
Could Renal Vascular Variations Be Associated with Resistant Hypertension? A Single-Center Study


Abstract
1. Introduction
2. Materials and Methods
- Individuals aged 18 years or older;
- Office systolic blood pressure (SBP) ≥ 140 mmHg and/or office diastolic blood pressure (DBP) ≥ 90 mmHg persisting despite ≥1 month of therapy with either optimal or maximum-tolerated doses of at least three medications, including a renin–angiotensin–aldosterone system (RAAS) inhibitor, a calcium channel blocker (CCB), and a thiazide/thiazide-like diuretic;
- The verification of poorly controlled blood pressure through 24 h ambulatory blood pressure monitoring (ABPM);
- Evidence of patient compliance with treatment regimens, achieving ≥80% adherence during the prescribed period.
- Achieved target BP levels with fewer than three antihypertensive drugs;
- Maintenance of SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg despite treatment with ≥3 drugs but not at optimal doses or/and not including the combination of RAAS blockers + CCB + thiazide/thiazide-like diuretic, or with a treatment duration of <1 month;
- Documented cases of secondary hypertension resulting from renal artery involvement (atherosclerotic, fibromuscular, or vasculitic), renal parenchymal disease, or other underlying endocrinological, metabolic, cardiovascular, or related conditions;
- Presence of clinical conditions and/or comorbidities that rendered the planned instrumental investigations impractical.
- Office SBP between 120 and 129 mmHg;
- Office DBP between 70 and 79 mmHg;
- Mean 24 h ABPM < 130 mmHg for SBP and <80 mmHg for DBP;
- Mean daytime ABPM < 135 mmHg for SBP and <85 mmHg for DBP;
- Mean nighttime ABPM < 120 mmHg for SBP and <70 mmHg for DBP;
- Blood pressure control was achieved using ≤3 drugs from different classes.
Statistical Analysis
3. Results
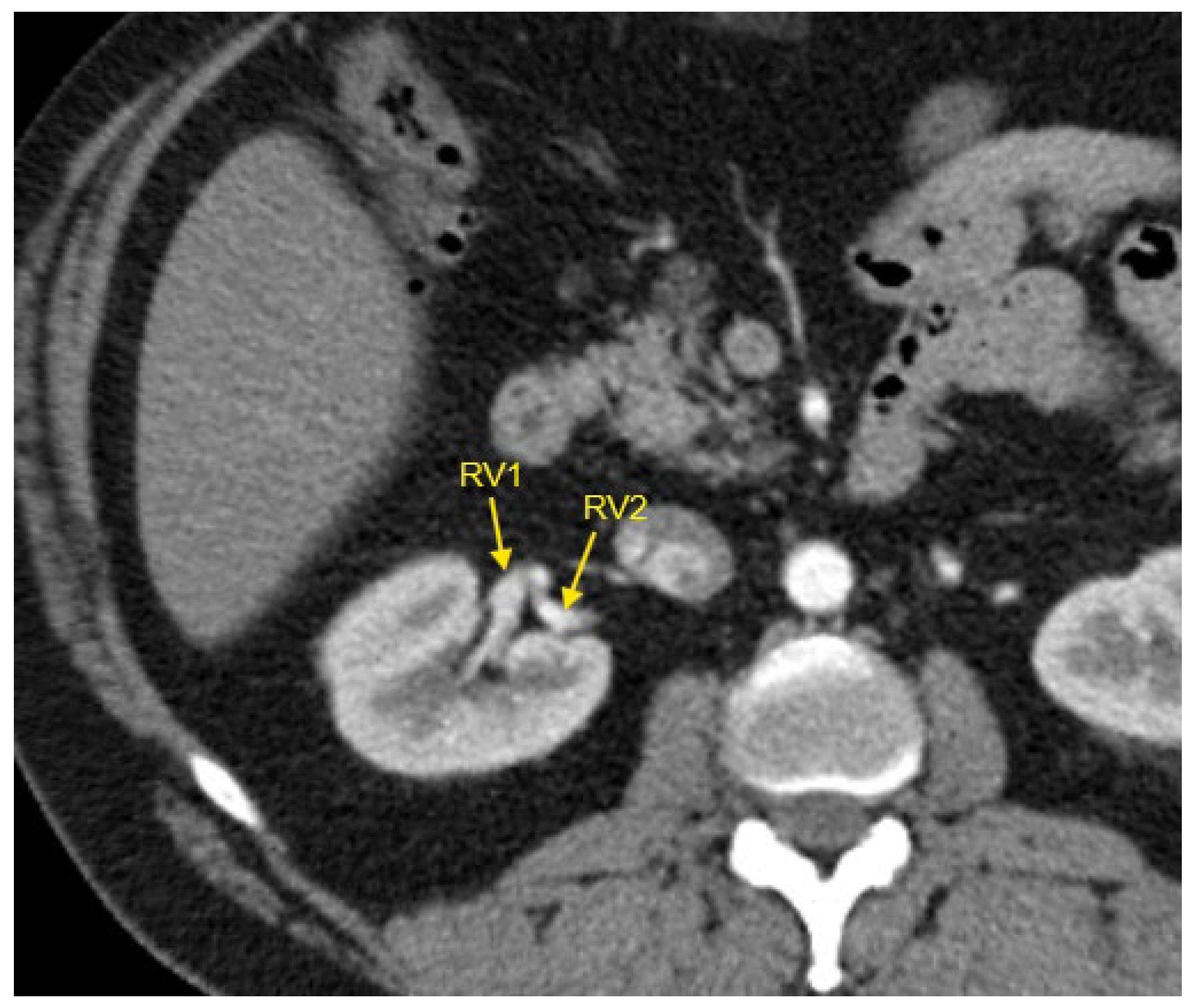
3.1. Renal Vascular Characteristics
3.2. Demographic and Clinical Characteristics
3.3. Laboratory Investigations
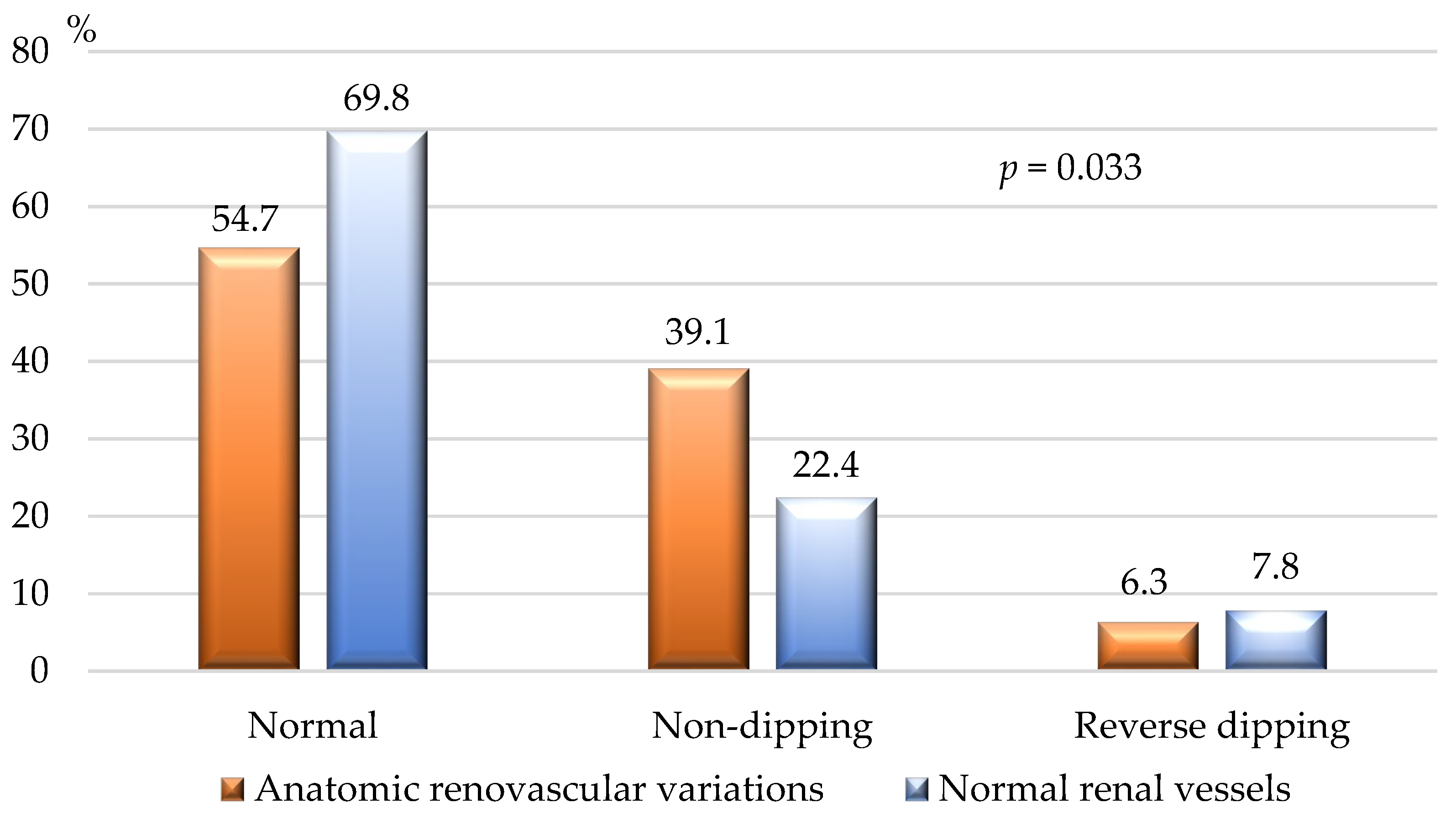
3.4. BP Measurement
3.5. Impact of Congenital Renal Vascular Variations on HTN Control
