

Ageing and BMI in Focus: Rethinking Risk Assessment for Vertebral Fragility and Pedicle Screw Loosening in Older Adults

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
- (1)
- Severe degenerative spinal stenosis with instability;
- (2)
- Idiopathic scoliosis;
- (3)
- Spondylolisthesis;
- (4)
- De novo lumbar scoliosis.
2.3. Methodological Details of Screw Augmentation and Loosening Diagnosis
2.4. Measurement of Vertebral Hounsfield Unit (HU) Values
2.5. Grouping and BMI Categories
2.6. Statistical Analyses
2.7. AI Statement
3. Results
3.1. Demographics of the Study Cohort
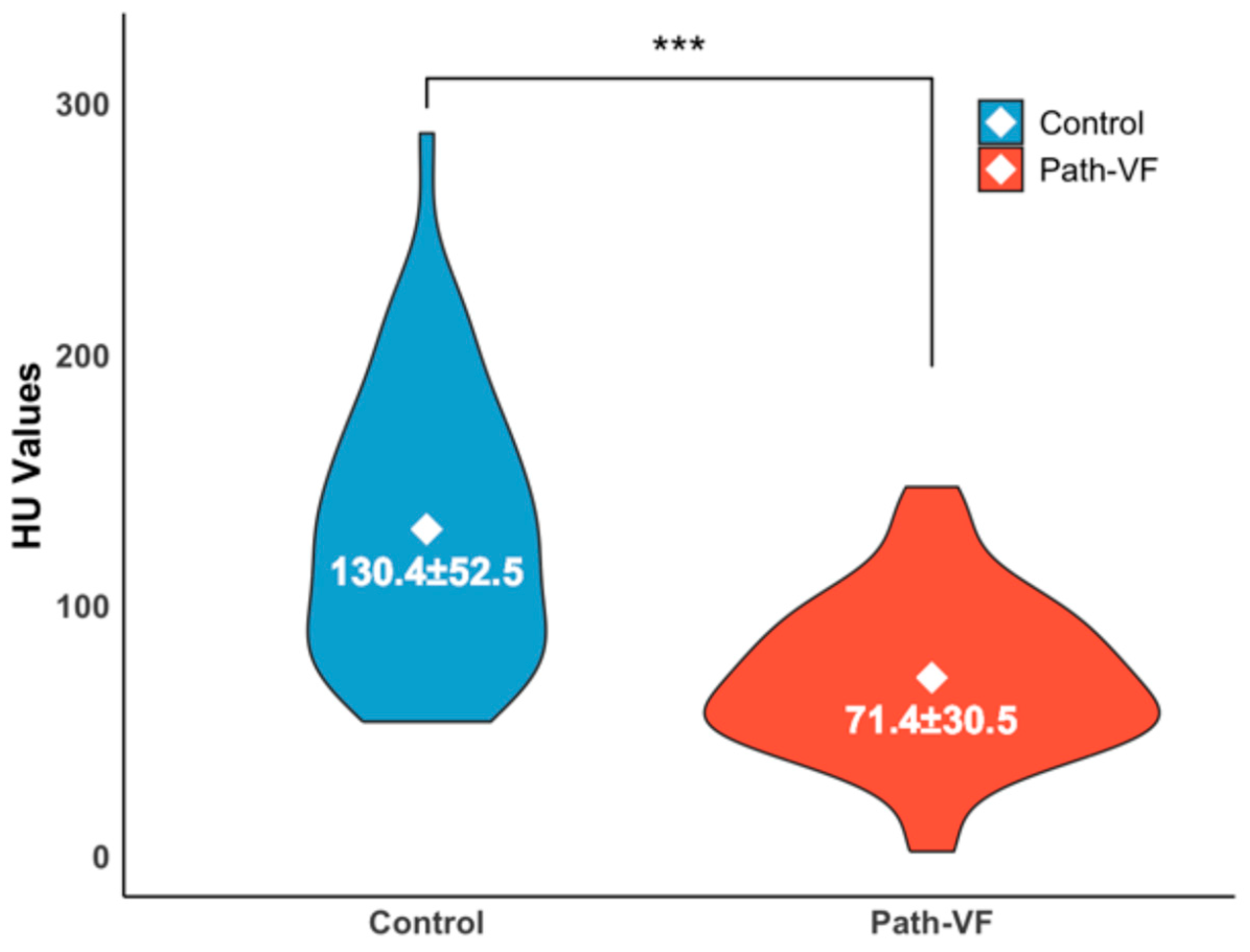
3.2. Differences in Vertebral HU Values Between the Path-VF and Control Groups
3.3. BMI Differences and Associations Between the Path-VF and Control Groups
3.4. Age-Related Distributions of BMI
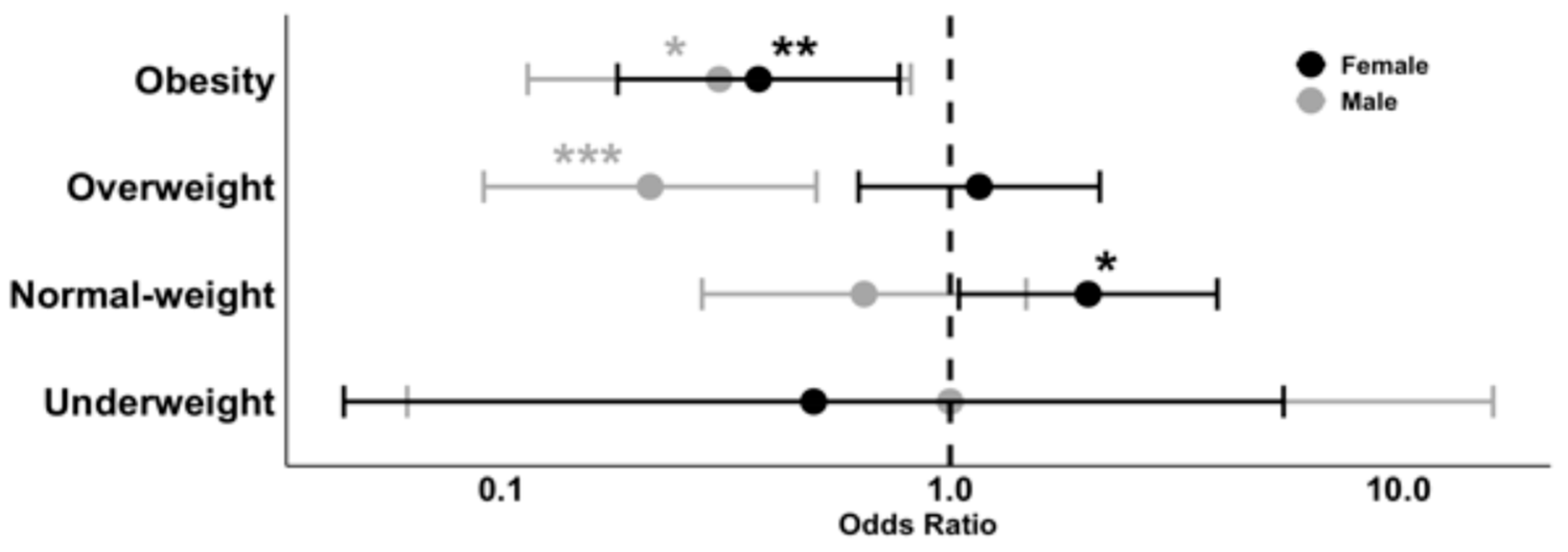
3.5. Binary Logistic Regression Analysis
4. Discussion
4.1. Protective Effects of Higher BMI in the Elderly
4.2. Age-Related Decline in Spinal Bone Strength
4.3. Impact of Underweight and Obesity on Spine Surgery Risk
4.4. Rethinking BMI Thresholds in Vertebral Fragility Assessment
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PSL | Pedicle screw loosening |
| PISF | Posterior instrumented spinal fusion |
| VF | Vertebral fragility |
| Path-VF | Pathological vertebral fragility |
| WHO | World Health Organization |
| BMI | Body mass index |
| HU | Hounsfield units |
| OR | Odds ratio |
| BMD | Bone mineral density |
| SD | Standard deviation |
| SE | Standard error |
| CI | Confidence intervals |
| ROC | Receiver operating characteristic curve |
| AUC | Area under the curve |
| d | Cohen’s d |
| r | Rank-biserial correlation coefficient |
| rp | Pearson’s correlation test coefficient |
| q | Fisher’s Z-test coefficient Cohen’s q |
References
- Singh, S.; Sarma, D.K.; Verma, V.; Nagpal, R.; Kumar, M. From Cells to Environment: Exploring the Interplay between Factors Shaping Bone Health and Disease. Medicina 2023, 59, 1546. [Google Scholar] [CrossRef]
- Zaidi, Q.; MacNeille, R.; Ramos, O.; Wycliffe, N.; Danisa, O.; İnceoğlu, S.; Cheng, W. Predicting Pedicle Screw Pullout and Fatigue Performance: Comparing Lateral Du-al-Energy X-Ray Absorptiometry, Anterior to Posterior Dual-Energy X-Ray Absorptiometry, and Computed Tomography Hounsfield Units. Int. J. Spine Surg 2023, 17, 43–50. [Google Scholar] [CrossRef]
- Khan, A.A.; Slart, R.H.J.A.; Ali, D.S.; Bock, O.; Carey, J.J.; Camacho, P.; Engelke, K.; Erba, P.A.; Harvey, N.C.; Lems, W.F. Osteoporotic Fractures: Diagnosis, Evaluation, and Significance From the Interna-tional Working Group on DXA Best Practices. Mayo Clin. Proc. 2024, 99, 1127–1141. [Google Scholar] [CrossRef]
