
Ten-Year Trend in the Potentially Inappropriate Prescribing of Renally-Dependent Medicines in Australian General Practice Patients with Dementia


Abstract
1. Introduction
2. Methods
2.1. Design and Data Source
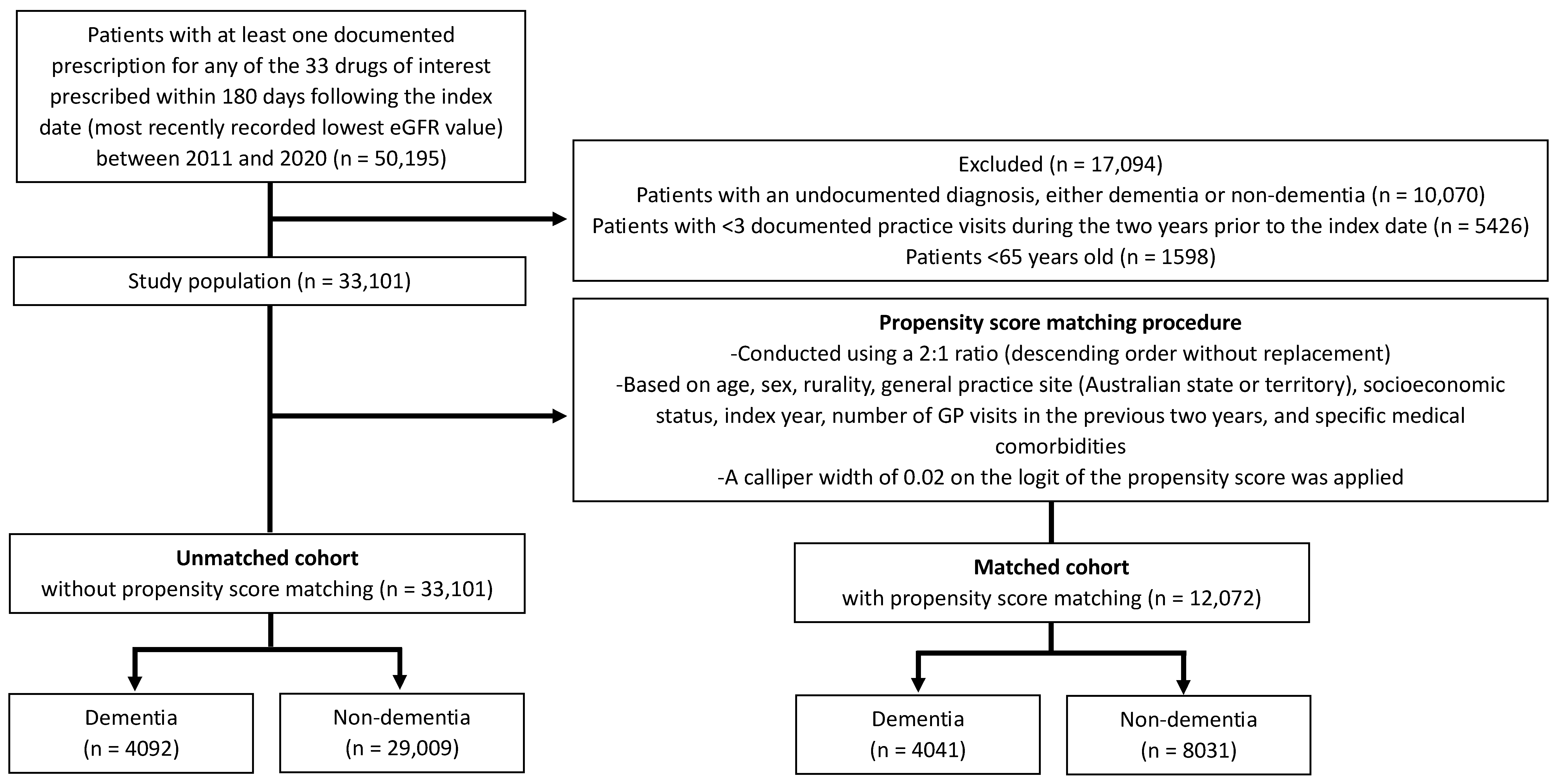
2.2. Study Population and Inclusion Criteria
2.3. Study Outcomes, Study Covariates and Statistical Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Jun, M.; Wick, J.; Neuen, B.L.; Kotwal, S.; Badve, S.V.; Woodward, M.; Chalmers, J.; Peiris, D.; Rodgers, A.; Nallaiah, K. The Prevalence of CKD in Australian Primary Care: Analysis of a National General Practice Dataset. Kidney Int. Rep. 2024, 9, 312–322. [Google Scholar] [CrossRef]
- Aucella, F.; Corsonello, A.; Soraci, L.; Fabbietti, P.; Prencipe, M.A.; Gatta, G.; Lattanzio, F.; Cortese, L.; Pagnotta, M.R.; Antonelli Incalzi, R. A focus on CKD reporting and inappropriate prescribing among older patients discharged from geriatric and nephrology units throughout Italy: A nationwide multicenter retrospective cross-sectional study. Front. Pharmacol. 2022, 13, 996042. [Google Scholar] [CrossRef]
- Hartmann, B.; Czock, D.; Keller, F. Drug therapy in patients with chronic renal failure. Dtsch. Ärzteblatt Int. 2010, 107, 647. [Google Scholar] [CrossRef]
- Molnar, A.O.; Bota, S.; Jeyakumar, N.; McArthur, E.; Battistella, M.; Garg, A.X.; Sood, M.M.; Brimble, K.S. Potentially inappropriate prescribing in older adults with advanced chronic kidney disease. PLoS ONE 2020, 15, e0237868. [Google Scholar] [CrossRef]
- Lohman, M.C.; Cotton, B.P.; Zagaria, A.B.; Bao, Y.; Greenberg, R.L.; Fortuna, K.L.; Bruce, M.L. Hospitalization risk and potentially inappropriate medications among Medicare home health nursing patients. J. Gen. Intern. Med. 2017, 32, 1301–1308. [Google Scholar] [CrossRef]
- Clark, C.M.; Shaver, A.L.; Aurelio, L.A.; Feuerstein, S.; Wahler Jr, R.G.; Daly, C.J.; Jacobs, D.M. Potentially inappropriate medications are associated with increased healthcare utilization and costs. J. Am. Geriatr. Soc. 2020, 68, 2542–2550. [Google Scholar] [CrossRef]
- Alyazeedi, A.; Fouad Algendy, A.; Sharabash, M.; Karawia, A. Prevalence, determinants and associated risk of potentially inappropriate prescribing for older adults in Qatar: A national retrospective study. Clin. Interv. Aging 2019, 14, 1889–1899. [Google Scholar] [CrossRef]
- Su, S.; Gao, L.; Ma, W.; Wang, C.; Cui, X.; Liu, T.; Yan, S. Number-dependent association of potentially inappropriate medications with clinical outcomes and expenditures among community-dwelling older adults: A population-based cohort study. Br. J. Clin. Pharmacol. 2022, 88, 3378–3391. [Google Scholar] [CrossRef]
- Tamura, M.K.; Yaffe, K. Dementia and cognitive impairment in ESRD: Diagnostic and therapeutic strategies. Kidney Int. 2011, 79, 14–22. [Google Scholar] [CrossRef]
- Wang, C.; Song, P.; Niu, Y. The management of dementia worldwide: A review on policy practices, clinical guidelines, end-of-life care, and challenge along with aging population. Biosci. Trends 2022, 16, 119–129. [Google Scholar] [CrossRef]
