
The Multifactorial Burden of Endometriosis: Predictors of Quality of Life
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
3. Results
3.1. Pain
3.2. Control and Powerlessness
3.3. Emotional Well-Being
3.4. Social Support
3.5. Self-Image
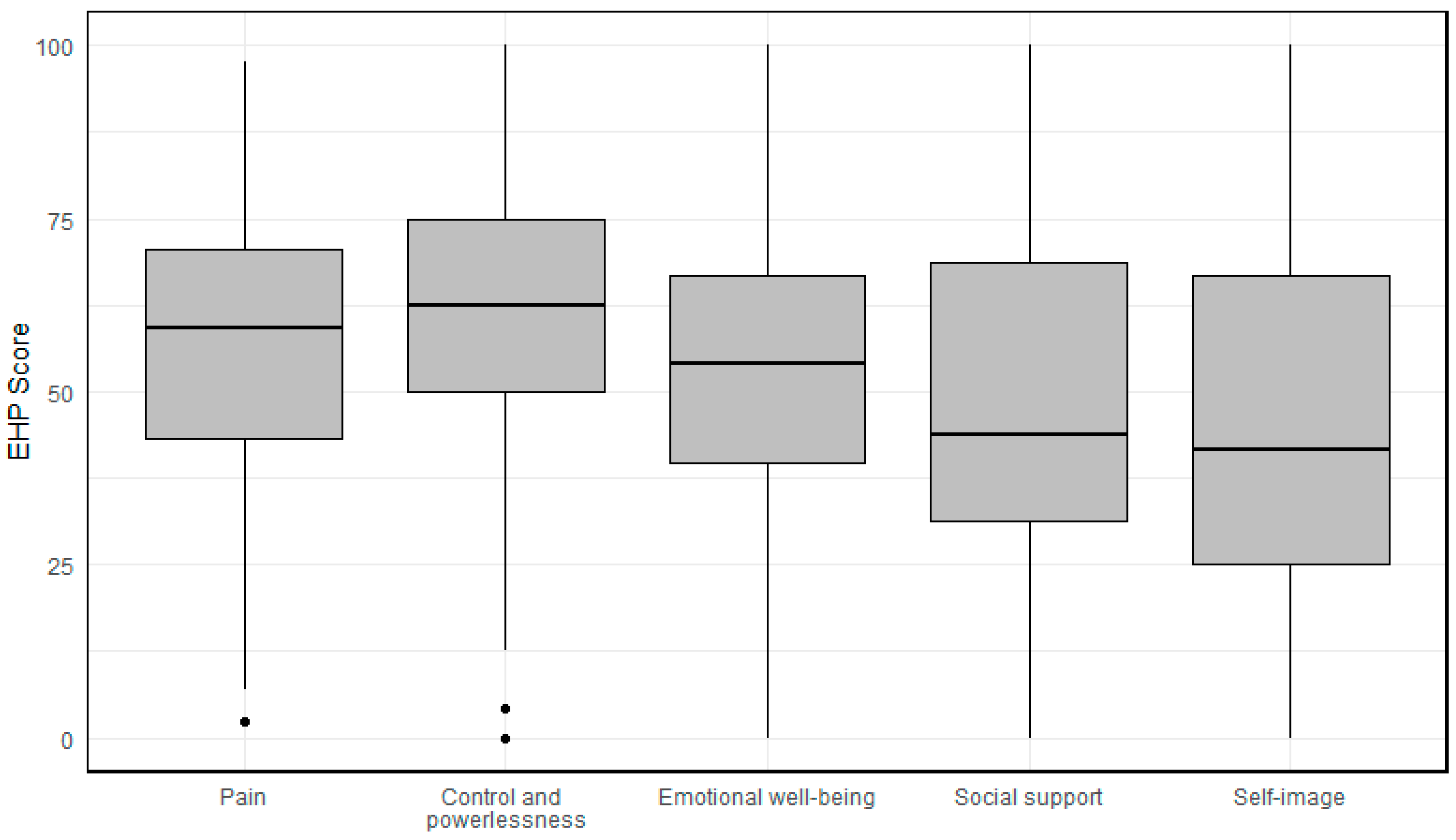
3.6. Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vercellini, P.; Viganò, P.; Somigliana, E.; Fedele, L. Endometriosis: Pathogenesis and treatment. Nat. Rev. Endocrinol. 2014, 10, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; d’Hooghe, T.; de Cicco Nardone, F.; de Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T. World Endometriosis Research Foundation Global Study of Women’s Health consortium. Reprint of: Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertil. Steril. 2019, 112 (Suppl. S1), e137–e152. [Google Scholar] [CrossRef] [PubMed]
- Facchin, F.; Barbara, G.; Saita, E.; Mosconi, P.; Roberto, A.; Fedele, L.; Vercellini, P. Impact of endometriosis on quality of life and mental health: Pelvic pain makes the difference. J. Psychosom. Obstet. Gynaecol. 2015, 36, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Nassiri Kigloo, H.; Itani, R.; Montreuil, T.; Feferkorn, I.; Raina, J.; Tulandi, T.; Mansour, F.; Krishnamurthy, S.; Suarthana, E. Endometriosis, chronic pain, anxiety, and depression: A retrospective study among 12 million women. J. Affect. Disord. 2024, 346, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Cuffaro, F.; Russo, E.; Amedei, A. Endometriosis, Pain, and Related Psychological Disorders: Unveiling the Interplay among the Microbiome, Inflammation, and Oxidative Stress as a Common Thread. Int. J. Mol. Sci. 2024, 25, 6473. [Google Scholar] [CrossRef] [PubMed]
- Ballard, K.D.; Seaman, H.E.; de Vries, C.S.; Wright, J.T. Can symptomatology help in the diagnosis of endometriosis? Findings from a national case-control study—Part 1. BJOG 2008, 115, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Shafrir, A.L.; Farland, L.V.; Shah, D.K.; Harris, H.R.; Kvaskoff, M.; Zondervan, K.; Missmer, S.A. Risk for and consequences of endometriosis: A critical epidemiologic review. Best. Pract. Res. Clin. Obstet. Gynaecol. 2018, 51, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Zondervan, K.T.; Becker, C.M.; Missmer, S.A. Endometriosis. N. Engl. J. Med. 2020, 382, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Simoens, S.; Dunselman, G.; Dirksen, C.; Hummelshoj, L.; Bokor, A.; Brandes, I.; Brodszky, V.; Canis, M.; Colombo, G.L.; DeLeire, T.; et al. The burden of endometriosis: Costs and quality of life of women with endometriosis and treated in referral centres. Hum. Reprod. 2012, 27, 1292–1299. [Google Scholar] [CrossRef]
