
Factors Associated with Complicated Parapneumonic Pleural Effusion/Empyema in Patients with Community-Acquired Pneumonia: The EMPIR Study
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
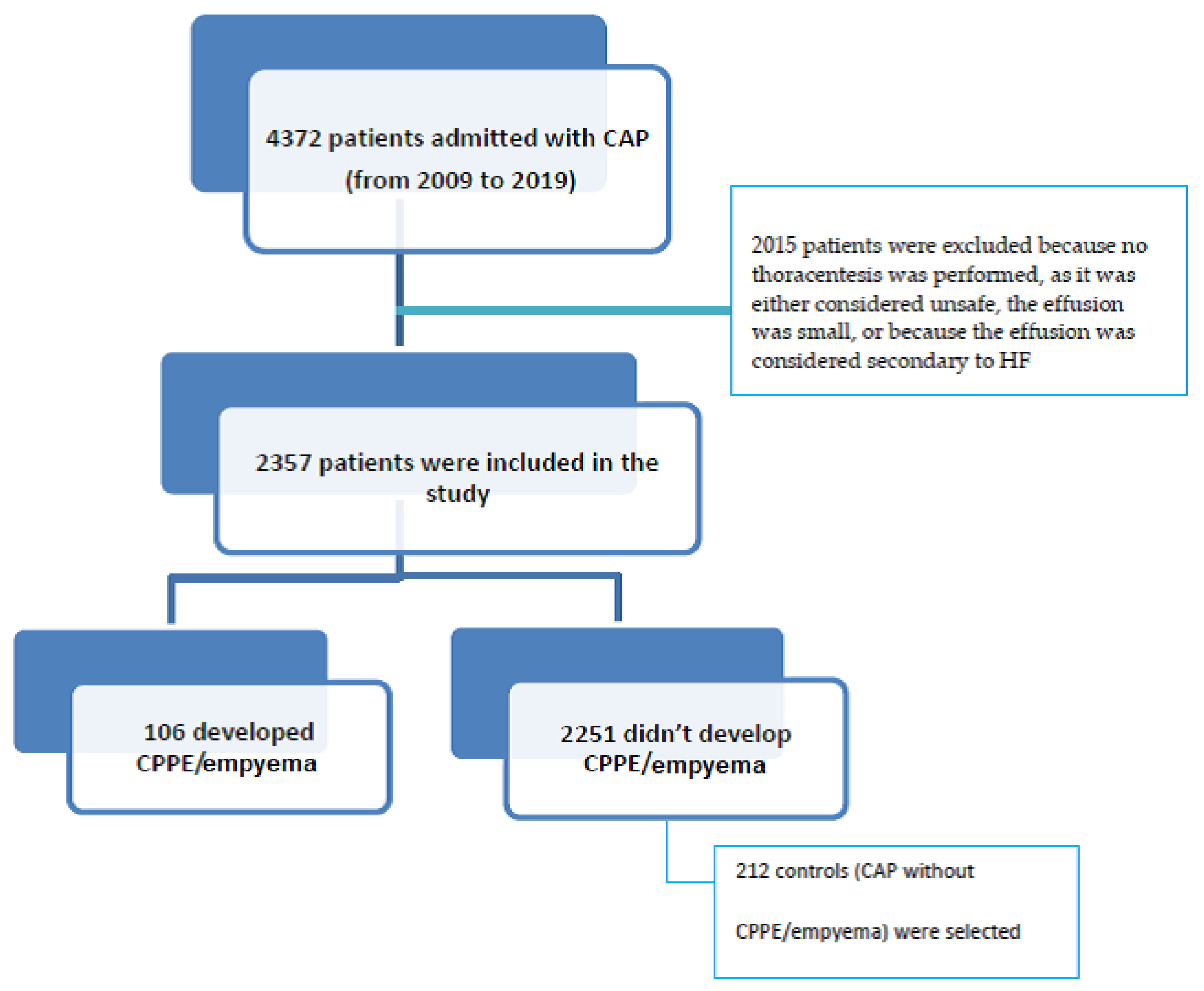
2.1. Study Design and Population
2.2. Variables
2.3. Ethics
2.4. Sample Size
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAP | community-acquired pneumonia |
| PPE | parapneumonic pleural effusion |
| CPPE | complicated parapneumonic pleural effusion |
| E | empyema |
| LDH | lactate dehydrogenase |
| CT | computed tomography |
| ICD | International Classification of Diseases |
| HF | heart failure |
| COPD | chronic obstructive pulmonary disease |
| HIV | human immunodeficiency virus |
| AIDS | acquired immune deficiency syndrome |
| RSV | respiratory syncytial virus |
| ED | emergency department |
| BP | blood pressure |
| CRP | C-reactive protein |
| PCT | procalcitonin |
| AST | aspartate aminotransferase |
| ALT | alanine aminotransferase |
| ABG | arterial blood gases |
| PaO2 | partial pressure of oxygen |
| PCO2 | partial pressure of carbon dioxide |
| HCO3 | bicarbonate |
| ATS | American Thoracic Society |
| OR | odds ratios |
| CIs | confidence intervals |
| LRT | likelihood ratio test |
| AUC | area under the curve |
| SD | standard deviation |
| PPV | positive predictive value |
| NPV | negative predictive value |
| LR+ | positive likelihood ratio |
| LR− | negative likelihood ratio |
References
- Light, R.W. Parapneumonic effusions and empyema. Proc. Am. Thorac. Soc. 2006, 3, 75–80. [Google Scholar] [CrossRef] [PubMed]
- McCauley, L.; Dean, N. Pneumonia and empyema: Causal, casual or unknown. J. Thorac. Dis. 2015, 7, 992–999. [Google Scholar] [PubMed]
- Light, R.W. A new classification of paraneumonic effusions and empyema. Chest 1995, 198, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Light, R.W. Pleural Efussion. N. Engl. J. Med. 2002, 346, 1971–1977. [Google Scholar] [CrossRef]
- Yang, W.; Zhang, B.; Zhang, Z.M. Infectious pleural effusion status and treatment progress. J. Thorac. Dis. 2017, 9, 4690–4699. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Morris, T.T.; Suri, T.; Morley, A.; Frost, V.; Vipond, I.B.; Medford, A.R.; Payne, R.A.; Muir, P.; et al. Epidemiology of pleural empyema in English hospitals and the impact of influenza. Eur. Respir. J. 2021, 57, 2003546. [Google Scholar] [CrossRef]
- Burgos, J.; Lujan, M.; Falcó, V.; Sánchez, A.; Puig, M.; Borrego, A.; Fontanals, D.; Planes, A.M.; Pahissa, A.; Rello, J. The spectrum of pneumococcal empyema in adults in the early 21st century. Clin. Infect. Dis. 2011, 53, 254–261. [Google Scholar] [CrossRef]
