
Comparing Two Types of Robotic Single-Site Myomectomy Using Propensity Score Matching: Coaxial with da Vinci Xi vs. da Vinci SP System


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Variables
2.3. Surgical Procedure
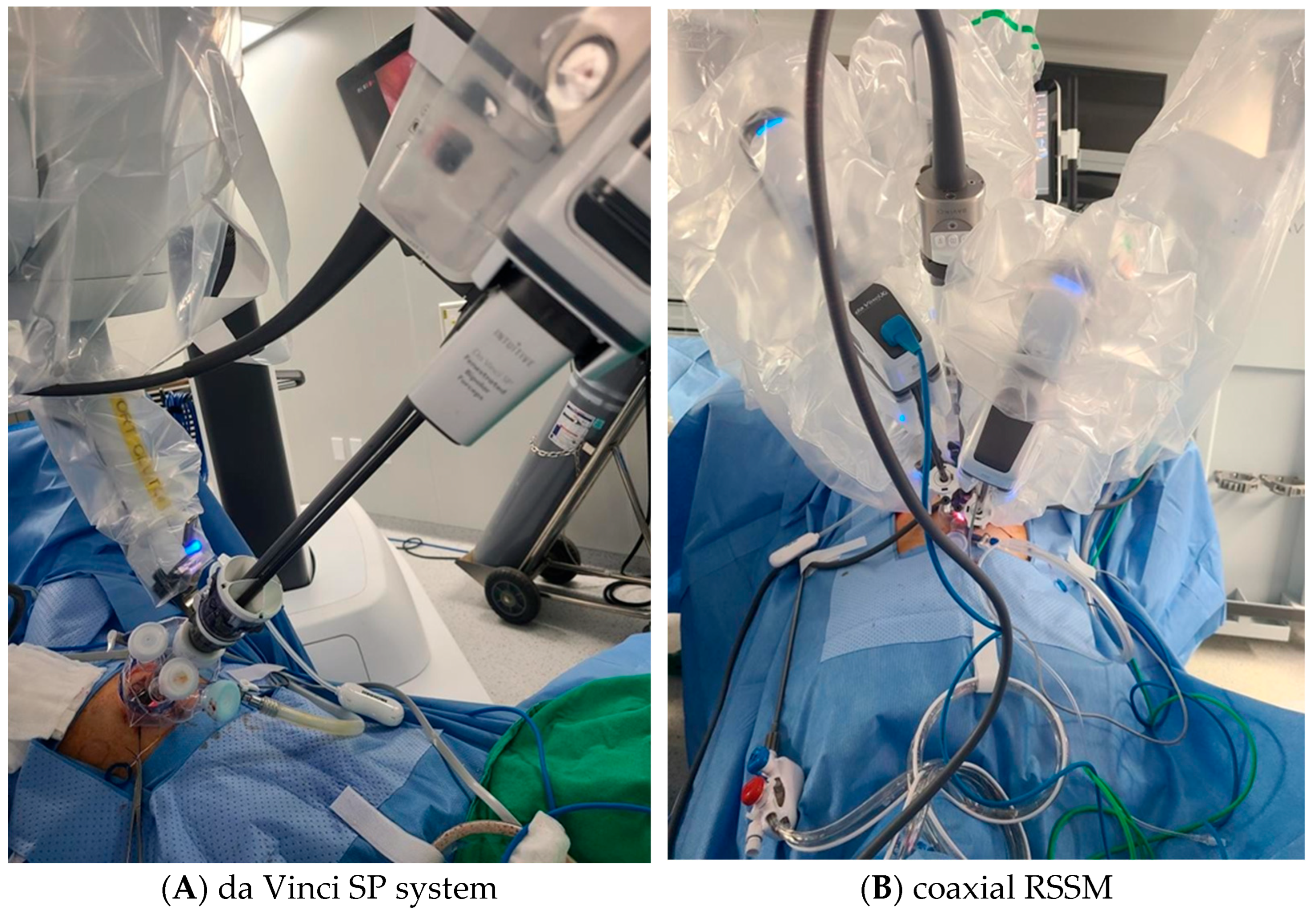
2.3.1. Coaxial RSSM
2.3.2. Da Vinci SP
2.4. Statistical Analysis
3. Results
3.1. A One-to-One Surgeon Comparative Analysis (Single Surgeon per Institution)
3.2. Four-to-One Surgeon Comparative Analysis (Multiple Surgeons at CHA vs. Single Surgeon at Asan)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sinha, R.; Rupa, B.; Raina, R.; Bag, M.; Hk, D.; Reddy, P. Reproductive Outcomes Following Robot-Assisted Laparoscopic Myomectomy: 10 Years’ Experience. Cureus 2024, 16, e70232. [Google Scholar] [CrossRef] [PubMed]
- Gala, R.B.; Margulies, R.; Steinberg, A.; Murphy, M.; Lukban, J.; Jeppson, P.; Aschkenazi, S.; Olivera, C.; South, M.; Lowenstein, L.; et al. Systematic review of robotic surgery in gynecology: Robotic techniques compared with laparoscopy and laparotomy. J. Minim. Invasive Gynecol. 2014, 21, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Kim, J.H.; Scheib, S.; Patzkowsky, K. Advantages of robotics in benign gynecologic surgery. Curr. Opin. Obstet. Gynecol. 2016, 28, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Quaas, A.M.; Einarsson, J.I.; Srouji, S.; Gargiulo, A.R. Robotic myomectomy: A review of indications and techniques. Rev. Obstet. Gynecol. 2010, 3, 185–191. [Google Scholar] [PubMed]
- Tsakos, E.; Xydias, E.M.; Ziogas, A.C.; Sorrentino, F.; Nappi, L.; Vlachos, N.; Daniilidis, A. Multi-Port Robotic-Assisted Laparoscopic Myomectomy: A Systematic Review and Meta-Analysis of Comparative Clinical and Fertility Outcomes. J. Clin. Med. 2023, 12, 4134. [Google Scholar] [CrossRef] [PubMed]
- Jayakumaran, J.; Wiercinski, K.; Buffington, C.; Caceres, A. Robotic laparoendoscopic single-site benign gynecologic surgery: A single-center experience. J. Robot. Surg. 2018, 12, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Vizza, E.; Giannini, A.; Bruno, V.; Baiocco, E.; Mancini, E.; Vizza, R.; Uccella, S.; Raspagliesi, F.; Bogani, G. Robotic-assisted single-port and multi-port surgical staging in early-stage endometrial cancer: A propensity matched comparison. Eur. J. Surg. Oncol. 2025, 51, 110269. [Google Scholar] [CrossRef] [PubMed]
