
Molecular Mechanisms Underlying Inflammation in Early-Onset Neonatal Sepsis: A Systematic Review of Human Studies

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
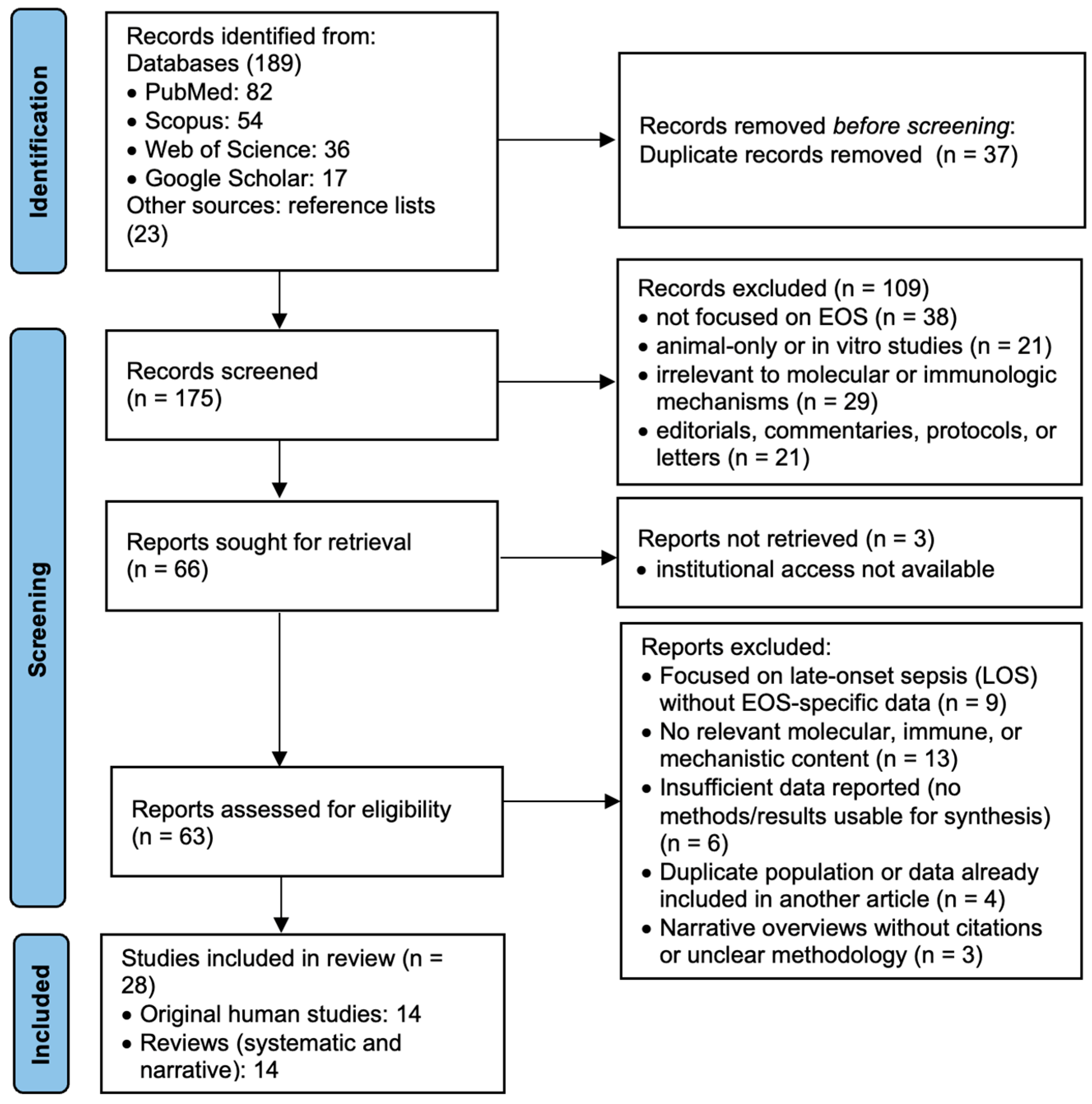
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
- Population: human studies involving neonates (≤72 h old) with either confirmed or suspected early-onset sepsis.
- Content: articles that described molecular mechanisms, biomarkers, immune signaling pathways, or host–pathogen interaction related to EOS.
- Study type: original research articles and review articles.
- Period: published between 1 January 2015 and 31 January 2025.
- Language: English.