- Robinson, W.A.; Carlson, B.C.; Poppendeck, H.; Wanderman, N.R.; Bunta, A.D.; Murphy, S.; Sietsema, D.L.; Daffner, S.D.; Edwards, B.J.; Watts, N.B. Osteoporosis-related Vertebral Fragility Fractures: A Review and Analysis of the American Orthopaedic Association’s Own the Bone Database. Spine 2020, 45, E430–E438. [Google Scholar] [CrossRef]
- Ottesen, T.D.; Galivanche, A.R.; Greene, J.D.; Malpani, R.; Varthi, A.G.; Grauer, J.N. Underweight patients are the highest risk body mass index group for perioperative adverse events following stand-alone anterior lumbar interbody fusion. Spine J. 2022, 22, 1139–1148. [Google Scholar] [CrossRef]
- Bono, O.J.; Poorman, G.W.; Foster, N.; Jalai, C.M.; Horn, S.R.; Oren, J.; Soroceanu, A.; Ramachandran, S.; Purvis, T.E.; Jain, D.; et al. Body mass index predicts risk of complications in lumbar spine surgery based on surgical invasiveness. Spine J. 2018, 18, 1204–1210. [Google Scholar] [CrossRef]
- Scaramuzzo, L.; Giudici, F.; Barone, G.; Pironti, P.; Viganò, M.; Ravier, D.; Minoia, L.; Archetti, M.; Zagra, A. Effect of Body Mass Index Percentile on Clinical and Radiographic Outcome and Risk of Complications after Posterior Instrumented Fusion for Adolescent Idiopathic Scoliosis: A Retrospective Cohort Study. J. Clin. Med. 2022, 12, 76. [Google Scholar] [CrossRef]
- Oberthür, S.; Roch, P.J.; Klockner, F.; Jäckle, K.B.; Viezens, L.; Lehmann, W.; Sehmisch, S.; Weiser, L. Can You Feel it?—Correlation Between Intraoperatively Perceived Bone Quality and Objectively Measured Bone Mineral Density. Glob. Spine J. 2024, 14, 631–638. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 May 2025).
- Schoof, B.; Stangenberg, M.; Mende, K.C.; Thiesen, D.M.; Ntalos, D.; Dreimann, M. Obesity in spontaneous spondylodiscitis: A relevant risk factor for severe disease courses. Sci. Rep. 2020, 10, 21919. [Google Scholar] [CrossRef]
- Chen, X.T.B.; Shahrestani, S.; Ballatori, A.M.B.; Ton, A.B.; Buser, Z.; Wang, J.C. The Influence of Body Mass Index in Obese and Morbidly Obese Patients on Complications and 30- and 90-day Readmissions Following Lumbar Spine Fusion. Spine 2021, 46, 965–972. [Google Scholar] [CrossRef]
- Malik, A.T.; Tamer, R.; Yu, E.; Kim, J.; Khan, S.N. The Impact of Body Mass Index (BMI) on 30-day Outcomes Following Posterior Spinal Fusion in Neuromuscular Scoliosis. Spine 2019, 44, 1348–1355. [Google Scholar] [CrossRef]