- Iavazzo, C.; Minis, E.E.; Gkegkes, I.D. Single-site port robotic-assisted hysterectomy: An update. J. Robot. Surg. 2018, 12, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Escobar, P.F.; Fader, A.N.; Paraiso, M.F.; Kaouk, J.H.; Falcone, T. Robotic-assisted laparoendoscopic single-site surgery in gynecology: Initial report and technique. J. Minim. Invasive Gynecol. 2009, 16, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, A.R.; Choussein, S.; Srouji, S.S.; Cedo, L.E.; Escobar, P.F. Coaxial robot-assisted laparoendoscopic single-site myomectomy. J. Robot. Surg. 2017, 11, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Bogliolo, S.; Ferrero, S.; Cassani, C.; Musacchi, V.; Zanellini, F.; Dominoni, M.; Spinillo, A.; Gardella, B. Single-site Versus Multiport Robotic Hysterectomy in Benign Gynecologic Diseases: A Retrospective Evaluation of Surgical Outcomes and Cost Analysis. J. Minim. Invasive Gynecol. 2016, 23, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Choi, S.H.; Won, S.; Jung, Y.W.; Kim, S.H.; Lee, J.Y.; Lim, C.K.; Yang, J.B.; Ha, J.G.; Seong, S.J. Comparison of Surgical Outcomes of Two New Techniques Complementing Robotic Single-Site Myomectomy: Coaxial Robotic Single-Site Myomectomy vs. Hybrid Robotic Single-Site Myomectomy. J. Pers. Med. 2024, 14, 439. [Google Scholar] [CrossRef] [PubMed]
- Garisto, J.D.; Bertolo, R.; Kaouk, J. Technique for Docking and Port Placement Using a Purpose-built Robotic System (SP1098) in Human Cadaver. Urology 2018, 119, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Massimello, F.; Cela, V. Role of single port robotic surgery in gynecology.Best Pract. Res. Clin. Obstet. Gynaecol. 2024, 95, 102497. [Google Scholar]
- Shin, H.J.; Yoo, H.K.; Lee, J.H.; Lee, S.R.; Jeong, K.; Moon, H.S. Robotic single-port surgery using the da Vinci SP(R) surgical system for benign gynecologic disease: A preliminary report. Taiwan. J. Obstet. Gynecol. 2020, 59, 243–247. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | C-RSSM (n = 45) | SP (n = 108) | p |
|---|---|---|---|
| Age, years | 36.42 ± 6.22 | 35.82 ± 5.14 | 0.571 |
| BMI, kg/m2 | 21.03 ± 2.31 | 22.90 ± 4.33 | 0.007 |
| Parity | 0 (0–2) | 0 (0–2) | 0.002 |
| Previous abdominal surgery | 0.28 | ||
| No | 37 (82.2) | 97 (89.8) | |
| Yes | 8 (17.8) | 11 (10.2) | |
| Peritoneal adhesion | 0.284 | ||
| No | 44 (97.8) | 100 (92.6) | |
| Yes | 1 (2.2) | 8 (7.4) | |
| Concurrent surgery | 0.849 | ||
| No | 40 (88.9) | 97 (89.8) | |
| Ovarian cystectomy | 4 (8.9) | 9 (8.3) | |
| USO | 0 (0) | 0 (0) | |
| Focal adenomyomectomy | 1 (2.2) | 2 (1.9) | |
| Total myoma, n | 1.89 ± 1.28 | 2.73 ± 2.42 | 0.029 |
| Largest myoma Size, cm | 6.88 ± 1.67 | 8.09 ± 2.43 | 0.001 |
