Transvaginal Ultrasound Findings Predicting Prolonged Pregnancy in Cases of Prolapsed Fetal Membrane: A Retrospective Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
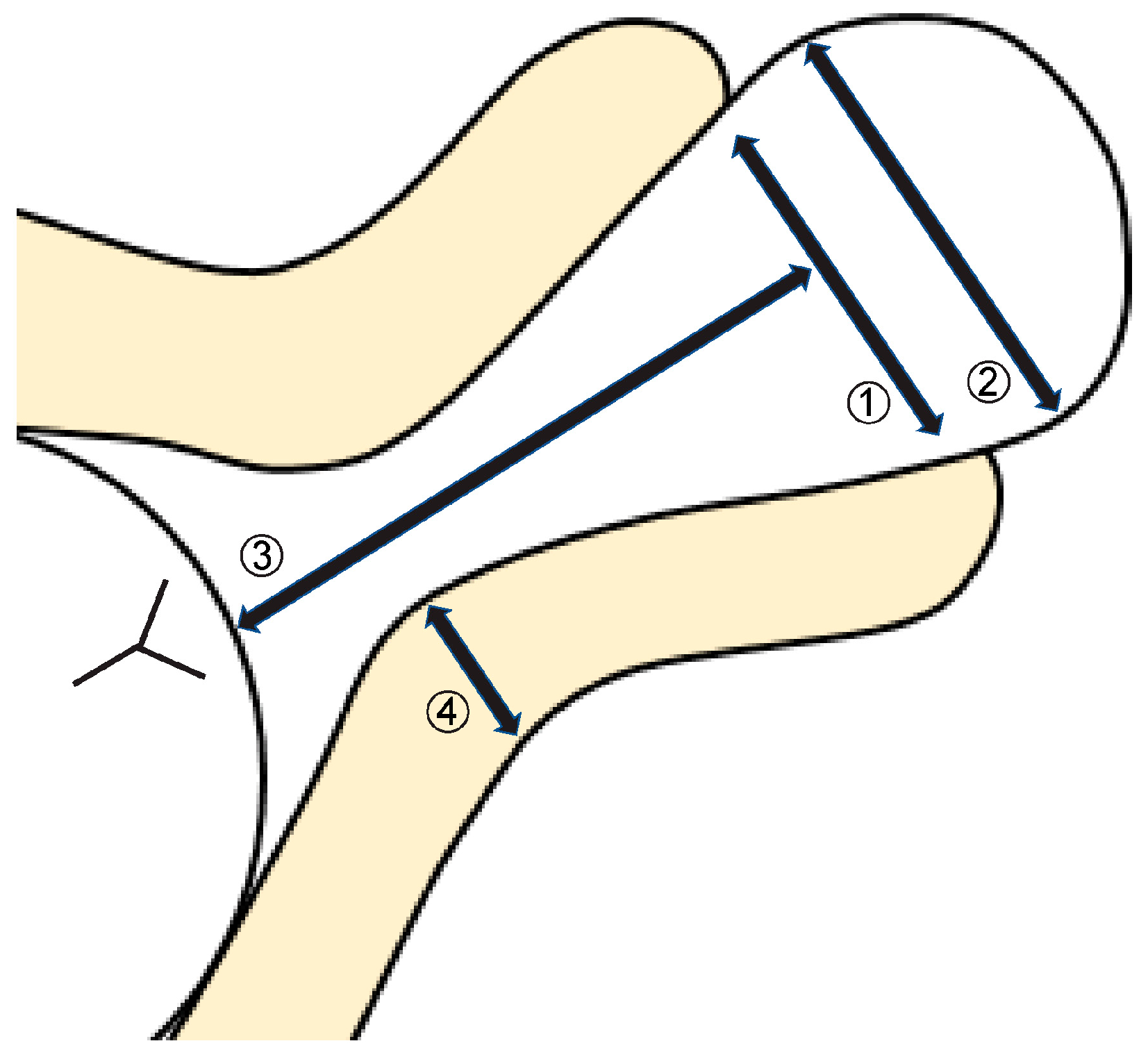
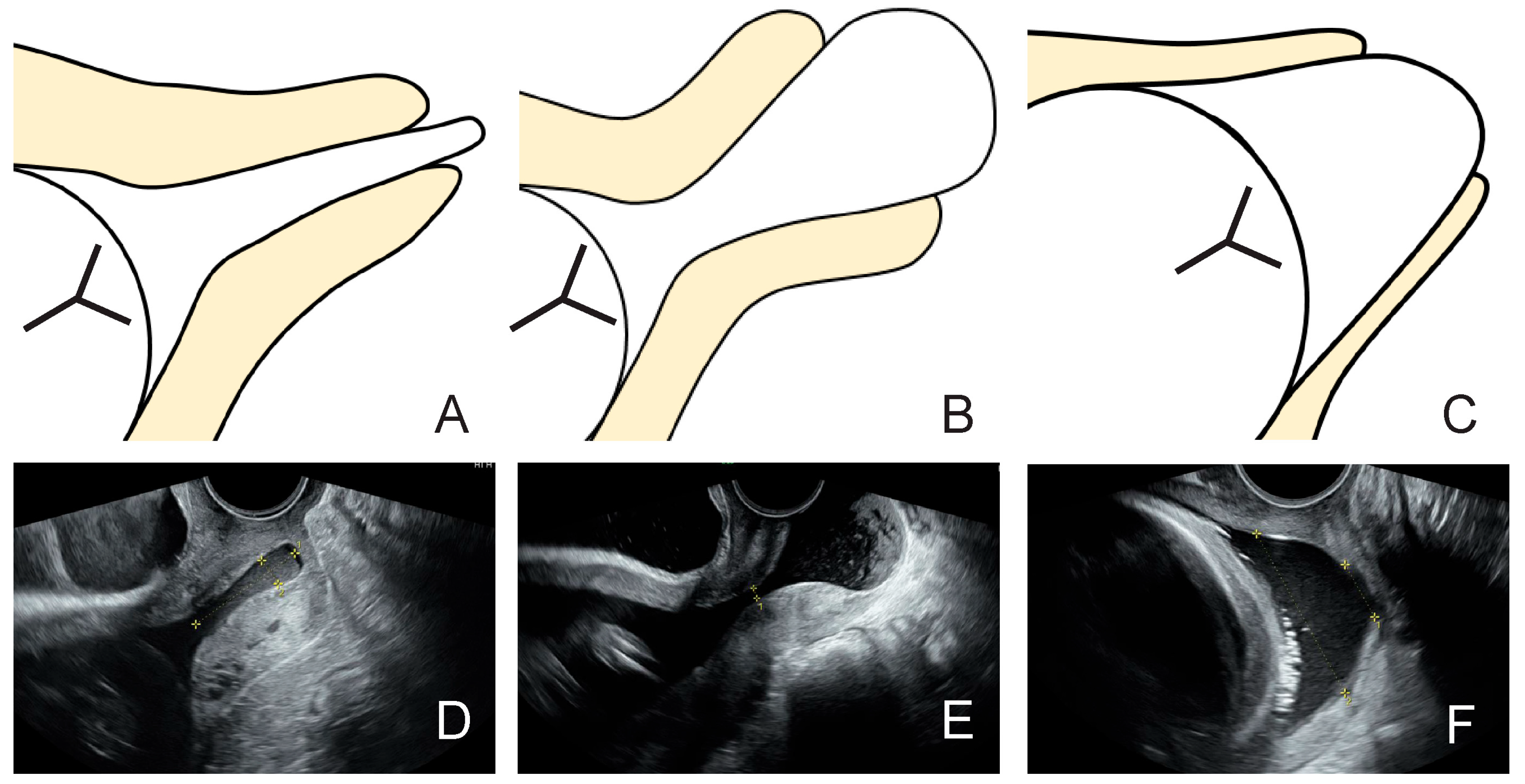
2.2. Ultrasound Findings
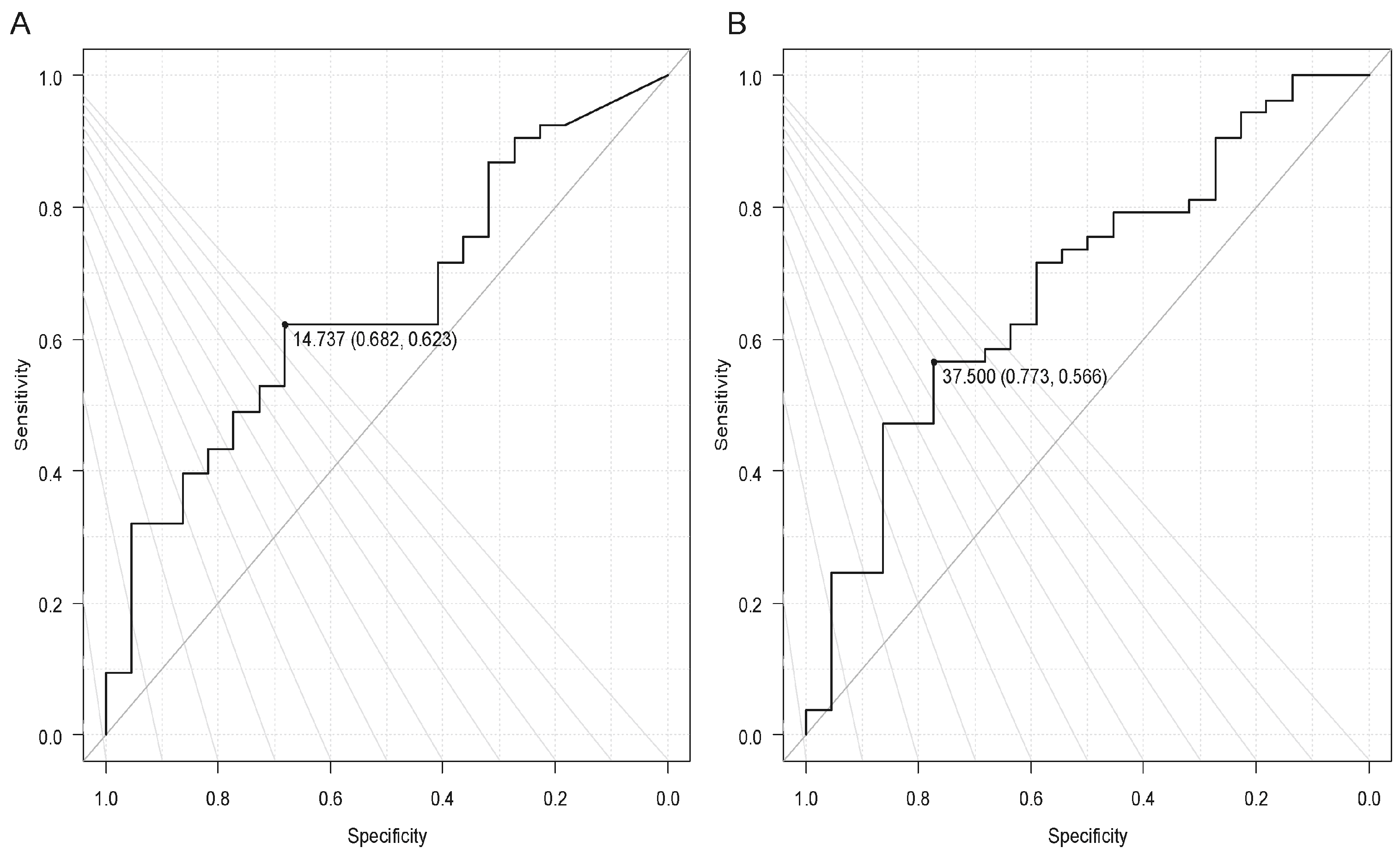
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PROM | Preterm rupture of membrane |
| CI | Confidence interval |
References
- Ocal, A.; Demirci, O.; Ozgokce, C.; Kahramanoglu, O.; Dizdarogullari, G.E.; Eyisoy, O.G.; Yarsilikal Guleroglu, F. Protruding vs. visible prolapsed fetal membranes adversely affects the outcome of cervical insufficiency. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 9937–9946. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No.142: Cerclage for the management of cervical insufficiency. Obstet. Gynecol. 2014, 123, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Granese, R.; Mantegna, S.; Mondello, S.; Amadore, D.; Imbesi, G.; Calagna, G.; Marci, R.; Magro Malosso, E.R.; Triolo, O. Preterm birth: Incidence, risk factors and second trimester cervical length in a single center population. A two-year retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4270–4277. [Google Scholar]
- Robertson, J.E.; Lisonkova, S.; Lee, T.; De Silva, D.A.; von Dadelszen, P.; Synnes, A.R.; Joseph, K.S.; Liston, R.M.; Magee, L.A.; Canadian Perinatal Network and Canadian Neonatal Network Collaborative Groups; et al. Fetal, infant and maternal outcomes among women with prolapsed membranes admitted before 29 weeks gestation. PLoS ONE 2016, 11, e0168285. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Romero, R.; Park, C.W.; Jun, J.K.; Yoon, B.H. The frequency and significance of intraamniotic inflammation in patients with cervical insufficiency. Am. J. Obstet. Gynecol. 2008, 198, 633.e1–633.e8. [Google Scholar] [CrossRef] [PubMed]