- Colice, G.L.; Curtis, A.; Deslauries, J.; Heffner, J.; Light, R.; Littenberg, B.; Sahn, S.; Weinstein, R.A.; Yusen, R.D. Medical and Surgical treatment of Paraneumonic effusions: An evidence-based guideline. Chest 2000, 118, 1158–1171. [Google Scholar] [CrossRef]
- Shen, K.R.; Bribriesco, A.; Crabtree, T.; Denlinger, C.; Eby, J.; Eiken, P.; Jones, D.R.; Keshavjee, S.; Maldonado, F.; Paul, S.; et al. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. J. Thorac Cardiovasc. Surg. 2017, 153, e129–e146. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef]
- Lim, W.S.; van der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, G.I.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A predictive rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Nathan, C.; Dean, N.C. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr. Regression Modeling Strategies; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar] [CrossRef]
- Falguera, M.; Carratalá, J.; Bielsa, S.; García-Vidal, C.; Ruiz-González, A.; Chica, I.; Gudiol, F.; Porcel, J. Predictive factors, microbiology and outcome of patients with parapneumonic effusion. Eur. Respir. J. 2011, 38, 1173–1179. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Singanayagam, A.; Murray, M.P.; Scally, C.; Fawzi, A.; Hill, A.T. Risk factors for complicated parapneumonic effusion and empyema on presentation to hospital with community-acquired pneumonia. Thorax 2009, 64, 592–597. [Google Scholar] [CrossRef]
- Ahmed, R.A.; Marrie, T.J.; Huang, J.Q. Thoracic empyema in patients with community-acquired pneumonia. Am. J. Med. 2006, 119, 877–883. [Google Scholar] [CrossRef]
- Alfageme, I.; Muñoz, F.; Peña, N.; Umbría, S. Empyema of the thorax in adults. Etiology, microbiologic findings, and management. Chest 1993, 103, 839–843. [Google Scholar] [CrossRef]
- Falguera, M.; Pifarre, R.; Martin, A.; Sheikh, A.; Moreno, A. Etiology and outcome of community-acquired pneumonia in patients with diabetes mellitus. Chest 2005, 128, 3233–3239. [Google Scholar] [CrossRef]
- Lu, H.Y.; Liao, K.M. Risk of empyema in patients with COPD. Int. J. Chron. Obstruct Pulmon Dis. 2018, 13, 317–324. [Google Scholar] [CrossRef]
- Cillóniz, C.; Ewig, S.; Polverino, E.; Muñoz-Almagro, C.; Marco, F.; Gabarrús, A.; Menéndez, R.; Mensa, J.; Torres, A. Pulmonary complications of pneumococcal community-acquired pneumonia: Incidence, predictors, and outcomes. Clin. Microbiol. Infect. 2012, 18, 1134–1142. [Google Scholar] [CrossRef]
- Zhong, M.; Ni, R.; Zhang, H.; Sun, Y. Analysis of clinical characteristics and risk factors of community-acquired pneumonia complicated by parapneumonic pleural effusion in elderly patients. BMC Pulm. Med. 2023, 23, 355. [Google Scholar] [CrossRef] [PubMed]
