
Nurse-Led, Remote Optimisation of Guideline-Directed Medical Therapy in Patients with Heart Failure and Reduced Ejection Fraction Across Australia
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Patient Recruitment and Natural Language Processing
2.3. Nurse-Led Titration Program
2.4. Program Coordination
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
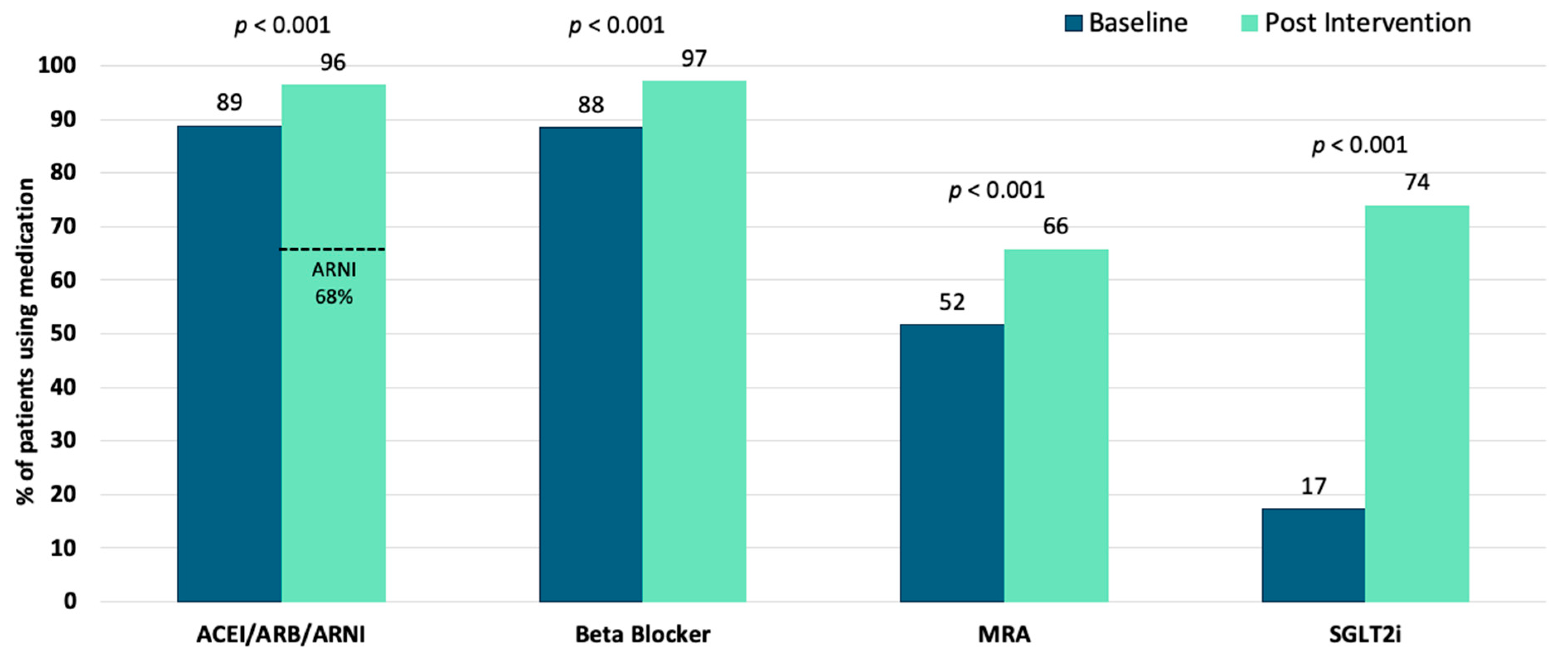
3.2. Four-Pillar Therapy Uptake
3.3. Barriers to Four-Pillar Therapy Uptake
3.4. Association Between Left Ventricular Ejection Fraction and Four-Pillar Therapy
3.5. Program Delivery Resources
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 4P-HF | Four-pillar heart failure |
| AI | Artificial intelligence |
| ACEI | Angiotensin converting enzyme inhibitor |
| ARB | Angiotensin receptor blocker |
| ARNI | Angiotensin receptor blocker–neprilysin inhibitor |
| BB | Beta blocker |
| CKD | Chronic kidney disease |
| EF | Ejection fraction |
| EMR | Electronic medical record |
| GDMT | Guideline directed medical therapy |
| HFrEF | Heart failure with reduced ejection fraction |
| HF | Heart failure |
| IQR | Interquartile range |
| LVEF | Left ventricular ejection fraction |
| NYHA | New York Heart Association |
| MRA | Mineralocorticoid receptor antagonist |
| NLP | Natural language processing |
| NT-proBNP | N-terminal prohormone of brain natriuretic peptide |
| RCT | Randomised control trial |
| SD | Standard deviation |
| SGLT2i | Sodium–glucose cotransporter 2 inhibitor |
| TTE | Transthoracic echocardiogram |
References
- Somaratne, J.B.; Berry, C.; McMurray, J.J.; Poppe, K.K.; Doughty, R.N.; Whalley, G.A. The prognostic significance of heart failure with preserved left ventricular ejection fraction: A literature-based meta-analysis. Eur. J. Heart Fail. 2009, 11, 855–862. [Google Scholar] [CrossRef]
- Chan, Y.K.; Tuttle, C.; Ball, J.; Teng, T.K.; Ahamed, Y.; Carrington, M.J.; Stewart, S. Current and projected burden of heart failure in the Australian adult population: A substantive but still ill-defined major health issue. BMC Health Serv. Res. 2016, 16, 501. [Google Scholar] [CrossRef]
- Chan, Y.-K.; Gerber, T.; Tuttle, C.; Ball, J.; Teng, T.-H.K.; Ahamed, Y.; Carrington, M. Rediscovering Heart Failure: The Contemporary Burden and Profile of Heart Failure in Australia; Baker IDI Heart and Diabetes Institute: Melbourne, Australia, 2015. [Google Scholar]