- Setting: studies conducted in hospitals or clinical laboratories, or translational research settings involving human neonatal samples (e.g., cord blood, serum, cells).
- Studies focused exclusively on late-onset sepsis (LOS).
- Studies that were based solely on animal models or in vitro experiments without direct human relevance.
- Reported clinical outcomes without addressing molecular, immunological, or mechanistic data.
- Studies which were categorized as editorials, letters, or commentaries without original data or formal review.
- (1)
- Direct—studies that explicitly addressed molecular or immunological mechanisms in early-onset neonatal sepsis (≤72 h).
- (2)
- Partial—studies that included both EOS and other forms of neonatal sepsis but presented stratified or relevant data for EOS.
- (3)
- Indirect—studies addressing related molecular pathways in neonatal immune responses without a clear focus on EOS.
- (4)
- Conceptual—theoretical or narrative articles discussing inflammation or sepsis frameworks applicable to the EOS context.

{kind=link}
| Author(s) | Study Type | Year and Country | Population Characteristics | Sample Size | EOS Definition | Molecular Targets/Pathways | EOS-Specific Relevance | Key Findings |
|---|---|---|---|---|---|---|---|---|
| Marchant et al. [28] | Original | 2015, Canada | Preterm neonates | 45 p | Clinical EOS, based on CDC guidelines | TLR2, TLR4, cytokines (IL-6, TNF-α) | Direct | Preterm neonates show impaired TLR responses and cytokine production. |
| Nakstad et al. [29] | Original | 2016, Norway | Cord blood model | 30 | In vitro stimulation model mimicking EOS | TLRs, IL-6 | Direct | Cord blood IL-6 response enables early GBS detection. |
| Dias et al. [30] | Review | 2021, Ireland | Narrative—humans | Not applicable | Not uniformly specified across studies included | TLR signaling | Direct | TLR pathways are promising targets for neonatal immune modulation. |
| Shane et al. [31] | Review | 2017, USA | Neonates—global data | N/A | Mixed (includes EOS and LOS, not always specified) | Immune mediators | Direct | Summarizes immune deficits, diagnostics, and pathogens in EOS. |
| Dong & Speer [32] | Review | 2015, Germany | Neonatal sepsis, all types | N/A | Includes both EOS and LOS, focus more on LOS | Immune maturation | Partial | Describes immune development affecting sepsis response. |
| Sweeney et al. [33] | Review | 2017, Australia | Perinatal infections | N/A | Broad perinatal infection model; no strict EOS separation | Microbial virulence factors | Partial | Details pathogen virulence mechanisms relevant to perinatal sepsis. |
| Raymond et al. [34] | Original | 2017, USA | Neonates, immune suppression | 36 | Clinical EOS (culture not required) | Cytokines, immune exhaustion | Direct | Highlights immune exhaustion and cytokine dysregulation in EOS. |
| Khaertynov et al. [35] | Original | 2017, Russia | Neonates with EOS vs. LOS | 58 (30 EOS, 28 LOS) | Culture-confirmed EOS (within 72 h) | Cytokines (IL-6, TNF-α) | Direct | EOS features elevated IL-6 and TNF-α vs. LOS. |
| Wynn & Wong [36] | Review | 2016, USA | Theoretical/Review | N/A | Not applied to specific patients | TLRs, NF-κB | Indirect | Explains role of TLRs and NF-κB in inflammation. |
| Ershad et al. [37] | Review | 2019, USA | General neonatal population | N/A | Includes sepsis in neonates; not limited to EOS | General cytokines | Partial | Describes cytokine profiles in neonatal infections. |
| Dong [38] | Review | 2019, Germany | Narrative neonatal focus | N/A | Includes EOS and general neonatal sepsis | Inflammation and immunity | Partial | Reviews inflammation and immune mechanisms in neonatal sepsis. |