- Qin, Q.N.X.; Ming, L.C.; Abd Wahab, M.S.; Tan, C.S.; Yuda, A.; Hermansyah, A. Drug-related problems among older people with dementia: A systematic review. Res. Soc. Adm. Pharm. 2023, 19, 873–881. [Google Scholar] [CrossRef]
- Zhao, M.; Chen, Z.; Xu, T.; Fan, P.; Tian, F. Global prevalence of polypharmacy and potentially inappropriate medication in older patients with dementia: A systematic review and meta-analysis. Front. Pharmacol. 2023, 14, 1221069. [Google Scholar] [CrossRef] [PubMed]
- Bergman, H.; Borson, S.; Jessen, F.; Krolak-Salmon, P.; Pirani, A.; Rasmussen, J.; Rodrigo, J.; Taddeo, D. Dementia and comorbidities in primary care: A scoping review. BMC Prim. Care 2023, 24, 277. [Google Scholar] [CrossRef] [PubMed]
- Hamiduzzaman, M.; Kuot, A.; Greenhill, J.; Strivens, E.; Isaac, V. Towards personalized care: Factors associated with the quality of life of residents with dementia in Australian rural aged care homes. PLoS ONE 2020, 15, e0233450. [Google Scholar] [CrossRef] [PubMed]
- Clague, F.; Mercer, S.W.; McLean, G.; Reynish, E.; Guthrie, B. Comorbidity and polypharmacy in people with dementia: Insights from a large, population-based cross-sectional analysis of primary care data. Age Ageing 2017, 46, 33–39. [Google Scholar] [CrossRef]
- Ruangritchankul, S.; Peel, N.M.; Hanjani, L.S.; Gray, L.C. Drug related problems in older adults living with dementia. PLoS ONE 2020, 15, e0236830. [Google Scholar] [CrossRef]
- Banta, J.E. Dementia: Morbidity and Medications; Oxford University Press: Oxford, UK, 2017; pp. 4–5. [Google Scholar]
- Mitchell, S.L.; Teno, J.M.; Kiely, D.K.; Shaffer, M.L.; Jones, R.N.; Prigerson, H.G.; Volicer, L.; Givens, J.L.; Hamel, M.B. The clinical course of advanced dementia. N. Engl. J. Med. 2009, 361, 1529–1538. [Google Scholar] [CrossRef]
- Scott, J.; Owen-Smith, A.; Tonkin-Crine, S.; Rayner, H.; Roderick, P.; Okamoto, I.; Leydon, G.; Caskey, F.; Methven, S. Decision-making for people with dementia and advanced kidney disease: A secondary qualitative analysis of interviews from the Conservative Kidney Management Assessment of Practice Patterns Study. BMJ Open 2018, 8, e022385. [Google Scholar] [CrossRef]
- Pépin, M.; Giannakou, K.; Levassort, H.; Farinha, A.; Bobot, M.; Lo Re, V.; Golenia, A.; Małyszko, J.; Mattace-Raso, F.; Klimkowcz-Mrowiec, A. Care pathways for patients with cognitive impairment and chronic kidney disease. Nephrol. Dial. Transplant. 2025, 40, ii28–ii36. [Google Scholar] [CrossRef]
- Delgado, J.; Bowman, K.; Clare, L. Potentially inappropriate prescribing in dementia: A state-of-the-art review since 2007. BMJ Open 2020, 10, e029172. [Google Scholar] [CrossRef]
- Sönnerstam, E.; Sjölander, M.; Gustafsson, M. Inappropriate prescription and renal function among older patients with cognitive impairment. Drugs Aging 2016, 33, 889–899. [Google Scholar] [CrossRef]
- Alhumaid, S.; Bezabhe, W.M.; Williams, M.; Peterson, G.M. Prevalence and Risk Factors of Inappropriate Drug Dosing among Older Adults with Dementia or Cognitive Impairment and Renal Impairment: A Systematic Review. J. Clin. Med. 2024, 13, 5658. [Google Scholar] [CrossRef] [PubMed]
