

Review of the Safety and Clinical Considerations of Vasoconstrictor Agents in Dental Anesthesia During Pregnancy


 ,
,  ,
,  and
and
Abstract
1. Introduction
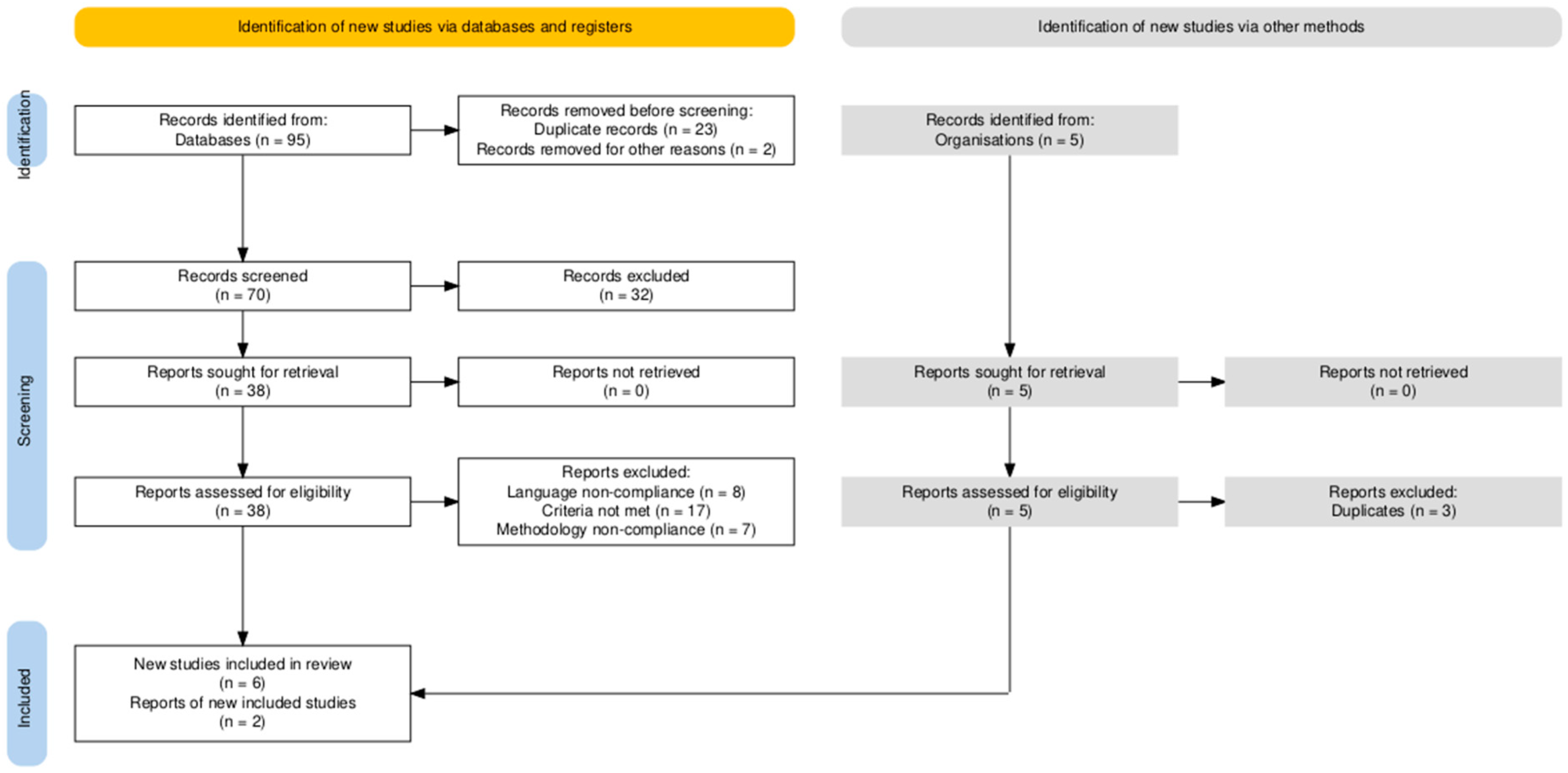
2. Materials and Methods
2.1. General Considerations
2.2. Study Selection
2.3. Study Design
3. Results
4. Discussions
4.1. Physiological and Genetic Factors Affecting Vasoconstrictor Response in Pregnancy
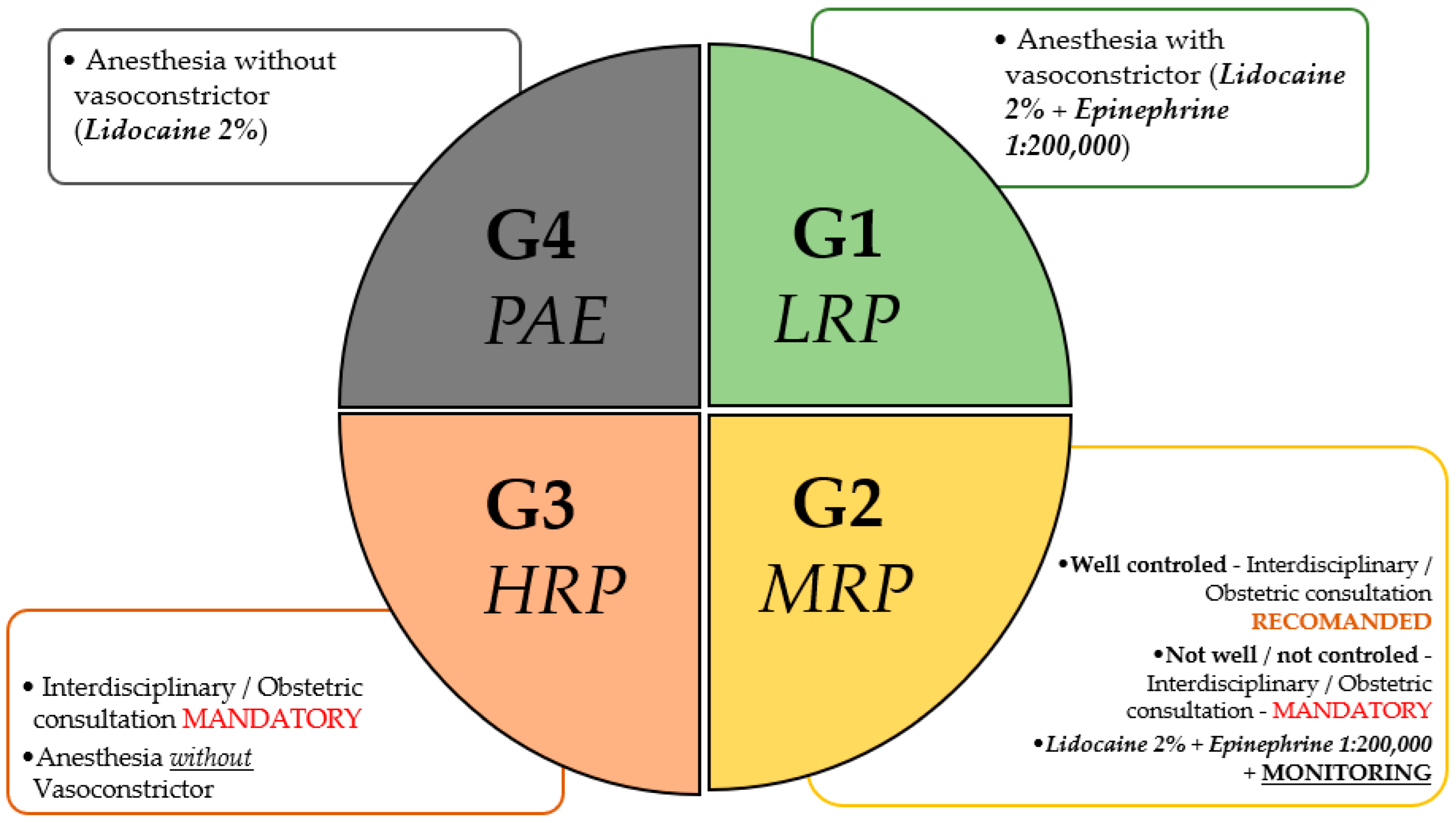
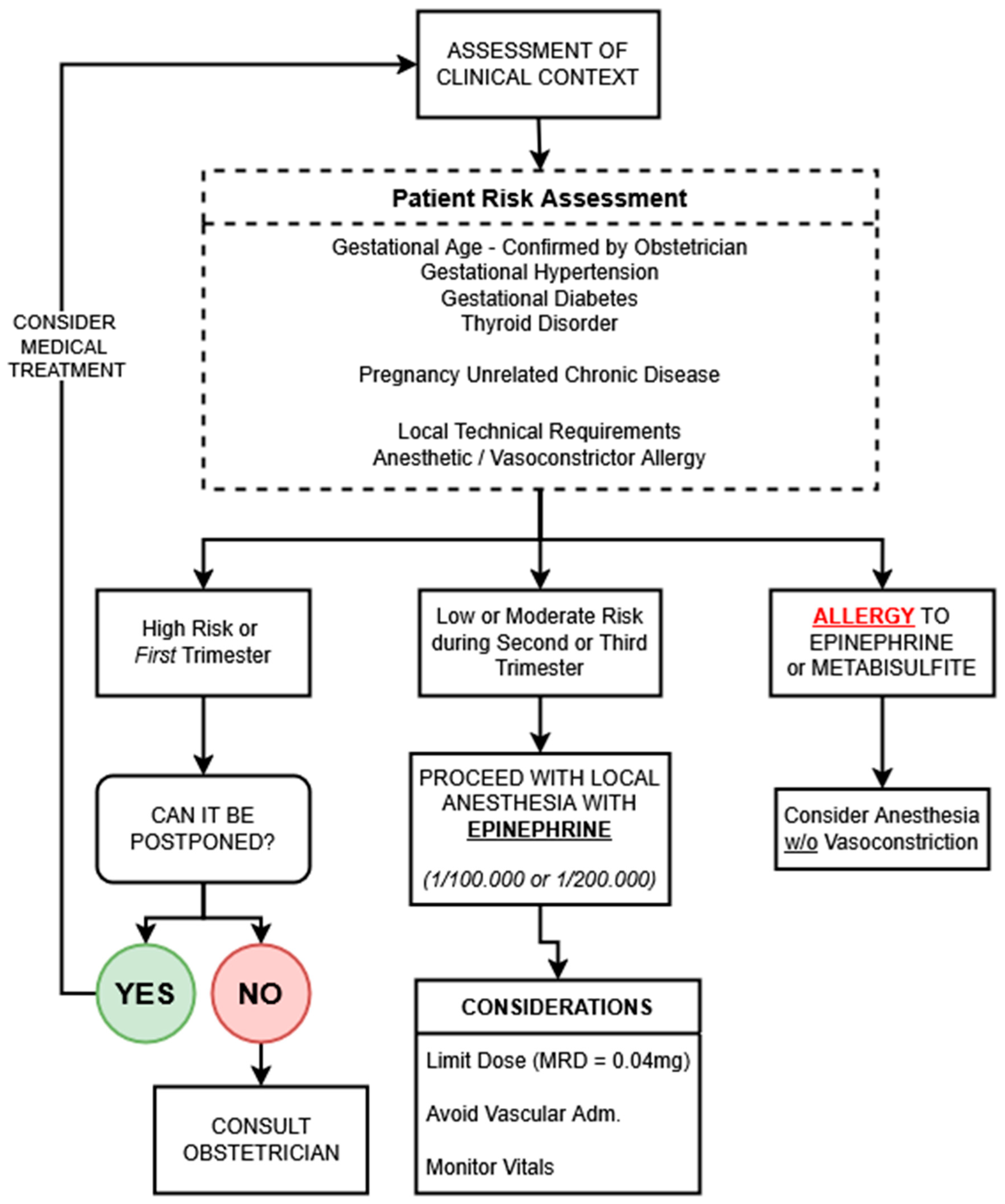
4.2. Clinical Risk Stratification and Counseling
4.3. Clinical Evidence: Uterine and Placental Effects of Vasoconstrictors
4.4. Limitations
4.5. Future Perspectives
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACOG | American College of Obstetricians and Gynecologists |
| ADA | American Dental Association |
| COMT | Catechol-O-methyltransferase |
| FDA | Food and Drug Administration |
| ISI | Institute for Scientific Information |