- Huntington, A.; Gilmour, J.A. A life shaped by pain: Women and endometriosis. J. Clin. Nurs. 2005, 14, 1124–1132. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Kennedy, S.; Barnard, A.; Wong, J.; Jenkinson, C. Development of an endometriosis quality-of-life instrument: The Endometriosis Health Profile-30. Obstet Gynecol. 2001, 98, 258–264. [Google Scholar] [CrossRef]
- van de Burgt, T.J.; Hendriks, J.C.; Kluivers, K.B. Quality of life in endometriosis: Evaluation of the Dutch-version Endometriosis Health Profile-30 (EHP-30). Fertil Steril. 2011, 95, 1863–1865. [Google Scholar] [CrossRef]
- Jones, G.L.; Budds, K.; Taylor, F.; Musson, D.; Raymer, J.; Churchman, D.; Kennedy, S.H.; Jenkinson, C. A systematic review to determine use of the Endometriosis Health Profiles to measure quality of life outcomes in women with endometriosis. Hum. Reprod. Update 2024, 30, 186–214. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Jenkinson, C.; Kennedy, S. Evaluating the responsiveness of the Endometriosis Health Profile Questionnaire: The EHP-30. Q. Life Res. 2004, 13, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Jenkinson, C.; Taylor, N.; Mills, A.; Kennedy, S. Measuring quality of life in women with endometriosis: Tests of data quality, score reliability, response rate and scaling assumptions of the Endometriosis Health Profile Questionnaire. Hum. Reprod. 2006, 21, 2686–2693. [Google Scholar] [CrossRef] [PubMed]
- Vincent, K.; Kennedy, S.; Stratton, P. Pain scoring in endometriosis: Entry criteria and outcome measures for clinical trials. Report from the Art and Science of Endometriosis meeting. Fertil. Steril. 2010, 93, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE guideline: Endometriosis. Hum. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef]
- Keckstein, J.; Saridogan, E.; Ulrich, U.A.; Sillem, M.; Oppelt, P.; Schweppe, K.W.; Krentel, H.; Janschek, E.; Exacoustos, C.; Malzoni, M.; et al. The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis. Acta Obstet. Gynecol. Scand. 2021, 100, 1165–1175. [Google Scholar] [PubMed]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring with a Traditional Paper-based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Control Syst. Technol. 1974, 19, 716–723. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 19 November 2024).
