

Efficacy of Myopia Prevention in At-Risk Children: A Systematic Review and Network Meta-Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Outcome Measures
2.4. Data Sources and Literature Searches
2.5. Risk-of-Bias Assessment
2.6. Data Extraction
2.7. Data Synthesis and Analysis
2.8. Data and Resource Availability
3. Results
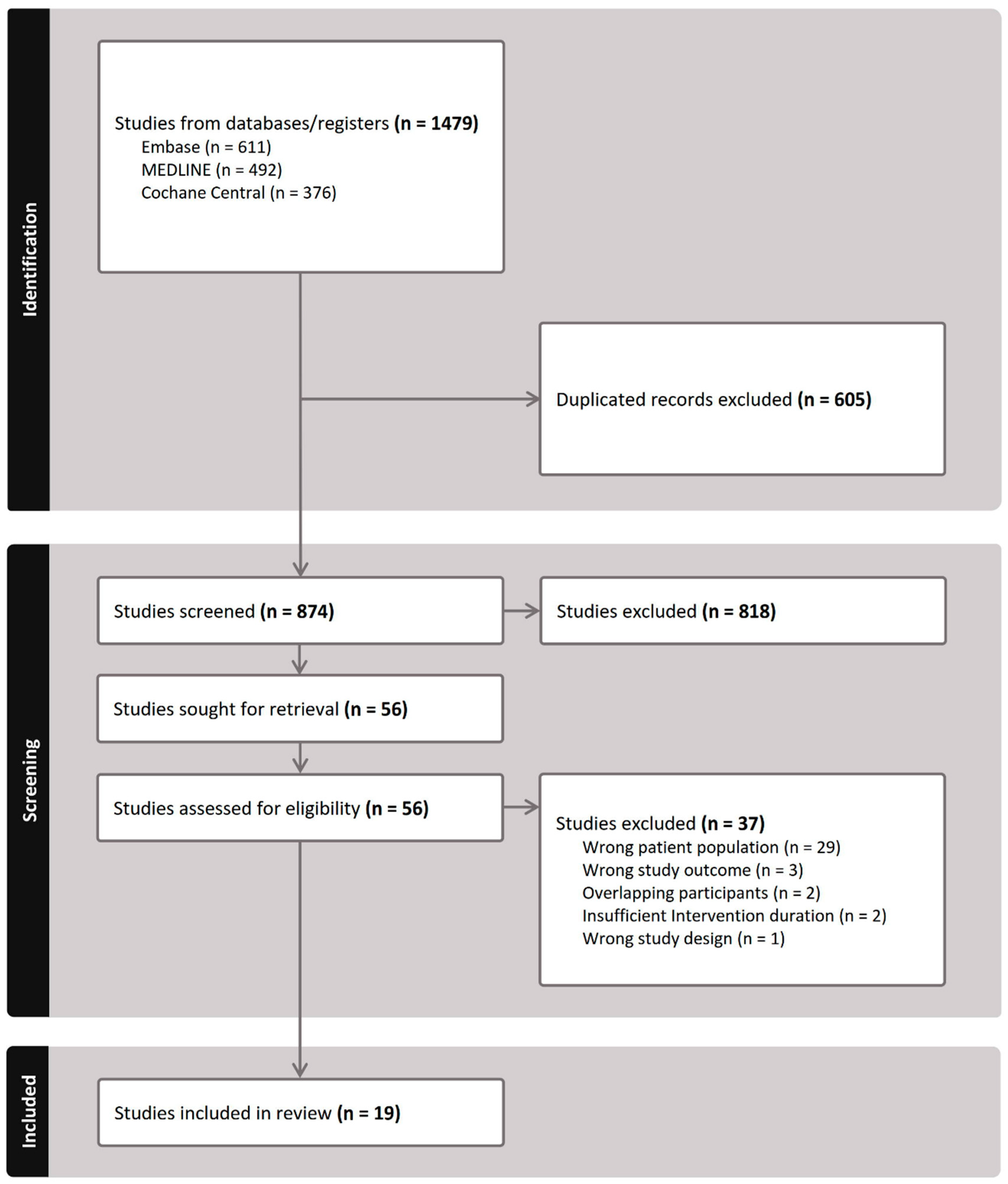
3.1. Literature Search
3.2. Characteristics of the Included Studies
3.3. Results of Risk-of-Bias Assessment
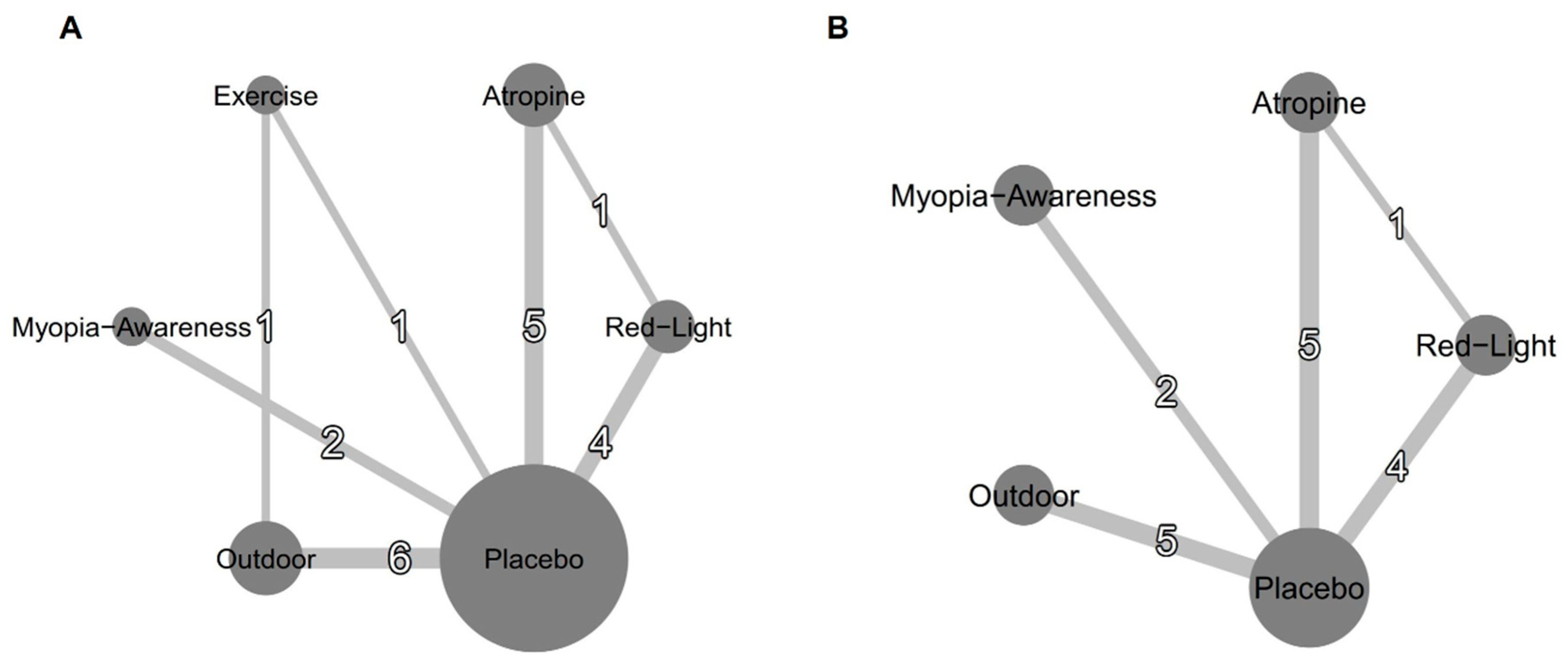
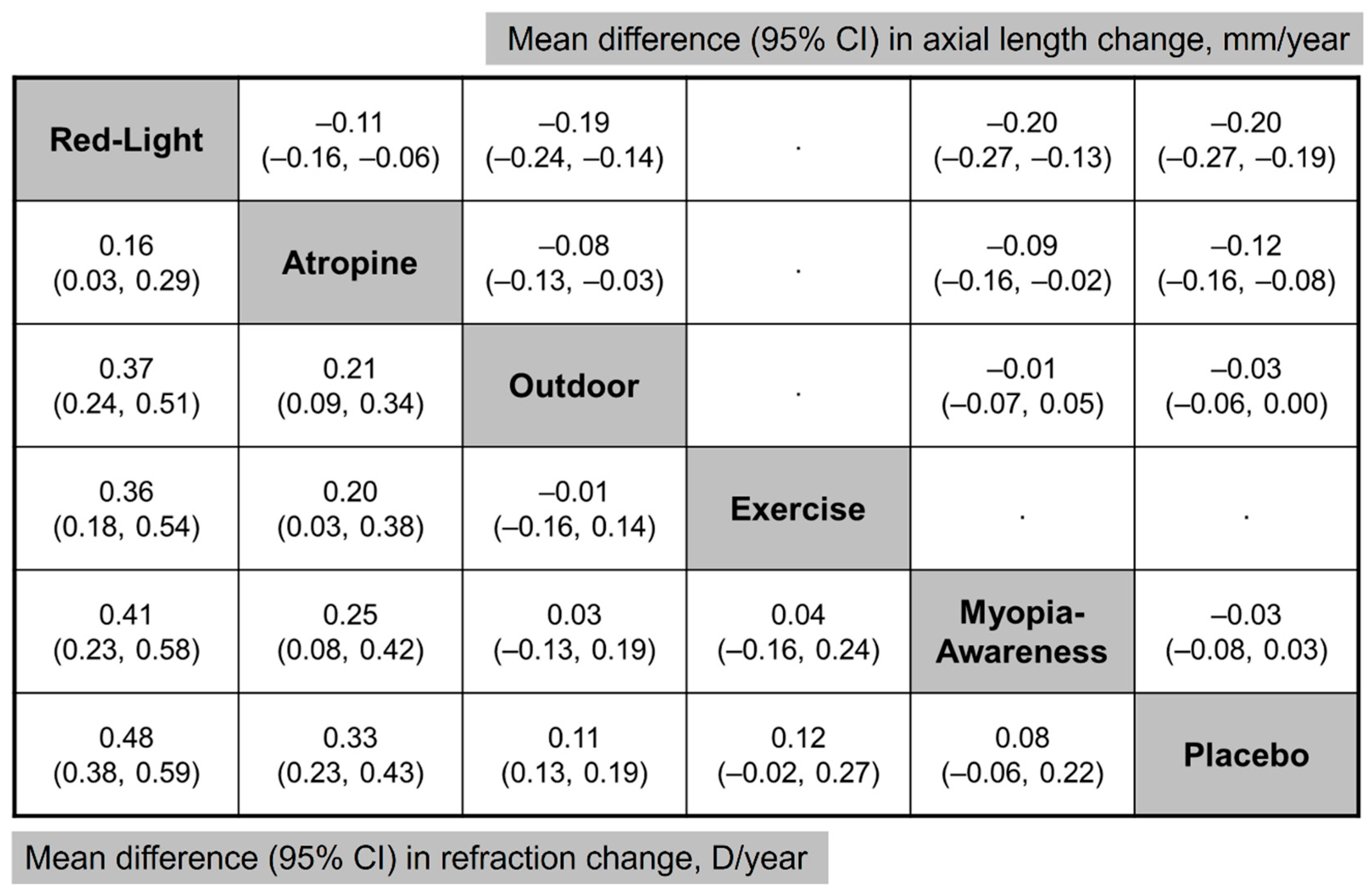
3.4. Primary Outcome: SE and AL
3.5. Secondary Outcome: Myopia Incidence and Adverse Events
3.6. Inconsistency Test and Sensitivity Analyses
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Dolgin, E. The myopia boom. Nature 2015, 519, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Tideman, J.W.; Snabel, M.C.; Tedja, M.S.; van Rijn, G.A.; Wong, K.T.; Kuijpers, R.W.; Vingerling, J.R.; Hofman, A.; Buitendijk, G.H.; Keunen, J.E.; et al. Association of Axial Length With Risk of Uncorrectable Visual Impairment for Europeans With Myopia. JAMA Ophthalmol. 2016, 134, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.L.; Sabanayagam, C.; Ding, Y.; Wong, C.W.; Yeo, A.C.; Cheung, Y.B.; Cheung, G.; Chia, A.; Ohno-Matsui, K.; Wong, T.Y.; et al. Prevalence, Risk Factors, and Impact of Myopic Macular Degeneration on Visual Impairment and Functioning Among Adults in Singapore. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4603–4613. [Google Scholar] [CrossRef]
- Pan, C.W.; Cheng, C.Y.; Saw, S.M.; Wang, J.J.; Wong, T.Y. Myopia and age-related cataract: A systematic review and meta-analysis. Am. J. Ophthalmol. 2013, 156, 1021–1033.e1021. [Google Scholar] [CrossRef]
- Marcus, M.W.; de Vries, M.M.; Junoy Montolio, F.G.; Jansonius, N.M. Myopia as a risk factor for open-angle glaucoma: A systematic review and meta-analysis. Ophthalmology 2011, 118, 1989–1994.e2. [Google Scholar] [CrossRef]
- Sankaridurg, P.; Berntsen, D.A.; Bullimore, M.A.; Cho, P.; Flitcroft, I.; Gawne, T.J.; Gifford, K.L.; Jong, M.; Kang, P.; Ostrin, L.A.; et al. IMI 2023 Digest. Investig. Ophthalmol. Vis. Sci. 2023, 64, 7. [Google Scholar] [CrossRef]