- Bujold, E.; Morency, A.M.; Rallu, F.; Ferland, S.; Tétu, A.; Duperron, L.; Audibert, F.; Laferrière, C. Bacteriology of amniotic fluid in women with suspected cervical insufficiency. J. Obstet. Gynaecol. Can. 2008, 30, 882–887. [Google Scholar] [CrossRef]
- Stupin, J.H.; David, M.; Siedentopf, J.P.; Dudenhausen, J.W. Emergency cerclage versus bed rest for amniotic sac prolapse before 27 gestational weeks. A retrospective, comparative study of 161 women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 139, 32–37. [Google Scholar] [CrossRef]
- Debby, A.; Sadan, O.; Glezerman, M.; Golan, A. Favorable outcome following emergency second trimester cerclage. Int. J. Gynaecol. Obstet. 2007, 96, 16–19. [Google Scholar] [CrossRef]
- Aoki, S.; Ohnuma, E.; Kurasawa, K.; Okuda, M.; Takahashi, T.; Hirahara, F. Emergency cerclage versus expectant management for prolapsed fetal membranes: A retrospective, comparative study. J. Obstet. Gynaecol. Res. 2014, 40, 381–386. [Google Scholar] [CrossRef]
- Hulshoff, C.C.; Bosgraaf, R.P.; Spaanderman, M.E.A.; IntHout, J.; Scholten, R.R.; Van Drongelen, J. The efficacy of emergency cervical cerclage in singleton and twin pregnancies: A systematic review with meta-analysis. Am. J. Obstet. Gynecol. MFM 2023, 5, 100971. [Google Scholar] [CrossRef]
- Althuisius, S.M.; Dekker, G.A.; Hummel, P.; van Geijn, H.P.; Cervical incompetence prevention randomized cerclage trial. Cervical incompetence prevention randomized cerclage trial: Emergency cerclage with bed rest versus bed rest alone. Am. J. Obstet. Gynecol. 2003, 189, 907–910. [Google Scholar] [CrossRef] [PubMed]
- Harger, J.H. Cerclage and cervical insufficiency: An evidence-based analysis. Obstet. Gynecol. 2002, 100, 1313–1327. [Google Scholar] [CrossRef] [PubMed]