- Kalfas, M.; Chisari, C.; Windgassen, S. Psychosocial factors associated with pain and health-related quality of life in Endometriosis: A systematic review. Eur. J. Pain. 2022, 26, 1827–1848. [Google Scholar] [CrossRef]
- Zeppernick, F.; Zeppernick, M.; Janschek, E.; Wölfler, M.; Bornemann, S.; Holtmann, L.; Oehmke, F.; Brandes, I.; Scheible, C.M.; Salehin, D. QS ENDO Real—A Study by the German Endometriosis Research Foundation (SEF) on the Reality of Care for Patients with Endometriosis in Germany, Austria and Switzerland. Geburtshilfe Frauenheilkd. 2020, 80, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.A.; Hawe, J.; Clayton, R.D.; Garry, R. The effects and effectiveness of laparoscopic excision of endometriosis: A prospective study with 2–5 year follow-up. Hum Reprod. 2003, 18, 1922–1927. [Google Scholar] [CrossRef]
- Weir, E.; Mustard, C.; Cohen, M.; Kung, R. Endometriosis: What is the risk of hospital admission, readmission, and major surgical intervention? J. Minim. Invasive Gynecol. 2005, 12, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Shakiba, K.; Bena, J.F.; McGill, K.M.; Minger, J.; Falcone, T. Surgical treatment of endometriosis: A 7-year follow-up on the requirement for further surgery. Obstet. Gynecol. 2008, 111, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Knabben, L.; Imboden, S.; Fellmann, B.; Nirgianakis, K.; Kuhn, A.; Mueller, M.D. Urinary tract endometriosis in patients with deep infiltrating endometriosis: Prevalence, symptoms, management, and proposal for a new clinical classification. Fertil. Steril. 2015, 103, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, B.; Nassif, J.; Trompoukis, P.; Barata, S.; Wattiez, A. Prevalence and management of urinary tract endometriosis: A clinical case series. Urology 2011, 78, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Maccagnano, C.; Pellucchi, F.; Rocchini, L.; Ghezzi, M.; Scattoni, V.; Montorsi, F.; Rigatti, P.; Colombo, R. Ureteral endometriosis: Proposal for a diagnostic and therapeutic algorithm with a review of the literature. Urol. Int. 2013, 91, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bulun, S.E.; Yilmaz, B.D.; Sison, C.; Miyazaki, K.; Bernardi, L.; Liu, S.; Kohlmeier, A.; Yin, P.; Milad, M.; Wei, J. Endometriosis. Endocr. Rev. 2019, 40, 1048–1079. [Google Scholar] [CrossRef] [PubMed]
- Kiani, Z.; Simbar, M.; Hajian, S.; Zayeri, F.; Shahidi, M.; Saei Ghare Naz, M.; Ghasemi, V. The prevalence of anxiety symptoms in infertile women: A systematic review and meta-analysis. Fertil. Res. Pract. 2020, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Kiani, Z.; Simbar, M.; Hajian, S.; Zayeri, F. The prevalence of depression symptoms among infertile women: A systematic review and meta-analysis. Fertil. Res. Pract. 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ruan, X.; Lu, D.; Sheng, J.; Mueck, A.O. Effect of laparoscopic endometrioma cystectomy on anti-Müllerian hormone (AMH) levels. Gynecol. Endocrinol. 2019, 35, 494–497. [Google Scholar] [CrossRef]