- Lawrenson, J.G.; Shah, R.; Huntjens, B.; Downie, L.E.; Virgili, G.; Dhakal, R.; Verkicharla, P.K.; Li, D.; Mavi, S.; Kernohan, A.; et al. Interventions for myopia control in children: A living systematic review and network meta-analysis. Cochrane Database Syst. Rev. 2023, 2023, Cd014758. [Google Scholar] [CrossRef]
- Jonas, J.B.; Ang, M.; Cho, P.; Guggenheim, J.A.; He, M.G.; Jong, M.; Logan, N.S.; Liu, M.; Morgan, I.; Ohno-Matsui, K.; et al. IMI Prevention of Myopia and Its Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 6. [Google Scholar] [CrossRef]
- Yam, J.C.; Zhang, X.J.; Zhang, Y.; Yip, B.H.K.; Tang, F.; Wong, E.S.; Bui, C.H.T.; Kam, K.W.; Ng, M.P.H.; Ko, S.T.; et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children: The LAMP2 Randomized Clinical Trial. JAMA 2023, 329, 472–481. [Google Scholar] [CrossRef]
- Dong, J.; Zhu, Z.; Xu, H.; He, M. Myopia Control Effect of Repeated Low-Level Red-Light Therapy in Chinese Children: A Randomized, Double-Blind, Controlled Clinical Trial. Ophthalmology 2023, 130, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Chen, Y.; Tan, Z.; Xiong, R.; McGuinness, M.B.; Müller, A. Interventions recommended for myopia prevention and control among children and adolescents in China: A systematic review. Br. J. Ophthalmol. 2023, 107, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; French, A.N.; Ashby, R.S.; Guo, X.; Ding, X.; He, M.; Rose, K.A. The epidemics of myopia: Aetiology and prevention. Prog. Retin. Eye Res. 2018, 62, 134–149. [Google Scholar] [CrossRef]
- Wu, P.-C.; Chen, C.-T.; Lin, K.-K.; Sun, C.-C.; Kuo, C.-N.; Huang, H.-M.; Poon, Y.-C.; Yang, M.-L.; Chen, C.-Y.; Huang, J.-C.; et al. Myopia Prevention and Outdoor Light Intensity in a School-Based Cluster Randomized Trial. Ophthalmology 2018, 125, 1239–1250. [Google Scholar] [CrossRef]
- Li, S.-M.; Ran, A.-R.; Kang, M.-T.; Yang, X.; Ren, M.-Y.; Wei, S.-F.; Gan, J.-H.; Li, L.; He, X.; Li, H.; et al. Effect of Text Messaging Parents of School-Aged Children on Outdoor Time to Control Myopia: A Randomized Clinical Trial. JAMA Pediatr. 2022, 176, 1077–1083. [Google Scholar] [CrossRef]