- Simcox, R.; Shennan, A. Cervical cerclage in the prevention of preterm birth. Best. Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 831–842. [Google Scholar] [CrossRef]
- Bishop, E.H. Pelvic scoring for elective induction. Obstet. Gynecol. 1964, 24, 266–268. [Google Scholar]
- van Dijk, C.E.; Breuking, S.H.; Jansen, S.; Limpens, J.C.E.J.M.; Kazemier, B.M.; Pajkrt, E. Perioperative complications of a transvaginal cervical cerclage in singleton pregnancies: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2023, 228, 521–534.e19. [Google Scholar] [CrossRef]
- Scheerer, L.J.; Lam, F.; Bartolucci, L.; Katz, M. A new technique for reduction of prolapsed fetal membranes for emergency cervical cerclage. Obstet. Gynecol. 1989, 74, 408–410. [Google Scholar]
- Kanai, M.; Ashida, T.; Ohira, S.; Osada, R.; Konishi, I. A new technique using a rubber balloon in emergency second trimester cerclage for fetal membrane prolapse. J. Obstet. Gynaecol. Res. 2008, 34, 935–940. [Google Scholar] [CrossRef]
- Locatelli, A.; Vergani, P.; Bellini, P.; Strobelt, N.; Arreghini, A.; Ghidini, A. Amnioreduction in emergency cerclage with prolapsed membranes: Comparison of two methods for reducing the membranes. Am. J. Perinatol. 1999, 16, 73–77. [Google Scholar] [CrossRef]
- Fuchs, F.; Bouyer, J.; Fernandez, H.; Gervaise, A.; Frydman, R.; Senat, M.V. Ultrasound cervical length measurement for prediction of delivery before 32 weeks in women with emergency cerclage for cervical insufficiency. Int. J. Gynaecol. Obstet. 2010, 110, 245–248. [Google Scholar] [CrossRef]
- Roman, A.; Gulersen, M.; Boelig, R.C.; Berghella, V. Proposed staging criteria for sonographic and physical exam for cervical changes at <24 weeks gestation to predict preterm birth. Am. J. Obstet. Gynecol. MFM 2023, 5, 100753. [Google Scholar] [CrossRef]
