
Quality Assurance of a Hospital-Based Auditory Verbal Intervention for Children with Hearing Loss


 ,
, 

Abstract
1. Introduction
1.1. Rehabilitation
1.2. AVT in Denmark
The AVT-Project
1.3. Aim
- Which precursors are crucial for the successful implementation of AV intervention in a hospital setting?
- What is the behavioural and emotional status of children with HL who have participated in the three-year AV intervention in a hospital setting?
2. Materials and Methods
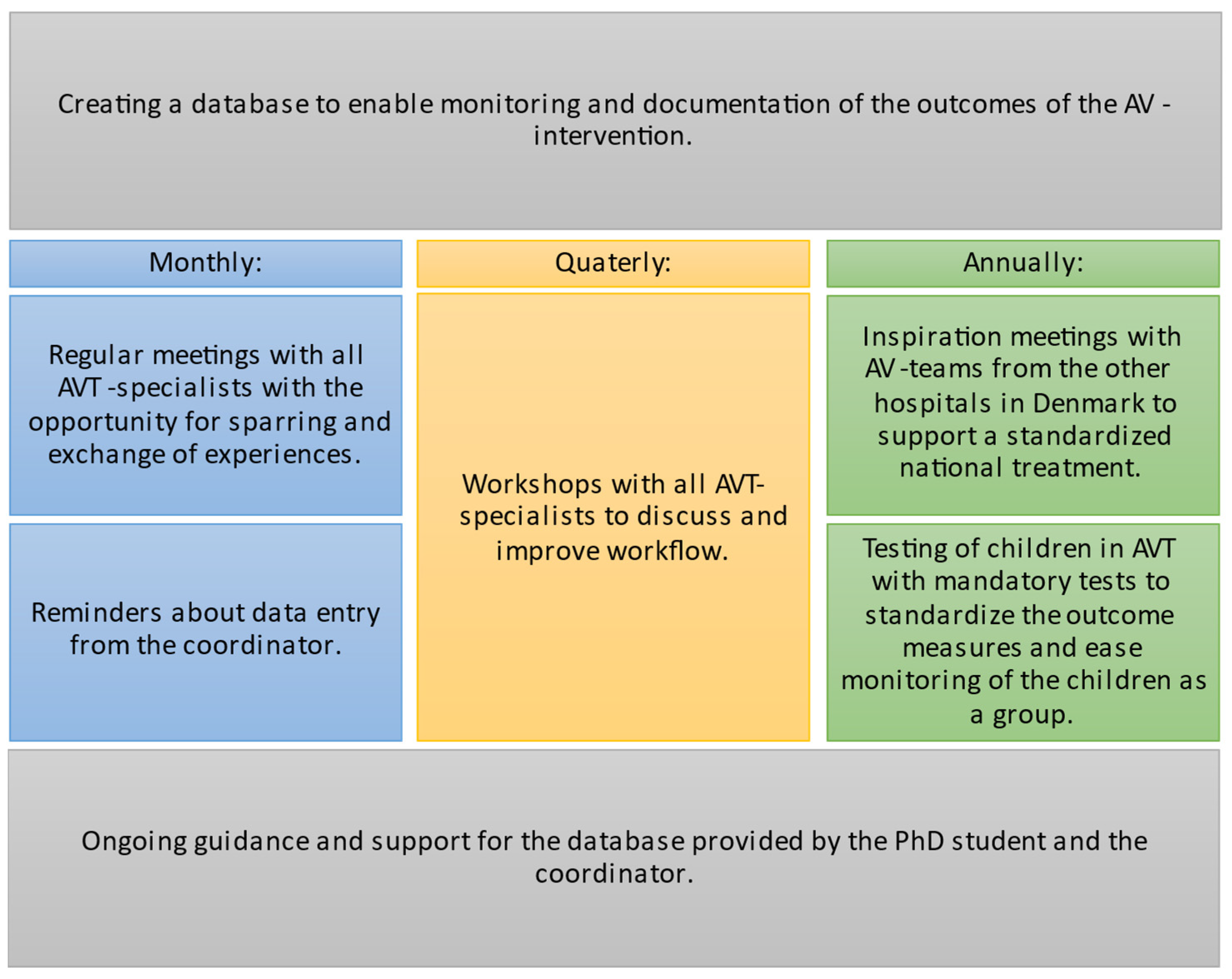
2.1. Procedure for Long-Term Implementation of AVT in a Hospital Setting
2.2. Quality Assurance of the AV Intervention
2.2.1. Mandatory Tests
Auditory Skills
Receptive Vocabulary
Behavioural and Emotional Status
2.2.2. Database
2.3. Social Well-Being
2.4. Data Analysis
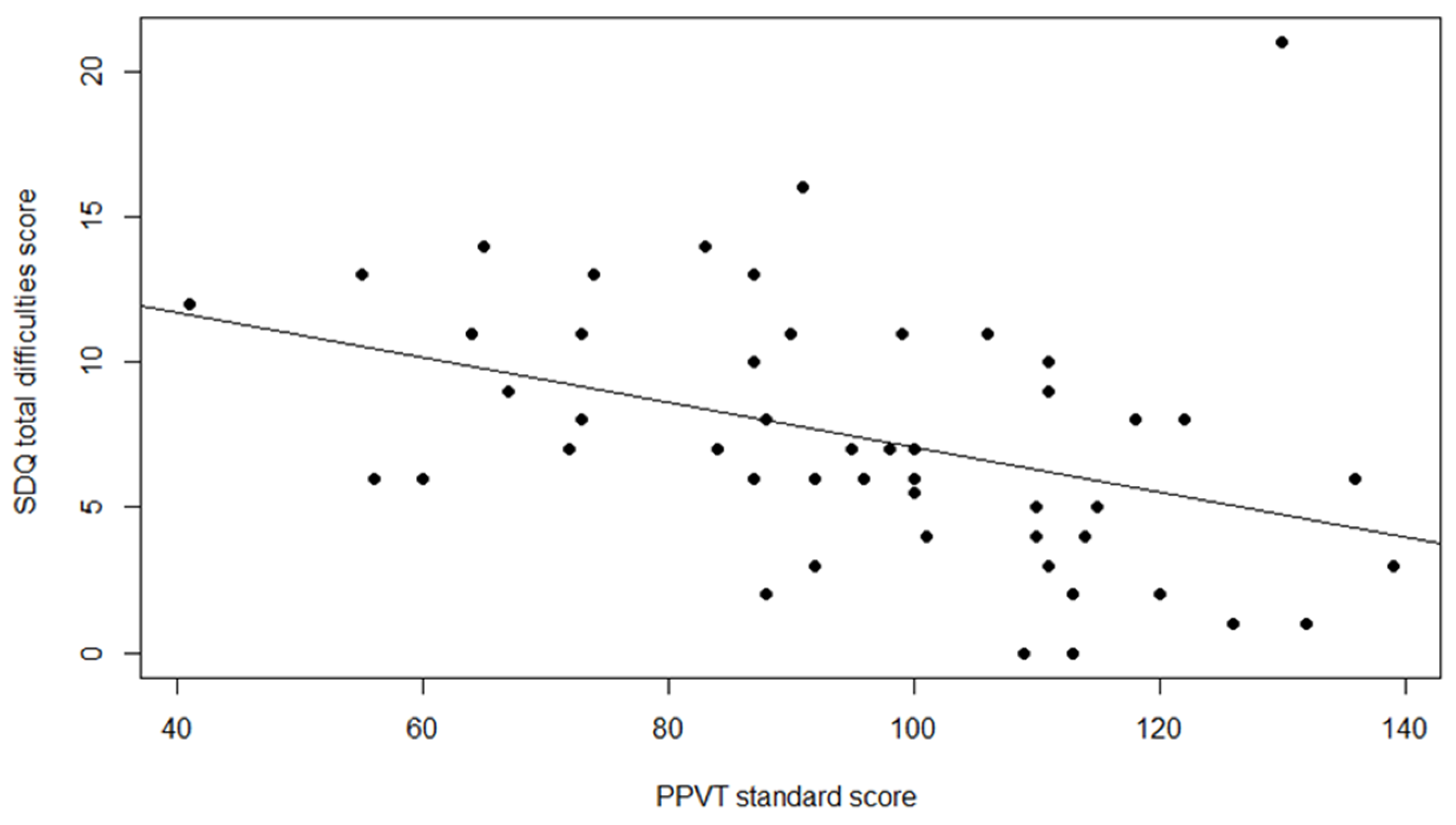
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maniaci, A.; La Via, L.; Lechien, J.R.; Sangiorgio, G.; Iannella, G.; Magliulo, G.; Pace, A.; Mat, Q.; Lavalle, S.; Lentini, M. Hearing Loss and Oxidative Stress: A Comprehensive Review. Antioxidants 2024, 13, 842. [Google Scholar] [CrossRef]
- Hammer, L.; Kamper, N.R.; Jantzen, L.; Serafin, S.; Percy-Smith, L. Self-Reported Social Well-Being of Children with Hearing Loss in 2023. Cochlear Implant. Int. 2024, 25, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Wischmann, S.; Josvassen, J.L.; Schiøth, C.; Percy-Smith, L. History Re-Written for Children with Hearing Impairment. Int. J. Pediatr. Otorhinolaryngol. 2022, 152, 110991. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.Y.C.; Leigh, G. Considering the Impact of Universal Newborn Hearing Screening and Early Intervention on Language Outcomes for Children with Congenital Hearing Loss. Hear. Balance Commun. 2020, 18, 215–224. [Google Scholar] [CrossRef]
- Fulcher, A.; Purcell, A.A.; Baker, E.; Munro, N. Listen up: Children with Early Identified Hearing Loss Achieve Age-Appropriate Speech/Language Outcomes by 3years-of-Age. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1785–1794. [Google Scholar] [CrossRef]
- Dornan, D.; Hickson, L.; Murdoch, B.; Houston, T. Longitudinal Study of Speech Perception, Speech, and Language for Children with Hearing Loss in an Auditory-Verbal Therapy Program. Volta Rev. 2009, 109, 61–85. [Google Scholar] [CrossRef]