- Ata, B.; Turkgeldi, E.; Seyhan, A.; Urman, B. Effect of hemostatic method on ovarian reserve following laparoscopic endometrioma excision; comparison of suture, hemostatic sealant, and bipolar dessication. A systematic review and meta-analysis. J. Minim. Invasive Gynecol. 2015, 22, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.P.W.; Law, T.S.M.; Mak, J.S.M.; Sahota, D.S.; Li, T.C. Ovarian reserve and recurrence 1 year post-operatively after using haemostatic sealant and bipolar diathermy for haemostasis during laparoscopic ovarian cystectomy. Reprod. Biomed. Online 2021, 43, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Drechsel-Grau, A.; Grube, M.; Neis, F.; Schoenfisch, B.; Kommoss, S.; Rall, K.; Brucker, S.Y.; Kraemer, B.; Andress, J. Long-Term Follow-Up Regarding Pain Relief, Fertility, and Re-Operation after Surgery for Deep Endometriosis. J. Clin. Med. 2024, 13, 5039. [Google Scholar] [CrossRef] [PubMed]
- Rindos, N.B.; Fulcher, I.R.; Donnellan, N.M. Pain and Quality of Life after Laparoscopic Excision of Endometriosis. J. Minim. Invasive Gynecol. 2020, 27, 1610–1617.e1. [Google Scholar] [CrossRef] [PubMed]
- Horton, J.; Sterrenburg, M.; Lane, S.; Maheshwari, A.; Li, T.C.; Cheong, Y. Reproductive, obstetric, and perinatal outcomes of women with adenomyosis and endometriosis: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 592–632. [Google Scholar] [CrossRef]
- Vercellini, P.; Viganò, P.; Bandini, V.; Buggio, L.; Berlanda, N.; Somigliana, E. Association of endometriosis and adenomyosis with pregnancy and infertility. Fertil. Steril. 2023, 119, 727–740. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Mean (SD) | |
|---|---|
| Age | 27.8 (8.79) |
| Pain severity (Visual analogue scale) | 7.25 (1.87) |
| Number of patients n (%) | |
| First diagnosis | 70 (40.0) |
| Previous therapy | 105 (60.0) |
| Current therapy | |
| None | 99 (56.6) |
| Endocrine therapy | 63 (36.0) |
| Analgesia | 13 (7.4) |
| Typical endometriosis symptoms | |
| Dysmenorrhoea | 169 (96.6) |
| Dyspareunia | 67 (38.3) |
| Dysuria | 18 (10.3) |
| Dyschezia | 33 (18.9) |
| Main complaints | |
| Pain | 167 (95.3) |
| Findings requiring clarification | 4 (2.3) |
| Follow-up | 9 (5.1) |
| Persistent endometriosis | 25 (14.3) |
| Recurrence | 23 (13.1) |
| Desire to have children | 34 (19.4) |
| Operations | |
| Previous abdominal surgery | 78 (44.6) |
| Previous endometriosis surgery | 60 (34.3) |
| Previous histological confirmation of endometriosis | 58 (33.1) |
| Location of endometriosis diagnosis | |
| Peritoneal (#ENZIAN P) | 111 (63.4) |
| Ovary (#ENZIAN O) | 10 (5.7) |
| Deep infiltrating endometriosis (#ENZIAN A/B/C) | 20 (11.4) |
| Adenomyosis uteri (#ENZIAN FA) | 74 (42.3) |
| Planned procedure | |
| Surgical therapy | 62 (35.4) |
| Drug-based pain therapy/analgesia | 17 (9.7) |
| Reproductive medicine | 5 (2.9) |
| Endocrine therapy | 127 (72.6) |
| Multiple R2 | |||
|---|---|---|---|
| Pain | Estimates | p-Values | R2 = 0.40 |
| Visual analogue scale pain | 6.27 | <0.0001 | |
| Dysuria | 15.10 | <0.001 | |
| Pain | −11.55 | 0.133 | |
| Persistent endometriosis | 11.69 | <0.01 | |