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- García-Barrios, A.; Cisneros-Gimeno, A.I.; Celma-Pitarch, A.; Whyte-Orozco, J. Anatomical Study about the Variations in Renal Vasculature. Folia Morphol. 2023, 83, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Aristotle, S. Anatomical Study of Variations in the Blood Supply of Kidneys. JCDR 2013, 7, 1555. [Google Scholar] [CrossRef]
- Khamanarong, K.; Prachaney, P.; Utraravichien, A.; Tong-Un, T.; Sripaoraya, K. Anatomy of Renal Arterial Supply. Clinical Anatomy 2004, 17, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Gulas, E.; Wysiadecki, G.; Szymański, J.; Majos, A.; Stefańczyk, L.; Topol, M.; Polguj, M. Morphological and Clinical Aspects of the Occurrence of Accessory (Multiple) Renal Arteries. Aoms 2018, 14, 442–453. [Google Scholar] [CrossRef] [PubMed]
- Urban, B.A.; Ratner, L.E.; Fishman, E.K. Three-Dimensional Volume-Rendered CT Angiography of the Renal Arteries and Veins: Normal Anatomy, Variants, and Clinical Applications. Radiographics 2001, 21, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Gulas, E.; Wysiadecki, G.; Cecot, T.; Majos, A.; Stefańczyk, L.; Topol, M.; Polguj, M. Accessory (Multiple) Renal Arteries–Differences in Frequency According to Population, Visualizing Techniques and Stage of Morphological Development. Vascular 2016, 24, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Satyapal, K.S.; Haffejee, A.A.; Singh, B.; Ramsaroop, L.; Robbs, J.V.; Kalideen, J.M. Additional Renal Arteries Incidence and Morphometry. Surg. Radiol. Anat. 2001, 23, 33–38. [Google Scholar] [CrossRef]
- Aremu, A.; Igbokwe, M.; Olatise, O.; Lawal, A.; Maduadi, K. Anatomical Variations of the Renal Artery: A Computerized Tomographic Angiogram Study in Living Kidney Donors at a Nigerian Kidney Transplant Center. Afr. Health Sci. 2021, 21, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Hostiuc, S.; Rusu, M.C.; Negoi, I.; Dorobanțu, B.; Grigoriu, M. Anatomical Variants of Renal Veins: A Meta-Analysis of Prevalence. Sci. Rep. 2019, 9, 10802. [Google Scholar] [CrossRef]
- Valenzuela Fuenzalida, J.J.; Vera-Tapia, K.; Urzúa-Márquez, C.; Yáñez-Castillo, J.; Trujillo-Riveros, M.; Koscina, Z.; Orellana-Donoso, M.; Nova-Baeza, P.; Suazo-Santibañez, A.; Sanchis-Gimeno, J.; et al. Anatomical Variants of the Renal Veins and Their Relationship with Morphofunctional Alterations of the Kidney: A Systematic Review and Meta-Analysis of Prevalence. JCM 2024, 13, 3689. [Google Scholar] [CrossRef]