- Tromp, J.; Ouwerkerk, W.; van Veldhuisen, D.J.; Hillege, H.L.; Richards, A.M.; van der Meer, P.; Anand, I.S.; Lam, C.S.; Voors, A.A. A systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. Heart Fail. 2022, 10, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Germinal, K.; Milfort, A.; Chen, W.-H.; Chang, S.-H.; Huang, W.; Li, Y.; Lu, Y.; Ahmed, M.M.; Kimmel, S.E. The most effective combination of pharmacological therapy for heart failure with reduced ejection fraction: A network meta-analysis of randomized controlled trials. BMC Cardiovasc. Disord. 2024, 24, 666. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Sindone, A.P.; De Pasquale, C.; Amerena, J.; Burdeniuk, C.; Chan, A.; Coats, A.; Hare, D.L.; Macdonald, P.; Sverdlov, A.; Atherton, J.J. Consensus statement on the current pharmacological prevention and management of heart failure. Med. J. Aust. 2022, 217, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; Voors, A.A. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet 2022, 400, 1938–1952. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O. 2023 focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef]
- Packer, M.; McMurray, J.J. Rapid evidence-based sequencing of foundational drugs for heart failure and a reduced ejection fraction. Eur. J. Heart Fail. 2021, 23, 882–894. [Google Scholar] [CrossRef]
- Harrington, J.; Leyva, M.; Rao, V.N.; Oakes, M.; Osude, N.; Bosworth, H.B.; Pagidipati, N.J. Implementing guideline-directed medical therapy: Stakeholder-identified barriers and facilitators. Am. Heart J. 2025, 281, 23–31. [Google Scholar] [CrossRef]
- Greene, S.J.; Butler, J.; Albert, N.M.; DeVore, A.D.; Sharma, P.P.; Duffy, C.I.; Hill, C.L.; McCague, K.; Mi, X.; Patterson, J.H.; et al. Medical Therapy for Heart Failure With Reduced Ejection Fraction: The CHAMP-HF Registry. J. Am. Coll. Cardiol. 2018, 72, 351–366. [Google Scholar] [CrossRef]
- Cowie, M.R.; Schöpe, J.; Wagenpfeil, S.; Tavazzi, L.; Böhm, M.; Ponikowski, P.; Anker, S.D.; Filippatos, G.S.; Komajda, M.; Investigators, Q. Patient factors associated with titration of medical therapy in patients with heart failure with reduced ejection fraction: Data from the QUALIFY international registry. ESC Heart Fail. 2021, 8, 861–871. [Google Scholar] [CrossRef]
- Berry, N.C.; Sheu, Y.S.; Chesbrough, K.; Bishop, R.C.; Vupputuri, S. Guideline-directed medical therapy rates in heart failure patients with reduced ejection fraction in a diverse cohort. ESC Heart Fail. 2025, 12, 1861–1871. [Google Scholar] [CrossRef]
- Brunner-La Rocca, H.P.; Linssen, G.C.; Smeele, F.J.; van Drimmelen, A.A.; Schaafsma, H.J.; Westendorp, P.H.; Rademaker, P.C.; van de Kamp, H.J.; Hoes, A.W.; Brugts, J.J.; et al. Contemporary Drug Treatment of Chronic Heart Failure With Reduced Ejection Fraction: The CHECK-HF Registry. JACC Heart Fail. 2019, 7, 13–21. [Google Scholar] [CrossRef]