| Hibbert et al. [39] | Original | 2018, Australia | Preterm and term neonates | 42 | Clinical diagnosis, based on signs and markers | Sepsis-induced immunosuppression | Direct | Sepsis induces immune suppression even in early phases. |
| Moon et al. [40] | Original | 2021, South Korea | FGR and chorioamnionitis neonates | 40 | Clinical EOS based on signs and inflammatory markers | DAMPs, sterile inflammation | Direct | FGR and inflammation predispose neonates to EOS. |
| Vincent [41] | Review | 2023, Belgium | Theoretical/discussion | N/A | Not neonatal-specific; discusses sepsis broadly | Sepsis/infection distinction | Conceptual | Distinguishes systemic inflammation from infection in sepsis. |
| Wynn & Polin [42] | Review | 2018, USA | Neonates with suspected EOS | N/A | Includes suspected EOS; focus on definitions and frameworks | Consensus definitions | Direct | Highlights needed for EOS-specific criteria in research. |
| Conti et al. [43] | Review | 2020, Italy | Human neonatal immune pathways | N/A | Focused on neonatal inflammation; EOS included as context | Immunometabolism, TLRs | Direct | Explores metabolic modulation of inflammation in EOS. |
| Parra-Llorca et al. [44] | Original | 2023, Spain | Preterm neonates with EOS | 52 | Confirmed or suspected EOS based on clinical and microbiological data | Immune response, ROS | Direct | EOS alters microbiome, immune response, and ROS signaling. |
| Tsantes et al. [45] | Review | 2023, Greece | Neonates with coagulopathy | N/A | Includes EOS as one of several contexts for coagulation | Coagulation pathways | Direct | Reviews EOS-related coagulopathy mechanisms. |
| Gialamprinou et al. [46] | Original | 2023, Greece | EOS patients, NICU | 28 EOS cases vs. 20 controls | Culture-confirmed EOS | Coagulation, Gram-positive EOS | Direct | Finds Gram-positive EOS associated with platelet dysfunction. |
| Hensler et al. [47] | Original | 2022, USA | Neonatal immune checkpoint focus | 34 | Clinical and laboratory-confirmed EOS | Immune checkpoints | Direct | Identifies immune checkpoints as regulators in EOS. |
| Yan & Zhou [48] | Original | 2022, China | Sepsis dataset—clinical validation | 56 (bioinformatics set) + 24 validation cases | Included EOS-specific analysis based on timing and markers | mRNA biomarkers | Direct | Integrates bioinformatics with clinical data to identify key markers. |
| Luo et al. [49] | Original | 2023, China | Transcriptome in EOS neonates | 60 | Confirmed EOS by clinical/lab criteria | DEGs, immune infiltration | Direct | Identifies DEGs linked to inflammation in EOS. |
| Celik et al. [50] | Review | 2022, Turkey | Narrative EOS review | N/A | Comprehensive review focused on EOS | General inflammatory pathways | Direct | Summarizes EOS immune mechanisms and diagnostics. |
| Ruan et al. [51] | Review | 2018, China | Systematic review, neonates | Meta-analysis (15 studies, >1000 neonates) | Defined EOS as sepsis within 72 h of life | Presepsin, CRP | Direct | Supports presepsin and CRP as EOS biomarkers. |
| Jouza et al. [52] | Original | 2022, Czech Republic | Neonatal blood samples | 46 neonates (23 EOS, 23 controls) | Culture-confirmed and clinical EOS | miRNA biomarkers | Direct | miRNAs hold promise as EOS biomarkers. |
| Ng et al. [53] | Review | 2015, Hong Kong | Review of lab biomarkers | N/A | Includes EOS cases; not always separated from LOS | CRP, IL-6, PCT | Direct | Evaluates CRP, IL-6, and PCT in EOS monitoring. |
