
Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment


 ,
,  ,
,  and
and
Abstract
1. Introduction
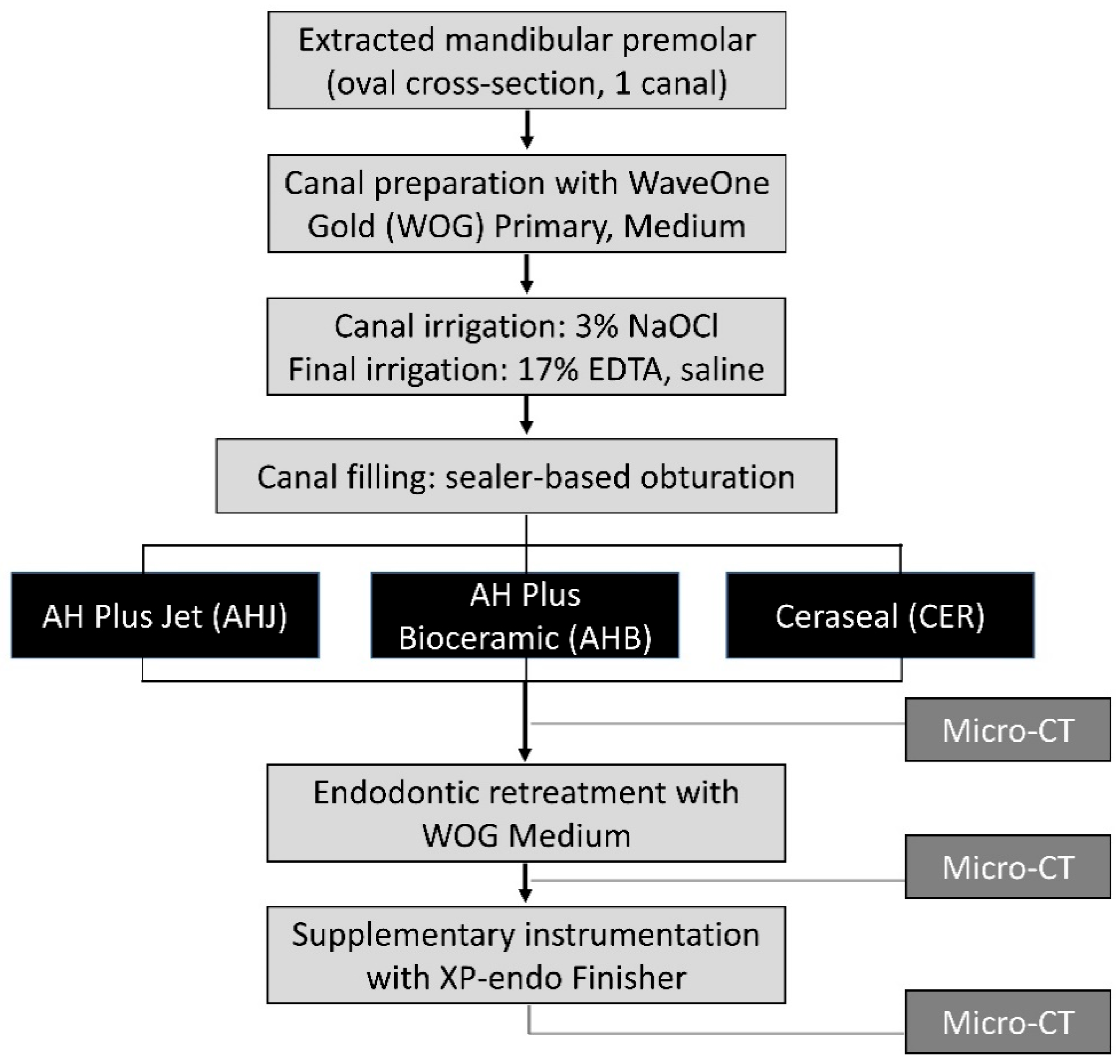
2. Materials and Methods
2.1. Specimen Preparation and Root Canal Treatment
2.2. Endodontic Retreatment
2.3. Micro-CT Scanning
2.4. Scanning Electron Microscopy Examination
2.5. Statistical Analysis
3. Results
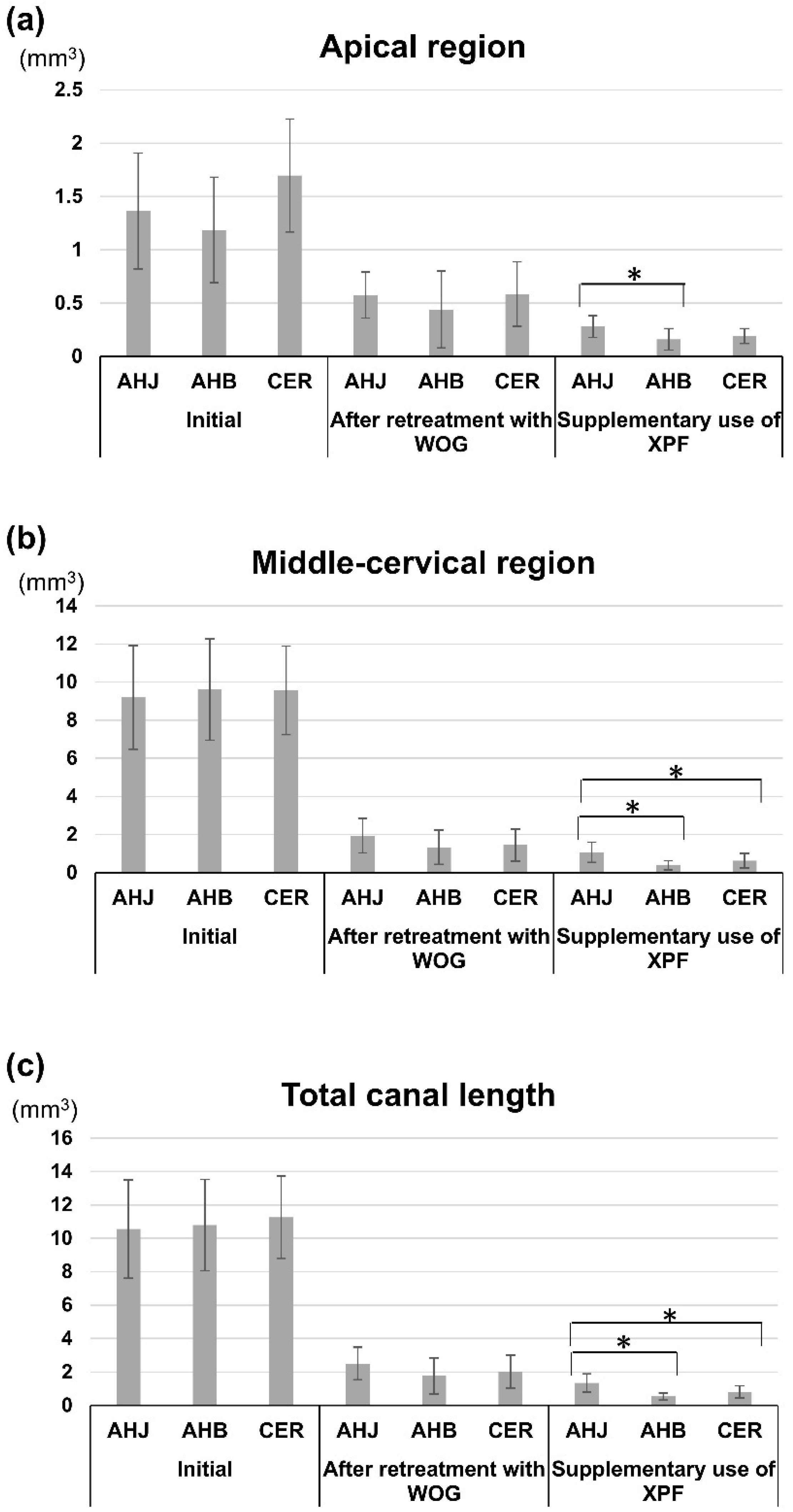
3.1. Root Canal Filling Volumes
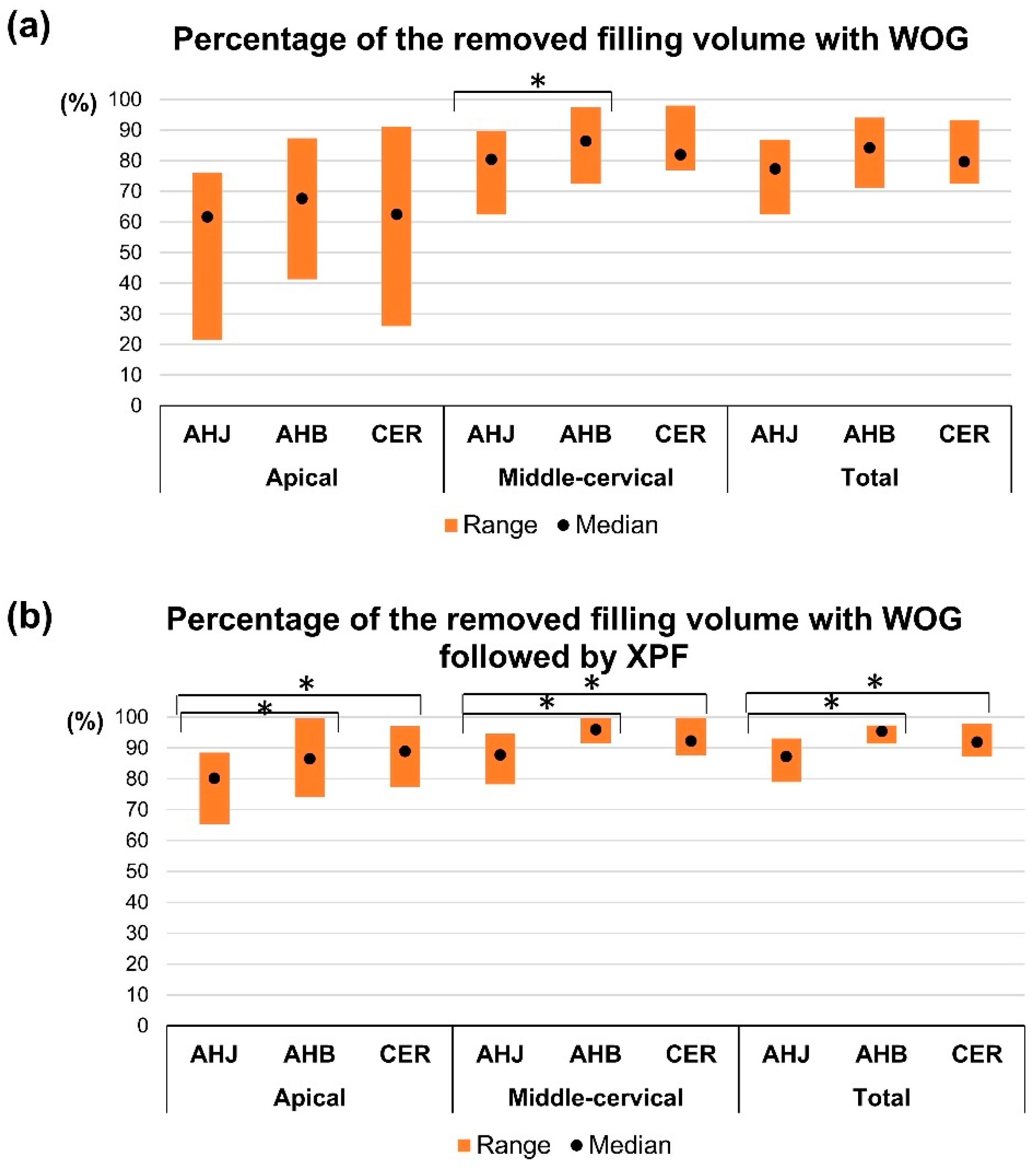
3.2. Assessment of the Ratio of the Removed Filling Volume After Endodontic Retreatment
3.3. Three-Way ANOVA Result
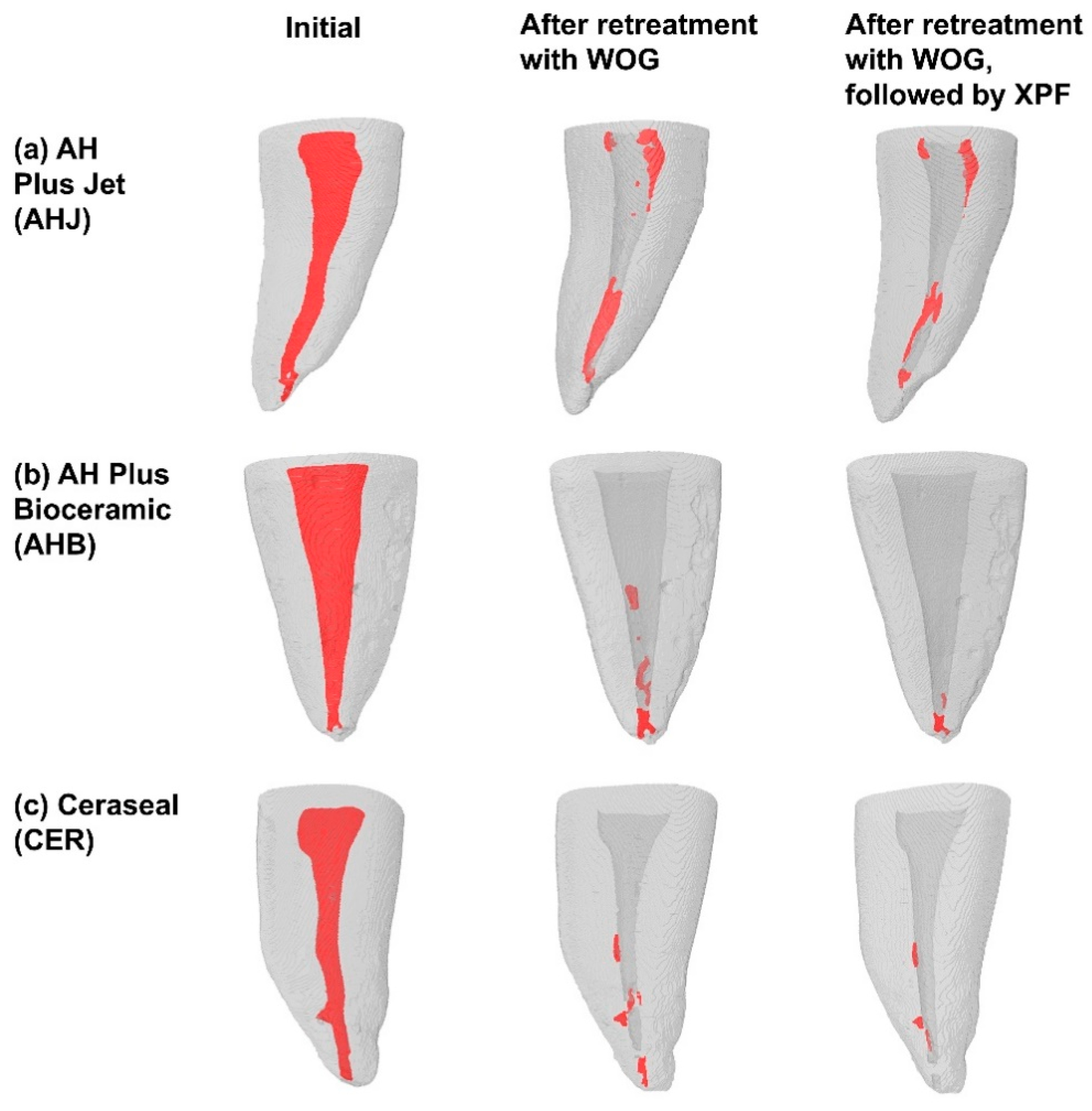
3.4. Three-Dimensional Visualization of the Roots
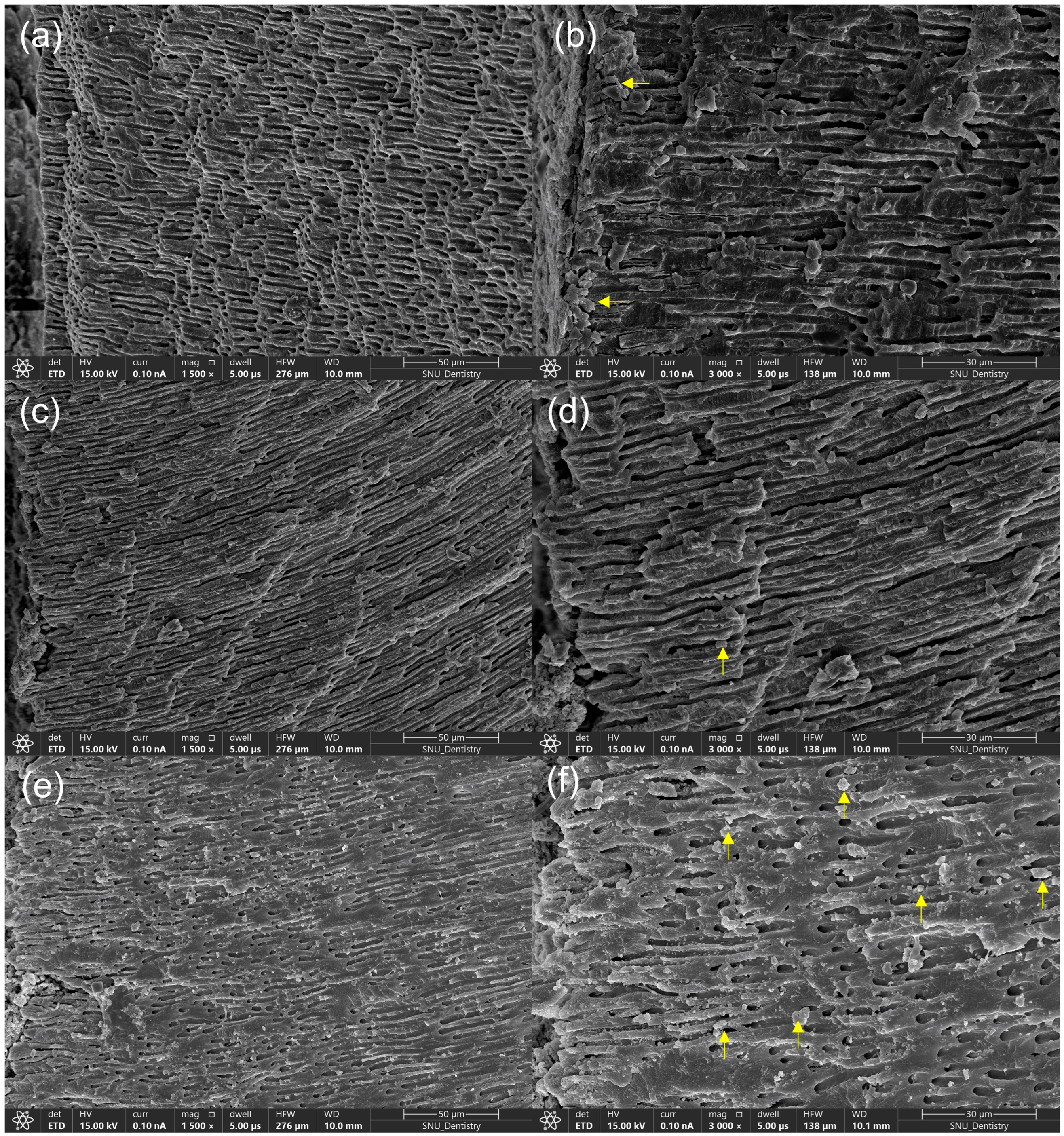
3.5. FE-SEM Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.W. Chemical characteristics of mineral trioxide aggregate and its hydration reaction. Restor. Dent. Endod. 