- Bezabhe, W.M.; Bereznicki, L.R.; Radford, J.; Wimmer, B.C.; Salahudeen, M.S.; Peterson, G.M. Eight-year trends in direct-acting oral anticoagulant dosing, based on age and kidney function, in patients with atrial fibrillation. J. Patient Saf. 2022, 18, 337–341. [Google Scholar] [CrossRef]
- Castelino, R.L.; Saunder, T.; Kitsos, A.; Peterson, G.M.; Jose, M.; Wimmer, B.; Khanam, M.; Bezabhe, W.; Stankovich, J.; Radford, J. Quality use of medicines in patients with chronic kidney disease. BMC Nephrol. 2020, 21, 216. [Google Scholar] [CrossRef] [PubMed]
- Khanal, A.; Peterson, G.M.; Castelino, R.L.; Jose, M.D. Potentially inappropriate prescribing of renally cleared drugs in elderly patients in community and aged care settings. Drugs Aging 2015, 32, 391–400. [Google Scholar] [CrossRef]
- Manski-Nankervis, J.-A.; Thuraisingam, S.; Sluggett, J.K.; Kilov, G.; Furler, J.; O’Neal, D.; Jenkins, A. Prescribing of diabetes medications to people with type 2 diabetes and chronic kidney disease: A national cross-sectional study. BMC Fam. Pract. 2019, 20, 29. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Busingye, D.M.R.; Mina, R.; Thistlethwaite, J.; Belcher, J.; Chidwick, K. MedicineInsight Report: Validation of the MedicineInsight Database: Completeness, Generalisability and Plausibility; NPS MedicineWise: Sydney, Australia, 2020; Available online: https://www.nps.org.au/assets/MedicineInsight-Validation-completeness-representativeness-plausibility_2020.pdf (accessed on 14 November 2024).
- Busingye, D.; Gianacas, C.; Pollack, A.; Chidwick, K.; Merrifield, A.; Norman, S.; Mullin, B.; Hayhurst, R.; Blogg, S.; Havard, A. Data Resource Profile: MedicineInsight, an Australian national primary health care database. Int. J. Epidemiol. 2019, 48, 1741–1741h. [Google Scholar] [CrossRef]
- Khanam, M.A.; Kitsos, A.; Stankovich, J.; Castelino, R.; Jose, M.; Peterson, G.M.; Wimmer, B.; Zaidi, T.R.; Radford, J. Association of continuity of care with blood pressure control in patients with chronic kidney disease and hypertension. Aust. J. Gen. Pract. 2019, 48, 300–306. [Google Scholar] [CrossRef]
- Australian Medicines Handbook 2024 (Online); Australian Medicines Handbook Pty Ltd.: Adelaide, Australia, 2024; Available online: https://amhonline.amh.net.au (accessed on 14 November 2024).
- NPS MedicineWise. MedicineInsight Databook; NPS MedicineWise: Sydney, Australia, 2021; Available online: https://www.nps.org.au/assets/NPS/pdf/MedicineInsight-databook-4.0-December-2021.pdf (accessed on 14 November 2024).
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas (SEIFA). Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 14 November 2024).
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, July 2016. Defining Remoteness Areas. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Latestproducts/1270.0.55.005Main%20Features15July%202016?opendocument&tabname=Summary&prodno=1270.0.55.005&issue=July%202016&num=&view= (accessed on 14 November 2024).