- Park, J.Y.; Oh, K.J.; Lee, S.; Kim, N.K.; Lee, Y.E.; Park, Y.H.; Hong, J.S. A new quantification system for assessing the degree of acute cervical insufficiency based on physical and sonographic examination. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Zilianti, M.; Azuaga, A.; Calderon, F.; Pagés, G.; Mendoza, G. Monitoring the effacement of the uterine cervix by transperineal sonography: A new perspective. J. Ultrasound Med. 1995, 14, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Aubin, A.M.; McAuliffe, L.; Williams, K.; Issah, A.; Diacci, R.; McAuliffe, J.E.; Sabdia, S.; Phung, J.; Wang, C.A.; Pennell, C.E. Combined vaginal progesterone and cervical cerclage in the prevention of preterm birth: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2023, 5, 101024. [Google Scholar] [CrossRef] [PubMed]
- Tolosa, J.E.; Boelig, R.C.; Bell, J.; Martínez-Baladejo, M.; Stoltzfus, J.; Mateus, J.; Quiñones, J.N.; Galeano-Herrera, S.; Pereira, L.; Burwick, R.; et al. Concurrent progestogen and cerclage to reduce preterm birth: A multicenter international retrospective cohort. Am. J. Obstet. Gynecol. MFM 2024, 6, 101351. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Adjusted OR | 95% CI | p-Value | |
|---|---|---|---|
| Body mass index | 0.623 | −0.16–1.41 | 0.117 |
| Nulliparity | 2.399 | 1.36–6.67 | 0.007 |
| Natural pregnancy | 1.050 | −8.92–11.02 | 0.834 |
| History of preterm birth | 7.727 | −7.55–23.0 | 0.316 |
| Width of external os | −0.167 | −0.41–0.07 | 0.166 |
| Width of prolapsed membrane | −0.024 | −0.28–0.23 | 0.853 |
| Distance between external os and baby | 0.173 | −0.08–0.43 | 0.173 |
| Thickness of posterior uterine lip | −0.053 | −1.13–1.02 | 0.921 |
| Gestational weeks at admission | 0.080 | −0.07–0.23 | 0.298 |
| Type of prolapsed fetal membrane | |||
| B comparing with A | −17.469 | −31.5–−3.47 | 0.0153 |
