
The Use of Highly Porous 3-D-Printed Titanium Acetabular Cups in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Criteria
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Data Collection
2.4. Assessment of Study Quality
2.5. Statistical Analysis
3. Results
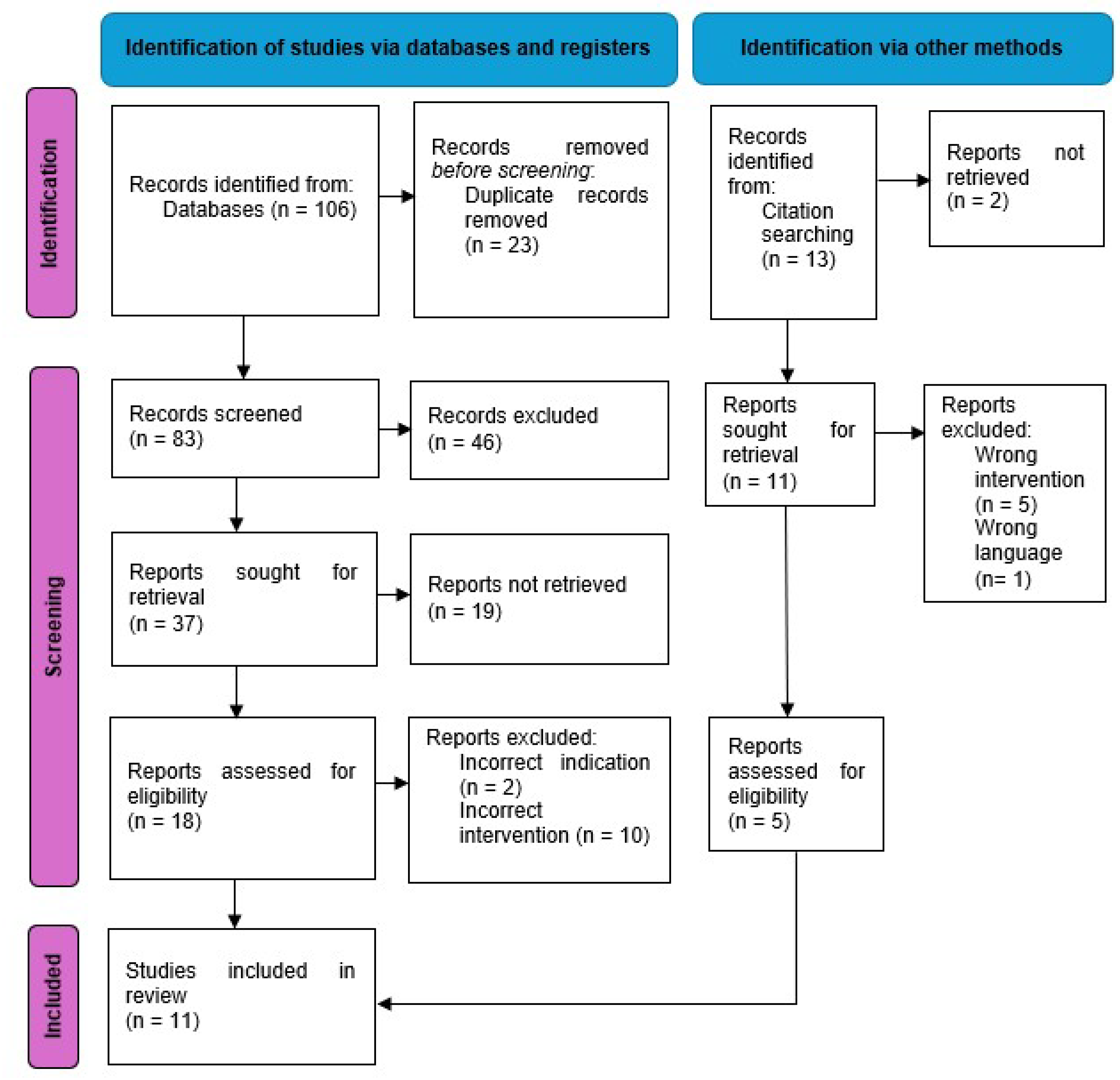
3.1. Search Results

{kind=link}
| Authors | Type of Study | Quality of Evidence | MINORS Score |
|---|---|---|---|
| Castagnini et al. (2021) [23] | retrospective case series | IV | 11 |
| Cozzi Lepri et al. (2022) [10] | retrospective cohort | III | 9 |
| De Meo et al. (2018) [11] | retrospective cohort | III | 11 |
| Shaarani et al. (2023) [12] | retrospective cohort | III | 10 |
| Shang et al. (2022) [24] | retrospective cohort | III | 11 |
| Shichman (2022) [25] | retrospective cohort | III | 10 |
| El Ghazawy et al. (2022) [26] | retrospective cohort | III | 10 |
| Perticarini et al. (2021) [27] | retrospective cohort | III | 10 |
| Munegato et al. (2018) [28] | retrospective cohort | III | 10 |
| Gallart et al. (2016) [29] | retrospective cohort | III | 10 |
| Steno et al. (2015) [17] | retrospective cohort | III | 11 |
3.2. Demographics
3.3. Indications for Surgery
3.4. Classification of Acetabular Defects
3.5. Type of Implants
| Authors | Manufacturer of Implant | Type of Acetabular Cup | Details of Acetabular Cup Size | Bearing Surfaces | Use of Grafts and Augments | Use of Screws |
|---|---|---|---|---|---|---|
| Castagnini et al. (2021) [23] | Adler | Ti-por cup | 50.6 mm ± 3.6 (range 46–56) (Mean) | not specified | 3 (16.7%) morselise bone allograft | 3 cases (16.7%) |
| Cozzi Lepri et al. (2022) [10] | Lima | Delta TT one in 30 (35.3%), Delta TT revision in 55 (64.7%) | not specified | 85 (100%) Dual mobility | 85 (100%), corticocancellous allograft, 12 (14.11%) medial wall meshes | 4.2 (range 2–7) (Mean) |
| De Meo et al. (2018) [11] | Lima | Delta TT one in 39 (60.9%), Delta TT revision in 25 (39.1%) | not specified | not specified | 34 (53.1%), morselise bone allograft, 4 (6.3%) augment | not specified |
| Shaarani et al. (2023) [12] | Smith and Nephew | REDAPT shell | 54 mm (Mode) | 29 (49.15%) Dual mobility | 6 (10.17%) augment | 4 (Median) |
| Shang et al. (2022) [24] | Aikang corp | Aikang TT | not specified | not specified | 4 (17.39%) augment, 1 (4.35%) structural bone graft, 5 (21.74%) augment and bone graft | not specified |
| Shichman (2022) [25] | Smith and Nephew | REDAPT shell | 60 mm (range 48–80) (Median) | 36 mm (range 28–36) (Median) | 12 (30%) Allograft | 4 (range 2–8) (Median) |
| El Ghazawy et al. (2022) [26] | Lima | Delta TT revision | Not stated | Head size not stated, 3 (12.5%) Dual mobility | 20 (83%) Morselised allograft, 19 (80%) augments | 3 (range 2–4) (mean) |
| Perticarini et al. (2021) [27] | Lima | Delta revision TT in 39 (41.1%), Delta One TT in 56 (58.9%) | 46–66 mm | 6 (6.3%) Dual mobility | 57 (60%) Allograft, 13 (13.7%) augments, 4 (4.2%) meshes | 2–6 screws (range) |
| Munegato et al. (2018) [28] | Lima | Delta TT revision | Not stated | Not stated | 24 (66.7%) Allograft, 11 (30.6%) synthetic bone graft | not stated |