- Sellares, J.; López-Giraldo, A.; Lucena, C.; Cilloniz, C.; Amaro, R.; Polverino, E.; Ferrer, M.; Menéndez, R.; Mensa, J.; Torres, A. Influence of previous use of inhaled corticoids on the development of pleural effusion in community-acquired pneumonia. Am. J. Respir. Crit. Care Med. 2013, 187, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Torres, A.; Nagavci, B.; Aliberti, S.; Antonelli, M.; Bassetti, M.; Bos, L.D.; Chalmers, J.D.; Derde, L.; de Waele, J.; et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive Care Med. 2023, 49, 615–632. [Google Scholar] [CrossRef]
- Dequin, P.F.; Meziani, F.; Quenot, J.P.; Kamel, T.; Ricard, J.D.; Badie, J.; Reignier, J.; Heming, N.; Plantefève, G.; Souweine, B.; et al. Hydrocortisone in Severe Community-Acquired Pneumonia. N. Engl. J. Med. 2023, 388, 1931–1941. [Google Scholar] [CrossRef]
- Fitzgerald, D.B.; Waterer, G.W.; Budgeon, C.; Shrestha, R.; Fysh, E.T.; Muruganandan, S.; Stanley, C.; Saghaie, T.; Badiei, A.; Sidhu, C.; et al. Steroid Therapy and Outcome of Parapneumonic Pleural Effusions (STOPPE) A Pilot Randomized Clinical Trial. Am. J. Respir. Crit. Care Med. 2022, 205, 1093–1101. [Google Scholar] [CrossRef]
- Skouras, V.; Chatzivasiloglou, F.; Iliopoulou, M.; Rimpa, T. Medical treatment of pleural infection: Antibiotic duration and corticosteroid usefulness. Breathe 2023, 19, 230134. [Google Scholar] [CrossRef]

{kind=link}
| Stage 1: Simple or uncomplicated parapneumonic effusion | The fluid is free flowing and has exudative features with a protein content greater than 0.5 of the serum value and/or a lactate dehydrogenase (LDH) level greater than 0.6 that in serum (but usually <1000 international units [IU]/L). The leukocyte count is variable but neutrophils usually predominate. The fluid will have a normal pH and glucose level and there will be no evidence of infection by microorganisms. |
| Stage 2: Complicated parapneumonic Effusion and empyema | It is a fibrinopurulent stage, where bacterial invasion stimulates an inflammatory response resulting in fibrin deposition and loculations within the pleural space. The fluid characteristics are exudative with an elevated leukocyte count, pH < 7.20, glucose < 2.2 mmol/L (<40 mg/dL), and LDH > 1000 IU/L. If there is no pus, it is referred to as complicated parapneumonic effusion, but if there is frank pus, it is referred to as empyema. |
| Stage 3: Chronic organization | In the most advanced stage, the pleural fluid becomes organized, resulting in the appearance of a fibrous layer that envelops the lung, hindering complete lung expansion, impairing lung function, and increasing the possibility of further infection. |