- Kasprzycki, K.; Petkow-Dimitrow, P.; Krawczyk-Ożóg, A.; Bartuś, S.; Rajtar-Salwa, R. Anatomic Variations of Renal Arteries as an Important Factor in the Effectiveness of Renal Denervation in Resistant Hypertension. JCDD 2023, 10, 371. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, A.T.A. Renal Artery Variations Clinical Significance and Implications. Int. J. Anat. Var. 2024, 17, 675–676. [Google Scholar]
- Sanghvi, K.; Wang, Y.; Daemen, J.; Mathur, A.; Jain, A.; Dohad, S.; Sapoval, M.; Azizi, M.; Mahfoud, F.; Lurz, P.; et al. Renal Artery Variations in Patients with Mild-to-Moderate Hypertension From the RADIANCE-HTN SOLO Trial. Cardiovasc. Revasc. Med. 2022, 39, 58–65. [Google Scholar] [CrossRef]
- Mancia, G.; Kreutz, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the Management of Arterial Hypertension The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, J.W.; McCarthy, C.P.; Bruno, R.M.; Brouwers, S.; Canavan, M.D.; Ceconi, C.; Christodorescu, R.M.; Daskalopoulou, S.S.; Ferro, C.J.; Gerdts, E.; et al. 2024 ESC Guidelines for the Management of Elevated Blood Pressure and Hypertension. Eur. Heart J. 2024, 45, 3912–4018. [Google Scholar] [CrossRef] [PubMed]
- Charles, K.; Lewis, M.J.; Montgomery, E.; Reid, M. The 2021 Chronic Kidney Disease Epidemiology Collaboration Race-Free Estimated Glomerular Filtration Rate Equations in Kidney Disease: Leading the Way in Ending Disparities. Health Equity 2024, 8, 39–45. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Kurklinsky, A.K.; Rooke, T.W. Nutcracker Phenomenon and Nutcracker Syndrome. Mayo Clin. Proc. 2010, 85, 552–559. [Google Scholar] [CrossRef]
- Rao, M.; Bhat, S.M.; Venkataramana, V.; Deepthinath, R.; Bolla, S.R. Bilateral Prehilar Multiple Branching of Renal Arteries: A Case Report and Literature Review. Kathmandu Univ. Med. J. (KUMJ) 2006, 4, 345–348. [Google Scholar] [PubMed]