- Liao, S.; Li, X.; Bai, N.; Wu, D.; Yang, W.; Wang, F.; Ji, H.Z. An empirical study on the effect of outdoor illumination and exercise intervention on Children’s vision. Front. Public Health 2023, 11, 1270826. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- White, I.R.; Barrett, J.K.; Jackson, D.; Higgins, J.P. Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression. Res. Synth. Methods 2012, 3, 111–125. [Google Scholar] [CrossRef]
- Higgins, J.P.; Jackson, D.; Barrett, J.K.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef]
- Cao, K.; Tian, L.; Ma, D.-L.; Zhao, S.-Q.; Li, A.; Jin, Z.-B.; Jie, Y. Daily Low-Level Red Light for Spherical Equivalent Error and Axial Length in Children With Myopia: A Randomized Clinical Trial. JAMA Ophthalmol. 2024, 142, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Xiong, R.; Zhang, J.; Han, X.; Jin, L.; Liu, W.; Qu, Y.; Chen, Q.; Chen, S.; Chen, X.; et al. Effect of Extracurricular After-School Physical Activities on Academic Performance of Schoolchildren: A Cluster Randomized Clinical Trial. JAMA Pediatr. 2023, 177, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Rong, H.; Liu, Y.; Wang, B.; Du, B.; Song, D.; Wei, R. Effectiveness of repeated low-level red light in myopia prevention and myopia control. Br. J. Ophthalmol. 2024, 108, 1299–1305. [Google Scholar] [CrossRef]
- He, M.; Xiang, F.; Zeng, Y.; Mai, J.; Chen, Q.; Zhang, J.; Smith, W.; Rose, K.; Morgan, I.G. Effect of Time Spent Outdoors at School on the Development of Myopia Among Children in China: A Randomized Clinical Trial. JAMA 2015, 314, 1142–1148. [Google Scholar] [CrossRef]
- He, X.; Sankaridurg, P.; Wang, J.; Chen, J.; Naduvilath, T.; He, M.; Zhu, Z.; Li, W.; Morgan, I.G.; Xiong, S.; et al. Time Outdoors in Reducing Myopia: A School-Based Cluster Randomized Trial with Objective Monitoring of Outdoor Time and Light Intensity. Ophthalmology 2022, 129, 1245–1254. [Google Scholar] [CrossRef]
- He, X.; Wang, J.; Zhu, Z.; Xiang, K.; Zhang, X.; Zhang, B.; Chen, J.; Yang, J.; Du, L.; Niu, C.; et al. Effect of Repeated Low-level Red Light on Myopia Prevention Among Children in China With Premyopia: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e239612. [Google Scholar] [CrossRef]
- Hua, W.; Jin, J.; Wu, X.; Yang, J.; Jiang, X.; Gao, G.; Tao, F. Elevated light levels in schools have a protective effect on myopia. Ophthalmic Physiol. Opt. 2015, 35, 252–262. [Google Scholar] [CrossRef]
