | Moderate (4) |
| Yalcin et al., 2005 [28] | * | 0 | ** | * | 0 | Moderate (4) |
| Overall | 9 | 1 | 12 | 7 | 0 | Moderate (29) |
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Certainty |
|---|---|---|---|---|---|---|---|
| Postmenopausal women—dental caries status | |||||||
| 7 | Observational studies | Not serious a | Serious b | Serious | Serious c | MD = 3.13 (2.12–4.15) p < 0.00001 | ⊕○○○ Very low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Areal-Quecuty, V.; Segura-Egea, J.J.; Simón-Soro, A.; León-López, M.; Cantiga-Silva, C.; Martín-González, J.; Sánchez-Domínguez, B.; Cabanillas-Balsera, D. Dental Caries Status in Postmenopausal Women: Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 1837. https://doi.org/10.3390/jcm14061837
Areal-Quecuty V, Segura-Egea JJ, Simón-Soro A, León-López M, Cantiga-Silva C, Martín-González J, Sánchez-Domínguez B, Cabanillas-Balsera D. Dental Caries Status in Postmenopausal Women: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2025; 14(6):1837. https://doi.org/10.3390/jcm14061837
Chicago/Turabian StyleAreal-Quecuty, Victoria, Juan J. Segura-Egea, Aurea Simón-Soro, María León-López, Cristiane Cantiga-Silva, Jenifer Martín-González, Benito Sánchez-Domínguez, and Daniel Cabanillas-Balsera. 2025. "Dental Caries Status in Postmenopausal Women: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 14, no. 6: 1837. https://doi.org/10.3390/jcm14061837
APA StyleAreal-Quecuty, V., Segura-Egea, J. J., Simón-Soro, A., León-López, M., Cantiga-Silva, C., Martín-González, J., Sánchez-Domínguez, B., & Cabanillas-Balsera, D. (2025). Dental Caries Status in Postmenopausal Women: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 14(6), 1837. https://doi.org/10.3390/jcm14061837