- Cho, Y.; Yoon, S.-P. Bilateral Inferior Renal Polar Arteries with a High Origin from the Abdominal Aorta. Folia Morphol. 2021, 80, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, U.; Oğuzkurt, L.; Tercan, F.; Kizilkiliç, O.; Koç, Z.; Koca, N. Renal Artery Origins and Variations: Angiographic Evaluation of 855 Consecutive Patients. Diagn. Interv. Radiol. 2006, 12, 183–186. [Google Scholar] [PubMed]
- Ugurel, M.S.; Battal, B.; Bozlar, U.; Nural, M.S.; Tasar, M.; Ors, F.; Saglam, M.; Karademir, I. Anatomical Variations of Hepatic Arterial System, Coeliac Trunk and Renal Arteries: An Analysis with Multidetector CT Angiography. BJR 2010, 83, 661–667. [Google Scholar] [CrossRef]
- Chobanian, A.V. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureThe JNC 7 Report. JAMA 2003, 289, 2560. [Google Scholar] [CrossRef] [PubMed]
- Dudenbostel, T.; Acelajado, M.C.; Pisoni, R.; Li, P.; Oparil, S.; Calhoun, D.A. Refractory Hypertension: Evidence of Heightened Sympathetic Activity as a Cause of Antihypertensive Treatment Failure. Hypertension 2015, 66, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A.; Jhamb, R. Resistant Hypertension: A Review. Int. J. Adv. Med. 2021, 8, 1433. [Google Scholar] [CrossRef]
- Cai, A.; Calhoun, D.A. Resistant Hypertension: An Update of Experimental and Clinical Findings. Hypertension 2017, 70, 5–9. [Google Scholar] [CrossRef]
- Piani, F.; Tossetta, G.; Cara-Fuentes, G.; Agnoletti, D.; Marzioni, D.; Borghi, C. Diagnostic and Prognostic Role of CD93 in Cardiovascular Disease: A Systematic Review. Biomolecules 2023, 13, 910. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Singh, V.; Kaur, R.; Kumari, P.; Pasricha, C.; Singh, R. ICAM-1 and VCAM-1: Gatekeepers in various inflammatory and cardiovascular disorders. Clin. Chim. Acta 2023, 548, 117487. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anatomical Renal Vascular Variations | Total n = 256 | Controlled HTN n = 128 | Resistant HTN n = 128 | p |
|---|---|---|---|---|
| Normal anatomy, n (%) | 192 (75.0%) | 113 (88.3%) | 79 (61.7%) | 0.005 |
| Accessory right-sided renal artery, n (%) | 16 (6.3%) | 4 (3.1%) | 12 (9.4%) | 0.04 |
| Accessory left-sided renal artery, n (%) | 18 (7.0%) | 4 (3.1%) | 14 (11%) | 0.04 |
| Accessory renal artery of both kidneys, n (%) | 4 (1.6%) | 1 (0.8%) | 3 (2.4%) | 0.321 |
| Accessory renal artery of the right kidney + 2 renal veins of the right kidney, n (%) | 4 (1.6%) | 2 (1.6%) | 2 (1.6%) | 1.000 |