- Jethani, J. Efficacy of low-concentration atropine (0.01%) eye drops for prevention of axial myopic progression in premyopes. Indian J. Ophthalmol. 2022, 70, 238–240. [Google Scholar] [CrossRef]
- Li, Q.; Guo, L.; Zhang, J.; Zhao, F.; Hu, Y.; Guo, Y.; Du, X.; Zhang, S.; Yang, X.; Lu, C. Effect of School-Based Family Health Education via Social Media on Children’s Myopia and Parents’ Awareness: A Randomized Clinical Trial. JAMA Ophthalmol. 2021, 139, 1165–1172. [Google Scholar] [CrossRef]
- Shang, L.; Gao, S.; Wang, W.; Chang, M.; Ma, N.; Huang, C.; Yu, S.; Wang, M.; Fu, A. Comparison of Changes in Retinal Vascular Density and Thickness After Using Low-Level Red Light and 0.01% Atropine in Premyopic Children. Transl. Vis. Sci. Technol. 2024, 13, 23. [Google Scholar] [CrossRef]
- Tong, L.; Chen, J.; Liu, L.; Kang, M.; Liao, X.; Ying, P.; Ling, Q.; Zou, J.; Wei, H.; Wang, Y.; et al. Temporal effects of an original myopia song on school children’s myopia and awareness: A 3-year prospective study. Clin. Exp. Optom. 2024, 107, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, F.; Yu, S.; Ma, N.; Huang, C.; Wang, M.; Wei, L.; Zhang, J.; Fu, A. Prevention of myopia shift and myopia onset using 0.01% atropine in premyopic children—A prospective, randomized, double-masked, and crossover trial. Eur. J. Pediatr. 2023, 182, 2597–2606. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Lyu, Y.; Wang, W.; Cui, C.; Wei, L.; Huang, C.; Ma, N.; Zhao, B.; Zhang, J.; Fu, A. Effects of 0.01% atropine eye drops on the prevention of myopia onset among schoolchildren: A randomized, double-blind, controlled trial. Chin. J. Exp. Ophthalmol. 2022, 40, 533–540. [Google Scholar] [CrossRef]
- Liu, Z.; Sun, Z.; Du, B.; Gou, H.; Wang, B.; Lin, Z.; Ren, N.; Pazo, E.E.; Liu, L.; Wei, R. The Effects of Repeated Low-Level Red-Light Therapy on the Structure and Vasculature of the Choroid and Retina in Children with Premyopia. Ophthalmol. Ther. 2024, 13, 739–759. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, L.; Guo, L.; Guo, Y.; Zhao, F.; Hu, Y.; Li, Q.; Du, X.; Deng, X.; Deng, N.; et al. Effects of online family health education on myopia prevention in children by parental myopia: A randomized clinical trial. Clin. Exp. Optom. 2024, 107, 299–306. [Google Scholar] [CrossRef]