| Gallart et al. (2016) [29] | Lima | Delta Revision TT 18 (25%), Delta One TT 54 (75%) | Not stated | Not stated | 22 (30.6%) Allograft, 17 (23.6%) augment | not stated |
| Steno et al. (2015) [17] | Lima | Delta TT 19 (23.5%), Delta One TT 49 (60.5%), Delta Revision TT 13 (16%) | Mode 58 (range 44–68) | 5 (6.2%) Dual mobility | 53 (65.4%) Morselised allograft, 3 (3.7%) structural allograft, 16 (19.8%) augments | 2–5 screws (range) |
3.6. Clinical Outcomes
3.7. Imaging Outcomes
3.8. Survival and Complication Rates
| Authors | Clinical Outcomes | Radiological Outcomes | Survival Rate | Complications | Causes for Re-Operation |
|---|---|---|---|---|---|
| Castagnini et al. (2021) [23] | HHS 88.3 ± 9.2 (range 68–97) | No cup loosening or cup migration at final follow up. No periacetabular radiolucency. Good cup osseointegration according to Moore et al. (2006) [30] of >3 in every case. | 100% | 4 complications in 3 (16.7%) cases. 1 (5.6%) PJI, 1 (5.6%) wound infection, 1 (5.6%) dislocation, 1 (5.6%) psoas tendonitis | No revision |
| Cozzi Lepri et al. (2022) [10] | HHS 89.7 (range 83–98) | Bone graft incorporation according to Gie et al. (1993) [31] type 1 (n = 8, 9.4%), type 2 (n = 22, 25.9%), type 3 (n = 55, 64.7%). | 5 year 100%, 10 year 88% | 19 (22.4%) DVT, 4 (4.7%) femoral neuropraxia, 1 (1.2%) aseptic loosening, 1 (1.2%) PJI | 2 (2.3%) cases re-operation after 5.6 years. 1 (1.2%) PJI, 1 (1.2%) aseptic loosening |
| De Meo et al. (2018) [11] | HHS 83.7 (range 58.9–91.3) | No radiolucent lines or signs of migration were observed. | Kaplan–Meier survivorship curve at 48.3 months showed survivorship of 89.7% for revision and 94.8% for acetabular cup removal | 3 (5.2%) instability, 2 (3.4%) PJI, 1 (1.7%) aseptic loosening | 6 (10.3%) cases re-operation. 3 (5.2%) instability, 2 (3.4%) PJI (3.4%), 1 (1.7%) aseptic loosening |
| Shaarani et al. (2023) [12] | OHS 83 (SD 15), SF-12 physical 44 (SD 11), SF-12 mental 56 (SD 10), WOMAC function score 84 (SD 17), WOMAC stiffness score 83 (SD 15), WOMAC pain score 85 (SD 15), WOMAC global score 85 (SD 17) | 2 (3.4%) Shell migration, no radiographs demonstrated radiolucency. | - | 2 (3.4%) shell migrations, 1 (1.7%) acute PJI | 1 (1.7%) revision of liner for PJI. 1 (1.7%) planned revision of cup migration |
| Shang et al. (2022) [24] | HHS 90.48 SD 3.65, SF-36 754.04 SD 22.74, VAS 1.14 SD 0.23 | All cups remained stable with no loosening and no changes in cup abduction angle. According to bone growth criteria from Anderson Orthopaedic Research institute, 2 cups had 2 signs, 17 had 3 signs, 4 had 4 signs. | 100% | 1 (4.3%) persistent pain, 1 (4.3%) persistent wound drainage | No revisions |
| Shichman (2022) [25] | HHS 83.53 ± 12.15, LOS 5.34 ± 3.34, | 39/40 (97.5%) cups had osteointegration, 1 (2.5%) reported cup migration. | Kaplan-Meier showed all-cause revision free survival rate of 95.0% at 6 months and 1 year, and 92.0% at 4 years | 2 (5%) Acute PJI, 1 (2.5%) implant migration with aspetic loosening, 1 (2.5%) DVT | 1 (2.5%) Implant migration with aspetic loosening, 2 (5%) PJI |
| El Ghazawy et al. (2022) [26] | HHS 85 (range 70–98) | No change in cup position. No progressive radiolucency. | 100% | No complications | No re-operations |