| Variables | Total N = 318 | Controls (No CPPE/Empyema) N = 212 | Cases (CPPE/Empyema) N = 106 | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | n | % | n | % | |||
| Sex | Female | 101 | (31.8) | 73 | (72.3) | 28 | (27.7) | 0.15 |
| Male | 217 | (68.2) | 139 | (64.1) | 78 | (35.9) | ||
| Alcohol intake | Drinker/ex-drinker | 273 | (85.8) | 188 | (68.9) | 85 | (31.1) | 0.041 |
| Never | 45 | (14.2) | 24 | (53.3) | 21 | (46.7) | ||
| Heart disease | No | 247 | (77.7) | 152 | (61.5) | 95 | (38.5) | <0.001 |
| Yes | 71 | (22.3) | 60 | (84.5) | 11 | (15.5) | ||
| COPD | No | 265 | (83.3) | 173 | (65.3) | 92 | (34.7) | 0.24 |
| Yes | 53 | (16.7) | 39 | (73.6) | 14 | (26.4) | ||
| Antibiotics in previous 3 months | No | 265 | (83.3) | 182 | (68.7) | 83 | (31.3) | 0.089 |
| Yes | 53 | (16.7) | 30 | (56.6) | 23 | (43.4) | ||
| Dyspnea | No | 152 | (47.8) | 101 | (66.4) | 51 | (33.6) | 0.94 |
| Yes | 166 | (52.2) | 111 | (66.9) | 55 | (33.1) | ||
| Cough | No | 96 | (30.2) | 58 | (60.4) | 38 | (39.6) | 0.12 |
| Yes | 222 | (69.8) | 154 | (69.4) | 68 | (30.6) | ||
| Expectoration | No | 164 | (51.6) | 103 | (62.8) | 61 | (37.2) | 0.13 |
| Yes | 154 | (48.4) | 109 | (70.8) | 45 | (29.2) | ||
| Pleuritic pain | No | 192 | (60.4) | 163 | (84.9) | 29 | (15.1) | <0.001 |
| Yes | 126 | (39.6) | 49 | (38.9) | 77 | (61.1) | ||
| Sepsis | No | 269 | (84.6) | 184 | (68.4) | 85 | (31.6) | 0.12 |
| Si | 49 | (15.4) | 28 | (57.1) | 21 | (42.9) | ||
| Pleural effusion | No | 210 | (66.0) | 210 | (100) | 0 | (0.0) | <0.001 |
| Yes | 108 | (34.0) | 2 | (1.9) | 106 | (98.1) | ||
| Radiological involvement | Unilobar | 220 | (69.2) | 169 | (76.8) | 51 | (23.2) | <0.001 |
| Multilobar | 98 | (30.8) | 43 | (43.9) | 55 | (56.1) | ||
| Corticosteroids | No | 254 | (79.9) | 156 | (61.4) | 98 | (38.6) | <0.001 |
| Yes | 64 | (20.1) | 56 | (87.5) | 8 | (12.5) | ||
| Variables | Total N = 318 | Controls (No CPPE/Empyema) N = 212 | Cases (CPPE/Empyema) N = 106 | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| n | (%col) | N | (%row) | n | (%row) | |||
| CURB65 | <2 | 118 | (37.1) | 67 | (56.8) | 51 | (43.2) | <0.001 |
| ≥2 | 174 | (54.7) | 135 | (77.6) | 39 | (22.4) | ||
| Missing | 26 | 8.2% | 10 | (38.5) | 16 | (61.5) | ||
| FINE | <90 | 204 | (64.2) | 132 | (64.7) | 72 | (35.3) | 0.32 |
| ≥90 | 114 | (35.8) | 80 | (70.2) | 34 | (29.8) | ||
| Systolic BP (mmHg) | Normal | 134 | (42.1) | 82 | (61.2) | 52 | (38.8) | 0.17 |
| <120 | 119 | (37.4) | 82 | (68.9) | 37 | (31.1) | ||
| >140 | 65 | (20.4) | 48 | (73.8) | 17 | (26.2) | ||
| Diastolic BP (mmHg) | Normal | 224 | (70.4) | 143 | (63.8) | 81 | (36.2) | 0.15 |
| <60 | 39 | (12.3) | 31 | (79.5) | 8 | (20.5) | ||
| >80 | 55 | (17.3) | 38 | (69.1) | 17 | (30.9) | ||