- Landis, E.G.; Park, H.N.; Chrenek, M.; He, L.; Sidhu, C.; Chakraborty, R.; Strickland, R.; Iuvone, P.M.; Pardue, M.T. Ambient Light Regulates Retinal Dopamine Signaling and Myopia Susceptibility. Investig. Ophthalmol. Vis. Sci. 2021, 62, 28. [Google Scholar] [CrossRef]
- Flitcroft, D.I. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog. Retin. Eye Res. 2012, 31, 622–660. [Google Scholar] [CrossRef]
- Wu, P.C.; Chen, C.T.; Chang, L.C.; Niu, Y.Z.; Chen, M.L.; Liao, L.L.; Rose, K.; Morgan, I.G. Increased Time Outdoors Is Followed by Reversal of the Long-Term Trend to Reduced Visual Acuity in Taiwan Primary School Students. Ophthalmology 2020, 127, 1462–1469. [Google Scholar] [CrossRef]
- Dolgin, E. A myopia epidemic is sweeping the globe. Here’s how to stop it. Nature 2024, 629, 989–991. [Google Scholar] [CrossRef]
- Lan, W.; Pan, W.; Wen, L.; Luo, Z.; Flitcroft, I.; Yang, Z. Effect of Outdoor Scene Classrooms on Myopia Prevention and Control: One-year Result from a Randomized Clinical Trial. Investig. Ophthalmol. Vis. Sci. 2024, 65, 129. [Google Scholar]
- Wang, C.Y.; Hsu, N.W.; Yang, Y.C.; Chen, Y.L.; Shyong, M.P.; Tsai, D.C. Premyopia at Preschool Age: Population-based Evidence of Prevalence and Risk Factors from a Serial Survey in Taiwan. Ophthalmology 2022, 129, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Wu, P.C.; Ostrin, L.A.; Tideman, J.W.L.; Yam, J.C.; Lan, W.; Baraas, R.C.; He, X.; Sankaridurg, P.; Saw, S.M.; et al. IMI Risk Factors for Myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 3. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Tarczy-Hornoch, K.; Cotter, S.A.; Matsumura, S.; Mitchell, P.; Rose, K.A.; Katz, J.; Saw, S.M.; Varma, R. Association of Parental Myopia With Higher Risk of Myopia Among Multiethnic Children Before School Age. JAMA Ophthalmol. 2020, 138, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.C.; Chung, M.Y.; Yu, H.J.; Wu, P.C. Prevention of myopia onset with 0.025% atropine in premyopic children. J. Ocul. Pharmacol. Ther. 2010, 26, 341–345. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Flitcroft, D.I.; Gifford, K.L.; Jong, M.; Jones, L.; Klaver, C.C.W.; Logan, N.S.; Naidoo, K.; Resnikoff, S.; Sankaridurg, P.; et al. IMI—Myopia Control Reports Overview and Introduction. Investig. Ophthalmol. Vis. Sci. 2019, 60, M1–M19. [Google Scholar] [CrossRef]