| Accessory renal artery of both kidneys + 2 renal veins of the right kidney, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Accessory renal vein of the right kidney, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Nutcracker syndrome—left-sided, n (%) | 4 (1.6%) | 1 (0.8%) | 3 (2.3%) | 0.321 |
| Nutcracker syndrome—right-sided, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Accessory and aberrant right renal arteries + accessory left renal artery + left-sided Nutcracker syndrome, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Left-sided double kidney with separate renal arteries, veins and ureters, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Aberrant lower-pole artery of the right kidney + right main renal artery stenosis, n (%) | 2 (0.8%) | 1 (0.8%) | 1 (0.8%) | 1.000 |
| Accessory right-sided renal artery + left renal vein stenosis, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Accessory left renal artery + right main renal artery stenosis + 2 renal veins and double draining system of the right kidney, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Accessory renal vein of the right kidney + calcification of the ostia of both renal arteries, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Double right kidney + accessory lower-pole right renal artery, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Early bifurcation of the right renal artery, n (%) | 2 (0.8%) | 1 (0.8%) | 1 (0.8%) | 1.000 |
| Multiple aneurisms of the right renal artery, n (%) | 1 (0.4%) | 0 (0%) | 1 (0.8%) | 0.318 |
| Retroaortic left renal vein, n (%) | 2 (0.8%) | 0 (0%) | 2 (1.6%) | 0.159 |
| Trifurcation of right renal artery with early separation of the branches, n (%) | 2 (0.8%) | 1 (0.8%) | 1 (0.8%) | 1.000 |
| Total n = 256 | Renal Vascular Variations n = 64 | Normal Renal Vasculature n = 192 | p | |
|---|---|---|---|---|
| Age (years), median (IQR) | 61.0 (51.0–69.0) | 54.0 (46.0–65.8) | 63.0 (54.0–71.0) | <0.001 |
| Gender, n (%) | ||||
| Males | 130 (50.8%) | 32 (50%) | 98 (51.0%) | 0.886 # |
| Females | 126 (49.2%) | 32 (50%) | 94 (49.0%) | |
| Resistant HTN, n (%) | 64 (25.0%) | 49 (76.6%) | 79 (41.1%) | <0.001 |
| HTN grade, n (%) | ||||