| MAO | Monoamine Oxidase |
| MeSH | Medical Subject Headings |
| MRD | Maximum Recommended Dose |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
References
- Padilla-Cáceres, T.; Arbildo-Vega, H.I.; Caballero-Apaza, L.; Cruzado-Oliva, F.; Mamani-Cori, V.; Cervantes-Alagón, S.; Munayco-Pantoja, E.; Panda, S.; Vásquez-Rodrigo, H.; Castro-Mejía, P.; et al. Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review. Dent. J. 2023, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Temur, I.; Temur, K.T.; Dönertas, S.N.; Dönertas, A.D.; Kacmaz, M. The relationship between maternal oral health parameters, inflammatory blood markers, and the evaluation of their effects on preterm low birth weight. BMC Pregnancy Childbirth 2025, 25, 231. [Google Scholar] [CrossRef] [PubMed]
- Deol, N.; Alvarez, G.; Elrabi, O.; Chen, G.; Ferraro, N. A comparative review of epinephrine and phenylephrine as vasoconstrictors in dental anesthesia: Exploring the factors behind epinephrine’s prevalence in the US. J. Dent. Anesth. Pain Med. 2023, 23, 293–302. [Google Scholar] [CrossRef]
- Serrera Figallo, M.A.; Velázquez Cayón, R.T.; Torres Lagares, D.; Corcuera Flores, J.R.; Machuca Portillo, G. Use of anesthetics associated to vasoconstrictors for dentistry in patients with cardiopathies. Review of the literature published in the last decade. J. Clin. Exp. Dent. 2012, 4, e107–e111. [Google Scholar] [CrossRef]
- Costantine, M. Physiologic and pharmacokinetic changes in pregnancy. Front. Pharmacol. 2014, 5, 65. Available online: https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2014.00065/full (accessed on 24 May 2025). [CrossRef] [PubMed]
- Cardiovascular Physiology of Pregnancy|Circulation. Available online: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.114.009029 (accessed on 24 May 2025).