- Schaeffel, F.; Swiatczak, B. Mechanisms of emmetropization and what might go wrong in myopia. Vis. Res. 2024, 220, 108402. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Jong, M.; Brennan, N.A. Myopia control: Seeing beyond efficacy. Optom. Vis. Sci. 2024, 101, 134–142. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhu, Z.; Tan, X.; Kong, X.; Zhong, H.; Zhang, J.; Xiong, R.; Yuan, Y.; Zeng, J.; Morgan, I.G.; et al. Effect of Repeated Low-Level Red-Light Therapy for Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology 2022, 129, 509–519. [Google Scholar] [CrossRef]
- Chia, A.; Lu, Q.S.; Tan, D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016, 123, 391–399. [Google Scholar] [CrossRef]
- Polling, J.R.; Kok, R.G.; Tideman, J.W.; Meskat, B.; Klaver, C.C. Effectiveness study of atropine for progressive myopia in Europeans. Eye 2016, 30, 998–1004. [Google Scholar] [CrossRef]
- Chen, J.; Wang, J.; Qi, Z.; Liu, S.; Zhao, L.; Zhang, B.; Dong, K.; Du, L.; Yang, J.; Zou, H.; et al. Smartwatch Measures of Outdoor Exposure and Myopia in Children. JAMA Netw. Open 2024, 7, e2424595. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C.; Sun, C.C.; Lee, T.C.; Wang, Y.N.; Liao, L.L. Shared decision-making, treatment decision regret, and vision-related quality of life among parents of children with myopia: An online survey in Taiwan. Cont. Lens Anterior Eye 2024, 47, 102283. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Tsai, P.C.; Chiu, Y.C.; Wang, J.H.; Chiu, C.J. Myopia progression after cessation of atropine in children: A systematic review and meta-analysis. Front. Pharmacol. 2024, 15, 1343698. [Google Scholar] [CrossRef] [PubMed]
- Xiong, R.; Zhu, Z.; Jiang, Y.; Kong, X.; Zhang, J.; Wang, W.; Kiburg, K.; Yuan, Y.; Chen, Y.; Zhang, S.; et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin. Exp. Ophthalmol. 2022, 50, 1013–1024. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, L.; Lv, Y.; Tang, P.; Feng, Y.; Wu, M.; Xu, L.; Jonas, J.B. Outdoor Jogging and Myopia Progression in School Children From Rural Beijing: The Beijing Children Eye Study. Transl. Vis. Sci. Technol. 2019, 8, 2. [Google Scholar] [CrossRef]