| Mild | 74 (28.9%) | 3 (4.7%) | 71 (37.0%) | <0.001 # |
| Moderate | 88 (34.4%) | 23 (35.9%) | 65 (33.9%) | |
| Severe | 94 (36.7%) | 38 (59.4%) | 56 (29.2%) | |
| HTN stage, n (%) | ||||
| 1st stage | 79 (30.9%) | 22 (34.4%) | 57 (29.7%) | 0.780 # |
| 2nd stage | 109 (40.6%) | 26 (40.6%) | 83 (43.2%) | |
| 3rd stage | 68 (26.6%) | 16 (25.0%) | 52 (27.1%) | |
| CKD, n (%) | 126 (49.2%) | 32 (50.0%) | 94 (49.0%) | 0.585 |
| Overweight/obesity, n (%) | 105 (41.0%) | 28 (43.8%) | 77 (40.1%) | 0.320 |
| Dyslipidemia, n (%) | 81 (31.6%) | 18 (28.1%) | 63 (32.8%) | 0.296 |
| Type 2 diabetes, n (%) | 38 (14.8%) | 10 (15.6%) | 28 (14.6%) | 0.272 |
| Ischemic heart disease, n (%) | 31 (12.1%) | 7 (10.9%) | 24 (12.5%) | 0.467 |
| Post-stroke, n (%) | 11 (4.3%) | 2 (3.1%) | 9 (4.7%) | 0.516 |
| PAD, n (%) | 11 (5.5%) | 3 (6.4%) | 8 (5.3%) | 0.723 |
| Heart failure, n (%) | 38 (14.8%) | 7 (10.9%) | 31 (16.1%) | 0.326 |
| Smoking, n (%) | ||||
| Active | 53 (20.7%) | 28 (43.8%) | 25 (13.0%) | <0.001 # |
| Ex-smoker | 16 (6.3%) | 4 (6.3%) | 12 (6.3%) | |
| Alcohol consumption * | 33 (12.9%) | 12 (18.8%) | 21 (10.9%) | 0.131 |
| Parameter | Total n = 256 | Renal Vascular Variations n = 64 | Normal Renal Vasculature n = 192 | p |
|---|---|---|---|---|
| Potassium, mmol/L, median (IQR) | 4.6 (4.2–4.9) | 4.7 (4.3–4.9) | 4.6 (4.5–4.9) | 0.007 |
| Sodium, mmol/L, median (IQR) | 142 (139–145) | 141 (138–145) | 142 (139–145) | 0.286 |
| Hemoglobin, g/L, median (IQR) | 148 (136–158) | 147 (134–160) | 148 (137–157) | 0.944 |
| Hematocrit, L/L, median (IQR) | 0.44 (0.42–0.46) | 0.45 (0.41–0.47) | 0.44 (0.42–0.46) | 0.353 |
| Fasting glucose, mmol/L, median (IQR) | 5.3 (4.8–6.2) | 5.2 (4.8–6.1) | 5.4 (4.9–6.2) | 0.361 |
| Creatinine, µmol/L, median (IQR) | 76 (66–92) | 77 (68–91) | 76 (66–92) | 0.960 |
| eGFR, mL/min/1.73 m2, median (IQR) | 92 (75–101) | 95 (76–105) | 92 (73–100) | 0.129 |
| Characteristics | Total n = 256 | Renovascular Variations n = 64 | Normal Renal Vasculature n = 192 | p |
|---|---|---|---|---|
| Office SBP (mm Hg), median (IQR) | 139.0 (130.0–150.0) | 147.0 (138.5–160.0) | 135.5 (130.0–150.0) | <0.001 |
| Office DBP (in mm Hg), median (IQR) | 85.0 (80.0–90.0) | 90.0 (83.5.0–95.0) | 85.0 (80.0–90.0) | <0.001 |