| Perticarini et al. (2021) [27] | HHS 84.4 (range 46–99) SD 7.56 | 1 (1.1%) graft resorption. All other cups no cup migration or aseptic loosening. | 88.54% (95 CI 80.18–93.52%) at 71 months | 7 (7.3%) PJI, 7 (7.3%) Instability, 1(1.1%) graft resorption with aseptic loosening, 2 (2.1%) periprosthetic femur fracture, 1 (1.1%) trochanteric bursitis, 3 (3.2%) heterotrophic ossification | 7 (7.3%) PJI, 5 (5.3%) instability, 1 (1.1%) graft resorption with aseptic loosening, 2 (2.1%) periprosthetic femur fracture |
| Munegato et al. (2018) [28] | HHS 87 (SD ± 7.7) | No signs of loosening, bone graft graded to Gie: 21 (58.3%) Type 3, 12 (33.3%) Type 2, 2 (5.6%) Type 1. | 100% for aseptic loosening, 91.7% for any revision | 1 (2.8%) PJI, 2 (5.6%) instability | 1 (2.8%) PJI with dislocation, 2 (5.6%) cases of instability that developed PJI after re-operation |
| Gallart et al. (2016) [29] | Merle d’Aubigné-Postel score pain 5.7 ± 0.7, walking 5.3 ± 0.7, range of motion 5.6 ± 0.7 | Not stated. | 88.89% | 3 (4.2%) PJI, 3 (4.2%) Instability, 2 (2.8) aseptic loosening | 3 (4.2%) PJI, 3 (4.2%) Instability, 2 (2.8) aseptic loosening |
| Steno et al. (2015) [17] | Merle d’Aubigné-Postel functional score 9.78, pain 5.45 (range 3–6), walking 4.33 (range 3–6) | 3 (3.7%) initial cup migrations that stabilised with no radiolucency at final follow up. | 98.77% | 3 (3.7%) cups with medial migration that stabilised, 1 (1.2%) instability | 1 (1.2%) instability |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| THA | Total hip arthroplasty |
| 3-D | 3-dimensional |
| CNC | computer numerical controlled |
| PRISMA | Preferred Reporting Items for Systematic reviews and meta-analyses |
| MINORS | Methodological Index for Non-Randomized Studies |
| HHS | Harris Hip Score |
| VAS | Visual Analogue scale |
| OHS | Oxford hip score |
| LOS | Length of stay |
| SF-12 | Short-form 12 |
| WOMAC | Western Ontario and McMaster Universities Osteoarthritis Index |
| EBM | Electron Beam Melting |
| SLM | Selective Laser Melting |
References
- Blom, A.W.; Donovan, R.L.; Beswick, A.D.; Whitehouse, M.R.; Kunutsor, S.K. Common elective orthopaedic procedures and their clinical effectiveness: Umbrella review of level 1 evidence. BMJ 2021, 374, n1511. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35, S79–S85. [Google Scholar] [CrossRef]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Shichman, I.; Roof, M.; Askew, N.; Nherera, L.; Rozell, J.C.; Seyler, T.M.; Schwarzkopf, R. Projections and Epidemiology of Primary Hip and Knee Arthroplasty in Medicare Patients to 2040–2060. JBJS Open Access 2023, 8, e22. [Google Scholar] [CrossRef]
- Deere, K.; Whitehouse, M.R.; Kunutsor, S.K.; Sayers, A.; Mason, J.; Blom, A.W. How long do revised and multiply revised hip replacements last? A retrospective observational study of the National Joint Registry. Lancet Rheumatol. 2022, 4, e468–e479. [Google Scholar] [CrossRef] [PubMed]
- Shichman, I.; Askew, N.; Habibi, A.; Nherera, L.; Macaulay, W.; Seyler, T.; Schwarzkopf, R. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2040-2060. Arthroplast. Today 2023, 21, 101152. [Google Scholar] [CrossRef]