| Chauhan et al. [27] | Review | 2017, India | Narrative review EOS biomarkers | N/A | Not strictly separated; includes experimental and clinical data | Immune and lab markers | Direct | Reviews emerging EOS biomarkers in clinical settings. |
| Pietrasanta et al. [54] | Review | 2019, Italy | Review of vascular function in EOS | N/A | Includes EOS in the context of endothelial injury | Endothelial dysfunction | Direct | Links endothelial injury to EOS pathogenesis. |
| Pathogen-Induced Inflammation | Systemic Inflammation | Sterile Inflammation | Interactions Between Mechanisms | Emerging Molecular Perspectives |
|---|---|---|---|---|
| Marchant et al., 2015 [28] | Raymond et al., 2017 [34] | Moon et al., 2021 [40] | Wynn & Polin, 2018 [42] | Yan & Zhou, 2022 [48] |
| Nakstad et al., 2016 [29] | Khaertynov et al., 2017 [35] | Vincent, 2023 [41] | Conti et al., 2020 [43] | Luo et al., 2023 [49] |
| Dias et al., 2021 [30] | Wynn & Wong, 2016 [36] | Hensler et al., 2022 [47] | Celik et al., 2022 [50] | Ruan et al., 2018 [51] |
| Shane et al., 2017 [31] | Ershad et al., 2019 [37] | Pietrasanta et al., 2019 [54] | Jouza et al., 2022 [52] | |
| Dong & Speer, 2015 [32] | Dong, 2019 [38] | Ng et al., 2015 [53] | ||
| Sweeney et al., 2017 [33] | Hibbert et al., 2018 [39] | Chauhan et al., 2017 [27] | ||
| Parra-Llorca et al., 2023 [44] | ||||
| Tsantes et al., 2023 [45] | ||||
| Gialamprinou et al., 2023 [46] |
3. Results
3.1. Pathogen-Induced Inflammation
3.1.1. Toll-like Receptor Signaling in Neonates
3.1.2. Bacterial Virulence and Barrier Invasion
3.1.3. Cytokine Response and Immune Amplification
3.1.4. Diagnostic Implications and Targeted Modulation
3.2. Systemic Inflammation
3.2.1. Cytokine Storm and Immune Dysregulation
3.2.2. Endothelial Injury and Microcirculatory Instability
3.2.3. Epigenetic and Transcriptomic Regulation
3.2.4. Sepsis-Induced Immunosuppression
3.2.5. Endothelial Dysfunction and Coagulopathy
3.2.6. Organ-Specific Sequelae
3.3. Sterile Inflammation
3.3.1. Triggers and Cellular Injury
3.3.2. Role of DAMPs and Inflammasome Activation
3.3.3. Immune Checkpoints and Regulatory Failure
3.3.4. Diagnostic and Therapeutic Implications
3.4. Interactions Between Infectious and Sterile Inflammatory Pathways
3.4.1. Dual Activation of Inflammatory Pathways
3.4.2. Synergistic Cytokine Amplification
3.4.3. Implications for Barrier Integrity and Immune Priming
3.4.4. Diagnostic Complexity and Clinical Overlap
3.5. Emerging Molecular Perspectives
3.5.1. Transcriptomic and Bioinformatic Profiling
3.5.2. Diagnostic Biomarkers: CRP, Presepsin, and miRNAs
3.5.3. Immune Checkpoints and Systems-Level Modulation
3.5.4. Toward Personalized Neonatal Sepsis Care
4. Discussion
4.1. Expanding the Understanding of EOS Pathogenesis
4.2. The Role of Non-Infectious Inflammation
4.3. Interactions Between Infectious and Sterile Triggers
4.4. Diagnostic Challenges and Clinical Implications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camacho-Gonzalez, A.; Spearman, P.W.; Stoll, B.J. Neonatal Infectious Diseases: Evaluation of Neonatal Sepsis. Pediatr. Clin. N. Am. 2013, 60, 367–389. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Sánchez, P.J.; Faix, R.G.; Poindexter, B.B.; Van Meurs, K.P.; Bizzarro, M.J.; Goldberg, R.N.; Frantz, I.D.; Hale, E.C. Early-Onset Neonatal Sepsis: The Burden of Group B Streptococcal and Escherichia Coli Disease Continues. Pediatrics 2011, 127, 817–826. [Google Scholar] [CrossRef]