| Temperature (°C) | Normal | 231 | (72.6) | 146 | (63.2) | 85 | (36.8) | 0.069 |
| <36 | 22 | (6.9) | 15 | (68.2) | 7 | (31.8) | ||
| >38 | 65 | (20.4) | 51 | (78.5) | 14 | (21.5) | ||
| Heart rate (bpm) | Normal | 219 | (68.9) | 157 | (71.7) | 62 | (28.3) | 0.005 |
| Abnormal | 99 | (31.1) | 55 | (55.6) | 44 | (44.4) | ||
| O2 sat (%) | Normal | 159 | (50.0) | 98 | (61.6) | 61 | (38.4) | 0.057 |
| Abnormal | 159 | (50.0) | 114 | (71.7) | 45 | (28.3) | ||
| pH (ABG) | Normal | 131 | (41.2) | 87 | (66.4) | 44 | (33.6) | 0.44 |
| Abnormal | 132 | (41.5) | 92 | (69.7) | 40 | (30.3) | ||
| Missing | 55 | (17.3) | 33 | (60.0) | 22 | (40.0) | ||
| PaO2 (ABG) (mmHg) | Normal | 33 | (10.4) | 20 | (60.6) | 13 | (39.4) | 0.31 |
| Abnormal | 219 | (68.6) | 152 | (69.4) | 67 | (30.6) | ||
| Missing | 66 | (20.8) | 40 | (60.6) | 26 | (39.4) | ||
| PCO2 (ABG) (mmHg) | Normal | 149 | (46.9) | 105 | (70.5) | 44 | (29.5) | 0.30 |
| Abnormal | 115 | (36.2) | 75 | (65.2) | 40 | (34.8) | ||
| Missing | 54 | (17.0) | 32 | (59.3) | 22 | (40.7) | ||
| Bicarbonate (ABG) (mmol/L) | Normal | 103 | (32.4) | 70 | (68.0) | 33 | (32.0) | 0.45 |
| Abnormal low (<22 mmol/L) | 89 | (28.0) | 60 | (67.4) | 29 | (32.6) | ||
| Abnormal high (>26 mmol/L) | 69 | (21.7) | 49 | (71.0) | 20 | (29.0) | ||
| Missing | 57 | (17.9) | 33 | (57.9) | 24 | (42.1) | ||
| Lactate (mg/dL) | Normal | 77 | (24.3) | 47 | (61.0) | 30 | (39.0) | 0.008 |
| Abnormal | 45 | (14.2) | 39 | (86.7) | 6 | (13.3) | ||
| Missing | 195 | (61.5) | 125 | (64.1) | 70 | (35.9) | ||
| Glucose (mg/dL) | Normal | 80 | (25.2) | 49 | (61.3) | 31 | (38.8) | 0.24 |
| Abnormal | 238 | (74.8) | 163 | (68.5) | 75 | (31.5) | ||
| Urea (mg/dL) | Normal | 189 | (59.4) | 121 | (64.0) | 68 | (36.0) | 0.23 |
| Abnormal | 129 | (40.6) | 91 | (70.5) | 38 | (29.5) | ||
| Creatinine (mg/dL) | Normal | 244 | (76.7) | 158 | (64.8) | 86 | (35.2) | 0.19 |
| Abnormal | 74 | (23.3) | 54 | (73.0) | 20 | (27.0) | ||
| Albumin (g/dL) | Normal | 41 | (12.9) | 34 | (82.9) | 7 | (17.1) | <0.001 |
| Abnormal | 22 | (6.9) | 3 | (13.6) | 19 | (86.4) | ||
| Missing | 254 | (80.1) | 174 | (68.5) | 80 | (31.5) | ||
| Sodium (mEq/L) | Normal | 225 | (70.8) | 153 | (68.0) | 72 | (32.0) | 0.43 |
| Abnormal | 93 | (29.2) | 59 | (63.4) | 34 | (36.6) | ||
| Potassium (mEq/L) | Normal | 274 | (86.2) | 188 | (68.6) | 86 | (31.4) | 0.066 |
| Abnormal | 44 | (13.8) | 24 | (54.5) | 20 | (45.5) | ||
| AST (IU/L) | Normal | 235 | (73.9) | 160 | (68.1) | 75 | (31.9) | 0.47 |
| Abnormal | 60 | (18.9) | 36 | (60.0) | 24 | (40.0) | ||
| Missing | 23 | (7.2) | 16 | (69.6) | 7 | (30.4) | ||
| ALT (IU/L) | Normal | 235 | (73.9) | 158 | (67.2) | 77 | (32.8) | 0.72 |
| Abnormal | 83 | (26.1) | 54 | (65.1) | 29 | (34.9) | ||