- Karachalios, T.; Komnos, G.; Koutalos, A. Total hip arthroplasty: Survival and modes of failure. EFORT Open Rev. 2018, 3, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Cozzi Lepri, A.; Innocenti, M.; Galeotti, A.; Carulli, C.; Villano, M.; Civinini, R. Trabecular titanium cups in acetabular revision arthroplasty: Analysis of 10-year survivorship, restoration of center of rotation and osteointegration. Arch. Orthop. Trauma. Surg. 2022, 142, 3523–3531. [Google Scholar] [CrossRef] [PubMed]
- De Meo, F.; Cacciola, G.; Bellotti, V.; Bruschetta, A.; Cavaliere, P. Trabecular Titanium acetabular cups in hip revision surgery: Mid-term clinical and radiological outcomes. HIP Int. 2018, 28 (Suppl. S2), 61–65. [Google Scholar] [CrossRef]
- Shaarani, S.R.; Jaibaji, M.; Yaghmour, K.M.; Vles, G.; Haddad, F.S.; Konan, S. Early clinical and radiological outcomes of the new porous titanium shell in combination with locking screw in revision total hip arthroplasty. Arthroplasty 2023, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Castagnini, F.; Bordini, B.; Stea, S.; Calderoni, P.P.; Masetti, C.; Busanelli, L. Highly porous titanium cup in cementless total hip arthroplasty: Registry results at eight years. Int. Orthop. 2019, 43, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Dall’Ava, L.; Hothi, H.; Di Laura, A.; Henckel, J.; Hart, A. 3D printed acetabular cups for total hip arthroplasty: A review article. Metals 2019, 9, 729. [Google Scholar] [CrossRef]
- Malahias, M.A.; Kostretzis, L.; Greenberg, A.; Nikolaou, V.S.; Atrey, A.; Sculco, P.K. Highly Porous Titanium Acetabular Components in Primary and Revision Total Hip Arthroplasty: A Systematic Review. J. Arthroplast. 2020, 35, 1737–1749. [Google Scholar] [CrossRef] [PubMed]
- Vutescu, E.S.; Hsiue, P.; Paprosky, W.; Nandi, S. Comparative survival analysis of porous tantalum and porous titanium acetabular components in total hip arthroplasty. HIP Int. 2017, 27, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Steno, B.; Kokavec, M.; Necas, L. Acetabular revision arthroplasty using trabecular titanium implants. Int. Orthop. 2015, 39, 389–395. [Google Scholar] [CrossRef]
- Kaneko, T.; Nakamura, S.; Hayakawa, K.; Tokimura, F.; Miyazaki, T. Clinical and radiological outcomes of total hip arthroplasty in octogenarian patients using a three-dimensional porous titanium cup: A retrospective analysis in Japanese patients. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Dall’ava, L.; Hothi, H.; Henckel, J.; Di Laura, A.; Tirabosco, R.; Eskelinen, A.; Skinner, J.; Hart, A. Osseointegration of retrieved 3D-printed, off-the-shelf acetabular implants Aims. Bone Joint Res. 2021, 10, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Castagnini, F.; Mariotti, F.; Tassinari, E.; Bordini, B.; Zuccheri, F.; Traina, F. lsolated acetabular revisions of articular surface replacement (ASR) XL implants with highly porous titanium cups and Delta bearings. HIP Int. 2021, 31, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Shang, G.; Xiang, S.; Guo, C.; Guo, J.; Wang, P.; Wang, Y.; Xu, H. Use of a new off-the-shelf 3D-printed trabecular titanium acetabular cup in Chinese patients undergoing hip revision surgery: Short- to mid-term clinical and radiological outcomes. BMC Musculoskelet Disord. 2022, 23, 636. [Google Scholar] [CrossRef] [PubMed]