- Polin, R.A. Management of Neonates with Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics 2012, 129, 1006–1015. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Benitz, W.E.; Zaoutis, T.E. Management of Neonates Born at ≥35 Weeks’ Gestation with Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics 2018, 142, e20182894. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.S.; Baker, C.J. Group B Streptococcal Infections in Elderly Adults. Clin. Infect. Dis. 2005, 41, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Bizzarro, M.J.; Dembry, L.M.; Baltimore, R.S.; Gallagher, P.G. Changing Patterns in Neonatal Escherichia Coli Sepsis and Ampicillin Resistance in the Era of Intrapartum Antibiotic Prophylaxis. Pediatrics 2008, 121, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Kollmann, T.R.; Levy, O.; Montgomery, R.R.; Goriely, S. Innate Immune Function by Toll-like Receptors: Distinct Responses in Newborns and the Elderly. Immunity 2012, 37, 771–783. [Google Scholar] [CrossRef]
- Levy, O. Innate Immunity of the Newborn: Basic Mechanisms and Clinical Correlates. Nat. Rev. Immunol. 2007, 7, 379–390. [Google Scholar] [CrossRef]
- Ng, P.C.; Lam, H.S. Diagnostic Markers for Neonatal Sepsis. Curr. Opin. Pediatr. 2006, 18, 125–131. [Google Scholar] [CrossRef]
- Melville, J.M.; Moss, T.J. The Immune Consequences of Preterm Birth. Front. Neurosci. 2013, 7, 79. [Google Scholar] [CrossRef]
- Marchant, E.A.; Boyce, G.K.; Sadarangani, M.; Lavoie, P.M. Neonatal Sepsis Due to Coagulase-Negative Staphylococci. Clin. Dev. Immunol. 2013, 2013, 586076. [Google Scholar] [CrossRef]
- Vincent, J.L.; Opal, S.M.; Marshall, J.C.; Tracey, K.J. Sepsis Definitions: Time for Change. Lancet 2013, 381, 774–775. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, S.; Puopolo, K.; Zupancic, J.A.F. Noninfectious Influencers of Early-Onset Sepsis Biomarkers. Pediatr. Res. 2021, 89, 501–507. [Google Scholar] [CrossRef]
- Andersson, U.; Tracey, K.J. HMGB1 Is a Therapeutic Target for Sterile Inflammation and Infection. Annu. Rev. Immunol. 2011, 29, 139–162. [Google Scholar] [CrossRef]
- Lotze, M.T.; Zeh, H.J.; Rubartelli, A.; Sparvero, L.J.; Amoscato, A.A.; Washburn, N.R.; De Vera, M.E.; Liang, X.; Tör, M.; Billiar, T. The Grateful Dead: Damage-Associated Molecular Pattern Molecules and Reduction/Oxidation Regulate Immunity. Immunol. Rev. 2007, 220, 60–81. [Google Scholar] [CrossRef]
- Krysko, D.V.; Agostinis, P.; Krysko, O.; Garg, A.D.; Bachert, C.; Lambrecht, B.N.; Vandenabeele, P. Emerging Role of Damage-Associated Molecular Patterns Derived from Mitochondria in Inflammation. Trends Immunol. 2011, 32, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Kepp, O.; Kroemer, G. Decoding Cell Death Signals in Inflammation and Immunity. Cell 2010, 140, 798–804. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Ince, C.; Mayeux, P.R.; Nguyen, T.; Gomez, H.; Kellum, J.A.; Ospina-Tascón, G.A.; Hernandez, G.; Murray, P.; De Backer, D., on behalf of the ADQI XIV Workgroup. The Endothelium in Sepsis. Shock 2016, 45, 259–270. [Google Scholar] [CrossRef]
- Gando, S.; Levi, M.; Toh, C.H. Disseminated Intravascular Coagulation. Nat. Rev. Dis. Primer 2016, 2, 16037. [Google Scholar] [CrossRef]
- Weiss, S.L.; Peters, M.J.; Alhazzani, W.; Agus, M.S.D.; Flori, H.R.; Inwald, D.P.; Nadel, S.; Schlapbach, L.J.; Tasker, R.C.; Argent, A.C.; et al. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Intensive Care Med. 2020, 46, 10–67. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-Induced Immunosuppression: From Cellular Dysfunctions to Immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef]
- van der Poll, T.; van de Veerdonk, F.L.; Scicluna, B.P.; Netea, M.G. The Immunopathology of Sepsis and Potential Therapeutic Targets. Nat. Rev. Immunol. 2017, 17, 407–420. [Google Scholar] [CrossRef]