- Lee, J.M.; Shin, T.J. Use of local anesthetics for dental treatment during pregnancy; safety for parturient. J. Dent. Anesth Pain Med. 2017, 17, 81–90. [Google Scholar] [CrossRef]
- Zhou, X.; Zhong, Y.; Pan, Z.; Zhang, J.; Pan, J. Physiology of pregnancy and oral local anesthesia considerations. PeerJ 2023, 11, e15585. [Google Scholar] [CrossRef]
- Lopes, I.C.; Carneiro, D.T.O. Analgesia in Pregnant Patients: A Literature Review. Braz. J. Dent. Oral Radiol. 2024, 3, bjd40. [Google Scholar] [CrossRef]
- Fayans, E.P.; Stuart, H.R.; Carsten, D.; Ly, Q.; Kim, H. Local Anesthetic Use in the Pregnant and Postpartum Patient. Dent. Clin. N. Am. 2010, 54, 697–713. [Google Scholar] [CrossRef]
- Curtin, C.; Stokes, S.; Shah, F. Pregnancy and Dentistry: A Guide for the General Dental Practitioner. Part 2. Available online: https://www.dental-update.co.uk/content/general-practice/pregnancy-and-dentistry-a-guide-for-the-general-dental-practitioner-part-2/ (accessed on 25 May 2025).