- Greene, S.J.; Ayodele, I.; Pierce, J.B.; Khan, M.S.; Lewsey, S.C.; Yancy, C.W.; Alhanti, B.; Van Spall, H.G.; Allen, L.A.; Fonarow, G.C. Eligibility and projected benefits of rapid initiation of quadruple therapy for newly diagnosed heart failure. Heart Fail. 2024, 12, 1365–1377. [Google Scholar] [CrossRef]
- Malgie, J.; Wilde, M.I.; Clephas, P.R.D.; Emans, M.E.; Koudstaal, S.; Schaap, J.; Mosterd, A.; van Ramshorst, J.; Wardeh, A.J.; van Wijk, S.; et al. Contemporary guideline-directed medical therapy in de novo, chronic, and worsening heart failure patients: First data from the TITRATE-HF study. Eur. J. Heart Fail. 2024, 26, 1549–1560. [Google Scholar] [CrossRef]
- Savarese, G.; Lindberg, F.; Christodorescu, R.M.; Ferrini, M.; Kumler, T.; Toutoutzas, K.; Dattilo, G.; Bayes-Genis, A.; Moura, B.; Amir, O.; et al. Physician perceptions, attitudes, and strategies towards implementing guideline-directed medical therapy in heart failure with reduced ejection fraction. A survey of the Heart Failure Association of the ESC and the ESC Council for Cardiology Practice. Eur. J. Heart Fail. 2024, 26, 1408–1418. [Google Scholar] [CrossRef]
- Phillips, L.S.; Branch Jr, W.T.; Cook, C.B.; Doyle, J.P.; El-Kebbi, I.M.; Gallina, D.L.; Miller, C.D.; Ziemer, D.C.; Barnes, C.S. Clinical inertia. Ann. Intern. Med. 2001, 135, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Swat, S.A.; Helmkamp, L.J.; Tietbohl, C.; Thompson, J.S.; Fitzgerald, M.; McIlvennan, C.K.; Harger, G.; Ho, P.M.; Ahmad, F.S.; Ahmad, T. Clinical inertia among outpatients with heart failure: Application of treatment nonintensification taxonomy to EPIC-HF trial. Heart Fail. 2023, 11, 1579–1591. [Google Scholar] [CrossRef]
- Gottlieb, S.H. Clinical Inertia Disturbs the Harmonious Treatment of Heart Failure. JACC Heart Fail. 2023, 11, 1592–1594. [Google Scholar] [CrossRef] [PubMed]
- Malgie, J.; Clephas, P.R.; Brunner-La Rocca, H.-P.; de Boer, R.A.; Brugts, J.J. Guideline-directed medical therapy for HFrEF: Sequencing strategies and barriers for life-saving drug therapy. Heart Fail. Rev. 2023, 28, 1221–1234. [Google Scholar] [CrossRef]
- Trinkley, K.E.; Dafoe, A.; Malone, D.C.; Allen, L.A.; Huebschmann, A.; Khazanie, P.; Lunowa, C.; Matlock, D.C.; Suresh, K.; Rosenberg, M.A.; et al. Clinician challenges to evidence-based prescribing for heart failure and reduced ejection fraction: A qualitative evaluation. J. Eval. Clin. Pract. 2023, 29, 1363–1371. [Google Scholar] [CrossRef]