| Location | 0.655 | ||
| Anterior | 22 (48.9) | 47 (43.5) | |
| Posterior | 16 (35.6) | 40 (37.0) | |
| Fundal | 1 (2.2) | 10 (9.3) | |
| Anterior fundal | 5 (11.1) | 6 (5.6) | |
| Posterior fundal | 2 (2.2) | 5 (4.6) | |
| Type (FIGO classification) | 0.116 | ||
| Submucosal (type 1–2) | 4 (8.9) | 4 (3.7) | |
| Intramural (type 3–5) | 34 (75.6) | 92 (85.2) | |
| Subserosal (type 6–8) | 7 (15.6) | 12 (11.1) | |
| Tumor weight, g | 142.40 ± 110.24 | 197.76 ± 167.84 | 0.044 |
| Characteristics | C-RSSM (n = 44) | SP (n = 44) | p |
|---|---|---|---|
| Age, years | 36.34 ± 6.27 | 35.59 ± 4.84 | 0.532 |
| BMI, kg/m2 | 21.06 ± 2.32 | 22.75 ± 4.80 | 0.038 |
| Parity | 0 (0–2) | 0 (0–2) | 0.021 |
| Previous abdominal surgery | 0.196 | ||
| No | 36 (81.8) | 41 (93.2) | |
| Yes | 8 (18.2) | 3 (6.8) | |
| Peritoneal adhesion | 0.196 | ||
| No | 36 (81.8) | 41 (93.2) | |
| Yes | 8 (18.2) | 3 (6.8) | |
| Concurrent surgery | >0.999 | ||
| No | 39 (88.6) | 39 (88.6) | |
| Ovarian cystectomy | 4 (9.1) | 4 (9.1) | |
| USO | 0 (0) | 0 (0) | |
| Focal adenomyomectomy | 1 (2.3) | 1 (2.3) | |
| Total myoma, n | 1.89 ± 1.30 | 1.95 ± 1.56 | 0.824 |
| Largest myoma Size, cm | 6.92 ± 1.68 | 7.25 ± 1.99 | 0.406 |
| Location | 0.686 | ||
| Anterior | 21 (47.7) | 17 (38.6) | |
| Posterior | 16 (36.4) | 19 (43.2) | |
| Fundal | 1 (2.3) | 4 (9.1) | |
| Anterior fundal | 5 (11.4) | 2 (4.5) | |
| Posterior fundal | 1 (2.3) | 2 (4.5) | |
| Type (FIGO classification) | 0.484 | ||
| Submucosal (type 1–2) | 4 (9.1) | 3 (6.8) | |
| Intramural (type 3–5) | 33 (75.0) | 36 (81.8) | |
| Subserosal (type 6–8) | 7(15.9) | 5 (11.4) | |
| Tumor weight, g | 144.73 ± 110.39 | 156.52 ± 143.49 | 0.667 |
| Characteristics | Total Data | In PSM Data | ||||
|---|---|---|---|---|---|---|
| C-RSSM (n = 45) | SP (n = 108) | p | C-RSSM (n = 44) | SP (n = 44) | p | |
| Operative time, mins | 91.22 ± 18.25 | 148.69 ± 45.62 | <0.001 | 90.57 ± 17.92 | 143.05 ± 49.35 | <0.001 |
| EBL, mL | 102.33 ± 61.01 | 203.98 ± 163.15 | <0.001 | 102.39 ± 61.72 | 153.18 ± 102.27 | 0.006 |
| Hemoglobin decrement, g/dL | (t)1.69 ± 0.93 1.69 ± 0.93 (n = 45) | (t)2.85 ± 1.30 2.84 ± 1.29 (n = 103) | <0.001 <0.001 | (t)1.72 ± 0.93 1.72 ± 0.93 (n = 44) | (t)2.30 ± 0.95 2.33 ± 0.95 (n = 42) | 0.005 0.003 |
| Transfusion | 0.243 | 0.494 | ||||
| No | 79 (98.8) | 103 (95.4) | 44 (100) | 42 (95.5) | ||
| Yes | 0 (0) | 5 (4.6) | 0 (0.0) | 2 (4.5) | ||
| Hospital stay, days | 4.27 ± 0.81 | 2.10 ± 0.30 | <0.001 | 4.27 ± 0.82 | 2.07 ± 0.26 | <0.001 |