- Wynn, J.L.; Wong, H.R. Pathophysiology and Treatment of Septic Shock in Neonates. Clin. Perinatol. 2010, 37, 439–479. [Google Scholar] [CrossRef]
- Ng, P.C.; Ma, T.P.; Lam, H.S.; Chan, I.H.; Lee, C.H.; Wong, R.P.; Fok, T.F. The Use of Pro-Inflammatory and Anti-Inflammatory Cytokine Ratios in the Early Diagnosis and Prognosis of Neonatal Sepsis. Clin. Biochem. 2004, 37, 427–432. [Google Scholar] [CrossRef]
- Bethou, A.; Bhat, B.V. Neonatal Sepsis: Newer Insights. Indian J. Pediatr. 2022, 89, 267–273. [Google Scholar] [CrossRef]
- Chauhan, N.; Tiwari, S.; Jain, U. Potential Biomarkers for Screening Neonatal Sepsis: An Overview. Microb. Pathog. 2017, 107, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Marchant, E.A.; Kan, B.; Sharma, A.A.; van Zanten, A.; Kollmann, T.R.; Brant, R.; Lavoie, P.M. Attenuated Innate Immune Defenses in Very Premature Neonates during the Neonatal Period. Pediatr. Res. 2015, 78, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Nakstad, B.; Sonerud, T.; Solevåg, A.L. Early Detection of Neonatal Group B Streptococcus Sepsis in a Cord Blood Model. Infect. Drug Resist. 2016, 9, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Dias, M.L.; O’Connor, K.M.; Dempsey, E.M.; O’Halloran, K.D.; McDonald, F.B. Targeting the Toll-like Receptor Pathway as a Therapeutic Strategy for Neonatal Infection. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2021, 321, R879–R902. [Google Scholar] [CrossRef]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal Sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Dong, Y.; Speer, C. Late-Onset Sepsis: Recent Developments. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F257–F263. [Google Scholar] [CrossRef]
- Sweeney, E.L.; Dando, S.J.; Kallapur, S.G.; Knox, C.L. The Human Ureaplasma Species as Causative Agents of Chorioamnionitis. Clin. Microbiol. Rev. 2017, 30, 349–379. [Google Scholar] [CrossRef]
- Raymond, S.L.; Stortz, J.A.; Mira, J.-C.; Larson, S.D.; Wynn, J.L.; Moldawer, L.L. Immunological Defects in Neonatal Sepsis and Potential Therapeutic Approaches. Front. Pediatr. 2017, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- Khaertynov, K.S.; Boichuk, S.V.; Khaiboullina, S.F.; Anokhin, V.A.; Andreeva, A.A.; Lombardi, V.C.; Satrutdinov, M.A.; Agafonova, E.A.; Rizvanov, A.A. Comparative Assessment of Cytokine Pattern in Early and Late Onset of Neonatal Sepsis. J. Immunol. Res. 2017, 2017, 8601063. [Google Scholar] [CrossRef]
- Wynn, J.L.; Wong, H.R. Pathophysiology of Neonatal Sepsis. Fetal Neonatal Physiol. 2016, 12, 321–329. [Google Scholar]
- Ershad, M.; Mostafa, A.; Dela Cruz, M.; Vearrier, D. Neonatal Sepsis. Curr. Emerg. Hosp. Med. Rep. 2019, 7, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Glaser, K.; Speer, C.P. Late-onset sepsis caused by Gram-negative bacteria in very low birth weight infants: A systematic review. Expert Rev. Anti-Infect. Ther. 2019, 17, 177–188. [Google Scholar] [CrossRef]
- Hibbert, J.E.; Currie, A.; Strunk, T. Sepsis-Induced Immunosuppression in Neonates. Front. Pediatr. 2018, 6, 357. [Google Scholar] [CrossRef]
- Moon, K.C.; Park, C.-W.; Park, J.K.; Jun, J.K. Fetal Growth Restriction and Sterile Intrauterine Inflammation as Risk Factors for EOS. J. Clin. Med. 2021, 10, 2018. [Google Scholar] [CrossRef]
- Vincent, J.-L. Sepsis and Infection: Two Words That Should Not Be Confused. Front. Med. 2023, 10, 1156732. [Google Scholar] [CrossRef] [PubMed]
- Wynn, J.L.; Polin, R.A. Progress in the Management of Neonatal Sepsis: The Importance of a Consensus Definition. Pediatr. Res. 2018, 83, 13–15. [Google Scholar] [CrossRef]