- Flexer, C. Cochlear Implants and Neuroplasticity: Linking Auditory Exposure and Practice. Cochlear Implant. Int. 2011, 12 (Suppl. S1), 18–21. [Google Scholar] [CrossRef] [PubMed]
- Ganek, H.; McConkey Robbins, A.; Niparko, J.K. Language Outcomes after Cochlear Implantation. Otolaryngol. Clin. N. Am. 2012, 45, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Percy-Smith, L.; Tønning, T.L.; Josvassen, J.L.; Mikkelsen, J.H.; Nissen, L.; Dieleman, E.; Hallstrøm, M.; Cayé-Thomasen, P. Auditory Verbal Habilitation Is Associated with Improved Outcome for Children with Cochlear Implant. Cochlear Implant. Int. 2018, 19, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Kral, A.; Sharma, A. Developmental Neuroplasticity after Cochlear Implantation. Trends Neurosci. 2012, 35, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Glick, H.; Sharma, A. Cross-Modal Plasticity in Developmental and Age-Related Hearing Loss: Clinical Implications. Hear. Res. 2017, 343, 191–201. [Google Scholar] [CrossRef]
- Gordon, K.A.; Wong, D.D.E.; Valero, J.; Jewell, S.F.; Yoo, P.; Papsin, B.C. Use It or Lose It? Lessons Learned from the Developing Brains of Children Who Are Deaf and Use Cochlear Implants to Hear. Brain Topogr. 2011, 24, 204–219. [Google Scholar] [CrossRef] [PubMed]
- Kral, A.; Lenarz, T. How the Brain Learns to Listen: Deafness and the Bionic Ear. eNeuroforum 2015, 6, 21–28. [Google Scholar] [CrossRef]
- De Raeve, L.; Cumpăt, M.C.; van Loo, A.; Costa, I.M.; Matos, M.A.; Dias, J.C.; Mârțu, C.; Cavaleriu, B.; Gherguț, A.; Maftei, A.; et al. Quality Standard for Rehabilitation of Young Deaf Children Receiving Cochlear Implants. Medicina 2023, 59, 1354. [Google Scholar] [CrossRef] [PubMed]
- Kaipa, R.; Danser, M.L. Efficacy of Auditory-Verbal Therapy in Children with Hearing Impairment: A Systematic Review from 1993 to 2015. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 124–134. [Google Scholar] [CrossRef]
- Binos, P.; Nirgianaki, E.; Psillas, G. How Effective Is Auditory–Verbal Therapy (AVT) for Building Language Development of Children with Cochlear Implants? A Systematic Review. Life 2021, 11, 239. [Google Scholar] [CrossRef] [PubMed]
- Auditory Verbal UK. A Sound of Future: Raising Expectations for Children with Deafness; CIICA: Brussels, Belgium, 2022. [Google Scholar]
