
The Safety of Apixaban Compared to Warfarin in Hospitalized Patients with Acute Kidney Injury

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Site and Design
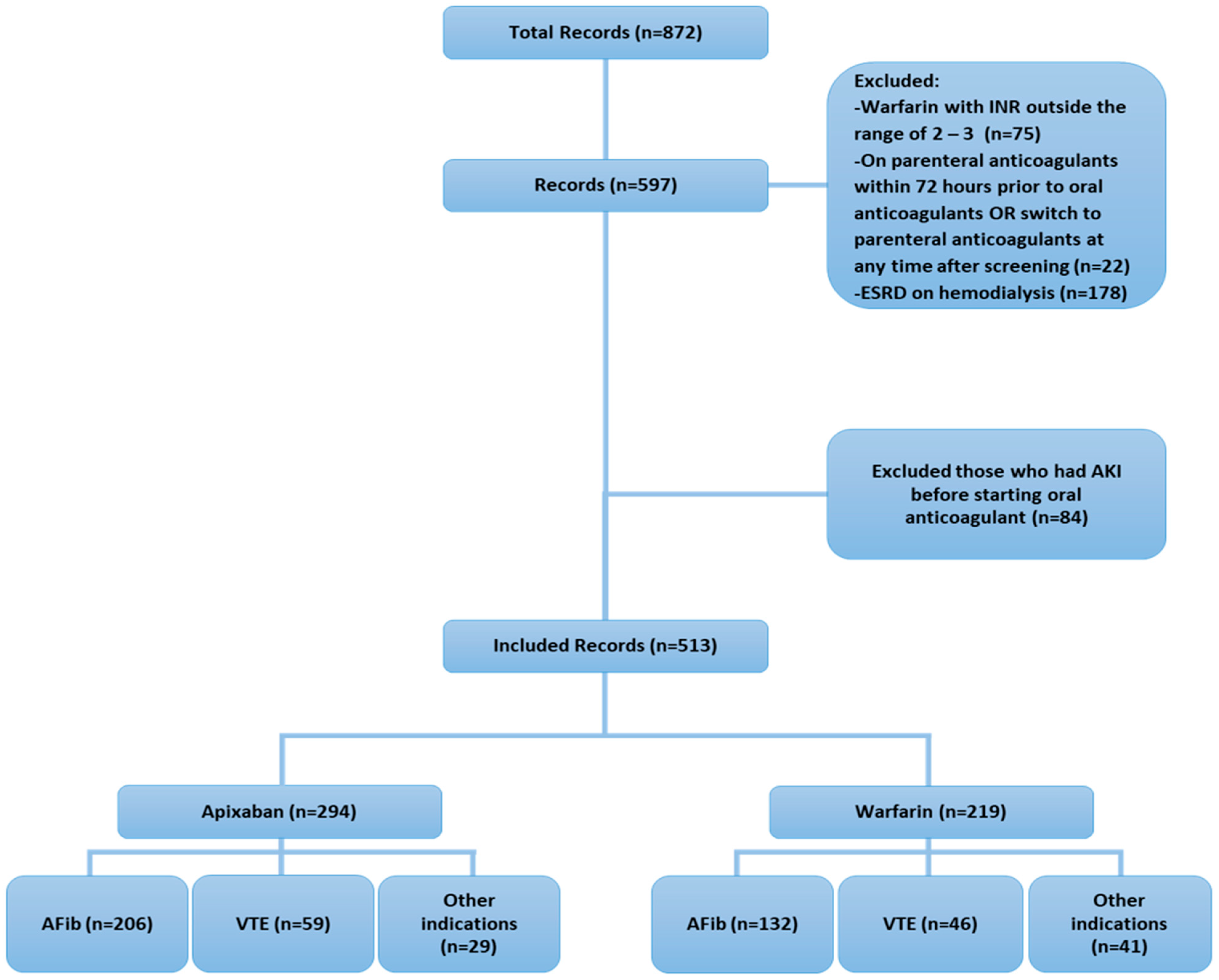
2.2. Study Subjects
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Outcomes
3.3. Subgroup Analysis of Clinical Outcomes
3.4. Multivariable Analysis of Factors Associated with Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e200. [Google Scholar] [CrossRef]
- Atreja, N.; Johannesen, K.; Subash, R.; Bektur, C.; Hagan, M.; Hines, D.M.; Dunnett, I.; Stawowczyk, E. US cost-effectiveness analysis of apixaban compared with warfarin, dabigatran and rivaroxaban for nonvalvular atrial fibrillation, focusing on equal value of life years and health years in total. J. Comp. Eff. Res. 2025, 14, e240163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Ingason, A.B.; Hreinsson, J.P.; Agustsson, A.S.; Lund, S.H.; Rumba, E.; Palsson, D.A.; Reynisson, I.E.; Gudmundsdottir, B.R.; Onundarson, P.T.; Bjornsson, E.S. Comparison of the effectiveness and safety of direct oral anticoagulants: A nationwide propensity score–weighted study. Blood Adv. 2023, 7, 2564–2572. [Google Scholar] [CrossRef] [PubMed]
- Ellenbogen, M.I.; Ardeshirrouhanifard, S.; Segal, J.B.; Streiff, M.B.; Deitelzweig, S.B.; Brotman, D.J. Safety and effectiveness of apixaban versus warfarin for acute venous thromboembolism in patients with end-stage kidney disease: A national cohort study. J. Hosp. Med. 2022, 17, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Sah, J.; Dhamane, A.D.; Lee, T.; Rosenblatt, L.; Hlavacek, P.; Emir, B.; Delinger, R.; Yuce, H.; Luo, X. Effectiveness and Safety of Apixaban versus Warfarin in Venous Thromboembolism Patients with Chronic Kidney Disease. Thromb. Haemost. 2022, 122, 926–938. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Frost, C.; Song, Y.; Barrett, Y.C.; Wang, J.; Schuster, A.; Barrett, M.; LaCreta, F. A randomized direct comparison of the pharmacokinetics and pharmacodynamics of apixaban and rivaroxaban. Clin. Pharmacol. 2014, 6, 179–187. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vio, R.; Proietti, R.; Rigato, M.; Calò, L.A. Clinical Evidence for the Choice of the Direct Oral Anticoagulant in Patients with Atrial Fibrillation According to Creatinine Clearance. Pharmaceuticals 2021, 14, 279. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kister, T.S.; Remmler, J.; Schmidt, M.; Federbusch, M.; Eckelt, F.; Isermann, B.; Richter, H.; Wehner, M.; Krause, U.; Halbritter, J.; et al. Acute kidney injury and its progression in hospitalized patients—Results from a retrospective multicentre cohort study with a digital decision support system. PLoS ONE 2021, 16, e0254608. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Khwaja, A. KDIGO clinical practice guideline for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Givens, G.; Neu, D.; Marler, J. The Risk of Major Bleeding with Apixaban Administration in Patients with Acute Kidney Injury. Ann. Pharmacother. 2023, 57, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Zarka, F.; Tayler-Gomez, A.; Ducruet, T.; Duca, A.; Albert, M.; Bernier-Jean, A.; Bouchard, J. Risk of incident bleeding after acute kidney injury: A retrospective cohort study. J. Crit. Care 2020, 59, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.S.; Lin, M.S.; Wu, V.C.; Chen, Y.L.; Chang, J.J.; Chu, P.H.; Lip, G.Y.H.; Chen, M.C. Differential Presentations of Arterial Thromboembolic Events Between Venous Thromboembolism and Atrial Fibrillation Patients. Front. Cardiovasc. Med. 2021, 8, 775564. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shariff, N.; Aleem, A.; Singh, M.; ZLi, Y.; Smith, S.J. AF and Venous Thromboembolism—Pathophysiology, Risk Assessment and CHADS-VASc score. J. Atr. Fibrillation 2012, 5, 649. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vu, A.; Qu, T.T.; Ryu, R.; Nandkeolyar, S.; Jacobson, A.; Hong, L.T. Critical Analysis of Apixaban Dose Adjustment Criteria. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211021158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bristol-Myers Squibb Company. Eliquis (Apixaban) [Package Insert]; Bristol-Myers Squibb Company: Princeton, NJ, USA, 2021. [Google Scholar]
- Pokorney, S.D.; Chertow, G.M.; Al-Khalidi, H.R.; Gallup, D.; Dignacco, P.; Mussina, K.; Bansal, N.; Gadegbeku, C.A.; Garcia, D.A.; Garonzik, S.; et al. Apixaban for Patients With Atrial Fibrillation on Hemodialysis: A Multicenter Randomized Controlled Trial. Circulation 2022, 146, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Reinecke, H.; Engelbertz, C.; Bauersachs, R.; Breithardt, G.; Echterhoff, H.H.; Gerß, J.; Haeusler, K.G.; Hewing, B.; Hoyer, J.; Juergensmeyer, S.; et al. A Randomized Controlled Trial Comparing Apixaban with the Vitamin K Antagonist Phenprocoumon in Patients on Chronic Hemodialysis: The AXADIA-AFNET 8 Study. Circulation 2023, 147, 296–309. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Characteristics | Overall (n = 513) | Apixaban (n = 294) | Warfarin (n = 219) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age | 73.4 ± 13.9 | 75 ± 13.0 | 71.3 ± 14.7 | 0.0028 |