2012, 37, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Taddei, P.; Tinti, A.; Prati, C. Apatite-forming ability (bioactivity) of ProRoot MTA. Int. Endod. J. 2010, 43, 917–929. [Google Scholar] [CrossRef] [PubMed]
- López-García, S.; Myong-Hyun, B.; Lozano, A.; García-Bernal, D.; Forner, L.; Llena, C.; Guerrero-Gironés, J.; Murcia, L.; Rodríguez-Lozano, F.J. Cytocompatibility, bioactivity potential, and ion release of three premixed calcium silicate-based sealers. Clin. Oral. Investig. 2020, 24, 1749–1759. [Google Scholar] [CrossRef]
- Sanz, J.L.; López-García, S.; Rodríguez-Lozano, F.J.; Melo, M.; Lozano, A.; Llena, C.; Forner, L. Cytocompatibility and bioactive potential of AH Plus Bioceramic Sealer: An in vitro study. Int. Endod. J. 2022, 55, 1066–1080. [Google Scholar] [CrossRef]
- Pelozo, L.L.; Souza-Gabriel, A.E.; Alves Dos Santos, G.N.; Camargo, R.V.; Lopes-Olhê, F.C.; Sousa-Neto, M.D.; Mazzi-Chaves, J.F. Canal drying protocols to use with calcium silicate-based sealer: Effect on bond strength and adhesive interface. J. Endod. 2023, 49, 1154–1160. [Google Scholar] [CrossRef]
- Kim, J.H.; Cho, S.Y.; Choi, Y.; Kim, D.H.; Shin, S.J.; Jung, I.Y. Clinical efficacy of sealer-based obturation using calcium silicate sealers: A randomized clinical trial. J. Endod. 2022, 48, 144–151. [Google Scholar] [CrossRef]
- Bardini, G.; Casula, L.; Ambu, E.; Musu, D.; Mercadè, M.; Cotti, E. A 12-month follow-up of primary and secondary root canal treatment in teeth obturated with a hydraulic sealer. Clin. Oral. Investig. 2021, 25, 2757–2764. [Google Scholar] [CrossRef]
- Subbiya, A.; Kishen, A.; Pradeepkumar, A.R.; Srinivasan, N.; JothiLatha, S.; Janani, B. Clinical outcome of nonsurgical root canal treatment using a matched single-cone obturation technique with a calcium hydroxide-based sealer: A retrospective analysis. J. Endod. 2022, 48, 1486–1492. [Google Scholar] [CrossRef]