- WHO. World Report on Hearing; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Mitchell, R.E.; Karchmer, M. Chasing the Mythical Ten Percent: Parental Hearing Status of Deaf and Hard of Hearing Students in the United States. Sign Lang. Stud. 2004, 4, 138–163. [Google Scholar] [CrossRef]
- Estabrooks, W.; Morrison, H.M.; MacIver-Lux, K. Auditory—Verbal Therapy: Science, Research, and Practice; Plural Publishing, Inc.: San Diego, CA, USA, 2020. [Google Scholar]
- Thomas, E.S.; Zwolan, T.A. Communication Mode and Speech and Language Outcomes of Young Cochlear Implant Recipients: A Comparison of Auditory-Verbal, Oral Communication, and Total Communication. Otol. Neurotol. 2019, 40, E975–E983. [Google Scholar] [CrossRef]
- Percy-Smith, L.; Wischmann, S.; Josvassen, J.L.; Schiøth, C.; Cayé-Thomasen, P. Language Development for the New Generation of Children with Hearing Impairment. J. Clin. Med. 2021, 10, 2350. [Google Scholar] [CrossRef]
- Monshizadeh, L.; Vameghi, R.; Sajedi, F.; Yadegari, F.; Hashemi, S.B.; Kirchem, P.; Kasbi, F. Comparison of Social Interaction between Cochlear-Implanted Children with Normal Intelligence Undergoing Auditory Verbal Therapy and Normal-Hearing Children: A Pilot Study. J. Int. Adv. Otol. 2018, 14, 35–40. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Cupples, L.; Leigh, G.; Hou, S.; Wong, A. Predicting Quality of Life and Behavior and Emotion from Functional Auditory and Pragmatic Language Abilities in 9-Year-Old Deaf and Hard-of-Hearing Children. J. Clin. Med. 2021, 10, 5357. [Google Scholar] [CrossRef] [PubMed]
- Percy-Smith, L.; Cayé-Thomasen, P.; Gudman, M.; Jensen, J.H.; Thomsen, J. Self-Esteem and Social Well-Being of Children with Cochlear Implant Compared to Normal-Hearing Children. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Constantinescu-Sharpe, G.; Phillips, R.L.; Davis, A.; Dornan, D.; Hogan, A. Social Inclusion for Children with Hearing Loss in Listening and Spoken Language Early Intervention: An Exploratory Study. BMC Pediatr. 2010, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- Ashori, M. Impact of Auditory-Verbal Therapy on Executive Functions in Children with Cochlear Implants. J. Otol. 2022, 17, 130–135. [Google Scholar] [CrossRef]