- Manautou, M.; Mayberry, M. Local Anesthetics and Pregnancy. A review of the evidence and why dentists should feel safe to treat pregnant people. J. Evid.-Based Dent. Pract. 2023, 23, 101833. [Google Scholar] [CrossRef]
- Ho, J.-P.T.F.; van Riet, T.C.T.; Afrian, Y.; Sem, K.T.H.C.J.; Spijker, R.; de Lange, J.; Lindeboom, J.A. Adverse effects following dental local anesthesia: A literature review. J. Dent. Anesth. Pain Med. 2021, 21, 507–525. [Google Scholar] [CrossRef]
- ADA Pregnancy. Available online: https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy (accessed on 25 May 2025).
- Oral Health Care During Pregnancy and Through the Lifespan. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan (accessed on 25 May 2025).
- Drug Therapy for the Pregnant Dental Patient|Procter & Gamble. Available online: https://cdeworld.com/courses/5081-drug-therapy-for-the-pregnant-dental-patient (accessed on 25 May 2025).
- Moore, P.A.; Hersh, E.V. Local Anesthetics: Pharmacology and Toxicity. Dent. Clin. N. Am. 2010, 54, 587–599. [Google Scholar] [CrossRef]
- Ouanounou, A.; Haas, D. Drug therapy during pregnancy: Implications for dental practice. Br. Dent, J. 2016, 220, 413–417. [Google Scholar] [CrossRef]
- Boeldt, D.S.; Bird, I.M. Vascular adaptation in pregnancy and endothelial dysfunction in preeclampsia. J. Endocrinol. 2017, 232, R27–R44. [Google Scholar] [CrossRef]
- Pariente, G.; Leibson, T.; Carls, A.; Adams-Webber, T.; Ito, S.; Koren, G. Pregnancy-Associated Changes in Pharmacokinetics: A Systematic Review. PLoS Med. 2016, 13, e1002160. [Google Scholar] [CrossRef]
- Feghali, M.; Venkataramanan, R.; Caritis, S. Pharmacokinetics of drugs in pregnancy. Semin. Perinatol. 2015, 39, 512–519. [Google Scholar] [CrossRef]
- Notarianni, L.J. Plasma protein binding of drugs in pregnancy and in neonates. Clin. Pharmacokinet. 1990, 18, 20–36. [Google Scholar] [CrossRef]
- Ahrens, S.; Singer, D. Placental Adaptation to Hypoxia: The Case of High-Altitude Pregnancies. Int. J. Environ. Res. Public Health 2025, 22, 214. [Google Scholar] [CrossRef]
- Arenas, G.A.; Lorca, R.A. Effects of hypoxia on uteroplacental and fetoplacental vascular function during pregnancy. Front. Physiol. 2024, 15, 1490154. Available online: https://www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2024.1490154/full (accessed on 25 May 2025). [CrossRef]
- Gogarten, W.; Strümper, D.; Buerkle, H.; Aken, H.V.; Marcus, M.A.E. Testing an epidural catheter in obstetrics: Epinephrine or isoproterenol? Int. J. Obstet. Anesth. 2001, 10, 40–45. [Google Scholar] [CrossRef]
- Bagci, B.; Karakus, S.; Bagci, G.; Sancakdar, E. Renalase gene polymorphism is associated with increased blood pressure in preeclampsia. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2016, 6, 115–120. [Google Scholar] [CrossRef]
- Felypressin—An Overview|ScienceDirect Topics. Available online: https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/felypressin?utm_source=chatgpt.com (accessed on 25 May 2025).