- Schuuring, M.J.; Treskes, R.W.; Castiello, T.; Jensen, M.T.; Casado-Arroyo, R.; Neubeck, L.; Lyon, A.R.; Keser, N.; Rucinski, M.; Marketou, M.; et al. Digital solutions to optimize guideline-directed medical therapy prescription rates in patients with heart failure: A clinical consensus statement from the ESC Working Group on e-Cardiology, the Heart Failure Association of the European Society of Cardiology, the Association of Cardiovascular Nursing & Allied Professions of the European Society of Cardiology, the ESC Digital Health Committee, the ESC Council of Cardio-Oncology, and the ESC Patient Forum. Eur. Heart J. Digit. Health 2024, 5, 670–682. [Google Scholar] [CrossRef]
- Ahmed, M.; Shafiq, A.; Zahid, M.; Dhawadi, S.; Javaid, H.; Rehman, M.E.U.; Chachar, M.A.; Siddiqi, A.K. Clinical outcomes with nurse-coordinated multidisciplinary care in patients with heart failure: A systematic review and meta-analysis. Curr. Probl. Cardiol. 2024, 49, 102041. [Google Scholar] [CrossRef]
- Weinstein, J.M.; Greenberg, D.; Sharf, A.; Simon-Tuval, T. The impact of a community-based heart failure multidisciplinary team clinic on healthcare utilization and costs. ESC Heart Fail. 2022, 9, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, A.; Meagher, S.; Kennedy, R.; Currey, J. Effect of intensive nurse-led optimization of heart failure medications in patients with heart failure: A meta-analysis of randomized controlled trials. J. Cardiovasc. Nurs. 2023, 10, 1097. [Google Scholar] [CrossRef] [PubMed]
- Atherton, J.J.; Sindone, A.; De Pasquale, C.G.; Driscoll, A.; MacDonald, P.S.; Hopper, I.; Kistler, P.M.; Briffa, T.; Wong, J.; Abhayaratna, W. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Guidelines for the prevention, detection, and management of heart failure in Australia 2018. Heart Lung Circ. 2018, 27, 1123–1208. [Google Scholar] [CrossRef]
- Man, J.P.; Klopotowska, J.; Asselbergs, F.W.; Handoko, M.L.; Chamuleau, S.A.; Schuuring, M.J. Digital solutions to optimize guideline-directed medical therapy prescriptions in heart failure patients: Current applications and future directions. Curr. Heart Fail. Rep. 2024, 21, 147–161. [Google Scholar] [CrossRef]
- Idris-Agbabiaka, A.; Anjum, M.M.; Semy, M.; Rath, S.; Rizwan, M.; Victoria, O.O.; Anwar, A.; Abiodun, I.F.; Ashinze, P. AI-assisted heart failure management: A review of clinical applications, case studies, and future directions. Glob. Cardiol. Sci. Pract. 2025, 2025. [Google Scholar] [CrossRef]
- AIHW. Health System Overview; AIHW: Canberra, Australia, 2024.
- Atlay, K. Dapagliflozin for HFrEF Fast-Tracked onto PBS. Available online: https://www.ausdoc.com.au/news/dapagliflozin-hfref-fasttracked-pbs/?utm_source=chatgpt.com (accessed on 20 July 2025).