- Iwagami, M.; Shinozaki, T. Introduction to matching in case-control and cohort studies. Ann. Clin. Epidemiol. 2022, 4, 33–40. [Google Scholar] [CrossRef]
- Ripollone, J.E.; Huybrechts, K.F.; Rothman, K.J.; Ferguson, R.E.; Franklin, J.M. Implications of the propensity score matching paradox in pharmacoepidemiology. Am. J. Epidemiol. 2018, 187, 1951–1961. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L.; Andersson, T.; Rosenqvist, M. Less dementia and stroke in low-risk patients with atrial fibrillation taking oral anticoagulation. Eur. Heart J. 2019, 40, 2327–2335. [Google Scholar] [CrossRef]
- Austin, P.C. Propensity-score matching in the cardiovascular surgery literature from 2004 to 2006: A systematic review and suggestions for improvement. J. Thorac. Cardiovasc. Surg. 2007, 134, 1128–1135.e3. [Google Scholar] [CrossRef] [PubMed]
- Lachin, J.M. Power and sample size evaluation for the Cochran–Mantel–Haenszel mean score (Wilcoxon rank sum) test and the Cochran–Armitage test for trend. Stat. Med. 2011, 30, 3057–3066. [Google Scholar] [CrossRef]
- Weisburd, D.; Britt, C.; Wilson, D.B.; Wooditch, A.; Weisburd, D.; Britt, C.; Wilson, D.B.; Wooditch, A. Comparing Means and Proportions in Two Samples to Test Hypotheses About Population Parameters. In Basic Statistics in Criminology and Criminal Justice; Springer: Cham, Switzerland, 2020; pp. 315–371. [Google Scholar]
- Pfister, B.; Jonsson, J.; Gustafsson, M. Drug-related problems and medication reviews among old people with dementia. BMC Pharmacol. Toxicol. 2017, 18, 52. [Google Scholar] [CrossRef]
- Delgado, J.; Jones, L.; Bradley, M.C.; Allan, L.M.; Ballard, C.; Clare, L.; Fortinsky, R.H.; Hughes, C.M.; Melzer, D. Potentially inappropriate prescribing in dementia, multi-morbidity and incidence of adverse health outcomes. Age Ageing 2021, 50, 457–464. [Google Scholar] [CrossRef]
- Lau, E.C.Y.; Jeon, Y.H.; Hilmer, S.N.; Tan, E.C. Prescribing patterns in people living with dementia in the community: A cross-sectional study. Australas. J. Ageing 2025, 44, e13380. [Google Scholar] [CrossRef] [PubMed]
- Hamrahian, S.M. Hypertension and cardiovascular disease in patients with chronic kidney disease. In Approaches to Chronic Kidney Disease: A Guide for Primary Care Providers and Non-Nephrologists; Springer: Cham, Switzerland, 2021; pp. 281–295. [Google Scholar]
- Dincer, N.; Dagel, T.; Afsar, B.; Covic, A.; Ortiz, A.; Kanbay, M. The effect of chronic kidney disease on lipid metabolism. Int. Urol. Nephrol. 2019, 51, 265–277. [Google Scholar] [CrossRef]
- Sinha, A.D.; Agarwal, R. Clinical pharmacology of antihypertensive therapy for the treatment of hypertension in CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 757–764. [Google Scholar] [CrossRef]
- Breton, G.; Froissart, M.; Janus, N.; Launay-Vacher, V.; Berr, C.; Tzourio, C.; Helmer, C.; Stengel, B. Inappropriate drug use and mortality in community-dwelling elderly with impaired kidney function—The Three-City population-based study. Nephrol. Dial. Transplant. 2011, 26, 2852–2859. [Google Scholar] [CrossRef]
- Therapeutic Guidelines Limited. Therapeutic Guidelines: Cardiovascular. Lipid Modification. Version 21; Therapeutic Guidelines Limited: North Melbourne, VIC, Australia, 2025; Available online: https://app-tg-org-au.ezproxy.utas.edu.au/viewTopic?etgAccess=true&guidelinePage=Cardiovascular&topicfile=cardiovascular-disease-risk-stratification&guidelinename=auto§ionId=r_CVG_Lipid-modificationtopic_28#r_CVG_Lipid-modificationtopic_28 (accessed on 14 April 2025).
- Wiggins, B.S.; Saseen, J.J.; Page, R.L.; Reed, B.N.; Sneed, K.; Kostis, J.B.; Lanfear, D.; Virani, S.; Morris, P.B. Recommendations for management of clinically significant drug-drug interactions with statins and select agents used in patients with cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2016, 134, e468–e495. [Google Scholar] [CrossRef]
- Mancini, G.J.; Pearson, G.J.; Barry, A.R.; Couture, P.; Dayan, N.; Francis, G.A.; Genest, J.; Gregoire, J.C.; Hegele, R.A.; Leiter, L.A. Prevention and Management of Cardiovascular Disease in Primary Care: A Comment on the PEER Simplified Lipid Guideline. CJC Open 2024, 6, 1189–1198. [Google Scholar] [CrossRef]
- Zhu, J.X.; Nash, D.M.; McArthur, E.; Farag, A.; Garg, A.X.; Jain, A.K. Nephrology comanagement and the quality of antibiotic prescribing in primary care for patients with chronic kidney disease: A retrospective cross-sectional study. Nephrol. Dial. Transplant. 2019, 34, 642–649. [Google Scholar] [CrossRef]
- Hoang, P.; Salbu, R.L. Updated nitrofurantoin recommendations in the elderly: A closer look at the evidence. Consult. Pharm. 2016, 31, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, F.J.; del Portal, D. Nitrofurantoin. [Updated 2023 May 29]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK470526/ (accessed on 11 March 2025).