| Pulse pressure (in mm Hg), median (IQR) | 51.0 (50.0–60.0) | 52.0 (50.0–65.0) | 51.0 (48.0–60.0) | 0.062 |
| Daytime ABPM SBP (in mm Hg), median (IQR) | 134.0 (128.5–145.0) | 142.0 (135.0–149.0) | 133.0 (126.5–142.0) | <0.001 |
| Daytime ABPM DBP (in mm Hg), median (IQR) | 84.0 (78.0–90.0) | 89.0 (82.5–94.0) | 83.0 (76.0–90.0) | <0.001 |
| Nighttime ABPM SBP (in mm Hg), median (IQR) | 123.0 (115.0–137.0) | 131.0 (124.0–142.0) | 119.0 (115.0–134.0) | <0.001 |
| Nighttime ABPM DBP (in mm Hg), median (IQR) | 74.0 (65.0–85.5) | 82.0 (73.5–90.0) | 69.0 (65.0–82.5) | <0.001 |
| 24 h ABPM SBP (in mm Hg), median (IQR) | 132.0 (122.0–141.0) | 139.0 (132.0–145.5) | 127.0 (121.0–139.0) | <0.001 |
| 24 h ABPM DBP (in mm Hg), median (IQR) | 79.0 (71.0–88.0) | 85.0 (78.0–92.0) | 77.0 (70.0–87.0) | <0.001 |
| Heart rate (beats/min.), median (IQR) | 74 (67–80) | 75 (70–85.0) | 74 (67.0–80.0) | 0.402 |
| Variable | OR | 95% CI for OR | ||
|---|---|---|---|---|
| Lower Limit | Upper Limit | p | ||
| Overall renal vascular variation(s) | 4.673 | 2.449 | 8.913 | <0.001 |
| Accessory renal artery(ies) | 6.373 | 2.744 | 14.799 | <0.001 |
| Accessory renal vein(s) | 6.153 | 1.240 | 12.541 | 0.026 |
| Normal renal vessels | 0.214 | 0.112 | 0.408 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naydenov, S.; Jekova, M.; Manov, E.; Runev, N. Could Renal Vascular Variations Be Associated with Resistant Hypertension? A Single-Center Study. J. Clin. Med. 2025, 14, 1268. https://doi.org/10.3390/jcm14041268
Naydenov S, Jekova M, Manov E, Runev N. Could Renal Vascular Variations Be Associated with Resistant Hypertension? A Single-Center Study. Journal of Clinical Medicine. 2025; 14(4):1268. https://doi.org/10.3390/jcm14041268
Chicago/Turabian StyleNaydenov, Stefan, Margarita Jekova, Emil Manov, and Nikolay Runev. 2025. "Could Renal Vascular Variations Be Associated with Resistant Hypertension? A Single-Center Study" Journal of Clinical Medicine 14, no. 4: 1268. https://doi.org/10.3390/jcm14041268
APA StyleNaydenov, S., Jekova, M., Manov, E., & Runev, N. (2025). Could Renal Vascular Variations Be Associated with Resistant Hypertension? A Single-Center Study. Journal of Clinical Medicine, 14(4), 1268. https://doi.org/10.3390/jcm14041268