- Heart Foundation. Clinical Fact Sheet: Pharmacological Management of Chronic Heart Failure with Reduced Left Ventricular Ejection Fraction (HFrEF); Heart Foundation Website—Resources to Support Patients with Heart Failure: Canberra, Australia, 2019; p. 3. [Google Scholar]
- Marti, C.N.; Fonarow, G.C.; Anker, S.D.; Yancy, C.; Vaduganathan, M.; Greene, S.J.; Ahmed, A.; Januzzi, J.L.; Gheorghiade, M.; Filippatos, G. Medication dosing for heart failure with reduced ejection fraction—Opportunities and challenges. Eur. J. Heart Fail. 2019, 21, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Shahim, A.; Linde, C.; Savarese, G.; Dahlström, U.; Lund, L.H.; Hage, C. Implementation of guideline-recommended therapies in heart failure with reduced ejection fraction according to heart failure duration: An analysis of 55 581 patients from the Swedish Heart Failure (SwedeHF) Registry. Eur. J. Heart Fail. 2025, 27, 421–431. [Google Scholar] [CrossRef]
- Agrawal, S.; Alhaddad, Z.; Nabia, S.; Rehman, O.U.; Kiyani, M.; Kumar, A.; Regmi, N.; Pingili, A.; GARG, T.; Allamaneni, R. Prescription Patterns in Management of Heart Failure and Its Association With Readmissions: A Retrospective Analysis. J. Card. Fail. 2025, 31, 635–645. [Google Scholar] [CrossRef]
- Paolillo, S.; Basile, C.; Marzano, F.; Bruzzese, D.; Agostoni, P.; Mattavelli, I.; Aloisio, A.; Ameri, P.; Solimano, M.; Brunetti, N.D. Implementation of guideline-directed medical therapy in patients with heart failure with reduced ejection fraction (OpTIMa-HF Registry). ESC Heart Fail. 2025, 12, 1786–1795. [Google Scholar] [CrossRef]
- Laborante, R.; Delvinioti, A.; Tudor, A.M.; Lenkowicz, J.; Iacomini, C.; Iaconelli, A.; Paglianiti, D.A.; Galli, M.; Rodolico, D.; Patarnello, S. Temporal trends in guideline-recommended medical therapy after an acute heart failure decompensation event: An observational analysis from Generator Heart Failure DataMart. BMJ Open 2025, 15, e088998. [Google Scholar] [CrossRef]
- Malgie, J.; Wilde, M.I.; Brunner-La Rocca, H.-P.; Emans, M.E.; De Boer, G.A.; Siegers, C.E.; van Stipdonk, A.M.; Wardeh, A.J.; Schaap, J.; Sanders-van Wijk, S. Newly diagnosed heart failure with reduced ejection fraction: Timing, sequencing, and titration of guideline-recommended medical therapy. Eur. Heart J. 2025, 46, 2394–2405. [Google Scholar] [CrossRef] [PubMed]
- Vasudevan, S.; Thayaparan, A.; Teng, L.E.; Lammoza, N.; Aung, A.K.; Edwards, G.; Gibbs, H.; Hopper, I. Physician Perceptions of Medication Prescribing in Heart Failure: A Scoping Review. Cardiology 2025, 150, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Kocabas, U.; Ergin, I.; Yavuz, V.; Altın, C.; Kaplan, M.; Yılmaz Öztekin, G.M.; Doğduş, M.; Murat, S.; Murat, B.; Kıvrak, T. Real-world data on Empagliflozin and Dapagliflozin use in patients with HEART failure: The RED–HEART study. ESC Heart Fail. 2025, 12, 434–446. [Google Scholar] [CrossRef]
- McGrane, S.; Lloyd, R.; Potts, C.; Ang, R.J. Prescribing Patterns of Guideline-Directed Medical Therapy for Heart Failure with Reduced Ejection Fraction: A Comparison Between Cardiology and General Medicine. Researh Clin. Pharm. 2024, 2, 27–37. [Google Scholar] [CrossRef]
- Nakamaru, R.; Kohsaka, S.; Shiraishi, Y.; Kohno, T.; Goda, A.; Nagatomo, Y.; Kitamura, M.; Nakano, S.; Takei, M.; Mizuno, A. Temporal trends in heart failure management and outcomes: Insights from a Japanese multicenter registry of tertiary care centers. J. Am. Heart Assoc. 2023, 12, e031179. [Google Scholar] [CrossRef] [PubMed]
- Berge, K.; Schirmer, H.; Øvrebotten, T.; Nahoui, H.; Gullestad, L.; Ingul, C.B.; Hole, T.; Mo, R.; Larsby, K.; Norekvål, T.M. Improvements in medical therapy and prognosis for patients with HFrEF following the 2021 ESC HF guidelines. ESC Heart Fail. 2025. [Google Scholar] [CrossRef]
- Dickstein, K.; Cohen-Solal, A.; Filippatos, G.; McMurray, J.J.V.; Ponikowski, P.; Poole-Wilson, P.A.; Strömberg, A.; van Veldhuisen, D.J.; Atar, D.; Hoes, A.W.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008 ‡: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur. Heart J. 2008, 29, 2388–2442. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.A.; Abraham, W.T.; Chin, M.H.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Jessup, M.; Konstam, M.A.; Mancini, D.M.; Michl, K.; et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). Circulation 2005, 112, e154–e235. [Google Scholar] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Wu, X.; Li, Z.; Tian, Q.; Ji, S.; Zhang, C. Effectiveness of nurse-led heart failure clinic: A systematic review. Int. J. Nurs. Sci. 2024, 11, 315–329. [Google Scholar] [CrossRef]
- Johnson, A.E.; Brewer, L.C.; Echols, M.R.; Mazimba, S.; Shah, R.U.; Breathett, K. Utilizing artificial intelligence to enhance health equity among patients with heart failure. Heart Fail. Clin. 2022, 18, 259–273. [Google Scholar] [CrossRef]
- AIHW. Heart, Stroke and Vascular Disease: Australian Facts. Available online: https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/hsvd-facts/contents/all-heart-stroke-and-vascular-disease/heart-failure-and-cardiomyopathy (accessed on 19 July 2025).