- Li, Y.; Yip, M.Y.T.; Ting, D.S.W.; Ang, M. Artificial intelligence and digital solutions for myopia. Taiwan J. Ophthalmol. 2023, 13, 142–150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Follow-Up (Months) | Intervention | Sample Size | Male (%) | Age (Years) | Baseline SE (D) | Baseline AL (mm) | Region |
|---|---|---|---|---|---|---|---|---|
| Cao 2024 [21] | 12 | Red Light (3 min/BID) | 56 | 46.4 | 9.1 ± 2.0 | 0.2 ± 0.6 | 23.1 ± 0.8 | China |
| Placebo | 56 | 48.2 | 9.0 ± 1.9 | 0.3 ± 0.5 | 23.1 ± 0.7 | |||
| D. Wang 2023 [22] | 9 | Outdoor (600 min/week) | 702 | 50.4 | 9.2 ± 0.6 | 0.6 ± 1.1 | 23.1 ± 0.8 | China |
| Placebo | 728 | 47.3 | 0.6 ± 1.1 | 23.1 ± 0.8 | ||||
| G. Liu 2024 [23] | 12 | Red Light (3 min/BID) | 40 | 55.0 | 9.0 ± 0.9 | 0.4 ± 0.3 | 23.4 ± 0.6 | China |
| Placebo | 36 | 47.2 | 8.9 ± 1.1 | 0.4 ± 0.3 | 23.3 ± 0.8 | |||
| He 2015 [24] | 36 | Outdoor (200 min/week) | 853 | 52.6 | 6.6 ± 0.3 | 1.3 ± 1.0 | 22.6 ± 0.7 | China |
| Placebo | 726 | 54.7 | 6.6 ± 0.3 | 1.3 ± 0.8 | 22.7 ± 0.7 | |||
| He 2022 [25] | 24 | Outdoor (200–400 min/week) | 3459 | 53.0 | 7.3 ± 0.7 | 1.0 ± 1.0 | 22.9 ± 0.8 | China |
| Placebo | 1608 | 53.9 | 7.2 ± 0.7 | 1.0 ± 1.0 | 22.9 ± 0.8 | |||
| He 2023 [26] | 12 | Red Light (3 min/BID) | 120 | 51.1 | 8.3 ± 1.1 | 0.1 ± 0.3 | 23.4 ± 0.7 | China |
| Placebo | 111 | 48.9 | 8.3 ± 1.1 | 0.2 ± 0.3 | 23.3 ± 0.7 | |||
| Hua 2015 [27] | 12 | Outdoor | 87 | 51.7 | 10.7 ± 2.4 | 0.6 ± 0.5 | 23.1 ± 0.6 | China |
| Placebo | 69 | 46.4 | 10.5 ± 2.3 | 0.6 ± 0.5 | 23.1 ± 0.7 | |||
| Jethani 2022 [28] | 24 | Atropine (0.01%QD) | 30 | N/A | 7.7 ± 2.1 | N/A | 20.8 ± 0.6 | India |
| Placebo | 30 | 7.2 ± 1.9 | 21.0 ± 0.5 | |||||
| Li 2021 [29] | 24 | Myopia Awareness Program | 544 | 54.6 | 6.3 ± 0.5 | 1.1 ± 1.0 | 22.7 ± 0.7 | China |
| Placebo | 700 | 54.9 | 6.3 ± 0.5 | 1.0 ± 1.0 | 22.7 ± 0.7 | |||
| Li 2022 [15] | 12 | Myopia Awareness Program | 114 | 52.6 | 8.4 ± 0.3 | 0.7 ± 1.1 | 23.1 ± 0.7 | China |
| Placebo | 110 | 57.1 | 8.4 ± 0.3 | 0.4 ± 1.3 | 23.2 ± 0.8 | |||
| Liao 2023 [16] | 12 | Outdoor (180 min/week) | 25 | 52.0 | 6.4 ± 0.5 | 1.5 ± 0.2 | N/A | China |
| Exercise (180 min/week) | 24 | 58.3 | 6.5 ± 0.5 | 1.6 ± 0.2 | ||||
| Placebo | 25 | 52.0 | 6.5 ± 0.5 | 1.5 ± 0.2 | ||||
| Shang 2024 [30] | 6 | Red Light (3 min/BID) | 32 | 46.9 | 8.8 ± 1.2 | −0.2 ± 0.3 | 23.6 ± 0.8 | China |