- Conti, M.G.; Angelidou, A.; Diray-Arce, J.; Smolen, K.K.; Lasky-Su, J.; De Curtis, M.; Levy, O. Immunometabolic Approaches to Prevent, Detect, and Treat Neonatal Sepsis. Pediatr. Res. 2020, 87, 399–405. [Google Scholar] [CrossRef]
- Parra-Llorca, A.; Pinilla-Gonzlez, A.; Torrejón-Rodríguez, L.; Lara-Cantón, I.; Kuligowski, J.; Collado, M.C.; Gormaz, M.; Aguar, M.; Vento, M.; Serna, E.; et al. Effects of Sepsis on Immune Response, Microbiome and Oxidative Metabolism in Preterm Infants. Children 2023, 10, 602. [Google Scholar] [CrossRef]
- Tsantes, A.G.; Parastatidou, S.; Tsantes, E.A.; Bonova, E.; Tsante, K.A.; Mantzios, P.G.; Vaiopoulos, A.G.; Tsalas, S.; Konstantinidi, A.; Houhoula, D.; et al. Sepsis-Induced Coagulopathy: An Update on Pathophysiology, Biomarkers, and Current Guidelines. Life 2023, 13, 350. [Google Scholar] [CrossRef]
- Gialamprinou, D.; Kontovazainitis, C.-G.; Pouliakis, A.; Fleva, A.; Markopoulou, M.; Bessina, M.-E.; Katsaras, G.N.; Chatziioannidis, I.; Giannakou, A.; Roilides, E.; et al. Sepsis-Induced Coagulopathy in Preterm Neonates with Gram-Positive Sepsis Presents with Hypercoagulation and Reduced Platelet Activation Compared with Healthy Preterm Neonates. Res. Pract. Thromb. Haemost. 2023, 7, 100100. [Google Scholar] [CrossRef]
- Hensler, E.; Petros, H.; Gray, C.C.; Chung, C.S.; Ayala, A.; Fallon, E.A. The Neonatal Innate Immune Response to Sepsis: Checkpoint Proteins as Novel Mediators of This Response and as Possible Therapeutic/Diagnostic Levers. Front. Immunol. 2022, 13, 940930. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Zhou, T. Identification of Key Biomarkers in Neonatal Sepsis by Integrated Bioinformatics Analysis and Clinical Validation. Heliyon 2022, 8, e11634. [Google Scholar] [CrossRef]
- Jiang, Z.; Luo, Y.; Wei, L.; Gu, R.; Zhang, X.; Zhou, Y.; Zhang, S. Bioinformatic Analysis and Machine Learning Methods in Neonatal Sepsis: Identification of Biomarkers and Immune Infiltration. Biomedicines 2023, 11, 1853. [Google Scholar] [CrossRef] [PubMed]
- Celik, I.H.; Hanna, M.; Canpolat, F.E.; Mohan, P. Diagnosis of Neonatal Sepsis: The Past, Present and Future. Pediatr. Res. 2022, 91, 337–350. [Google Scholar] [CrossRef]
- Ruan, L.; Chen, G.; Liu, Z.; Zhao, Y.; Xu, G.-Y.; Li, S.-F.; Li, C.-N.; Chen, L.-S.; Tao, Z. Presepsin and CRP in Neonatal Sepsis: A Meta-Analysis. Crit. Care 2018, 22, 316. [Google Scholar] [CrossRef]
- Jouza, M.; Bohosová, J.; Staníková, A.; Pecl, J.; Slaby, O.; Jabandziev, P. MicroRNA as an Early Biomarker of Neonatal Sepsis. Front. Pediatr. 2022, 10, 854324. [Google Scholar] [CrossRef]
- Ng, P.C.; Ma, T.P.; Lam, H.S. The Use of Laboratory Biomarkers in Neonatal Sepsis. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F518–F525. [Google Scholar] [CrossRef]
- Pietrasanta, C.; Pugni, L.; Ronchi, A.; Bottino, I.; Ghirardi, B.; Sanchez-Schmitz, G.; Borriello, F.; Mosca, F.; Levy, O. Vascular Endothelium in Neonatal Sepsis: Basic Mechanisms and Translational Opportunities. Front. Pediatr. 2019, 7, 340. [Google Scholar] [CrossRef] [PubMed]
- Klingenberg, C.; Kornelisse, R.F.; Buonocore, G.; Maier, R.F.; Stocker, M. Culture-negative early-onset neonatal sepsis: At the crossroad between efficient sepsis care and antimicrobial stewardship. Front. Pediatr. 2018, 6, 285. [Google Scholar] [CrossRef] [PubMed]
- Ng, P.C.; Li, G.; Chui, K.M.; Chu, W.C.W.; Li, K.; Wong, R.P.O.; Chik, K.W.; Wong, E.; Fok, T.F. Neutrophil CD64 is a sensi-tive diagnostic marker for early-onset neonatal infection. Pediatr. Res. 2004, 56, 796–803. [Google Scholar] [CrossRef] [PubMed]