| Gender | 0.4584 | |||
| Male | 251 (48.9) | 148 (50.3) | 103 (47.0) | |
| Female | 262 (51.1) | 146 (49.7) | 116 (53.0) | |
| Comorbidities * | ||||
| Hypertension | 427 (83.2) | 248 (84.4) | 179 (81.7) | 0.4323 |
| Diabetes Miletus | 372 (72.5) | 223 (75.9) | 149 (68.0) | 0.0499 |
| Heart Failure | 195 (38.0) | 117 (39.8) | 78 (35.6) | 0.3347 |
| Chronic Kidney Disease | 177 (34.5) | 94 (32.0) | 83 (37.9) | 0.1625 |
| Dyslipidemia | 152 (29.6) | 101 (34.4) | 51 (23.3) | 0.0066 |
| Ischemic Heart Disease | 124 (24.2) | 85 (28.9) | 39 (17.8) | 0.0037 |
| Respiratory Disease | 80 (15.6) | 46 (15.6) | 34 (15.5) | 0.9702 |
| Hypothyroidism | 72 (14.0) | 38 (12.9) | 34 (15.5) | 0.4017 |
| Liver Disease | 55 (10.7) | 29 (9.9) | 26 (11.9) | 0.4671 |
| Stroke | 33 (6.4) | 20 (6.8) | 13 (5.9) | 0.6923 |
| Indication | 0.0060 | |||
| Atrial Fibrillation | 340 (66.3) | 208 (70.7) | 132 (60.3) | |
| DVT | 54 (10.5) | 27 (9.2) | 27 (12.3) | |
| PE | 49 (9.6) | 31 (10.5) | 18 (8.2) | |
| DVT+PE | 6 (1.2) | 4 (1.4) | 2 (0.9) | |
| Other | 64 (12.5) | 24 (8.2) | 40 (18.3) | |
| Drug–Drug interaction | 199 (38.8) | 116 (39.5) | 83 (37.9) | 0.7205 |
| Drug–Drug interaction category | ||||
| Strong | 10 (1.9) | 7 (2.4) | 3 (1.4) | 0.7311 |
| Moderate | 162 (31.6) | 93 (31.6) | 69 (31.5) | |
| Pharmacodynamic | 27 (5.3) | 16 (5.4) | 11 (5.0) | |
| Thromboembolic and Bleeding Risk | ||||
| Chadsvasc Score | 4.6 ± 1.4 | 4.8 ± 1.4 | 4.3 ± 1.4 | 0.0150 |
| HAS-BLED Score | 2.7 ± 1.0 | 2.7 ± 1.0 | 2.8 ± 1.1 | 0.9292 |
| Laboratory values | ||||
| Baseline SCr, | 1.7 ± 1.2 | 1.7 ± 1.2 | 1.8 ± 1.2 | 0.3837 |
| SCr admission | 3.2 ± 2.2 | 3.1 ± 2.1 | 3.5 ± 2.5 | 0.1052 |
| Pre-transfusion HgB ** | 74.3 ± 21.7 | 74.6 ± 21.7 | 74.1 ± 22.4 | 0.6152 |
| AKI Stages *** | 0.2351 | |||
| Stage 1 | 327 (63.7) | 189 (64.3) | 138 (63.0) | |
| Stage 2 | 104 (20.3) | 61 (20.7) | 43 (19.6) | |
| Stage 3 | 66 (12.9) | 32 (10.9) | 34 (15.5) | |
| Not documented | 16 (3.1) | 12 (4.1) | 4 (1.8) | |
| SCr fold changes from baseline | 2.1 ± 1.5 | 2.1 ± 1.4 | 2.2 ± 1.5 | 0.2976 |
| Overall (n = 513) | Apixaban (n = 294) | Warfarin (n = 219) | p-Value | |
|---|---|---|---|---|
| Major bleeding | 26 (5.1) | 10 (3.4) | 16 (7.3) | 0.0461 |
| Minor bleeding | 31 (6.0) | 19 (6.5) | 12 (5.5) | 0.6439 |
| Blood transfusion | 48 (9.4) | 24 (8.2) | 24 (11.0) | 0.2822 |
| Thrombotic event | 35 (6.8) | 19 (6.5) | 16 (7.3) | 0.7079 |
| Type of thrombotic event | 0.4728 | |||
| DVT | 14 (2.7) | 8 (2.7) | 6 (2.7) | |