- Clark, R.A.; Driscoll, A.; Nottage, J.; McLennan, S.; Coombe, D.M.; Bamford, E.J.; Wilkinson, D.; Stewart, S. Inequitable provision of optimal services for patients with chronic heart failure: A national geo-mapping study. Med. J. Aust. 2007, 186, 169–173. [Google Scholar] [CrossRef]
- Man, J.P.; Koole, M.A.; Meregalli, P.G.; Handoko, M.L.; Stienen, S.; de Lange, F.J.; Winter, M.M.; Schijven, M.P.; Kok, W.E.; Kuipers, D.I. Digital consults in heart failure care: A randomized controlled trial. Nat. Med. 2024, 30, 2907–2913. [Google Scholar] [CrossRef]
- Vijay, A.; Yancy, C.W. Health equity in heart failure. Prog. Cardiovasc. Dis. 2024, 82, 55–60. [Google Scholar] [CrossRef]
- McKee, G.; Kerins, M.; Hamilton, G.; Hansen, T.; Hendriks, J.; Kletsiou, E.; Lambrinou, E.; Jennings, C.; Fitzsimons, D. Barriers to ESC guideline implementation: Results of a survey from the European Council on Cardiovascular Nursing and Allied Professions (CCNAP). Eur. J. Cardiovasc. Nurs. 2017, 16, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.; Rao, V.N.; Leyva, M.; Oakes, M.; Mentz, R.J.; Bosworth, H.B.; Pagidipati, N.J. Improving guideline-directed medical therapy for patients with heart failure with reduced ejection fraction: A review of implementation strategies. J. Card. Fail. 2024, 30, 376–390. [Google Scholar] [CrossRef]
- Tang, A.B.; Brownell, N.K.; Roberts, J.S.; Haidar, A.; Osuna-Garcia, A.; Cho, D.J.; Bokhoor, P.; Fonarow, G.C. Interventions for optimization of guideline-directed medical therapy: A systematic review. JAMA Cardiol. 2024, 9, 397–404. [Google Scholar] [CrossRef]
- Mukhopadhyay, A.; Reynolds, H.R.; Phillips, L.M.; Nagler, A.R.; King, W.C.; Szerencsy, A.; Saxena, A.; Aminian, R.; Klapheke, N.; Horwitz, L.I. Cluster-randomized trial comparing ambulatory decision support tools to improve heart failure care. J. Am. Coll. Cardiol. 2023, 81, 1303–1316. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, J.M.; Jaarsma, T. The multidisciplinary team approach in cardiovascular care. Eur. J. Cardiovasc. Nurs. 2021, 20, 91–92. [Google Scholar] [CrossRef]
- Saposnik, G.; Redelmeier, D.; Ruff, C.C.; Tobler, P.N. Cognitive biases associated with medical decisions: A systematic review. BMC Med. Inform. Decis. Mak. 2016, 16, 138. [Google Scholar] [CrossRef]
- Mayer, J.; Kipps, C.; Cock, H.R. Implementing clinical guidelines. Pract. Neurol. 2019, 19, 529–535. [Google Scholar] [CrossRef]
- Nargesi, A.A.; Adejumo, P.; Dhingra, L.S.; Rosand, B.; Hengartner, A.; Coppi, A.; Benigeri, S.; Sen, S.; Ahmad, T.; Nadkarni, G.N. Automated identification of heart failure with reduced ejection fraction using deep learning-based natural language processing. Heart Fail. 2025, 13, 75–87. [Google Scholar] [CrossRef]
- Adair, J.G. The Hawthorne effect: A reconsideration of the methodological artifact. J. Appl. Psychol. 1984, 69, 334. [Google Scholar] [CrossRef]