- Noel, A.; Manikandan, M.; Kumar, P. Efficacy of Auditory Verbal Therapy in Children with Cochlear Implantation Based on Auditory Performance–A Systematic Review. Cochlear Implant. Int. 2023, 24, 43–53. [Google Scholar] [CrossRef]
- WHO. Constitution of the World Health Organization: Public Health Report; WHO: Geneva, Switzerland, 1946; Volume 61, pp. 1268–1277. [Google Scholar]
- Percy-Smith, L.; Cayé-Thomasen, P.; Breinegaard, N.; Jensen, J.H. Parental Mode of Communication Is Essential for Speech and Language Outcomes in Cochlear Implanted Children. Acta Otolaryngol. 2010, 130, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Percy-Smith, L.; Busch, G.W.; Sandahl, M.; Nissen, L.; Josvassen, J.L.; Bille, M.; Lange, T.; Cayé-Thomasen, P. Significant Regional Differences in Denmark in Outcome after Cochlear Implants in Children. Dan. Med. J. 2012, 59, A4435. [Google Scholar]
- Hitchins, A.R.C.; Hogan, S.C. Outcomes of Early Intervention for Deaf Children with Additional Needs Following an Auditory Verbal Approach to Communication. Int. J. Pediatr. Otorhinolaryngol. 2018, 115, 125–132. [Google Scholar] [CrossRef]
- Schiøth, C.; Hallstrøm, M.; Sigtryggsdóttir, I.; Dyrberg, S.; Cordtz, S.M. Evaluering af det 3-årige AVT-forløb 2017–2021 [Evaluation of the Three-Year AVT-Program 2017–2021]; Decibel: Copenhagen, Denmark, 2022. [Google Scholar]
- Coninx, F.; Weichbold, V.; Tsiakpini, L.; Autrique, E.; Bescond, G.; Tamas, L.; Compernol, A.; Georgescu, M.; Koroleva, I.; Le Maner-Idrissi, G.; et al. Validation of the LittlEARS® Auditory Questionnaire in Children with Normal Hearing. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1761–1768. [Google Scholar] [CrossRef]
- Dunn, L.M.; Dunn, D.M. The Peabody Picture Vocabulary Test, Fourth Edition, 4th ed.; NCS Pearson, Inc.: Bloomington, MN, USA, 2007. [Google Scholar]
- Dale, P.S.; Paul, A.; Rosholm, M.; Bleses, D. Prediction from Early Childhood Vocabulary to Academic Achievement at the End of Compulsory Schooling in Denmark. Int. J. Behav. Dev. 2023, 47, 123–134. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Arnfred, J.; Svendsen, K.; Rask, C.; Jeppesen, P.; Fensbo, L.; Houmann, T.; Obel, C.; Niclasen, J.; Bilenberg, N. Danish Norms for the Strengths and Difficulties Questionnaire. Dan. Med. J. 2019, 66, A5546. [Google Scholar] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)-A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.; Kjøge, G.S. Viborg Materialet, 1st ed.; Specialpædagogisk Forlag: Herning, Denmark, 2005. [Google Scholar]