| Atropine (0.01%QD) | 30 | 53.3 | 8.8 ± 1.1 | −0.2 ± 0.3 | 23.6 ± 0.7 | |||
| Tong 2024 [31] | 36 | Myopia Awareness Program | 163 | 51.0 | 9.4 ± 1.5 | N/A | N/A | China |
| Placebo | 159 | 52.5 | 9.2 ± 1.2 | |||||
| W. Wang 2023 [32] | 6 | Atropine (0.01%QD) | 26 | 46.7 | 8.6 ± 1.7 | −0.2 ± 0.3 | 23.6 ± 0.8 | China |
| Placebo | 25 | 50.0 | 8.5 ± 1.7 | −0.2 ± 0.3 | 23.6 ± 0.8 | |||
| Wu 2018 [14] | 12 | Outdoor (660 min/week) | 235 | 55.1 | 6.3 ± 0.5 | 0.4 ± 1.1 | 22.8 ± 0.8 | Taiwan |
| Placebo | 385 | 50.3 | 0.3 ± 1.0 | 22.8 ± 0.8 | ||||
| Yam 2023 [10] | 24 | Atropine (0.01%QD) | 122 | 49.1 | 6.9 ± 1.4 | 0.5 ± 0.3 | 22.9 ± 0.7 | Hong Kong |
| Atropine (0.05%QD) | 116 | 50.6 | 6.9 ± 1.4 | 0.5 ± 0.3 | 22.8 ± 0.7 | |||
| Placebo | 115 | 50.3 | 6.8 ± 1.3 | 0.5 ± 0.3 | 22.8 ± 0.6 | |||
| Yu 2022 [33] | 6 | Atropine (0.01%QD) | 26 | 42.3 | 8.4 ± 1.5 | −0.2 ± 0.3 | 23.5 ± 0.7 | China |
| Placebo | 25 | 48.0 | 8.7 ± 1.9 | −0.2 ± 0.3 | 23.6 ± 0.8 | |||
| Z. Liu 2024 [34] | 12 | Red Light (3 min/BID) | 43 | 55.8 | 9.0 ± 1.3 | 0.2 ± 0.4 | 23.6 ± 0.8 | China |
| Placebo | 42 | 52.4 | 9.0 ± 1.5 | 0.3 ± 0.4 | 23.3 ± 0.7 | |||
| Zhang 2024 [35] | 36 | Myopia Awareness Program | 1138 | 53.9 | 6.9 ± 0.7 | 1.0 ± 0.9 | 22.9 ± 0.7 | China |
| Placebo | 1238 | 55.1 | 6.8 ± 0.7 | 1.0 ± 0.9 | 22.9 ± 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Tseng, B.-Y.; Wang, J.-H.; Chiu, C.-J. Efficacy of Myopia Prevention in At-Risk Children: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2025, 14, 1665. https://doi.org/10.3390/jcm14051665
Lee S-H, Tseng B-Y, Wang J-H, Chiu C-J. Efficacy of Myopia Prevention in At-Risk Children: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2025; 14(5):1665. https://doi.org/10.3390/jcm14051665
Chicago/Turabian StyleLee, Ssu-Hsien, Bor-Yuan Tseng, Jen-Hung Wang, and Cheng-Jen Chiu. 2025. "Efficacy of Myopia Prevention in At-Risk Children: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 14, no. 5: 1665. https://doi.org/10.3390/jcm14051665
APA StyleLee, S.-H., Tseng, B.-Y., Wang, J.-H., & Chiu, C.-J. (2025). Efficacy of Myopia Prevention in At-Risk Children: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine, 14(5), 1665. https://doi.org/10.3390/jcm14051665