- Shichman, I.; Somerville, L.; Lutes, W.B.; Jones, S.A.; McCalden, R.; Schwarzkopf, R. Outcomes of novel 3D-printed fully porous titanium cup and a cemented highly cross-linked polyethylene liner in complex and revision total hip arthroplasty. Arthroplasty 2022, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- El Ghazawy, A.K.; Bassiony, A.A.; Abdelazim, H.; Gameel, S. Acetabular revision using trabecular titanium (Delta TT) revision cups: A retrospective case series. SICOT J. 2022, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Perticarini, L.; Rossi, S.M.P.; Medetti, M.; Benazzo, F. Clinical and radiological outcomes of acetabular revision surgery with trabecular titanium cups in Paprosky type II and III bone defects. J. Orthop. Traumatol. 2021, 22, 9. [Google Scholar] [CrossRef]
- Munegato, D.; Bigoni, M.; Sotiri, R.; Bruschetta, A.; Omeljaniuk, R.J.; Turati, M.; Andrea, R.; Zatti, G. Clinical and radiological outcomes of acetabular revision with the Delta Revision TT cup. HIP Int. 2018, 28 (Suppl. S2), 54–60. [Google Scholar] [CrossRef] [PubMed]
- Gallart, X.; Fernández-Valencia, J.A.; Riba, J.; Bori, G.; García, S.; Tornero, E.; Combalía, A. Trabecular TitaniumTM cups and augments in revision total hip arthroplasty: Clinical results, radiology and survival outcomes. HIP Int. 2016, 26, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.S.; McAuley, J.P.; Young, A.M.; Engh, C.A. Radiographic signs of osseointegration in porous-coated acetabular components. Clin. Orthop. Relat. Res. 2006, 444, 176–183. [Google Scholar] [CrossRef]
- Gie, G.A.; Linder, L.; Ling, R.S.M.; Simon, J.P.; Slooff, T.J.J.H.; Timperley, A.J. Impacted Cancellous Allografts And Cement For Revision Total Hip Arthroplasty. J. Bone Jt. Surg. Br. Vol. 1993, 75, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Apostu, D.; Lucaciu, O.; Berce, C.; Lucaciu, D.; Cosma, D. Current methods of preventing aseptic loosening and improving osseointegration of titanium implants in cementless total hip arthroplasty: A review. J. Int. Med. Res. 2018, 46, 2104–2119. [Google Scholar] [CrossRef] [PubMed]
- Tsikandylakis, G.; Mortensen, K.R.L.; Gromov, K.; Troelsen, A.; Malchau, H.; Mohaddes, M. The Use of Porous Titanium Coating and the Largest Possible Head Do Not Affect Early Cup Fixation. JBJS Open Access 2020, 5, E2000107. [Google Scholar] [CrossRef] [PubMed]
- Strahl, A.; Boese, C.K.; Ries, C.; Hubert, J.; Beil, F.T.; Rolvien, T. Outcome of different reconstruction options using allografts in revision total hip arthroplasty for severe acetabular bone loss: A systematic review and meta-analysis. Arch. Orthop. Trauma. Surg. 2023, 143, 6403–6422. [Google Scholar] [CrossRef]
- Argyropoulou, E.; Sakellariou, E.; Galanis, A.; Karampinas, P.; Rozis, M.; Koutas, K.; Tsalimas, G.; Vasiliadis, E.; Vlamis, J.; Pneumaticos, S. Porous Tantalum Acetabular Cups in Primary and Revision Total Hip Arthroplasty: What Has Been the Experience So Far?—A Systematic Literature Review. Biomedicines 2024, 12, 959. [Google Scholar] [CrossRef]