- Burgstaller, J.M.; Held, U.; Brunner, F.; Porchet, F.; Farshad, M.; Steurer, J.; Ulrich, N. The Impact of Obesity on the Outcome of Decompression Surgery in Degener-ative Lumbar Spinal Canal Stenosis: Analysis of the Lumbar Spinal Outcome Study (LSOS): A Swiss Prospective Multicenter Cohort Study. Spine 2016, 41, 82–89. [Google Scholar] [CrossRef]
- Sun, W.; Zhou, J.; Sun, M.; Qin, X.; Qiu, Y.; Zhu, Z.; Xu, L. Low body mass index can be predictive of bracing failure in patients with adolescent idiopathic scoliosis: A retrospective study. Eur. Spine J. 2017, 26, 1665–1669. [Google Scholar] [CrossRef]
- Alsoof, D.; Johnson, K.; McDonald, C.L.; Daniels, A.H.; Cohen, E.M. Body Mass Index and Risk of Complications After Posterior Lumbar Spine Fusion: A Matched Cohort Analysis Investigating Underweight and Obese Patients. J. Am. Acad. Orthop. Surg. 2023, 31, e394–e402. [Google Scholar] [CrossRef]
- Kim, J.G.; Hong, J.-Y.; Park, J.; Park, S.-M.; Han, K.; Kim, H.-J.; Yeom, J.S. Risk of fracture according to temporal changes of low body weight changes in adults over 40 years: A nationwide population-based cohort study. BMC Public Health 2023, 23, 948. [Google Scholar] [CrossRef]
- Park, S.-M.; Park, J.; Han, S.; Jang, H.-D.; Hong, J.-Y.; Han, K.; Kim, H.-J.; Yeom, J.S. Underweight and risk of fractures in adults over 40 years using the nationwide claims database. Sci. Rep. 2023, 13, 8013. [Google Scholar] [CrossRef]
- Nakajima, K.; Miyahara, J.; Ohtomo, N.; Nagata, K.; Kato, S.; Doi, T.; Matsubayashi, Y.; Taniguchi, Y.; Kawamura, N.; Higashikawa, A.; et al. Impact of body mass index on outcomes after lumbar spine surgery. Sci. Rep. 2023, 13, 7862. [Google Scholar] [CrossRef]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and all-cause mortality in older adults: A meta-analysis. Am. J. Clin. Nutr. 2014, 99, 875–890. [Google Scholar] [CrossRef]
- Al-Barghouthi, A.; Lee, S.; Solitro, G.F.; Latta, L.; Travascio, F. Relationships Among Bone Mor-phological Parameters and Mechanical Properties of Cadaveric Human Vertebral Cancellous Bone. JBMR Plus 2020, 4, e10351. [Google Scholar] [CrossRef]
- Boucas, P.; Mamdouhi, T.; Rizzo, S.E.; Megas, A. Cement Augmentation of Pedicle Screw Instru-mentation: A Literature Review. Asian Spine J. 2023, 17, 939–948. [Google Scholar] [CrossRef]
- Song, Z.; Zhou, Q.; Jin, X.; Zhang, J. Cement-augmented pedicle screw for thoracolumbar degenera-tive diseases with osteoporosis: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2023, 18, 631. [Google Scholar] [CrossRef]
- Ohtori, S.; Inoue, G.; Orita, S.; Yamauchi, K.; Eguchi, Y.; Ochiai, N.; Kishida, S.; Kuniyoshi, K.; Aoki, Y.; Nakamura, J.; et al. Comparison of Teriparatide and Bisphosphonate Treatment to Reduce Pedicle Screw Loosening After Lumbar Spinal Fusion Surgery in Postmenopausal Women With Osteoporosis From a Bone Quality Perspective. Spine 2013, 38, E487–E492. [Google Scholar] [CrossRef]