| C comparing with A | −15.369 | −28.11–−2.63 | 0.019 |
| Delivery < 7 Days (n = 53) | Delivery > 7 Days (n = 22) | p-Value | |
|---|---|---|---|
| Width of external os (mm) | 19.9 (0–93.5) | 13.3 (0–51.7) | 0.040 |
| Width of prolapsed fetal membrane (mm) | 38.2 (6.6–93.5) | 27.0 (0–86.1) | 0.013 |
| Distance from external os to baby (mm) | 15.7 (0–68.2) | 24.4 (2.43–60.6) | 0.067 |
| Thickness of the posterior lip (mm) | 8.50 (0–23.1) | 6.74 (0.75–14.6) | 0.093 |
| Type of prolapsed fetal membrane | 0.037 | ||
| A | 3/9 (33.3%) | 6/9 (66.7%) | |
| B | 32/41 (78.0%) | 9/41 (22.0%) | |
| C | 18/25 (72%) | 7/25 (28%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondo, T.; Tsuda, H.; Tsugeno, E.; Nakamura, Y.; Ito, Y.; Tezuka, A.; Ando, T. Transvaginal Ultrasound Findings Predicting Prolonged Pregnancy in Cases of Prolapsed Fetal Membrane: A Retrospective Study. J. Clin. Med. 2025, 14, 1592. https://doi.org/10.3390/jcm14051592
Kondo T, Tsuda H, Tsugeno E, Nakamura Y, Ito Y, Tezuka A, Ando T. Transvaginal Ultrasound Findings Predicting Prolonged Pregnancy in Cases of Prolapsed Fetal Membrane: A Retrospective Study. Journal of Clinical Medicine. 2025; 14(5):1592. https://doi.org/10.3390/jcm14051592
Chicago/Turabian StyleKondo, Tomohiro, Hiroyuki Tsuda, Eri Tsugeno, Yumi Nakamura, Yumiko Ito, Atsuko Tezuka, and Tomoko Ando. 2025. "Transvaginal Ultrasound Findings Predicting Prolonged Pregnancy in Cases of Prolapsed Fetal Membrane: A Retrospective Study" Journal of Clinical Medicine 14, no. 5: 1592. https://doi.org/10.3390/jcm14051592
APA StyleKondo, T., Tsuda, H., Tsugeno, E., Nakamura, Y., Ito, Y., Tezuka, A., & Ando, T. (2025). Transvaginal Ultrasound Findings Predicting Prolonged Pregnancy in Cases of Prolapsed Fetal Membrane: A Retrospective Study. Journal of Clinical Medicine, 14(5), 1592. https://doi.org/10.3390/jcm14051592