- Ma, K.; Ma, Z.; Cheng, L.; Zhao, D. Progress in the Application of Porous Tantalum Metal in Hip Joint Surgery. Orthop. Surg. 2024, 16, 2877–2886. [Google Scholar] [CrossRef] [PubMed]
- Castagnini, F.; Caternicchia, F.; Biondi, F.; Masetti, C.; Faldini, C.; Traina, F. Off-the-shelf 3D printed titanium cups in primary total hip arthroplasty. World J. Orthop. 2021, 12, 376–385. [Google Scholar] [CrossRef]
- Dall’Ava, L.; Hothi, H.; Henckel, J.; Di Laura, A.; Shearing, P.; Hart, A. Comparative analysis of current 3D printed acetabular titanium implants. 3D Print Med. 2019, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Cacciola, G.; Giustra, F.; Bosco, F.; De Meo, F.; Bruschetta, A.; De Martino, I.; Risitano, S.; Sabatini, L.; Massè, A.; Cavaliere, P. Trabecular titanium cups in hip revision surgery: A systematic review of the literature. Ann. Jt. 2023, 8, 36. [Google Scholar] [CrossRef] [PubMed]
- Ramappa, M.; Bajwa, A.; Kulkarni, A.; Mcmurtry, I.; Port, A. Early results of a new highly porous modular acetabular cup in revision arthroplasty. Hip Int. 2009, 19, 239244. [Google Scholar] [CrossRef] [PubMed]
- Delanois, R.E.; Gwam, C.U.; Mohamed, N.; Khlopas, A.; Chughtai, M.; Malkani, A.L.; Mont, M.A. Midterm Outcomes of Revision Total Hip Arthroplasty With the Use of a Multihole Highly-Porous Titanium Shell. J. Arthroplast. 2017, 32, 2806–2809. [Google Scholar] [CrossRef]
- Hosny, H.A.H.; El-Bakoury, A.; Srinivasan, S.C.M.; Yarlagadda, R.; Keenan, J. Tritanium Acetabular Cup in Revision Hip Replacement: A Six to Ten Years of Follow-Up Study. J. Arthroplast. 2018, 33, 2566–2570. [Google Scholar] [CrossRef] [PubMed]
- Meneghini, R.M.; Meyer, C.; Buckley, C.A.; Hanssen, A.D.; Lewallen, D.G. Mechanical stability of novel highly porous metal acetabular components in revision total hip arthroplasty. J. Arthroplast. 2010, 25, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Qin, Y.; Li, Y.; Tang, X.; Xiao, J. Trabecular metal versus non-trabecular metal acetabular components for acetabular revision surgery: A systematic review and meta-analysis. Int. J. Surg. 2022, 100, 106597. [Google Scholar] [CrossRef] [PubMed]
| Authors | Number of Hips (Patients) | Gender F | Gender M | Mean Age | Mean BMI (kg/m2) | Mean Follow Up |
|---|---|---|---|---|---|---|
| Castagnini et al. (2021) [23] | 18 (16) | 13 | 3 | 62.3 ± 8.3 (range 51–83) | 26.2 ± 3.1 (range 21.4–31.2) | 5.7 years ± 0.7 (range 5–7 years) |
| Cozzi Lepri et al. (2022) [10] | 85 | 50 | 35 | 67.8 (range 32–83) | 26.9 (95% confidence interval 25.4–27.7, range 18.3–33) | 6.12 years (range 2–10.2) |
| De Meo et al. (2018) [11] | 64 | 37 | 27 | 78.4 (range 42–87) | 26.1 (range 23.5–33.2) | 48.3 months (range 38–82.3) |
| Shaarani et al. (2023) [12] | 59 (55) | 34 | 25 | 68.8 SD 12.3 | 26.6 SD 5.9 | 25.7 months SD 13.8 (range 4–52) |
| Shang et al. (2022) [24] | 23 | 13 | 10 | 70.35 ± 8.1 | 25.61 ± 2.80 | 41.82 months ±11.44 (range 24–64) |
| Shichman (2022) [25] | 40 | 22 | 18 | 71.42 ± 9.97 | 30.36 ± 6.88 | 2.21 years ±0.77 |
| El Ghazawy et al. (2022) [26] | 24 | 6 | 18 | 56 (range 30–67) | Not stated | 20.75 months (14–30) |