- Okoro, R.N.; Farate, V.T. The use of nephrotoxic drugs in patients with chronic kidney disease. Int. J. Clin. Pharm. 2019, 41, 767–775. [Google Scholar] [CrossRef]
- Solak, Y.; Biyik, Z.; Gaipov, A.; Kayrak, M.; Ciray, H.; Cizmecioglu, A.; Tonbul, H.Z.; Turk, S. Drug dose adjustment in dialysis patients admitted in clinics other than internal medicine. Am. J. Ther. 2016, 23, e68–e73. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.A.; Rottura, M.; Cicala, G.; Mandraffino, R.; Marino, S.; Irrera, N.; Mannucci, C.; Santoro, D.; Squadrito, F.; Arcoraci, V. Chronic kidney disease management in general practice: A focus on inappropriate drugs prescriptions. J. Clin. Med. 2020, 9, 1346. [Google Scholar] [CrossRef] [PubMed]
- MacRae, C.; Mercer, S.; Guthrie, B. Potentially inappropriate primary care prescribing in people with chronic kidney disease: A cross-sectional analysis of a large population cohort. Br. J. Gen. Pract. 2021, 71, e483–e490. [Google Scholar] [CrossRef]
- Silva-Almodóvar, A.; Hackim, E.; Wolk, H.; Nahata, M.C. Potentially inappropriately prescribed medications among Medicare medication therapy management eligible patients with chronic kidney disease: An observational analysis. J. Gen. Intern. Med. 2021, 36, 2346–2352. [Google Scholar] [CrossRef]
- Zuber, K.; Liles, A.M.; Davis, J. Medication dosing in patients with chronic kidney disease. JAAPA 2013, 26, 19–25. [Google Scholar] [CrossRef]
- Deed, G.; Ackermann, E.; Arthur, I.; Barlow, J.; Jagadeesan, S.; Kawol, D.; Kilov, G.; Leow, S.; Manski-Nankervis, J.-A.; Rasalam, R. General Practice Management of Type 2 Diabetes: 2016–18. Royal Australian College of General Practitioners (RACGP); RACGP: East Melbourne, VIC, Australia, 2016. [Google Scholar]
- Alhumaid, S.; Bezabhe, W.M.; Williams, M.; Peterson, G.M. Trends in renal function testing in patients with dementia: A repeated cross-sectional analysis in Australian general practice. J. Nephrol. 2025, 1–9. [Google Scholar] [CrossRef]
- Barmano, N.; Walfridsson, U.; Walfridsson, H.; Karlsson, J.-E. Structured care of patients with atrial fibrillation improves guideline adherence. J. Atr. Fibrillation 2016, 9, 1498. [Google Scholar] [CrossRef] [PubMed]
- Brieger, D.; Amerena, J.; Attia, J.R.; Bajorek, B.; Chan, K.H.; Connell, C.; Freedman, B.; Ferguson, C.; Hall, T.; Haqqani, H.M. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Med. J. Aust. 2018, 209, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Lane, D.A. Stroke prevention in atrial fibrillation: A systematic review. JAMA 2015, 313, 1950–1962. [Google Scholar] [CrossRef]
- Bezabhe, W.M.; Bereznicki, L.R.; Radford, J.; Wimmer, B.C.; Curtain, C.; Salahudeen, M.S.; Peterson, G.M. Factors influencing oral anticoagulant use in patients newly diagnosed with atrial fibrillation. Eur. J. Clin. Investig. 2021, 51, e13457. [Google Scholar] [CrossRef]
- Kefale, A.T.; Bezabhe, W.M.; Peterson, G.M. Oral anticoagulant use in patients with atrial fibrillation at low risk of stroke and associated bleeding complications. J. Clin. Med. 2023, 12, 6182. [Google Scholar] [CrossRef] [PubMed]
- Kefale, B.; Peterson, G.M.; Mirkazemi, C.; Dwyer, N.B.; Salahudeen, M.S.; Radford, J.; Boland, C.M.; Bezabhe, W.M. Does hospitalisation improve oral anticoagulant optimisation in patients with atrial fibrillation? Eur. J. Clin. Investig. 2025, 55, e70011. [Google Scholar] [CrossRef]
- Tesfaye, W.H.; Castelino, R.L.; Wimmer, B.C.; Zaidi, S.T.R. Inappropriate prescribing in chronic kidney disease: A systematic review of prevalence, associated clinical outcomes and impact of interventions. Int. J. Clin. Pract. 2017, 71, e12960. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Before Matching | Propensity-Score Matched | ||||