- El-Badawy, S.; Botros, S.K.; Sorour, A.E.; Ghany, E.A.; Elbatran, G.; Ali, R. Neutrophil CD64 as a Diagnostic Marker of Sepsis in Neonates. J. Investig. Med. 2014, 62, 644–649. [Google Scholar] [CrossRef]
- Wang, H.; Li, Q.; Wang, Z.; Zheng, H.; Xu, D.; Wang, G. Diagnostic and prognostic value of interleukin-10 in neonatal sepsis: A systematic review and meta-analysis. Cytokine 2021, 148, 155664. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Z.; Chen, X.; Yu, F.; Huang, H.; Shen, X.; Tan, Y.; Wu, Q. Relationship Between the Expression of PD-1 and CTLA-4 on T Lymphocytes and the Severity and Prognosis of Sepsis. Int. J. Gen. Med. 2023, 16, 1513–1525. [Google Scholar] [CrossRef]
- Zonneveld, R.; Jongman, R.; Juliana, A.; Zijlmans, W.; Plötz, F.; Molema, G.; van der Werf, T.S.; Kuijpers, T.W. Low serum angiopoietin-1, high serum angiopoietin-2, and a high Ang-2/Ang-1 protein ratio are associated with ear-ly-onset sepsis in Surinamese newborns. Shock 2017, 48, 638–643. [Google Scholar] [CrossRef]
- Xing, W.; Wang, Y.; Liu, J.; Pei, J.; Yu, C. Role of interleukins in the detection of neonatal sepsis: A network meta-analysis. Front. Pediatr. 2023, 11, 1267777. [Google Scholar] [CrossRef]
- Simonsen, K.A.; Anderson-Berry, A.; Delair, S.F.; Davies, H.D. Early-Onset Neonatal Sepsis. Clin. Microbiol. Rev. 2014, 27, 21–47. [Google Scholar] [CrossRef]
- Glaser, M.A.; Hughes, L.M.; Speer, C.P. Neonatal Sepsis: Pathophysiology and Management. Adv. Neonatal Care 2021, 21, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V. Toll-like Receptors in Sepsis-Associated Cytokine Storm and Their Endogenous Negative Regulators as Future Immunomodulatory Targets. Int. Immunopharmacol. 2020, 89, 107087. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, L.; Ramy, N.; Saied, D.; Akmal, D. Emerging Antimicrobial Resistance in Early and Late-Onset Neonatal Sepsis. Antimicrob. Resist. Infect. Control 2017, 6, 63. [Google Scholar] [CrossRef]
- Khakpour, S.; Wilhelmsen, K.; Hellman, J. Vascular Endothelial Cell Toll-like Receptor Pathways in Sepsis. Innate Immun. 2015, 21, 827–846. [Google Scholar] [CrossRef] [PubMed]
- Eichberger, J.; Resch, E.; Resch, B. Diagnosis of Neonatal Sepsis: The Role of Inflammatory Markers. Front. Pediatr. 2022, 10, 840288. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vulcănescu, A.; Siminel, M.-A.; Dijmărescu, A.-L.; Manolea, M.-M.; Săndulescu, S.-M.; Rădulescu, V.M.; Gheorman, V.; Dinescu, S.-N. Molecular Mechanisms Underlying Inflammation in Early-Onset Neonatal Sepsis: A Systematic Review of Human Studies. J. Clin. Med. 2025, 14, 5315. https://doi.org/10.3390/jcm14155315
Vulcănescu A, Siminel M-A, Dijmărescu A-L, Manolea M-M, Săndulescu S-M, Rădulescu VM, Gheorman V, Dinescu S-N. Molecular Mechanisms Underlying Inflammation in Early-Onset Neonatal Sepsis: A Systematic Review of Human Studies. Journal of Clinical Medicine. 2025; 14(15):5315. https://doi.org/10.3390/jcm14155315
Chicago/Turabian StyleVulcănescu, Anca, Mirela-Anișoara Siminel, Anda-Lorena Dijmărescu, Maria-Magdalena Manolea, Sidonia-Maria Săndulescu, Virginia Maria Rădulescu, Valeriu Gheorman, and Sorin-Nicolae Dinescu. 2025. "Molecular Mechanisms Underlying Inflammation in Early-Onset Neonatal Sepsis: A Systematic Review of Human Studies" Journal of Clinical Medicine 14, no. 15: 5315. https://doi.org/10.3390/jcm14155315
APA StyleVulcănescu, A., Siminel, M.-A., Dijmărescu, A.-L., Manolea, M.-M., Săndulescu, S.-M., Rădulescu, V. M., Gheorman, V., & Dinescu, S.-N. (2025). Molecular Mechanisms Underlying Inflammation in Early-Onset Neonatal Sepsis: A Systematic Review of Human Studies. Journal of Clinical Medicine, 14(15), 5315. https://doi.org/10.3390/jcm14155315