- Reath, J.S.; O’Mara, P. Closing the gap in cardiovascular risk for Aboriginal and Torres Strait Islander Australians. Med. J. Aust. 2018, 209, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Ledwidge, M.; Barry, M.; Cahill, J.; Ryan, E.; Maurer, B.; Ryder, M.; Travers, B.; Timmons, L.; McDonald, K. Is multidisciplinary care of heart failure cost-beneficial when combined with optimal medical care? Eur. J. Heart Fail. 2003, 5, 381–389. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Data | Intervention Baseline n = 2004 1 | Post Intervention n = 2004 | p-Value |
|---|---|---|---|
| Age, years | 72.7 ± 11.6 | - | - |
| Male | 1444 (72.1) | - | - |
| Regional | 732 (36.5) | - | - |
| Metropolitan | 1271 (63.5) | - | - |
| LVEF, % | 38.2 ± 10.8 | - | - |
| eGFR mL/min/1.73 m2 (n = 1612) | 61.3 ± 19.8 | - | - |
| CKD4-5 | 95 (5.9) | - | - |
| Diabetes Mellitus (n = 1085) | 187 (17.2) | - | - |
| Medication class used | |||
| ACEI/ARB/ARNI | 1779 (88.8) | 1932 (96.4) | <0.001 |
| ACEI/ARB | - | 573 (28.6) | |
| ARNI | - | 1359 (67.8) | |
| BB | 1771 (88.4) | 1944 (97.0) | <0.001 |
| MRA | 1035 (51.6) | 1316 (65.7) | <0.001 |
| SGLT2i | 347 (17.3) | 1481 (73.9) | <0.001 |
| Number of heart failure medications | |||
| 0 | 55 (2.7) | 3 (0.1) | <0.001 |
| 1 | 221 (11.0) | 27 (1.3) | <0.001 |
| 2 | 712 (35.5) | 274 (13.7) | <0.001 |
| 3 | 794 (39.6) | 702 (35.0) | 0.003 |
| 4 | 222 (11.1) | 998 (49.8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freedman, G.; Watt, R.; Chowdhury, E.K.; Quinlan, K.; Eccleston, D.; Driscoll, A.; Theuerle, J.; Kearney, L. Nurse-Led, Remote Optimisation of Guideline-Directed Medical Therapy in Patients with Heart Failure and Reduced Ejection Fraction Across Australia. J. Clin. Med. 2025, 14, 5371. https://doi.org/10.3390/jcm14155371
Freedman G, Watt R, Chowdhury EK, Quinlan K, Eccleston D, Driscoll A, Theuerle J, Kearney L. Nurse-Led, Remote Optimisation of Guideline-Directed Medical Therapy in Patients with Heart Failure and Reduced Ejection Fraction Across Australia. Journal of Clinical Medicine. 2025; 14(15):5371. https://doi.org/10.3390/jcm14155371
Chicago/Turabian StyleFreedman, Gabrielle, Racheal Watt, Enayet Karim Chowdhury, Kate Quinlan, David Eccleston, Andrea Driscoll, James Theuerle, and Leighton Kearney. 2025. "Nurse-Led, Remote Optimisation of Guideline-Directed Medical Therapy in Patients with Heart Failure and Reduced Ejection Fraction Across Australia" Journal of Clinical Medicine 14, no. 15: 5371. https://doi.org/10.3390/jcm14155371
APA StyleFreedman, G., Watt, R., Chowdhury, E. K., Quinlan, K., Eccleston, D., Driscoll, A., Theuerle, J., & Kearney, L. (2025). Nurse-Led, Remote Optimisation of Guideline-Directed Medical Therapy in Patients with Heart Failure and Reduced Ejection Fraction Across Australia. Journal of Clinical Medicine, 14(15), 5371. https://doi.org/10.3390/jcm14155371