- Maharti, I.D.; Suprastiwi, E.; Agusnar, H.; Herdianto, N.; Margono, A. Characterization, physical properties, and biocompatibility of novel tricalcium silicate-chitosan endodontic sealer. Eur. J. Dent. 2023, 17, 127–135. [Google Scholar] [CrossRef]
- Cardinali, F.; Camilleri, J. A critical review of the material properties guiding the clinician’s choice of root canal sealers. Clin. Oral. Investig. 2023, 27, 4147–4155. [Google Scholar] [CrossRef] [PubMed]
- Zamparini, F.; Prati, C.; Taddei, P.; Spinelli, A.; Di Foggia, M.; Gandolfi, M.G. Chemical-physical properties and bioactivity of new premixed calcium silicate-bioceramic root canal sealers. Int. J. Mol. Sci. 2022, 23, 13914. [Google Scholar] [CrossRef] [PubMed]
- Park, M.G.; Kim, I.R.; Kim, H.J.; Kwak, S.W.; Kim, H.C. Physicochemical properties and cytocompatibility of newly developed calcium silicate-based sealers. Aust. Endod. J. 2021, 47, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Pontoriero, D.I.K.; Ferrari Cagidiaco, E.; Maccagnola, V.; Manfredini, D.; Ferrari, M. Outcomes of endodontic-treated teeth obturated with bioceramic sealers in combination with warm gutta-percha obturation techniques: A prospective clinical study. J. Clin. Med. 2023, 12, 2867. [Google Scholar] [CrossRef]
- Spinelli, A.; Zamparini, F.; Lenzi, J.; Gandolfi, M.G.; Prati, C. Three-year clinical outcome of root canal treatment using a single-cone technique and Ceraseal premixed bioceramic sealer: A prospective cohort study. Eur. Endod. J. 2024, 9, 383–393. [Google Scholar] [CrossRef]
- ISO 6876:2012; Dentistry—Root Canal Sealing Materials. International Organization for Standardization: Geneva, Switzerland, 2012.