- Kapur, B.M.; Lala, P.K.; Shaw, J.L.V. Pharmacogenetics of chronic pain management. Clin. Biochem. 2014, 47, 1169–1187. [Google Scholar] [CrossRef]
- Karahoda, R.; Vachalova, V.; Portillo, R.; Mahrla, F.; Viñas-Noguera, M.; Abad, C.; Staud, F. Developmental expression of catecholamine system in the human placenta and rat fetoplacental unit. Sci. Rep. 2024, 14, 6948. [Google Scholar] [CrossRef] [PubMed]
- Horackova, H.; Karahoda, R.; Vachalova, V.; Turkova, H.; Abad, C.; Staud, F. Functional characterization of dopamine and norepinephrine transport across the apical and basal plasma membranes of the human placental syncytiotrophoblast. Sci. Rep. 2022, 12, 11603. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.; Staalsoe, J.M.; Ullum, H.; Secher, N.H.; Nielsen, H.B.; Olsen, N.V. The Gly16 Allele of the Gly16Arg Single-Nucleotide Polymorphism in the β2-Adrenergic Receptor Gene Augments Perioperative Use of Vasopressors: A Retrospective Cohort Study. Anesth. Analg. 2016, 122, 1385–1393. [Google Scholar] [CrossRef]
- Frey, U.H.; Karlik, J.; Herbstreit, F.; Peters, J. β2-Adrenoceptor gene variants affect vasopressor requirements in patients after thoracic epidural anaesthesia. Br. J. Anaesth. 2014, 112, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Vallada, H.; Curtis, D.; Arranz, M.; Xu, K.; Cai, G.; Deng, H.; Liu, J.; Murray, R.; Liu, X.; et al. Catechol-O-methyltransferase Val158Met polymorphism: Frequency analysis in Han Chinese subjects and allelic association of the low activity allele with bipolar affective disorder. Pharmacogenetics 1997, 7, 349–353. [Google Scholar] [CrossRef]
- Gazal, G.; Omar, E.; Elmalky, W. Rules of selection for a safe local anesthetic in dentistry. J. Taibah Univ. Med. Sci. 2023, 18, 1195–1196. [Google Scholar] [CrossRef]
- Themes UFO. Local Anesthetics for Dentistry. Pocket Dentistry. 2020. Available online: https://pocketdentistry.com/local-anesthetics-for-dentistry/ (accessed on 25 May 2025).
- Indian Dental Association. Available online: https://www.ida.org.in/Membership/Details/Anaesthetics?utm_source=chatgpt.com (accessed on 25 May 2025).
- Albright, G.A.; Jouppila, R.; Hollmén, A.I.; Jouppila, P.; Vierola, H.; Koivula, A. Epinephrine does not alter human intervillous blood flow during epidural anesthesia. Anesthesiology 1981, 54, 131–135. [Google Scholar] [CrossRef]
- Hollmén, A.I.; Jouppila, R.; Jouppila, P. Regional anaesthesia and uterine blood flow. Ann. Chir. Gynaecol. 1984, 73, 149–152. [Google Scholar]
- Yurth, D.A. Placental transfer of local anesthetics. Clin. Perinatol. 1982, 9, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, S.C.; Kien, N.; Martucci, R.W.; Gelzleichter, T.R.; Witschi, H.; Hendrickx, A.G.; Last, J.A. Nicotine- or epinephrine-induced uteroplacental vasoconstriction and fetal growth in the rat. Toxicology 1994, 94, 69–80. Available online: https://pubmed.ncbi.nlm.nih.gov/7801331/?utm (accessed on 26 May 2025). [CrossRef]
- Chestnut, D.H.; Weiner, C.P.; Martin, J.G.; Herrig, J.E.; Wang, J.P. Effect of intravenous epinephrine on uterine artery blood flow velocity in the pregnant guinea pig. Anesthesiology 1986, 65, 633–636. Available online: https://pubmed.ncbi.nlm.nih.gov/3789435/?utm (accessed on 25 May 2025). [CrossRef]
- Robertson, V.J.; Taylor, S.E.; Gage, T.W. Quantitative and qualitative analysis of the pressor effects of levonordefrin. J. Cardiovasc. Pharmacol. 1984, 6, 929–935. [Google Scholar] [CrossRef]
- A Synthetic Analogue of Vasopressin-Felypressin—Creative Peptides. Available online: https://www.creative-peptides.com/article/a-synthetic-analogue-of-vasopressin-felypressin-186.html?utm_source=chatgpt.com (accessed on 26 May 2025).