| Hemoglobin (g/dL) | Normal | 210 | (66.0) | 146 | (69.5) | 64 | (30.5) | 0.13 |
| Abnormal | 108 | (34.0) | 66 | (61.1) | 42 | (38.9) | ||
| Leukocytes (cells/µL) | Normal | 111 | (34.9) | 96 | (86.5) | 15 | (13.5) | <0.001 |
| Abnormal | 207 | (65.1) | 116 | (56.0) | 91 | (44.0) | ||
| Platelets (cells/µL) | Normal | 243 | (76.4) | 168 | (69.1) | 75 | (30.9) | <0.001 |
| Abnormal low (<150,000) | 40 | (12.6) | 31 | (77.5) | 9 | (22.5) | ||
| Abnormal high (>450,000) | 35 | (11.0) | 13 | (37.1) | 22 | (62.9) | ||
| CRP (mg/L) | Normal | 10 | (3.1) | 8 | (80.0) | 2 | (20.0) | 0.51 |
| Abnormal | 308 | (96.9) | 204 | (66.2) | 104 | (33.8) | ||
| PCT (ng/mL) | Normal | 174 | (54.7) | 118 | (67.8) | 56 | (32.2) | 0.18 |
| Abnormal | 55 | (17.3) | 31 | (56.4) | 24 | (43.6) | ||
| Missing | 89 | (28.0) | 63 | (70.8) | 26 | (29.2) | ||
| Microbiological Study | Cases (N = 106) | Controls (N = 212) | p |
|---|---|---|---|
| Antigens in urine, n (%) performed | 72 (67.9%) | 164 (77.3%) | |
| Total | 10 (13.9%) | 13 (7.9%) | |
| Legionella | 0 | 1 | 0.67 |
| Pneumococcus | 10 | 12 | 0.10 |
| Blood tests, n (%) performed | 66 (62.3%) | 79 (37.3%) | |
| Total | 5 (7.6%) | 8 (10.1%) | 0.59 |
| Coagulase-negative staphylococci | 1 | ||
| Streptococcus pneumoniae | 3 | 1 | |
| Streptococcus mitis | 1 | ||
| Staphylococcus aureus | 1 | 1 | |
| Staphylococcus epidermidis | 1 | ||
| Staphylococcus hominis | 1 | ||
| Bacteroides | 1 | ||
| Corynebacterium | 1 | ||
| Enterococcus faecium | 1 | ||
| Sputum cultures, n (%) performed | 51 (48.1%) | 75 (35.4%) | |
| Total | 10 (19.6%) | 20 (26.7%) | 0.36 |
| S. pneumoniae | 3 | 1 | |
| Haemophylus influenzeae | 2 | 5 | |
| Enterococcus aerogens | 1 | ||
| Stenotrophomonas maltophilia | 1 | ||
| Pseudomonas aeruginosa | 1 | 2 | |
| Serratia marcescens | 1 | ||
| Moraxella catarrhalis | 1 | ||
| S. aureus | 4 | ||
| Klebsiella pneumoniae | 2 | ||
| Escherichia coli | 1 | ||
| Alcaligens | 1 | ||
| Corynebacterium | 1 | ||
| Shewanella | 1 | ||
| Enterobacter cloacae | 1 | ||
| Citrobacter youngae | 1 | ||
| Pleural fluid culture, n (%) performed | 106 (100%) | - | |
| Total | 33 (31.1%) | ||
| Streptococcus constellatus | 12 | ||
| S. pneumoniae | 6 | ||
| Streptococcus viridans | 2 | ||
| Streptococcus pyogenes | 2 | ||
| Streptococcus anginosus | 1 | ||
| Staphylococcus intermedius | 1 | ||
| Staphylococcus aureus | 3 | ||
| Staphylococcus epidermidis | 2 | ||
| E. cloaecae | 1 | ||
| Gemella | 1 | ||
| Peptoestreptococcus | 1 | ||
| Fusobacterium nucleatum | 1 |
| Quantitative Variables | Controls (No CPPE/Empyema) N = 212 | Cases (CPPE/Empyema) N = 106 | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age in years | 67.91 | 18.92 | 59.41 | 17.43 | <0.001 |