| Complications | 0.503 | 0.317 | ||||
| None | 44 (97.8) | 107 (99.1) | 43 (97.7) | 44 (100) | ||
| Ileus | 1 (2.2) | 1 (0.9) | 1 (2.3) | 0 (0) | ||
| Fever > 3 days | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Wound dehiscence | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Characteristics | C-RSSM (n = 81) | SP (n = 108) | p |
|---|---|---|---|
| Age, years | 37.31 ± 6.29 | 35.82 ± 5.14 | 0.076 |
| BMI, kg/m2 | 21.73 ± 2.53 | 22.90 ± 4.33 | 0.031 |
| Parity | 0.41 ± 0.72 (0, 0–2) | 0.13 ± 0.46 (0, 0–2) | 0.001 |
| Previous abdominal surgery | 0.061 | ||
| No | 64 (79.0) | 97 (89.8) | |
| Yes | 17 (21.0) | 11 (10.2) | |
| Peritoneal adhesion | 0.357 | ||
| No | 78 (96.3) | 100 (92.6) | |
| Yes | 3 (3.7) | 8 (7.4) | |
| Concurrent surgery | 0.900 | ||
| No | 73 (90.1) | 97 (89.8) | |
| Ovarian cystectomy | 6 (7.4) | 9 (8.3) | |
| USO | 0 (0) | 0 (0) | |
| Focal adenomyomectomy | 2 (2.5) | 2 (1.9) | |
| Total myoma, n | 2.33 ± 1.90 | 2.73 ± 2.42 | 0.207 |
| Largest myoma Size, cm | 7.09 ± 1.57 | 8.09 ± 2.43 | 0.001 |
| Location | 0.454 | ||
| Anterior | 40 (49.4) | 47 (43.5) | |
| Posterior | 30 (37.0) | 40 (37.0) | |
| Fundal | 1 (1.2) | 10 (9.3) | |
| Anterior fundal | 8 (9.9) | 6 (5.6) | |
| Posterior fundal | 2 (2.5) | 5 (4.6) | |
| Type (FIGO classification) | 0.001 | ||
| Submucosal (type 1–2) | 11 (13.6) | 4 (3.7) | |
| Intramural (type 3–5) | 52 (64.2) | 92 (85.2) | |
| Subserosal (type 6–8) | 18 (22.2) | 12 (11.1) | |
| Tumor weight, g | 148.05 ± 111.71 | 197.76 ± 167.84 | 0.016 |
| Characteristics | C-RSSM (n = 68) | SP (n = 68) | p |
|---|---|---|---|
| Age, years | 37.04 ± 6.49 | 35.60 ± 4.87 | 0.145 |
| BMI, kg/m2 | 21.72 ± 2.67 | 22.78 ± 4.63 | 0.102 |
| Parity | 0.40 ± 0.69 (0, 0–2) | 0.16 ± 0.51 (0, 0–2) | 0.026 |
| Previous abdominal surgery | 0.074 | ||
| No | 55 (80.9) | 63 (92.6) | |
| Yes | 13 (19.1) | 5 (7.4) | |
| Peritoneal adhesion | 0.441 | ||
| No | 66 (97.1) | 63 (92.6) | |
| Yes | 2 (2.9) | 5 (7.4) | |
| Concurrent surgery | 0.610 | ||
| No | 62 (91.2) | 51 (89.7) | |
| Ovarian cystectomy | 5 (7.4) | 5 (7.4) | |
| USO | 0 (0) | 0 (0) | |
| Focal adenomyomectomy | 1 (1.5) | 2 (2.9) | |
| Total myoma, n | 2.09 ± 1.45 | 2.15 ± 1.35 | 0.807 |
| Largest myoma Size, cm | 7.32 ± 1.51 | 7.53 ± 2.28 | 0.537 |
| Location | 0.933 | ||
| Anterior | 32 (47.1) | 30 (44.1) | |
| Posterior | 27 (39.7) | 27 (39.7) | |
| Fundal | 1 (1.5) | 7 (10.3) | |
| Anterior fundal | 6 (8.8) | 1 (1.5) | |
| Posterior fundal | 2 (2.9) | 3 (4.4) | |