- Edward, S.; Letts, C.; Sinka, I. The New Reynell Developmental Scales; GL-Assessment: London, UK, 2011. [Google Scholar]
- Semel, E.; Wiig, E.H.; Secord, W.A. Clinical Evaluation of Language Fundamentals, Fourth Edition (CELF-4), 4th ed.; Pearson: London, UK, 2003. [Google Scholar]
- Eriks-Brophy, A.; Ganek, H.; DuBois, G. Evaluating the Research Examining Outcomes of 59 Auditory-Verbal Therapy: Moving from evidence-based to evidence-informed practice. In Auditory-Verbal Therapy, Science, Research, and Practice; Estabrooks, W., Morrison, H.M., MacIver-Lux, K., Eds.; Plural Publishing: San Diego, CA, USA, 2020; pp. 59–144. [Google Scholar]
- Campbell, W.N.; Douglas, N.F. Supporting Evidence-Based Practice in Speech-Language Pathology: A Review of Implementation Strategies for Promoting Health Professional Behavior Change. Evid. Based Commun. Assess. Interv. 2017, 11, 72–81. [Google Scholar] [CrossRef]
- Olswang, L.B.; Goldstein, H. Collaborating on the Development and Implementation of Evidence-Based Practices: Advancing Science and Practice. Evid. Based Commun. Assess. Interv. 2017, 11, 61–71. [Google Scholar] [CrossRef]
- Johnson, M.J.; May, C.R. Promoting Professional Behaviour Change in Healthcare: What Interventions Work, and Why? A Theory-Led Overview of Systematic Reviews. Open 2015, 5, 8592. [Google Scholar] [CrossRef]
- Stevenson, J.; Kreppner, J.; Pimperton, H.; Worsfold, S.; Kennedy, C. Emotional and Behavioural Difficulties in Children and Adolescents with Hearing Impairment: A Systematic Review and Meta-Analysis. Eur. Child Adolesc. Psychiatry 2015, 24, 477–496. [Google Scholar] [CrossRef] [PubMed]
- Roland, L.; Fischer, C.; Tran, K.; Rachakonda, T.; Kallogjeri, D.; Lieu, J.E.C. Quality of Life in Children with Hearing Impairment: Systematic Review and Meta-Analysis. In Proceedings of the American Academy of Otolaryngology-Head and Neck Surgery Annual Meeting, Dallas, TX, USA, 27–30 September 2016; SAGE Publications Inc.: Newcastle-upon-Tyne, UK, 2016; Volume 155, pp. 208–219. [Google Scholar]