| Charlson index | 3.62 | 2.33 | 2.76 | 2.64 | 0.003 |
| Pre-treatment interval | 5.50 | 7.56 | 13.17 | 14.78 | <0.001 |
| OR | 95% CI | p Value | ||
| Male sex | 1.91 | (0.94–3.88) | 0.074 | |
| Age | 0.99 | (0.97–1.02) | 0.56 | |
| Pre-treatment interval | 1.08 | (1.04–1.12) | <0.001 | |
| Charlson index | 1.01 | (0.82–1.23) | 0.95 | |
| Pleuritic pain | 7.42 | (3.83–14.38) | <0.001 | |
| Radiological involvement | Unilobar | 1 | ||
| Multilobar | 4.48 | (2.26–8.88) | <0.001 | |
| Leukocytes | Normal 3800–11,500 | 1 | ||
| Abnormal | 4.12 | (1.94–8.76) | <0.001 | |
| Corticosteroid treatment | No | 1 | ||
| Yes | 0.24 | (0.09–0.61) | 0.003 | |
| Cutoff | Sensitivity | Specificity | Youden Index | Total Accuracy % | ||
|---|---|---|---|---|---|---|
| % | (95% CI) | % | (95% CI) | |||
| 0.05 | 98.1 | (95.5–100.7) | 32.5 | (26.2–38.8) | 0.306 | 54.4 |
| 0.10 | 96.2 | (92.6–99.8) | 47.2 | (40.5–53.9) | 0.434 | 63.5 |
| 0.15 | 93.4 | (88.7–98.1) | 59.9 | (53.3–66.5) | 0.533 | 71.1 |
| 0.20 | 89.6 | (83.8–95.4) | 70.3 | (64.1–76.5) | 0.599 | 76.7 |
| 0.25 | 84.0 | (77.0–91.0) | 75.5 | (69.7–81.3) | 0.595 | 78.3 |
| 0.30 | 79.2 | (71.5–86.9) | 80.2 | (74.8–85.6) | 0.594 | 79.9 |
| 0.35 | 77.4 | (69.4–85.4) | 83.0 | (77.9–88.1) | 0.604 | 81.1 |
| 0.40 | 74.5 | (66.2–82.8) | 85.4 | (80.6–90.2) | 0.599 | 81.8 |
| 0.45 | 72.6 | (64.1–81.1) | 88.7 | (84.4–93.0) | 0.613 | 83.3 |
| 0.50 | 71.7 | (63.1–80.3) | 90.1 | (86.1–94.1) | 0.618 | 84.0 |
| 0.55 | 68.9 | (60.1–77.7) | 92.0 | (88.3–95.7) | 0.609 | 84.3 |
| 0.60 | 61.3 | (52.0–70.6) | 95.3 | (92.5–98.1) | 0.566 | 84.0 |
| 0.65 | 55.7 | (46.2–65.2) | 95.8 | (93.1–98.5) | 0.515 | 82.4 |
| 0.70 | 50.0 | (40.5–59.5) | 96.7 | (94.3–99.1) | 0.467 | 81.1 |
| 0.75 | 44.3 | (34.8–53.8) | 96.7 | (94.3–99.1) | 0.410 | 79.2 |
| 0.80 | 38.7 | (29.4–48.0) | 97.2 | (95.0–99.4) | 0.359 | 77.7 |
| 0.85 | 30.2 | (21.5–38.9) | 97.6 | (95.5–99.7) | 0.278 | 75.2 |
| 0.90 | 17.0 | (9.8–24.2) | 98.6 | (97.0–100.2) | 0.156 | 71.4 |
| 0.95 | 8.5 | (3.2–13.8) | 99.5 | (98.6–100.4) | 0.080 | 69.2 |
| Cutoff | PPV | (95% CI) | NPV | (95% CI) | LR+ | (95% CI) | LR− | (95% CI) |
|---|---|---|---|---|---|---|---|---|
| 0.05 | 42.1 | (35.9–48.3) | 97.2 | (93.4–101.0) | 1.4 | (1.3–1.6) | 0.1 | (0.0–0.2) |
| 0.10 | 47.7 | (41.0–54.4) | 96.2 | (92.5–99.9) | 1.8 | (1.6–2.1) | 0.1 | (0.0–0.2) |
| 0.15 | 53.8 | (46.6–61.0) | 94.8 | (91.0–98.6) | 2.3 | (2.0–2.8) | 0.1 | (0.1–0.2) |
| 0.20 | 60.1 | (52.5–67.7) | 93.1 | (89.2–97.0) | 3.0 | (2.4–3.7) | 0.1 | (0.1–0.3) |
| 0.25 | 63.1 | (55.1–71.1) | 90.4 | (86.1–94.7) | 3.4 | (2.7–4.4) | 0.2 | (0.1–0.3) |
| 0.30 | 66.7 | (58.5–74.9) | 88.5 | (84.0–93.0) | 4.0 | (3.0–5.3) | 0.3 | (0.2–0.4) |