- Kwak, S.W.; Koo, J.; Song, M.; Jang, I.H.; Gambarini, G.; Kim, H.C. Physicochemical properties and biocompatibility of various bioceramic root canal sealers: In vitro study. J. Endod. 2023, 49, 871–879. [Google Scholar] [CrossRef]
- Souza, L.C.; Neves, G.S.T.; Kirkpatrick, T.; Letra, A.; Silva, R. Physicochemical and biological properties of AH Plus Bioceramic. J. Endod. 2023, 49, 69–76. [Google Scholar] [CrossRef]
- Kwak, Y.; Choi, J.; Kim, K.; Shin, S.J.; Kim, S.; Kim, E. The 5-year survival rate of nonsurgical endodontic treatment: A population-based cohort study in Korea. J. Endod. 2019, 45, 1192–1199. [Google Scholar] [CrossRef]
- Chugal, N.M.; Clive, J.M.; Spångberg, L.S. A prognostic model for assessment of the outcome of endodontic treatment: Effect of biologic and diagnostic variables. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2001, 91, 342–352. [Google Scholar] [CrossRef]
- Tabassum, S.; Khan, F.R. Failure of endodontic treatment: The usual suspects. Eur. J. Dent. 2016, 10, 144–147. [Google Scholar] [CrossRef]
- Karaoğlan, F.; Miçooğulları Kurt, S.; Çalışkan, M.K. Outcome of single- versus two-visit root canal retreatment in teeth with periapical lesions: A randomized clinical trial. Int. Endod. J. 2022, 55, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Maharti, I.D.; Rosseti, R.; Asrianti, D.; Herdianto, N.; Rianti, W. Calcium silicate-based sealers: Apatite deposition on root canal dentin and pH variation analysis. Eur. J. Dent. 2025. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, C.; Zamparini, F.; Prati, C. Osteoinductive and regenerative potential. Int. Endod. J. 2024, 57, 1264–1278. [Google Scholar] [CrossRef] [PubMed]
- Alsubait, S.; Alhathlol, N.; Alqedairi, A.; Alfawaz, H. A micro-computed tomographic evaluation of retreatability of BioRoot RCS in comparison with AH Plus. Aust. Endod. J. 2021, 47, 222–227. [Google Scholar] [CrossRef]
- Jamleh, A.; Nassar, M.; Alfadley, A.; Alanazi, A.; Alotiabi, H.; Alghilan, M.; Alfouzan, K. Assessment of bioceramic sealer retreatability and its influence on force and torque generation. Materials 2022, 15, 3316. [Google Scholar] [CrossRef]
- Donnermeyer, D.; Bunne, C.; Schäfer, E.; Dammaschke, T. Retreatability of three calcium silicate-containing sealers and one epoxy resin-based root canal sealer with four different root canal instruments. Clin. Oral. Investig. 2018, 22, 811–817. [Google Scholar] [CrossRef]
- Oltra, E.; Cox, T.C.; LaCourse, M.R.; Johnson, J.D.; Paranjpe, A. Retreatability of two endodontic sealers, EndoSequence BC Sealer and AH Plus: A micro-computed tomographic comparison. Restor. Dent. Endod. 2017, 42, 19–26. [Google Scholar] [CrossRef]
- Romeiro, K.; de Almeida, A.; Cassimiro, M.; Gominho, L.; Dantas, E.; Chagas, N.; Velozo, C.; Freire, L.; Albuquerque, D. Reciproc and Reciproc Blue in the removal of bioceramic and resin-based sealers in retreatment procedures. Clin. Oral. Investig. 2020, 24, 405–416. [Google Scholar] [CrossRef]
- Baranwal, H.C.; Singh, N.; Kumari, A. XP Endo® File: An update review. Indian J. Dent. Sci. 2020, 12, 53–55. [Google Scholar] [CrossRef]
- Alves, F.R.; Marceliano-Alves, M.F.; Sousa, J.C.; Silveira, S.B.; Provenzano, J.C.; Siqueira, J.F., Jr. Removal of root canal fillings in curved canals using either reciprocating single- or rotary multi-instrument systems and a supplementary step with the XP-Endo Finisher. J. Endod. 2016, 42, 1114–1119. [Google Scholar] [CrossRef]
- Aksel, H.; Küçükkaya Eren, S.; Askerbeyli Örs, S.; Serper, A.; Ocak, M.; Çelik, H.H. Micro-CT evaluation of the removal of root fillings using the ProTaper Universal Retreatment system supplemented by the XP-Endo Finisher file. Int. Endod. J. 2019, 52, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Kiraz, G.; Kaya, B.; Ocak, M.; Uzuner, M.B.; Çelik, H.H. Micro-CT evaluation of the removal of root fillings using rotary and reciprocating systems supplemented by XP-Endo Finisher, the Self-Adjusting File, or Er,Cr:YSGG laser. Restor. Dent. Endod. 2023, 48, e36. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.; Belladonna, F.G.; Zuolo, A.S.; Rodrigues, E.; Ehrhardt, I.C.; Souza, E.M.; De-Deus, G. Effectiveness of XP-endo Finisher and XP-endo Finisher R in removing root filling remnants: A micro-CT study. Int. Endod. J. 2018, 51, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Ersev, H.; Yilmaz, B.; Dinçol, M.E.; Dağlaroğlu, R. The efficacy of ProTaper Universal rotary retreatment instrumentation to remove single gutta-percha cones cemented with several endodontic sealers. Int. Endod. J. 2012, 45, 756–762. [Google Scholar] [CrossRef]