- Jastak, J.T.; Yagiela, J.A. Vasoconstrictors and local anesthesia: A review and rationale for use. J. Am. Dent. Assoc. 1983, 107, 623–630. [Google Scholar] [CrossRef]
- Hersh, E.V.; Giannakopoulos, H. Beta-adrenergic Blocking Agents and Dental Vasoconstrictors. Dent. Clin. N. Am. 2010, 54, 687–696. [Google Scholar] [CrossRef]
- Hersh, E.V.; Giannakopoulos, H.; Levin, L.M.; Secreto, S.; Moore, P.A.; Peterson, C.; Hutcheson, M.; Bouhajib, M.; Mosenkis, A.; Townsend, R.R. The pharmacokinetics and cardiovascular effects of high-dose articaine with 1:100,000 and 1:200,000 epinephrine. J. Am. Dent. Assoc. 2006, 137, 1562–1571. [Google Scholar] [CrossRef] [PubMed]
- Topical Hemostatic Agents at Time of Obstetric and Gynecologic Surgery. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/10/topical-hemostatic-agents-at-time-of-obstetric-and-gynecologic-surgery (accessed on 26 May 2025).
- Laser-Assisted Dental Procedures: Is It a Safe Tool to Be Considered in Pregnant Patients? A Brief Review. Available online: https://www.researchgate.net/publication/368292483_Laser-assisted_Dental_Procedures_Is_it_a_Safe_Tool_to_be_Considered_in_Pregnant_Patients_A_Brief_Review?utm_source=chatgpt.com (accessed on 26 May 2025).

{kind=link}
{kind=link}
{kind=link}
| Study/Source and Year | Type of Source | Vasoconstrictor(s) Assessed | Key Findings |
|---|---|---|---|
| Lee and Shin (2017) [7] | Narrative Review | Epinephrine | Low-dose epinephrine (1:100,000–1:200,000) unlikely to cause significant uterine vasoconstriction; rapid metabolism reduces fetal risk. |
| Lopes and Carneiro (2024) [9] | Review Article | Epinephrine | Supports the use of lidocaine with epinephrine (1:100,000) in pregnancy; highlights relative safety and cautions for other anesthetics. |
| Fayans et al. (2010) [10] | Review Article | Epinephrine, Levonordefrin | Not recommended in pregnancy due to cardiovascular stimulation and lack of safety data. |
| Curtin et al. (2022) [11] | Review Article | Epinephrine | Considered safe when administered correctly during pregnancy. |
| Manautou and Mayberry (2023) [12] | Review Article | Felypressin, Epinephrine | Felypressin not recommended due to oxytocic effects; epinephrine safe at dental doses. |
| Ho et al. (2021) [13] | Review Article | Epinephrine, Levonordefrin | Summarizes adverse effects of local anesthesia, including systemic reactions and the need for caution in pregnancy. |
| ADA Clinical Guidelines [14] | Clinical Guideline | Epinephrine | Supports the use of epinephrine-containing anesthetics with proper technique. |
| ACOG Committee Opinion (2017) [15] | Clinical Guideline | Epinephrine | Dental procedures with epinephrine-containing anesthetics are generally safe if necessary. |
| Parameter | Epinephrine | Levonordefrin | Felypressin |
|---|---|---|---|
| Mechanism of Action | α and β adrenergic agonist | Primarily α adrenergic agonist | Vasopressin receptor agonist (non-adrenergic) |
| Onset of Action | Rapid (1–2 min) | Rapid (2–3 min) | Rapid (2–4 min) |
| Duration of Effect | Intermediate (60–120 min) | Intermediate (60–120 min) | Intermediate (60–120 min) |
| Systemic Absorption | Minimal at dental doses (aspiration reduces systemic exposure) | Moderate (higher systemic absorption potential) | Moderate (similar systemic exposure potential) |