- Marie-Hardy, L.; Pascal-Moussellard, H.; Barnaba, A.; Bonaccorsi, R.; Scemama, C. Screw Loosen-ing in Posterior Spine Fusion: Prevalence and Risk Factors. Global Spine J. 2020, 10, 598–602. [Google Scholar] [CrossRef]
- Galbusera, F.; Volkheimer, D.; Reitmaier, S.; Berger-Roscher, N.; Kienle, A.; Wilke, H.-J. Pedicle screw loosening: A clinically relevant complication? Eur. Spine J. 2015, 24, 1005–1016. [Google Scholar] [CrossRef]
- Oh, B.H.; Kim, J.Y.; Lee, J.B.; Hong, J.T.; Sung, J.H.; Than, K.D.; Lee, H.J.; Kim, I.S. Screw Insertional Torque Measurement in Spine Surgery: Correlation With Bone Mineral Density and Hounsfield Unit. Neurospine 2023, 20, 1177–1185. [Google Scholar] [CrossRef]
- Carter, J.V.; Pan, J.; Rai, S.N.; Galandiuk, S. ROC-ing along: Evaluation and interpretation of re-ceiver operating characteristic curves. Surgery 2016, 159, 1638–1645. [Google Scholar] [CrossRef]
- Huang, Y.; Peng, J.; Wang, W.; Zheng, X.; Qin, G.; Xu, H. Age-Dependent Association Between Body Mass Index and All-Cause Mortality Among Patients with Hypertension: A Longitudinal Population-Based Cohort Study in China. Clin. Epidemiol. 2023, 15, 1159–1170. [Google Scholar] [CrossRef]
- Winter, J.E.; MacInnis, R.J.; Nowson, C.A. The Influence of Age the BMI and All-Cause Mortali-ty Association: A Meta-Analysis. J. Nutr. Health Aging. 2017, 21, 1254–1258. [Google Scholar] [CrossRef]
- Woolley, C.; Thompson, C.; Hakendorf, P.; Horwood, C. The Effect of Age upon the Interrelation-ship of BMI and Inpatient Health Outcomes. J. Nutr. Health Aging 2019, 23, 558–563. [Google Scholar] [CrossRef]
- Kamei, T.; Aoyagi, K.; Matsumoto, T.; Ishida, Y.; Iwata, K.; Kumano, H.; Murakami, Y.; Kato, Y. Age-Related Bone Loss: Relationship between Age and Regional Bone Mineral Density. Tohoku J. Exp. Med. 1999, 187, 141–147. [Google Scholar] [CrossRef]
- Szulc, P.; Marchand, F.; Duboeuf, F.; Delmas, P. Cross-sectional assessment of age-related bone loss in men: The MINOS study. Bone 2000, 26, 123–129. [Google Scholar] [CrossRef]
- Rondanelli, M.; Gasparri, C.; Perdoni, F.; Riva, A.; Petrangolini, G.; Peroni, G.; Faliva, M.A.; Naso, M.; Perna, S. Bone Mineral Density Reference Values in 18- to 95-Year-Old Population in Lombardy Region, Italy. Am. J. Men’s Health 2022, 16, 15579883221119363. [Google Scholar] [CrossRef]
- Henderson, R.M. The bigger the healthier: Are the limits of BMI risk changing over time? Econ. Hum. Biol. 2005, 3, 339–366. [Google Scholar] [CrossRef]