|---|---|---|---|---|---|---|
| Dementia (n = 4092) | Non-Dementia (n = 29,009) | Standardized Differences * | Dementia (n = 4041) | Non-Dementia (n = 8031) | Standardized Differences * | |
| Age (years), median (IQR) | 81 (76–86) | 82 (77–87) | 0.167 | 81 (76–86) | 81 (76–86) | 0.005 |
| Age group (years) | 0.159 | 0.013 | ||||
| 65–74 | 855 (20.9) | 4555 (15.7) | 840 (20.8) | 1620 (20.2) | ||
| 75–84 | 1919 (46.9) | 13,344 (46) | 1895 (46.9) | 3789 (47.2) | ||
| ≥85 | 1318 (32.2) | 11,110 (38.3) | 1306 (32.3) | 2622 (32.6) | ||
| Sex-female (%) | 2355 (57.6) | 16,982 (58.4) | 0.016 | 2329 (57.6) | 4641 (57.8) | 0.003 |
| Index year (%) | 0.356 | −0.014 | ||||
| 2011–2012 | 913 (22.3) | 4312 (14.9) | 894 (22.1) | 1906 (23.7) | ||
| 2013–2014 | 886 (21.7) | 4755 (16.4) | 874 (21.6) | 1781 (22.2) | ||
| 2015–2016 | 825 (20.2) | 4966 (17.1) | 814 (20.1) | 1486 (18.5) | ||
| 2017–2018 | 793 (19.4) | 5974 (20.6) | 786 (19.5) | 1338 (16.7) | ||
| 2019–2020 | 675 (16.5) | 9002 (31) | 673 (16.7) | 1520 (18.9) | ||
| Aboriginal and Torres Strait Islander (%) | 0.041 | −0.017 | ||||
| Yes | 31 (0.8) | 191 (0.7) | 31 (0.8) | 48 (0.6) | ||
| No | 3284 (80.3) | 23,807 (82.1) | 3243 (80.3) | 6418 (79.9) | ||
| Unknown | 777 (19) | 5011 (17.3) | 767 (19) | 1565 (19.5) | ||
| Rurality (%) | −0.091 | −0.015 | ||||
| Outer regional, remote and very remote | 2155 (52.7) | 16,342 (56.3) | 2150 (53.2) | 4245 (52.9) | ||
| Inner regional | 1314 (32.1) | 9170 (31.6) | 1308 (32.4) | 2743 (34.2) | ||
| Major cities | 591 (14.4) | 3361 (11.6) | 583 (14.4) | 1043 (13) | ||
| SEIFA quintiles (%) | 0.041 | −0.002 | ||||
| 1 (least advantaged) | 878 (21.5) | 6214 (21.4) | 872 (21.6) | 1758 (21.9) | ||
| 2 | 995 (24.3) | 6625 (22.8) | 991 (24.5) | 1998 (24.9) | ||
| 3 | 745 (18.2) | 5359 (18.5) | 739 (18.3) | 1495 (18.6) | ||
| 4 | 690 (16.9) | 4547 (15.7) | 686 (17) | 1147 (14.3) | ||
| 5 (most advantaged) | 754 (18.4) | 6141 (21.2) | 753 (18.6) | 1633 (20.3) | ||
| General practice site (state location) | −0.055 | −0.009 | ||||
| New South Wales/Australian Capital Territory | 1740 (42.5) | 12,640 (43.6) | 1713 (42.4) | 3369 (41.9) | ||
| Victoria | 748 (18.3) | 5956 (20.5) | 742 (18.4) | 1655 (20.6) | ||
| Queensland | 663 (16.2) | 4486 (15.5) | 656 (16.2) | 1222 (15.2) | ||
| Western Australia | 332 (8.1) | 1992 (6.9) | 328 (8.1) | 583 (7.3) | ||
| South Australia/Northern Territory | 108 (2.6) | 665 (2.3) | 108 (2.7) | 174 (2.2) | ||
| Tasmania | 501 (12.2) | 3270 (11.3) | 494 (12.2) | 1028 (12.8) | ||
| Number of visits to the GP in the preceding 2 years | 0.019 | 0.007 | ||||
| 3–5 GP visits | 487 (11.9) | 3043 (10.5) | 479 (11.9) | 874 (10.9) | ||
| 6–14 GP visits | 1101 (26.9) | 8235 (28.4) | 1090 (27) | 2284 (28.4) | ||
| ≥15 GP visits | 2504 (61.2) | 17,731 (61.1) | 2472 (61.2) | 4873 (60.7) | ||
| Number of renally-dependent drugs prescribed (out of the 33 drugs of interest) | −0.009 | −0.036 | ||||
| 1 drug | 2532 (61.9) | 17,900 (61.7) | 2501 (61.9) | 5043 (62.8) | ||
| 2 drugs | 1026 (25.1) | 7570 (26.1) | 1010 (25) | 2068 (25.8) | ||
| ≥3 drugs | 534 (13) | 3539 (12.2) | 530 (13.1) | 920 (11.5) | ||
| Comorbidities | ||||||
| Heart failure | 874 (21.4) | 6959 (24) | 0.063 | 861 (21.3) | 1913 (23.8) | 0.060 |
| Hypertension | 3072 (75.1) | 22,290 (76.8) | 0.041 | 3033 (75.1) | 6039 (75.2) | 0.003 |
| Stroke | 1055 (25.8) | 5311 (18.3) | −0.181 | 1032 (25.5) | 2030 (25.3) | −0.006 |
| Atrial fibrillation | 1268 (31) | 9231 (31.8) | 0.018 | 1253 (31) | 2528 (31.5) | 0.010 |
| Atrial flutter | 87 (2.1) | 672 (2.3) | 0.013 | 87 (2.2) | 179 (2.2) | 0.005 |
| Anxiety | 1161 (28.4) | 5766 (19.9) | −0.199 | 1142 (28.3) | 2242 (27.9) | −0.008 |
| Arthritis | 2874 (70.2) | 20,483 (70.6) | 0.008 | 2842 (70.3) | 5631 (70.1) | −0.005 |