| Desire to have children | −11.13 | <0.001 | |
| Previous endometritis surgery | −5.56 | 0.087 | |
| Control and powerlessness | R2 = 0.32 | ||
| Visual analogue scale pain | 5.63 | <0.0001 | |
| Dysmenorrhoea | −13.47 | 0.151 | |
| Dysuria | 16.07 | <0.001 | |
| Follow-up | 17.51 | <0.05 | |
| Persistent endometriosis | 15.40 | <0.01 | |
| Previous abdominal surgery | 8.63 | 0.079 | |
| Previous endometriosis surgery | −8.03 | 0.152 | |
| Peritoneal endometriosis | 7.91 | <0.05 | |
| Adenomyosis uteri | 5.24 | <0.01 | |
| Emotional well-being | R2 = 0.18 | ||
| Age | −0.38 | <0.05 | |
| Visual analogue scale pain | 3.00 | <0.01 | |
| Dysuria | 10.48 | <0.05 | |
| Pain | −14.60 | 0.095 | |
| Findings requiring clarification | 14.28 | 0.147 | |
| Recurrence | −7.41 | 0.150 | |
| Previous abdominal surgery | 14.16 | <0.01 | |
| Previous endometriosis surgery | −9.43 | 0.084 | |
| Ovary | 16.09 | <0.05 | |
| Reproductive medicine | 12.62 | 0.141 | |
| Social support | R2 = 0.14 | ||
| Dysuria | 14.57 | <0.05 | |
| Persistent endometriosis | 8.04 | 0.129 | |
| Recurrence | −14.21 | <0.05 | |
| Ovary | 19.03 | <0.05 | |
| Surgical therapy | 15.92 | <0.001 | |
| Endocrine therapy | 9.84 | 0.053 | |
| Self-image | R2 = 0.052 | ||
| First diagnosis | −6.89 | 0.156 | |
| Previous abdominal surgery | 18.90 | <0.01 | |
| Previous endometriosis surgery | −18.89 | <0.05 |
| MAE (Mean Absolute Error)/Leave One Out | RMSE (Root Mean Square Error)/Leave One Out | |||
|---|---|---|---|---|
| Performance Metrics Multivariate Linear Regression | Performance Metrics Random Forest | Performance Metrics Multivariate Linear Regression | Performance Metrics Random Forest | |
| Pain | 13.68 | 14.25 | 16.80 | 17.70 |
| Control and Powerlessness | 15.65 | 16.55 | 19.54 | 20.51 |
| Emotional well-being | 15.07 | 15.79 | 19.04 | 19.90 |
| Social support | 19.42 | 19.77 | 24.28 | 24.75 |
| Self-image | 22.39 | 22.40 | 26.05 | 26.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kupec, T.; Kennes, L.N.; Senger, R.; Meyer-Wilmes, P.; Najjari, L.; Stickeler, E.; Wittenborn, J. The Multifactorial Burden of Endometriosis: Predictors of Quality of Life. J. Clin. Med. 2025, 14, 323. https://doi.org/10.3390/jcm14020323
Kupec T, Kennes LN, Senger R, Meyer-Wilmes P, Najjari L, Stickeler E, Wittenborn J. The Multifactorial Burden of Endometriosis: Predictors of Quality of Life. Journal of Clinical Medicine. 2025; 14(2):323. https://doi.org/10.3390/jcm14020323
Chicago/Turabian StyleKupec, Tomas, Lieven Nils Kennes, Rebecca Senger, Philipp Meyer-Wilmes, Laila Najjari, Elmar Stickeler, and Julia Wittenborn. 2025. "The Multifactorial Burden of Endometriosis: Predictors of Quality of Life" Journal of Clinical Medicine 14, no. 2: 323. https://doi.org/10.3390/jcm14020323
APA StyleKupec, T., Kennes, L. N., Senger, R., Meyer-Wilmes, P., Najjari, L., Stickeler, E., & Wittenborn, J. (2025). The Multifactorial Burden of Endometriosis: Predictors of Quality of Life. Journal of Clinical Medicine, 14(2), 323. https://doi.org/10.3390/jcm14020323