| 0.35 | 69.5 | (61.2–77.8) | 88.0 | (83.5–92.5) | 4.5 | (3.4–6.2) | 0.3 | (0.2–0.4) |
| 0.40 | 71.8 | (63.4–80.2) | 87.0 | (82.4–91.6) | 5.1 | (3.7–7.1) | 0.3 | (0.2–0.4) |
| 0.45 | 76.2 | (67.9–84.5) | 86.6 | (82.1–91.1) | 6.4 | (4.4–9.4) | 0.3 | (0.2–0.4) |
| 0.50 | 78.4 | (70.2–86.6) | 86.4 | (81.9–90.9) | 7.2 | (4.8–10.9) | 0.3 | (0.2–0.4) |
| 0.55 | 81.1 | (73.0–89.2) | 85.5 | (80.9–90.1) | 8.6 | (5.4–13.7) | 0.3 | (0.3–0.5) |
| 0.60 | 86.7 | (79.0–94.4) | 83.1 | (78.4–87.8) | 13.0 | (7.1–24.0) | 0.4 | (0.3–0.5) |
| 0.65 | 86.8 | (78.8–94.8) | 81.2 | (76.4–86.0) | 13.3 | (7.0–25.3) | 0.5 | (0.4–0.6) |
| 0.70 | 88.3 | (80.2–96.4) | 79.5 | (74.6–84.4) | 15.2 | (7.3–31.6) | 0.5 | (0.4–0.6) |
| 0.75 | 87.0 | (78.0–96.0) | 77.7 | (72.7–82.7) | 13.4 | (6.4–28.0) | 0.6 | (0.5–0.7) |
| 0.80 | 87.2 | (77.6–96.8) | 76.0 | (70.9–81.1) | 13.8 | (6.2–30.6) | 0.6 | (0.5–0.7) |
| 0.85 | 86.5 | (75.5–97.5) | 73.7 | (68.6–78.8) | 12.6 | (5.3–30.1) | 0.7 | (0.6–0.8) |
| 0.90 | 85.7 | (70.7–100.7) | 70.4 | (65.2–75.6) | 12.1 | (3.9–37.6) | 0.8 | (0.8–0.9) |
| 0.95 | 90.0 | (71.4–108.6) | 68.5 | (63.3–73.7) | 17.0 | (2.4–120.6) | 0.9 | (0.9–1.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravo Jover, R.M.; Gil-Guillen, V.F.; Pérez Barba, C.; Quesada, J.A.; García López, M.; García Soriano, I.; Pascual Pérez, M.d.l.R. Factors Associated with Complicated Parapneumonic Pleural Effusion/Empyema in Patients with Community-Acquired Pneumonia: The EMPIR Study. J. Clin. Med. 2025, 14, 1739. https://doi.org/10.3390/jcm14051739
Bravo Jover RM, Gil-Guillen VF, Pérez Barba C, Quesada JA, García López M, García Soriano I, Pascual Pérez MdlR. Factors Associated with Complicated Parapneumonic Pleural Effusion/Empyema in Patients with Community-Acquired Pneumonia: The EMPIR Study. Journal of Clinical Medicine. 2025; 14(5):1739. https://doi.org/10.3390/jcm14051739
Chicago/Turabian StyleBravo Jover, Rosa María, Vicente F. Gil-Guillen, Carlos Pérez Barba, Jose Antonio Quesada, María García López, Isabel García Soriano, and María de los Reyes Pascual Pérez. 2025. "Factors Associated with Complicated Parapneumonic Pleural Effusion/Empyema in Patients with Community-Acquired Pneumonia: The EMPIR Study" Journal of Clinical Medicine 14, no. 5: 1739. https://doi.org/10.3390/jcm14051739
APA StyleBravo Jover, R. M., Gil-Guillen, V. F., Pérez Barba, C., Quesada, J. A., García López, M., García Soriano, I., & Pascual Pérez, M. d. l. R. (2025). Factors Associated with Complicated Parapneumonic Pleural Effusion/Empyema in Patients with Community-Acquired Pneumonia: The EMPIR Study. Journal of Clinical Medicine, 14(5), 1739. https://doi.org/10.3390/jcm14051739