| Uteroplacental Risk | Low–moderate; dose-dependent vasoconstriction of uterine arteries at higher doses; acceptable at low dental doses | Moderate–high; theoretically more potent uterine vasoconstriction; insufficient human safety data | High; directly stimulates uterine contractions, significant risk of premature labor and fetal compromise |
| Placental Transfer | Limited placental transfer; rapid metabolism minimizes fetal exposure | Limited data; presumed moderate placental transfer based on structure | Limited data; presumed moderate–high due to smaller molecular size |
| FDA Pregnancy Category | Category C (risk not ruled out, considered safe at low doses) | Not individually categorized by the FDA; however, 2% mepivacaine + 1:20,000 levonordefrin is Category C in the USA | Not categorized by the FDA; not available in the USA as single or combination product (contraindicated due to known uterotonic risk) |
| Accessibility | Widely available globally | Less commonly available; limited international usage | Limited availability; primarily in European and Asian markets |
| Price (Cost) | Low-cost; economical and widely used | Moderate; slightly higher cost, limited market availability | Moderate–high; higher cost due to specialized market |
| Clinical Guidelines | Endorsed by the ADA and ACOG for use with caution in pregnancy | Not clearly endorsed; guidelines recommend caution or avoidance due to limited data | Contraindicated by clinical guidelines and professional consensus during pregnancy |
| Cardiovascular Effects | α1 and β2 adrenergic activity; pressor effect moderated by β2-induced vasodilation; well tolerated at low doses | Primarily α1 adrenergic stimulation; limited β2 activity; may cause hypertension with reflex bradycardia | Minimal cardiovascular stimulation; negligible adrenergic activity but risk related to direct stimulation of uterine smooth muscle; risk of preterm labor |
| Metabolism | Rapid enzymatic degradation (COMT, MAO); very short half-life (~2 min) | Moderate enzymatic degradation (MAO); half-life slightly longer (~2–5 min) | Metabolized rapidly by enzymatic degradation in circulation (vasopressinase); short half-life (~10 min) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urîtu, A.; Buciu, V.B.; Roi, C.; Chioran, D.; Serban, D.M.; Nicoleta, N.; Rusu, E.L.; Ionac, M.; Riviș, M.; Ciurescu, S. Review of the Safety and Clinical Considerations of Vasoconstrictor Agents in Dental Anesthesia During Pregnancy. J. Clin. Med. 2025, 14, 4773. https://doi.org/10.3390/jcm14134773
Urîtu A, Buciu VB, Roi C, Chioran D, Serban DM, Nicoleta N, Rusu EL, Ionac M, Riviș M, Ciurescu S. Review of the Safety and Clinical Considerations of Vasoconstrictor Agents in Dental Anesthesia During Pregnancy. Journal of Clinical Medicine. 2025; 14(13):4773. https://doi.org/10.3390/jcm14134773
Chicago/Turabian StyleUrîtu, Andrei, Victor Bogdan Buciu, Ciprian Roi, Doina Chioran, Denis Mihai Serban, Nicolae Nicoleta, Elena Lavinia Rusu, Mihai Ionac, Mircea Riviș, and Sebastian Ciurescu. 2025. "Review of the Safety and Clinical Considerations of Vasoconstrictor Agents in Dental Anesthesia During Pregnancy" Journal of Clinical Medicine 14, no. 13: 4773. https://doi.org/10.3390/jcm14134773
APA StyleUrîtu, A., Buciu, V. B., Roi, C., Chioran, D., Serban, D. M., Nicoleta, N., Rusu, E. L., Ionac, M., Riviș, M., & Ciurescu, S. (2025). Review of the Safety and Clinical Considerations of Vasoconstrictor Agents in Dental Anesthesia During Pregnancy. Journal of Clinical Medicine, 14(13), 4773. https://doi.org/10.3390/jcm14134773