| Asthma | 711 (17.4) | 5468 (18.8) | 0.038 | 700 (17.3) | 1378 (17.2) | −0.004 |
| Diabetes | 1370 (33.5) | 9324 (32.1) | −0.028 | 1351 (33.4) | 2655 (33.1) | −0.008 |
| Deep vein thrombosis | 83 (2) | 657 (2.3) | 0.016 | 81 (2) | 178 (2.2) | 0.015 |
| Depression | 1840 (45) | 8103 (27.9) | −0.360 | 1802 (44.6) | 3542 (44.1) | −0.010 |
| Cancer | 2064 (50.4) | 14,171 (48.9) | −0.032 | 2031 (50.3) | 3974 (49.5) | −0.015 |
| Coronary heart disease | 1336 (32.6) | 9540 (32.9) | 0.005 | 1315 (32.5) | 2618 (32.6) | 0.001 |
| Chronic kidney disease | 315 (7.7) | 2384 (8.2) | 0.019 | 312 (7.7) | 580 (7.2) | −0.019 |
| Chronic liver disease | 35 (0.9) | 233 (0.8) | −0.006 | 35 (0.9) | 63 (0.8) | −0.009 |
| Chronic obstructive pulmonary disease | 758 (18.5) | 5296 (18.3) | −0.007 | 745 (18.4) | 1472 (18.3) | −0.003 |
| Substance abuse | 149 (3.6) | 668 (2.3) | −0.079 | 144 (3.6) | 278 (3.5) | −0.005 |
| Osteoporosis | 1499 (36.6) | 10,775 (37.1) | 0.010 | 1485 (36.7) | 2928 (36.5) | −0.006 |
| Pain | 1972 (48.2) | 13,779 (47.5) | −0.014 | 1948 (48.2) | 3905 (48.6) | 0.008 |
| Schizophrenia | 76 (1.9) | 168 (0.6) | −0.121 | 65 (1.6) | 93 (1.2) | −0.039 |
| eGFR (mL/min/1.73 m2), median (IQR) | 53 (39–65) | 51 (37–64) | −0.083 | 53 (39–65) | 52 (38–65) | −0.035 |
| eGFR category (mL/min/1.73 m2) | −0.084 | −0.061 | ||||
| ≥30 | 3617 (88.4) | 24,827 (85.6) | 3571 (88.4) | 6935 (86.4) | ||
| <30 | 475 (11.6) | 4182 (14.4) | 470 (11.6) | 1096 (13.6) | ||
| Medicines ¶ | Patients Prescribed N (%) | Patients with Inappropriate Use of Drug N (%) | Medicines ¶ | Patients Prescribed N (%) | Patients with Inappropriate Use of Drug N (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Dementia | Control | Dementia | Control | Dementia | Control | Dementia | Control | ||
| Antidiabetic Medicines | Psychotropic Medicines | ||||||||
| Sitagliptin | 8 (0.2) | 30 (0.4) | <5 | 8 (26.7) | Paroxetine | 70 (1.7) | 156 (1.9) | <5 | - |
| Alogliptin | - | <5 | - | <5 | Duloxetine | 88 (2.2) | 175 (2.2) | 5 (5.7) | 12 (6.8) |
| Saxagliptin | <5 | <5 | - | - | Risperidone | 112 (2.8) | 58 (0.7) | - | <5 |
| Vildagliptin | <5 | <5 | <5 | <5 | Anti-dementia medicines | ||||
| Metformin | 374 (9.2) | 654 (8.1) | 100 (26.7) | 178 (27.2) | Memantine | 35 (0.9) | 20 (0.2) | - | <5 |
| Antihypertensive medicines | Galantamine | 29 (0.7) | 47 (0.6) | - | - | ||||
| Olmesartan | 70 (1.7) | 151 (1.9) | 6 (8.6) | 12 (7.9) | Antihistamines | ||||
| Valsartan | 52 (1.3) | 124 (1.5) | 7 (13.5) | 14 (11.3) | Famotidine | 13 (0.3) | 32 (0.4) | <5 | 13 (40.6) |
| Spironolactone | 121 (3) | 388 (4.8) | 27 (22.3) | 126 (32.5) | Nizatidine | 36 (0.9) | 72 (0.9) | 10 (27.8) | 35 (48.6) |
| Moxonidine | 47 (1.2) | 136 (1.7) | 15 (31.9) | 40 (29.4) | Anticoagulant medicines | ||||
| Antibiotics | Dabigatran | 55 (1.4) | 103 (1.3) | <5 | 11 (10.7) | ||||
| Nitrofurantoin | 64 (1.6) | 108 (1.3) | 40 (62.5) | 72 (66.7) | Apixaban | 197 (4.9) | 371 (4.6) | 8 (4.1) | 29 (7.8) |
| Lipid lowering medicines | Rivaroxaban | 180 (4.4) | 330 (4.1) | 44 (24.4) | 77 (23.3) | ||||
| Fenofibrate | 49 (1.2) | 105 (1.3) | 33 (67.3) | 67 (63.8) | Neurological medicines | ||||
| Gemfibrozil | 7 (0.2) | 30 (0.4) | <5 | 7 (23.3) | Pregabalin | 346 (8.6) | 886 (11) | <5 | 37 (4.2) |
| Rosuvastatin | 714 (17.7) | 1432 (17.8) | 31 (4.3) | 63 (4.4) | Antiarrhythmics | ||||
| Analgesic, antipyretic and anti-inflammatory medicines | Digoxin | 443 (11) | 954 (11.9) | <5 | 6 (0.6) | ||||
| Diclofenac | 71 (1.7) | 157 (1.9) | <5 | 5 (3.2) | |||||
| Ibuprofen | 55 (1.4) | 94 (1.2) | <5 | <5 | |||||
| Indomethacin | 30 (0.7) | 39 (0.5) | <5 | <5 | |||||
| Mefenamic acid | - | <5 | - | - | |||||
| Naproxen | 41 (1) | 102 (1.3) | <5 | 9 (8.8) | |||||