- Sousa-Neto, M.D.; Silva Coelho, F.I.; Marchesan, M.A.; Alfredo, E.; Silva-Sousa, Y.T. Ex vivo study of the adhesion of an epoxy-based sealer to human dentine submitted to irradiation with Er:YAG and Nd:YAG lasers. Int. Endod. J. 2005, 38, 866–870. [Google Scholar] [CrossRef]
- Shieh, K.; Yang, J.; Zhu, E.H.; Peters, O.A.; Hosseinpour, S. Dentinal tubule penetrability and bond strength of two novel calcium silicate-based root canal sealers. Materials 2023, 16, 3309. [Google Scholar] [CrossRef]
- Kharouf, N.; Sauro, S.; Eid, A.; Zghal, J.; Jmal, H.; Seck, A.; Macaluso, V.; Addiego, F.; Inchingolo, F.; Affolter-Zbaraszczuk, C.; et al. Physicochemical and mechanical properties of premixed calcium silicate and resin sealers. J. Funct. Biomater. 2023, 14, 9. [Google Scholar] [CrossRef]
- Kharouf, N.; Cardinali, F.; Al-Rayesse, R.; Eid, A.; Moujaes, Z.; Nafash, M.; Jmal, H.; Addiego, F.; Haikel, Y. Mechanical and physicochemical characteristics of a novel premixed calcium silicate sealer. Materials 2024, 17, 3374. [Google Scholar] [CrossRef]
- Zancan, R.F.; Di Maio, A.; Tomson, P.L.; Duarte, M.A.H.; Camilleri, J. The presence of smear layer affects the antimicrobial action of root canal sealers. Int. Endod. J. 2021, 54, 1369–1382. [Google Scholar] [CrossRef]
- Andriukaitiene, L.; Song, X.; Yang, N.; Lassila, L.V.J.; Vallittu, P.K.; Kerosuo, E. The effect of smear layer removal on E. faecalis leakage and bond strength of four resin-based root canal sealers. BMC Oral. Health 2018, 18, 213. [Google Scholar] [CrossRef]
- Choudhury, S.; Shivanand, S.; Patil, A.C.; Patil, S.A.; Doddwad, P.K.; Patil, C. Evaluation of push-out bond strength of a resin sealer to dentin after a final flush of three irrigants. J. Contemp. Dent. Pract. 2020, 21, 982–985. [Google Scholar] [CrossRef] [PubMed]
- Versiani, M.A.; Leoni, G.B.; Steier, L.; De-Deus, G.; Tassani, S.; Pécora, J.D.; Sousa-Neto, M.D. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. J. Endod. 2013, 39, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.M.B.; Duque, J.A.; Zancan, R.F.; Vivan, R.R.; Bernardes, R.A.; Duarte, M.A.H. Efficacy of reciprocating systems for removing root filling material plus complementary cleaning methods in flattened canals: Microtomography and scanning electron microscopy study. Microsc. Res. Tech. 2019, 82, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Tavares, K.I.M.C.; Pinto, J.C.; Santos-Junior, A.O.; Duarte, M.A.H.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M. Effect of additional apical preparation on retreatment of curved root canals filled with different sealers. Eur. J. Dent. 2023, 17, 636–641. [Google Scholar] [CrossRef]
- Rödig, T.; Reicherts, P.; Konietschke, F.; Dullin, C.; Hahn, W.; Hülsmann, M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int. Endod. J. 2014, 47, 942–948. [Google Scholar] [CrossRef]
- Bernardes, R.A.; Duarte, M.A.H.; Vivan, R.R.; Alcalde, M.P.; Vasconcelos, B.C.; Bramante, C.M. Comparison of three retreatment techniques with ultrasonic activation in flattened canals using micro-computed tomography and scanning electron microscopy. Int. Endod. J. 2016, 49, 890–897. [Google Scholar] [CrossRef]
- Agarwal, D.; Raghavendra, S.S. Cleaning efficacy and debris extrusion of supplementary file systems XP-endo Finisher and XP-endo Finisher R in endodontic retreatment. J. Conserv. Dent. Endod. 2024, 27, 498–502. [Google Scholar] [CrossRef]
- Dreger, L.A.; Felippe, W.T.; Reyes-Carmona, J.F.; Felippe, G.S.; Bortoluzzi, E.A.; Felippe, M.C. Mineral trioxide aggregate and Portland cement promote biomineralization in vivo. J. Endod. 2012, 38, 324–329. [Google Scholar] [CrossRef]