- Castellanos, I.; Kronenberger, W.G.; Pisoni, D.B. Psychosocial Outcomes in Long-Term Cochlear Implant Users. Ear Hear. 2018, 39, 527–539. [Google Scholar] [CrossRef]
- Wong, C.L.; Ching, T.Y.; Leigh, G.; Cupples, L.; Button, L.; Marnane, V.; Whitfield, J.; Gunnourie, M.; Martin, L. Psychosocial Development of 5-Year-Old Children with Hearing Loss: Risks and Protective Factors. Int. J. Audiol. 2018, 57, S81–S92. [Google Scholar] [CrossRef]
- Lingås Haukedal, C. Quality of Life in Children with Hearing Loss. Ph.D. Thesis, Department of Special Needs Education, University of Oslo, Oslo, Norway, 2020. [Google Scholar]
- Ikiz, M.; Yucel, E. Examination of Language, Behavioral, Academic, and Social Skills of Cochlear Implant Users in Early Primary Education. J. Am. Acad. Audiol. 2022, 33, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Extended Version of the Strengths and Difficulties Questionnaire as a Guide to Child Psychiatric Caseness and Consequent Burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef]
- Lai, K.Y.C.; Leung, P.W.L.; Luk, E.S.L.; Wong, A.S.L. Use of the Extended Strengths and Difficulties Questionnaire (SDQ) to Predict Psychiatric Caseness in Hong Kong. Child Psychiatry Hum. Dev. 2014, 45, 703–711. [Google Scholar] [CrossRef]
- Percy-Smith, L.; Jantzen, L.; Cayé-Thomasen, P. Cochleaimplantation Til Børn. Dan. Med. J. 2023, 185, V07230480. [Google Scholar]
- Howell, T.; Sung, V.; Smith, L.; Dettman, S. Australian Families of Deaf and Hard of Hearing Children: Are They Using Sign? Int. J. Pediatr. Otorhinolaryngol. 2024, 179, 111930. [Google Scholar] [CrossRef] [PubMed]
- UN Committee on the Rights of the Child (CRC). General Comment No. 15 (2013) on the Right of the Child to the Enjoyment of the Highest Attainable Standard of Health (Art. 24); UNHCR: Geneva, Switzerland, 2013. [Google Scholar]

{kind=link}
{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Gender | Boy | 22 (42%) |
| Girl | 31 (58%) | |
| Diagnosis of HL/Aetiology 1 | Birth complications | 1 (2%) |
| Infections | 6 (11%) | |
| Auditory neuropathy | 2 (4%) | |
| Hereditary HL | 16 (30%) | |
| Genetics without evidence of heredity | 4 (8%) | |
| Syndromes | 17 (32%) | |
| Ear anomalies | 5 (9%) | |
| Other | 2 (4%) | |
| Unknown | 17 (32%) | |
| Additional disabilities | 8 (15%) | |
| Hearing device | Bilateral CI | 25 (47%) |