| Perticarini et al. (2021) [27] | 95 | 65 | 30 | 70 (range 29–90) SD 11 | 25.68 (range 17–36.67) SD 3.7 | 91 months (24–146) |
| Munegato et al. (2018) [28] | 36 (34) | 24 | 14 | 75 (range 45–92) | Not stated | 39.8 months (12–91.5) |
| Gallart et al. (2016) [29] | 72 (69) | 34 | 38 | 70.7 SD 10.3 | Not stated | 30.5 months SD 16.9 |
| Steno et al. (2015) [17] | 81 (80) | 51 | 30 | 68.3 (range 32–84) | Not stated | 38.14 months (24–62) |
| Authors | Acetabular Defects | Indication for Surgery |
|---|---|---|
| Castagnini et al. (2021) [23] | Paprosky I 15 (83.3%), Paprosky II 3 (16.7%) | All cases were revisions of Du Puy ASR XL metal on metal bearing surface. 5 (27.8%) aseptic loosening and raised metal ions, 8 (44.4%) pain and metal ions over threshold, 4 (22.2%) osteolysis, 1 (5.6%) pseudotumour. |
| Cozzi Lepri et al. (2022) [10] | Paprosky IIB 23 (27.1%), Paprosky IIC 20 (23.5%), Paprosky IIIA 24 (28.2%), Paprosky IIIB 18 (21.2%) | 31 (36.5%) aseptic loosening, 19 (22.3%) recurrent instability, 15 (17.6%) adverse reaction to metal debris (ARMD), 11 (13%) PJI, 9 (10.6%) periprosthetic fracture. |
| De Meo et al. (2018) [11] | Paprosky IIB 25 (39%), Paprosky IIC 15 (23.4%), Paprosky IIIA 15 (23.4%), Paprosky IIIB 9 (14.1%) | 28 (43.75%) aseptic loosening, 26 (40.6%) instability, 10 (15.6%) wear debris osteolysis. |
| Shaarani et al. (2023) [12] | paprosky I 21 (35.6%), Paprosky IIA 19 (32.2%), Paprosky IIB 3 (5.1%), Paprosky IIC 9 (15.3%), Paprosky IIIA 4 (6.8%), Paprosky IIIB 3 (5.1%) | 21 (35.59%) aseptic loosening, 11 (18.64%) PJI, 3 (5.08%) instability, 3 (5.08%) failed DHS, 5 (%) failed hip resurfacing, 2 (3.39%) metastatic disease, 1 (1.69%) acetabular erosion from hemi arthroplasty, 1 (1.69%) squeaking ceramic on ceramic, 1 (1.69%) native hip joint dislocation, 1 (1.69%) broken cement/osteolysis, 1 (1.69%) neck of femur fracture, 1.69%) acetabular fracture, 8 (13.56%) peri-prosthetic fracture, 1 (1.69%) stem fracture. |
| Shang et al. (2022) [24] | Paprosky I 4 (17.39%), Paprosky II 15 (65.22%), Paprosky III 4 (17.39%) | 17 (73.91%) aseptic loosening, 6 (26.09%) PJI. |
| Shichman (2022) [25] | Paprosky I 1 (2.5%), Paprosky IIA 10 (25%), Paprosky IIB 14 (35.0%), Paprosky IIC 2 (5%), Paprosky IIIB 11 (35%), Paprosky IIIC 2 (5%) | 22 (55%) aseptic loosening, 8 (32%) PJI, 2 (5%) instability, 1 (2.5%) trunnionosis, 1 (2.5%) pseudotumour, 6 (15%) complex primary. |
| El Ghazawy et al. (2022) [26] | Paprosky IIIA 7 (29.2%), Paprosky IIIB 15 (62.5%), Paprosky IIB 2 (8.3%) | 19 (79.2%) aseptic loosening, 3 (12.5%) PJI, 2 (8.3%) revision hemiarthroplasty for acetabular erosion. |
| Perticarini et al. (2021) [27] | Paprosky II 53 (55.8%), Paprosky III 42 (44.2%) | 86 (82.69%) aseptic loosening, 8 (7.69%) metallosis, 4 (3.85%) periprosthetic fracture, 3 (2.88%) implant failure, 2 (1.92%) instability, 1 (0.96%) PJI. |
| Munegato et al. (2018) [28] | Paprosky IIB 5 (13.9%), Paprosky IIC 7 (19.4%), Paprosky IIIA 15 (41.7%), Paprosky IIIB 9 (25%) | 33 (91.7%) aseptic loosening, 2 (5.6%) PJI, 2 (2.7%) instability. |
| Gallart et al. (2016) [29] | Paprosky I 19 (26.4%), Paprosky IIA 12 (16.7%), Paprosky IIB 9 (12.5%), Paprosky IIC 16 (22.2%), Paprosky IIIA 12 (16.7%), Paprosky IIIB 4 (5.6%) | 31 (43.1%) aseptic loosening, 27 (37.5%) PJI, 4 (5.6%) instability, 3 (4.2%) metallosis, 2 (2.8%) IMN failure, 1 (1.4%) RA, 1 (1.4%) spondyloarthritis. |