- Yoo, Y.J.; Baek, S.H.; Kum, K.Y.; Shon, W.J.; Woo, K.M.; Lee, W. Dynamic intratubular biomineralization following root canal obturation with pozzolan-based mineral trioxide aggregate sealer cement. Scanning 2016, 38, 50–56. [Google Scholar] [CrossRef]
- Oh, S.; Cho, S.I.; Perinpanayagam, H.; You, J.; Hong, S.H.; Yoo, Y.J.; Chang, S.W.; Shon, W.J.; Yoo, J.S.; Baek, S.H.; et al. Novel calcium zirconate silicate cement biomineralize and seal root canals. Materials 2018, 11, 588. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sealer | Type | Manufacturer | Composition | |
|---|---|---|---|---|
| Paste A | Paste B | |||
| AH Plus Jet (AHJ) | Epoxy resin-based sealer | Dentsply Sirona, Charlotte, NC, USA | Epoxy resin, calcium tungstate, zirconium oxide, aerosol, iron oxide | 1-adamantane amine, N,N’-dibenzyl-5-oxanonandiamin-1,9, tricyclodecane diamine, calcium tungstate, zirconium oxide, aerosol, silicone oil |
| AH Plus Bioceramic (AHB) | CSBS | Dentsply Sirona, Ballaigues, Switzerland | Zirconium dioxide 50–75%, tricalcium silicate 5–15%, dimethyl sulfoxide 10–30%, lithium carbonate < 0.5%, thickening agent < 6% | |
| Ceraseal (CER) | CSBS | Metabiomed, Cheongju, South Korea | Zirconium dioxide 45–50%, tricalcium silicate 20–30%, dicalcium silicate 1–10%, tricalcium aluminate 1–10%, thickening agent | |
| Initial Filling Volume | Residual Filling Volume After Retreatment with WOG | Residual Filling Volume After Supplementary Use of XPF | |||||||
|---|---|---|---|---|---|---|---|---|---|
| group | AHJ | AHB | CER | AHJ | AHB | CER | AHJ | AHB | CER |
| Apical | 1.36 ± 0.54 | 1.19 ± 0.49 | 1.7 ± 0.53 | 0.57 ± 0.22 | 0.44 ± 0.36 | 0.58 ± 0.3 | 0.28 ± 0.1 b | 0.16 ± 0.1 a | 0.19 ± 0.07 a,b |
| Middle-cervical | 9.2 ± 2.73 | 9.61 ± 2.65 | 9.57 ± 2.32 | 1.95 ± 0.9 | 1.34 ± 0.9 | 1.45 ± 0.84 | 1.07 ± 0.52 b | 0.39 ± 0.24 a | 0.63 ± 0.39 a |
| Total canal | 10.56 ± 2.95 | 10.79 ± 2.73 | 11.26 ± 2.47 | 2.52 ± 0.97 | 1.78 ± 1.08 | 2.03 ± 0.99 | 1.35 ± 0.55 b | 0.55 ± 0.21 a | 0.82 ± 0.35 a |
| After Retreatment with WOG | After Retreatment with WOG Followed by XPF | |||||
|---|---|---|---|---|---|---|
| Group | AHJ | AHB | CER | AHJ | AHB | CER |
| Apical | 55.1 ± 17.6 | 65.8 ± 15.9 | 62.9 ± 18.6 | 78.3 ± 7.5 a | 86.3 ± 6.7 b | 87.9 ± 5.7 b |
| Middle-cervical | 78.9 ± 7.7 a | 86.9 ± 7.1 b | 84.6 ± 7.5 a,b | 88.1 ± 5.1 a | 95.9 ± 2.6 b | 93.2 ± 3.9 b |
| Total canal | 76 ± 7.1 | 84.4 ± 7.2 | 81.6 ± 7.7 | 87.1 ± 4.4 a | 94.8 ± 2.1 b | 92.5 ± 3.1 b |
| Source | Sum of Squares | Degree of Freedom | Mean Squares | F | p-Value |
|---|---|---|---|---|---|
| Sealer | 2018.501 | 2 | 1009.251 | 9.649 | <0.001 |
| Root region | 8370.105 | 1 | 8370.105 | 80.019 | <0.001 |
| Instrument | 9137.663 | 1 | 9137.663 | 87.357 | <0.001 |
| Sealer × root region | 64.183 | 2 | 32.092 | 0.307 | 0.736 |
| Sealer × instrument | 26.541 | 2 | 13.271 | 0.127 | 0.881 |
| Root region × instrument | 1760.533 | 1 | 1760.533 | 16.831 | <0.001 |
| Sealer × root region × instrument | 36.837 | 2 | 18.418 | 0.176 | 0.839 |
| AHJ | AHB | CER | |
|---|---|---|---|
| C | 25.13 | 25.78 | 25.24 |
| N | 11.66 | 13.25 | |
| O | 33.53 | 39.09 | 31.59 |
| F | 3.75 | 4.09 | |
| Na | 1.99 | 1.34 | 1.31 |
| Mg | 0.94 | 1 | 0.52 |
| P | 11.72 | 16.01 | 11.19 |
| Ca | 11.28 | 16.78 | 12.81 |
| total | 100 | 100 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shim, E.; Son, J.W.; Kwon, J.; Kim, H.-J.; Jang, J.-H.; Chang, S.W.; Oh, S. Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment. J. Clin. Med. 2025, 14, 1826. https://doi.org/10.3390/jcm14061826
Shim E, Son JW, Kwon J, Kim H-J, Jang J-H, Chang SW, Oh S. Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment. Journal of Clinical Medicine. 2025; 14(6):1826. https://doi.org/10.3390/jcm14061826
Chicago/Turabian StyleShim, Eurok, Jee Woo Son, Jiyoung Kwon, Hyun-Jung Kim, Ji-Hyun Jang, Seok Woo Chang, and Soram Oh. 2025. "Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment" Journal of Clinical Medicine 14, no. 6: 1826. https://doi.org/10.3390/jcm14061826
APA StyleShim, E., Son, J. W., Kwon, J., Kim, H.-J., Jang, J.-H., Chang, S. W., & Oh, S. (2025). Retrieval of AH Plus Bioceramic and Ceraseal Versus AH Plus in Endodontic Retreatment. Journal of Clinical Medicine, 14(6), 1826. https://doi.org/10.3390/jcm14061826