- Park, J.; Han, S.; Park, S.-M.; Hwang, Y.; Park, J.; Han, K.; Suh, D.H.; Hong, J.-Y. Weight changes after smoking cessation affect the risk of vertebral fractures: A nation-wide population-based cohort study. Spine J. 2024, 24, 867–876. [Google Scholar] [CrossRef]
- Chan, C.T.; A Rees, C. Association between body mass index and posterior spine fusion among patients with adolescent idiopathic scoliosis. PLoS ONE 2023, 18, e0286001. [Google Scholar] [CrossRef]
- Mi, B.; Zhang, J.; Jiang, K.; Meng, H.; Shan, L.; Hao, D. Weight-adjusted waist index is a potential early predictor of degraded bone microarchitecture: A cross-sectional study of the national health and nutrition examination survey 2007–2008. J. Orthop. Surg. 2024, 32, 10225536241268827. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; Kim, S.S.; Lee, J.-P.; Kim, J.S.; Jung, J.G.; Yoon, S.J.; Kim, K.P.; Park, C.-K.; Kim, Y.-H. Association between body mass index and fragility fracture in postmenopausal women: A cross-sectional study using Korean National Health and Nutrition Examination Survey 2008-2009 (KNHANES IV). BMC Women Health 2021, 21, 60. [Google Scholar] [CrossRef]
- Park, J.; Han, S.; Jang, H.-D.; Shin, G.; Han, K.; Hong, J.-Y. Underweight as a risk factor for vertebral fractures in the South Korean population. Spine J. 2023, 23, 877–884. [Google Scholar] [CrossRef]
- Gleeson, M.M.; Solomito, M.J.; Kostyun, R.O.; Esmende, S.; Makanji, H. Low Body Mass Index Patients Undergoing an Anterior Lumbar Fusion May Have an Increased Risk of Perioperative Complications. Int. J. Spine Surg. 2023, 17, 787–793. [Google Scholar] [CrossRef]
- Schreiber, J.J.; Anderson, P.A.; Hsu, W.K. Use of computed tomography for assessing bone mineral density. Neurosurg. Focus 2014, 37, E4. [Google Scholar] [CrossRef]
- Katsevman, G.A.; Daffner, S.D.; Brandmeir, N.J.; Emery, S.E.; France, J.C.; Sedney, C.L. Complexities of spine surgery in obese patient populations: A narrative review. Spine J. 2020, 20, 501–511. [Google Scholar] [CrossRef]
- El Maghraoui, A.; Sadni, S.; El Maataoui, A.; Majjad, A.; Rezqi, A.; Ouzzif, Z.; Mounach, A. Influence of obesity on vertebral fracture prevalence and vitamin D status in postmenopausal women. Nutr. Metab. 2015, 12, 44. [Google Scholar] [CrossRef]
- Bae, K.; Han, S.; Han, K.; Park, J.; Hong, J.-Y.; Choi, S.H. Is Overweight Protective Against Fracture Occurrence? Age and Site-Dependent Different Association Between Body Mass Index and the Incidence of Hip and Vertebral Fractures. Glob. Spine J. 2025; online ahead of print. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | |||||