| Steno et al. (2015) [17] | Paprosky type I 9 (11.1%), Paprosky IIA 11 (13.6%), Paprosky IIB 27 (33.3%), Paprosky IIC 6 (7.4%), Paprosky IIIA 15 (18.5%), Paprosky IIIB 13 (16%) | 66 (81.5%) aseptic loosening, 3 (3.7%) conversion hemiarthroplasty, 4 (4.9%) instability, 8 (9.9%) PJI. |
| Manufacturer | Acetabular Cup | Composition | Tradename Porous Structure | Porosity (%) | Pore Diameter (μm) | Production Method | References: |
|---|---|---|---|---|---|---|---|
| Lima Corporate (San Daniele, Italy) | Delta TT cup | Titanium | Trabecular titanium | 65 | 640 | EBM | [37,38] |
| Delta revision TT | Titanium | Trabecular titanium | 65 | 640 | EBM | [37,38] | |
| Delta one TT | Titanium | Trabecular titanium | 65 | 640 | EBM | [37,38] | |
| Smith and Nephew (Memphis, TN, USA) | REDAPT | Titanium | Conceloc Advanced Porous Titanium | 60–80 | 200–934 | EBM | [14,37] |
| Aikang Corp. (Beijing, China) | 3D ACT | Titanium | - | 80 | 600–1000 | EBM | [24] |
| Adler Ortho (Milan, Italy) | Omnia | Titanium | Tri-Por Cup | 65–70 | 700 | EBM | [14,37] |
| Polymax ti-por | Titanium | Tri-Por Cup | 65–70 | 700 | EBM | [14,37] | |
| Omnia ti-por | Titanium | Tri-Por Cup | 65–70 | 700 | EBM | [14,37] | |
| Fixa ti-por | Titanium | Tri-Por Cup | 65–70 | 700 | EBM | [14,37] | |
| Agilis ti-por | Titanium | Tri-Por Cup | 65–70 | 700 | EBM | [14,37] | |
| Stryker (Mahwah, NJ, USA) | Trident II | Titanium | Tritanium | 55–65 | 100–700 | SLM | [14,37,38] |
| Zimmer (Warsaw, IN, USA) | G7 | Titanium | OsseoTi porous technology | 70 | 475 | - | [14,37] |
| Medacta (Castel San Pietro, Switzerland) | Mpact 3D metal | Titanium | 3D Metal | 75 | 600–800 | EBM | [37,38] |
| Kyocera (Kyoto, Japan) | SQRUM TT | Titanium | - | 60 | 640 | EBM | [18,37] |
| Implantcast (Buxtehude, Germany) | Ecofit Epore | Titanium | EPORE | 60 | 100–500 | EBM | [14,37] |
| Corin (Cirencester, UK) | Trinity Plus | Titanium | PLUS (Porous layer unique structure) | 50–90 | 300–900 | - | [37] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, P.R.; Macpherson, G.J.; Simpson, P.; Gaston, P.; Clement, N.D. The Use of Highly Porous 3-D-Printed Titanium Acetabular Cups in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 938. https://doi.org/10.3390/jcm14030938
Almeida PR, Macpherson GJ, Simpson P, Gaston P, Clement ND. The Use of Highly Porous 3-D-Printed Titanium Acetabular Cups in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2025; 14(3):938. https://doi.org/10.3390/jcm14030938
Chicago/Turabian StyleAlmeida, Peter Richard, Gavin J. Macpherson, Philip Simpson, Paul Gaston, and Nick D. Clement. 2025. "The Use of Highly Porous 3-D-Printed Titanium Acetabular Cups in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 14, no. 3: 938. https://doi.org/10.3390/jcm14030938
APA StyleAlmeida, P. R., Macpherson, G. J., Simpson, P., Gaston, P., & Clement, N. D. (2025). The Use of Highly Porous 3-D-Printed Titanium Acetabular Cups in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 14(3), 938. https://doi.org/10.3390/jcm14030938