| Bilateral HA | 15 (28%) | |
| Bimodal CI/HA | 12 (23%) | |
| Bilateral BAHS | 1 (2%) | |
| Degree of hearing loss | 41–60 dB HL (moderate) | 11 (21%) |
| 61–80 dB HL (severe) | 5 (9%) | |
| >80 dB HL (profound) | 37 (70%) | |
| Diagnosed through UNHS | Yes | 46 (87%) |
| No | 7 (13%) | |
| Parent–child language | Danish | 36 (68%) |
| Danish and/or another language 2 | 16 (30%) | |
| Danish/Arabic/sign-support | 1 (2%) | |
| Mean age in years (SD) | Start of AVT | 1.8 (1.5) |
| End of AVT | 5.1 (2.1) | |
| Test with PPVT-4 | 4.9 (1.6) | |
| Test with SDQ | 6.6 (2.1) |
| SDQ | Close to Average n (%) | Slightly Raised/ Slightly lowered n (%) | High/ Low n (%) | Very High/ Very Low n (%) |
|---|---|---|---|---|
| Emotional problems * | 49 (92%) | 3 (6%) | 0 (0%) | 1 (2%) |
| Conduct problems * | 46 (87%) | 4 (8%) | 2 (4%) | 1 (2%) |
| Hyperactivity * | 44 (83%) | 3 (6%) | 2 (4%) | 4 (8%) |
| Peer problems * | 46 (87%) | 1 (2%) | 4 (8%) | 2 (4%) |
| Total difficulties * | 43 (81%) | 8 (15%) | 1 (2%) | 1 (2%) |
| Prosocial behaviour ** | 46 (87%) | 2 (4%) | 3 (6%) | 2 (4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wischmann, S.; Samar, C.F.; Hestbæk, M.K.; Serafin, S.; Cayé-Thomasen, P.; Percy-Smith, L. Quality Assurance of a Hospital-Based Auditory Verbal Intervention for Children with Hearing Loss. J. Clin. Med. 2025, 14, 1098. https://doi.org/10.3390/jcm14041098
Wischmann S, Samar CF, Hestbæk MK, Serafin S, Cayé-Thomasen P, Percy-Smith L. Quality Assurance of a Hospital-Based Auditory Verbal Intervention for Children with Hearing Loss. Journal of Clinical Medicine. 2025; 14(4):1098. https://doi.org/10.3390/jcm14041098
Chicago/Turabian StyleWischmann, Signe, Cecilia Fernandez Samar, Marianne Kyhne Hestbæk, Stefania Serafin, Per Cayé-Thomasen, and Lone Percy-Smith. 2025. "Quality Assurance of a Hospital-Based Auditory Verbal Intervention for Children with Hearing Loss" Journal of Clinical Medicine 14, no. 4: 1098. https://doi.org/10.3390/jcm14041098
APA StyleWischmann, S., Samar, C. F., Hestbæk, M. K., Serafin, S., Cayé-Thomasen, P., & Percy-Smith, L. (2025). Quality Assurance of a Hospital-Based Auditory Verbal Intervention for Children with Hearing Loss. Journal of Clinical Medicine, 14(4), 1098. https://doi.org/10.3390/jcm14041098