|---|---|---|---|---|---|
| n | Min. | Mean | Max. | SD | |
| Total | 225 | 17 | 68.11 | 92 | 15.16 |
| Male | 88 | 17 | 65.26 | 92 | 17.78 |
| Female | 137 | 23 | 69.95 | 87 | 12.94 |
| The path-VF group | 94 | ||||
| Male | 26 | 53 | 75.72 | 87.4 | 9.83 |
| Female | 68 | 52 | 75.85 | 87 | 8.27 |
| The control group | 131 | ||||
| Male | 62 | 17 | 60.00 | 92 | 18.57 |
| Female | 69 | 23 | 64.13 | 86 | 14.09 |
| Balloon Kyphoplasty (exclusive tumour) | 33 | 58 | 78.27 | 87 | 8.68 |
| 1st PISF with reinforcement | 47 | 53 | 74.77 | 86 | 8.21 |
| 1st PISF without reinforcement | 141 | 17 | 63.38 | 92 | 16.25 |
| 2nd PISF due to PSL within six months | 29 | 52 | 71.80 | 84 | 9.19 |
| Gender | BMI-Classification | Control (n) | Path-VF (n) | Total (n) |
|---|---|---|---|---|
| Female | Obesity | 28 | 12 | 40 |
| Overweight | 23 | 26 | 49 | |
| Normal weight | 16 | 29 | 45 | |
| Underweight | 2 | 1 | 3 | |
| Male | Obesity | 17 | 6 | 23 |
| Overweight | 28 | 8 | 36 | |
| Normal weight | 16 | 11 | 27 | |
| Underweight | 1 | 1 | 2 |
| Predictor: | β | SE β | z Value | p |
|---|---|---|---|---|
| Constant | −5.03 | 1.20 | −4.19 | 2.77 × 10−5 *** |
| Gender (Female) | 0.73 | 0.38 | 1.93 | 0.054 |
| Age | 0.41 | 0.08 | 4.84 | 1.29 × 10−6 *** |
| BMI | −0.10 | 0.04 | −2.17 | 0.03 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Strahl, A.; Kunze, B.; Krebs, S.; Stangenberg, M.; Viezens, L.; Strube, P.; Dreimann, M. Ageing and BMI in Focus: Rethinking Risk Assessment for Vertebral Fragility and Pedicle Screw Loosening in Older Adults. J. Clin. Med. 2025, 14, 5296. https://doi.org/10.3390/jcm14155296
Li J, Strahl A, Kunze B, Krebs S, Stangenberg M, Viezens L, Strube P, Dreimann M. Ageing and BMI in Focus: Rethinking Risk Assessment for Vertebral Fragility and Pedicle Screw Loosening in Older Adults. Journal of Clinical Medicine. 2025; 14(15):5296. https://doi.org/10.3390/jcm14155296
Chicago/Turabian StyleLi, Jun, André Strahl, Beate Kunze, Stefan Krebs, Martin Stangenberg, Lennart Viezens, Patrick Strube, and Marc Dreimann. 2025. "Ageing and BMI in Focus: Rethinking Risk Assessment for Vertebral Fragility and Pedicle Screw Loosening in Older Adults" Journal of Clinical Medicine 14, no. 15: 5296. https://doi.org/10.3390/jcm14155296
APA StyleLi, J., Strahl, A., Kunze, B., Krebs, S., Stangenberg, M., Viezens, L., Strube, P., & Dreimann, M. (2025). Ageing and BMI in Focus: Rethinking Risk Assessment for Vertebral Fragility and Pedicle Screw Loosening in Older Adults. Journal of Clinical Medicine, 14(15), 5296. https://doi.org/10.3390/jcm14155296