| PE | 5 (1.0) | 4 (1.4) | 1 (0.5) | |
| Stroke | 10 (1.9) | 5 (1.7) | 5 (2.3) | |
| Other | 6 (1.2) | 2 (0.7) | 4 (1.8) | |
| Readmission or ED visit | 202 (39.4) | 115 (39.1) | 87 (39.7) | 0.8887 |
| Death | 41 (8.0) | 26 (8.8) | 15 (6.8) | 0.4100 |
| Outcomes | Indication | AKI Stage * | ||||
|---|---|---|---|---|---|---|
| Atrial Fibrillation (n = 340) | Other Indications (VTE and Others) (n = 173) | p-Value † | Stage 1 (n = 327) | Stages 2 or 3 (n = 170) | p-Value † | |
| Major bleeding | 13 (3.8) | 13 (7.5) | 0.0716 | 10 (3.1) | 16 (9.4) | 0.0025 |
| Minor bleeding | 23 (6.8) | 8 (4.6) | 0.3361 | 17 (5.2) | 13(7.7) | 0.2769 |
| Blood transfusion | 29 (8.5) | 19 (11.0) | 0.3670 | 23 (7.0) | 25 (14.7) | 0.0060 |
| Thrombotic event | 17 (5.0) | 18 (10.4) | 0.0217 | 23 (7.0) | 10 (5.9) | 0.6248 |
| Readmission or ED visit | 135 (39.7) | 67 (38.7) | 0.8304 | 126 (38.5) | 73 (42.9) | 0.3413 |
| Death | 26 (7.7) | 15 (8.7) | 0.6861 | 21 (6.4) | 19 (11.2) | 0.0645 |
| Variables/Outcomes | Major Bleeding | Thrombotic Events | Mortality | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | OR (95% CI) * | No | Yes | OR (95% CI) * | No | Yes | OR (95% CI) * | |
| Age | 73.7 ± 13.8 | 69.5 ± 14.4 | --- | 73.5 ± 13.9 | 72.7 ± 13.3 | --- | 73.1 ± 14.0 | 77.9 ± 11.2 | --- |
| Medication, warfarin | 203 (92.7) | 16 (7.3) | Ref | 203 (92.7) | 16 (7.3) | --- | 204 (93.2) | 15 (6.8) | --- |
| Apixaban | 284 (96.6) | 10 (3.4) | 0.42 (0.18–0.96) | 275 (93.5) | 19 (6.5) | --- | 268 (91.2) | 26 (8.8) | --- |
| Gender, female (vs. male) | 247 (94.3) | 15 (5.7) | --- | 243 (92.7) | 19 (7.3) | --- | 239 (91.2) | 23 (8.8) | --- |
| Comorbidities | |||||||||
| Hypertension | 407 (95.3) | 20 (4.7) | --- | 396 (92.7) | 31 (7.3) | 2.21 (0.72–6.76) | 393 (92.0) | 34 (8.0) | --- |
| Diabetes Miletus | 352 (94.6) | 20 (5.4) | --- | 348 (93.5) | 24 (6.5) | --- | 342 (91.9) | 30 (8.1) | --- |
| Heart Failure | 184 (94.4) | 11 (5.6) | --- | 186 (95.4) | 9 (4.6) | --- | 174 (89.2) | 21 (10.8) | 2.08 (1.04–4.13) |
| Chronic Kidney Disease | 168 (94.9) | 9 (5.1) | --- | 165 (93.2) | 12 (6.8) | --- | 166 (93.8) | 11 (6.2) | 0.61 (0.29–1.27) |
| Dyslipidemia | 142 (93.4) | 10 (6.6) | 1.77 (0.77–4.07) | 139 (91.4) | 13 (8.6) | --- | 136 (89.5) | 16 (10.5) | --- |
| Ischemic Heart Disease | 117 (94.4) | 7 (5.6) | --- | 117 (94.4) | 7 (5.6) | --- | 114 (91.9) | 10 (8.1) | --- |
| Respiratory Disease | 73 (91.3) | 7 (8.8) | 2.15 (0.86–5.34) | 72 (90.0) | 8 (10.0) | 2.14 (0.89–5.13) | 72 (90.0) | 8 (10.0) | --- |
| Hypothyroidism | 69 (95.8) | 3 (4.2) | --- | 67 (93.1) | 5 (6.9) | --- | 64 (88.9) | 8 (11.1) | 1.79 (0.77–4.16) |