| Type (FIGO classification) | 0.759 | ||
| Submucosal (type 1–2) | 3 (4.4) | 4 (5.9) | |
| Intramural (type 3–5) | 50 (73.5) | 53 (16.2) | |
| Subserosal (type 6–8) | 15 (22.1) | 11 (16.2) | |
| Tumor weight, g | 157.58 ± 115.78 | 162.38 ± 144.84 | 0.831 |
| Characteristics | Total Data | In PSM Data | ||||
|---|---|---|---|---|---|---|
| C-RSSM (n = 81) | SP (n = 108) | p | C-RSSM (n = 68) | SP (n = 68) | p | |
| Operative time, mins | 98.09 ± 27.80 | 148.69 ± 45.62 | <0.001 | 94.34 ± 21.58 | 136.29 ± 39.19 | <0.001 |
| EBL, mL | 142.41 ± 115.99 | 203.98 ± 163.15 | <0.001 | 128.46 ± 89.52 | 188.97 ± 137.95 | 0.003 |
| Hemoglobin decrement, g/dL | (t)1.60 ± 0.91 1.67 ± 0.83 (n = 79) | (t)2.85 ± 1.29 2.84 ± 1.29 (n = 103) | <0.001 <0.001 | (t)1.69 ± 0.88 1.73 ± 0.83 (n = 67) | (t)2.78 ± 1.33 2.76 ± 1.31 (n = 66) | <0.001 <0.001 |
| Transfusion | 0.243 | >0.999 | ||||
| No | 79 (97.5) | 103 (95.4) | 67 (98.5) | 66 (97.1) | ||
| Yes | 2 (2.5) | 5 (4.6) | 1 (1.5) | 2 (2.9) | ||
| Hospital stay, days | 4.05 ± 0.72 | 2.10 ± 0.30 | <0.001 | 4.07 ± 0.76 | 2.06 ± 0.24 | <0.001 |
| Complications | 0.838 | >0.999 | ||||
| None | 80 (98.8) | 126 (95.5) | 67 (98.5) | 67 (98.5) | ||
| Ileus | 1 (2.2) | 1 (0.9) | 1 (1.5) | 1 (1.5) | ||
| Fever > 3 days | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Wound dehiscence | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.; Choi, S.H.; Kim, M.-L.; Lee, S.R.; Seong, S.J. Comparing Two Types of Robotic Single-Site Myomectomy Using Propensity Score Matching: Coaxial with da Vinci Xi vs. da Vinci SP System. J. Clin. Med. 2025, 14, 5106. https://doi.org/10.3390/jcm14145106
Lee N, Choi SH, Kim M-L, Lee SR, Seong SJ. Comparing Two Types of Robotic Single-Site Myomectomy Using Propensity Score Matching: Coaxial with da Vinci Xi vs. da Vinci SP System. Journal of Clinical Medicine. 2025; 14(14):5106. https://doi.org/10.3390/jcm14145106
Chicago/Turabian StyleLee, Nara, Su Hyeon Choi, Mi-La Kim, Sa Ra Lee, and Seok Ju Seong. 2025. "Comparing Two Types of Robotic Single-Site Myomectomy Using Propensity Score Matching: Coaxial with da Vinci Xi vs. da Vinci SP System" Journal of Clinical Medicine 14, no. 14: 5106. https://doi.org/10.3390/jcm14145106
APA StyleLee, N., Choi, S. H., Kim, M.-L., Lee, S. R., & Seong, S. J. (2025). Comparing Two Types of Robotic Single-Site Myomectomy Using Propensity Score Matching: Coaxial with da Vinci Xi vs. da Vinci SP System. Journal of Clinical Medicine, 14(14), 5106. https://doi.org/10.3390/jcm14145106