| Meloxicam | 228 (5.6) | 601 (7.5) | 11 (4.8) | 31 (5.1) | |||||
| Celecoxib | 190 (4.7) | 412 (5.1) | 12 (6.3) | 23 (5.6) | |||||
| Etoricoxib | <5 | - | - | - | |||||
| N | At Least One Inappropriate Prescription, n (%) | Unadjusted | Adjusted § | |||
|---|---|---|---|---|---|---|
| OR (95% CI) ¶ | p Value | OR (95% CI) ¶ | p Value | |||
| Age | ||||||
| <75 | 855 | 59 (6.9) | Ref | Ref | ||
| ≥75 | 3237 | 322 (9.9) | 1.49 (1.12–1.99) | 0.007 | 1.13 (0.82–1.56) | 0.438 |
| Gender | ||||||
| Females | 2355 | 210 (8.9) | Ref | Ref | ||
| Males | 1737 | 171 (9.8) | 1.11 (0.90–1.38) | 0.313 | 1.21 (0.95–1.54) | 0.125 |
| Index year | <0.001 | 0.483 | ||||
| 2011–2012 | 913 | 66 (7.2) | Ref | Ref | ||
| 2013–2014 | 886 | 96 (10.8) | 1.56 (1.12–2.16) | 0.008 | 1.34 (0.93–1.93) | 0.122 |
| 2015–2016 | 825 | 80 (9.7) | 1.38 (0.98–1.94) | 0.065 | 1.14 (0.78–1.67) | 0.510 |
| 2017–2018 | 793 | 76 (9.6) | 1.36 (0.96–1.92) | 0.080 | 1.08 (0.73–1.59) | 0.693 |
| 2019–2020 | 675 | 63 (9.3) | 1.32 (0.92–1.89) | 0.130 | 1.32 (0.88–1.97) | 0.173 |
| Rurality | <0.001 | 0.661 | ||||
| Major cities | 591 | 49 (8.3) | Ref | Ref | ||
| Outer regional/remote/very remote | 2155 | 197 (9.1) | 1.11 (0.80–1.54) | 0.521 | 1.14 (0.76–1.71) | 0.520 |
| Inner regional | 1314 | 132 (10) | 1.23 (0.88–1.74) | 0.228 | 1.20 (0.81–1.76) | 0.363 |
| SEIFA quintiles | <0.001 | 0.310 | ||||
| 1 (least advantaged) | 878 | 78 (8.9) | 1.15 (0.81–1.63) | 0.442 | 0.81 (0.53–1.27) | 0.369 |
| 2 | 995 | 100 (10.1) | 1.32 (0.94–1.84) | 0.110 | 1.11 (0.74–1.65) | 0.624 |
| 3 | 745 | 75 (10.1) | 1.32 (0.92–1.88) | 0.129 | 1.20 (0.80–1.81) | 0.371 |
| 4 | 690 | 66 (9.6) | 1.25 (0.86–1.80) | 0.241 | 1.14 (0.76–1.72) | 0.524 |
| 5 (most advantaged) | 754 | 59 (7.8) | Ref | Ref | ||
| eGFR category (mL/min/1.73 m2) | ||||||
| ≥30 | 3617 | 179 (4.9) | Ref | Ref | ||
| <30 | 475 | 202 (42.5) | 14.21 (11.22–18.00) | <0.001 | 15.13 (11.71–19.56) | <0.001 |
| Comorbidities | ||||||
| Hypertension | 3072 | 321 (10.4) | 1.87 (1.40–2.48) | <0.001 | 1.24 (0.91–1.70) | 0.174 |
| Stroke | 1055 | 106 (10) | 1.12 (0.89–1.42) | 0.339 | 0.94 (0.71–1.23) | 0.645 |
| Diabetes | 1370 | 200 (14.6) | 2.40 (1.94–2.97) | <0.001 | 2.22 (1.74–2.83) | <0.001 |
| Cancer | 2064 | 200 (9.7) | 1.09 (0.89–1.35) | 0.400 | 0.94 (0.74–1.20) | 0.624 |
| Chronic obstructive pulmonary disease | 758 | 67 (8.8) | 0.93 (0.71–1.23) | 0.620 | 0.80 (0.58–1.10) | 0.167 |
| Atrial fibrillation | 1268 | 100 (7.9) | 0.77 (0.61–0.98) | 0.036 | 0.60 (0.46–0.79) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhumaid, S.; Bezabhe, W.M.; Williams, M.; Peterson, G.M. Ten-Year Trend in the Potentially Inappropriate Prescribing of Renally-Dependent Medicines in Australian General Practice Patients with Dementia. J. Clin. Med. 2025, 14, 4734. https://doi.org/10.3390/jcm14134734
Alhumaid S, Bezabhe WM, Williams M, Peterson GM. Ten-Year Trend in the Potentially Inappropriate Prescribing of Renally-Dependent Medicines in Australian General Practice Patients with Dementia. Journal of Clinical Medicine. 2025; 14(13):4734. https://doi.org/10.3390/jcm14134734
Chicago/Turabian StyleAlhumaid, Saad, Woldesellassie M. Bezabhe, Mackenzie Williams, and Gregory M. Peterson. 2025. "Ten-Year Trend in the Potentially Inappropriate Prescribing of Renally-Dependent Medicines in Australian General Practice Patients with Dementia" Journal of Clinical Medicine 14, no. 13: 4734. https://doi.org/10.3390/jcm14134734
APA StyleAlhumaid, S., Bezabhe, W. M., Williams, M., & Peterson, G. M. (2025). Ten-Year Trend in the Potentially Inappropriate Prescribing of Renally-Dependent Medicines in Australian General Practice Patients with Dementia. Journal of Clinical Medicine, 14(13), 4734. https://doi.org/10.3390/jcm14134734