| Liver Disease | 50 (90.9) | 5 (9.1) | 2.10 (0.75–5.91) | 50 (90.9) | 5 (9.1) | --- | 50 (90.9) | 5 (9.1) | --- |
| Stroke | 32 (97.0) | 1 (3.0) | --- | 28 (84.8) | 5 (15.2) | 2.92 (1.01–8.41) | 28 (84.8) | 5 (15.2) | 2.43 (0.86–6.91) |
| Indication | |||||||||
| Atrial Fibrillation | 327 (96.2) | 13 (3.8) | --- | 323 (95.0) | 17 (5.0) | Ref | 314 (92.4) | 26 (7.6) | Ref |
| Deep Vein Thrombosis (DVT) | 50 (92.6) | 4 (7.4) | --- | 46 (85.2) | 8 (14.8) | 4.75 (1.82–12.4) | 48 (88.9) | 6 (11.1) | 2.20 (0.81–5.95) |
| Pulmonary Embolism (PE) | 45 (91.8) | 4 (8.2) | --- | 45 (91.8) | 4 (8.2) | 1.74 (0.55–5.48) | 42 (85.7) | 7 (14.3) | 2.33 (0.93–5.85) |
| DVT + PE | 6 (100.0) | 0 (0.0) | --- | 6 (100.0) | 0 (0.0) | NA | 6 (100.0) | 0 (0.0) | NA |
| Other | 59 (92.2) | 5 (7.8) | --- | 58 (90.6) | 6 (9.4) | 2.35 (0.86–6.47) | 62 (96.9) | 2 (3.1) | 0.44 (0.10–1.95) |
| Thromboembolic and Bleeding Risk | |||||||||
| CHADS-VASc Score | 4.6 ± 1.4 | 4.9 ± 1.7 | --- | 4.6 ± 1.3 | 5.1 ± 2.1 | --- | 4.6 ± 1.3 | 4.8 ± 1.7 | --- |
| HAS-BLED Score | 2.7 ± 1.0 | 4 ± 0.9 | --- | 2.7 ± 1.0 | 3.3 ± 1.1 | --- | 2.7 ± 1.0 | 3.0 ± 1.2 | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Yami, M.S.; Alfehaid, L.; Alshehri, A.M.; Alqahtani, N.; Almuaither, G.; Alonazi, S.H.; Alzahrani, M.Y.; Badawoud, A.M.; Almohammed, O.A. The Safety of Apixaban Compared to Warfarin in Hospitalized Patients with Acute Kidney Injury. J. Clin. Med. 2025, 14, 4685. https://doi.org/10.3390/jcm14134685
Al Yami MS, Alfehaid L, Alshehri AM, Alqahtani N, Almuaither G, Alonazi SH, Alzahrani MY, Badawoud AM, Almohammed OA. The Safety of Apixaban Compared to Warfarin in Hospitalized Patients with Acute Kidney Injury. Journal of Clinical Medicine. 2025; 14(13):4685. https://doi.org/10.3390/jcm14134685
Chicago/Turabian StyleAl Yami, Majed S., Lama Alfehaid, Abdulmajeed M. Alshehri, Norah Alqahtani, Ghadah Almuaither, Shaden H. Alonazi, Mohammed Y. Alzahrani, Amal M. Badawoud, and Omar A. Almohammed. 2025. "The Safety of Apixaban Compared to Warfarin in Hospitalized Patients with Acute Kidney Injury" Journal of Clinical Medicine 14, no. 13: 4685. https://doi.org/10.3390/jcm14134685
APA StyleAl Yami, M. S., Alfehaid, L., Alshehri, A. M., Alqahtani, N., Almuaither, G., Alonazi, S. H., Alzahrani, M. Y., Badawoud, A. M., & Almohammed, O. A. (2025). The Safety of Apixaban Compared to Warfarin in Hospitalized Patients with Acute Kidney Injury. Journal of Clinical Medicine, 14(13), 4685. https://doi.org/10.3390/jcm14134685