
Evolution of Surgical Approaches for Trigeminal Schwannomas: A Meta-Regression Analysis from Past to Present

 , , ,
, , ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
2.2. Literature Search and Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Statistical Analysis
2.6. Risk of Bias
2.7. Assessment of Reporting Bias and Sensitivity Analysis
3. Results
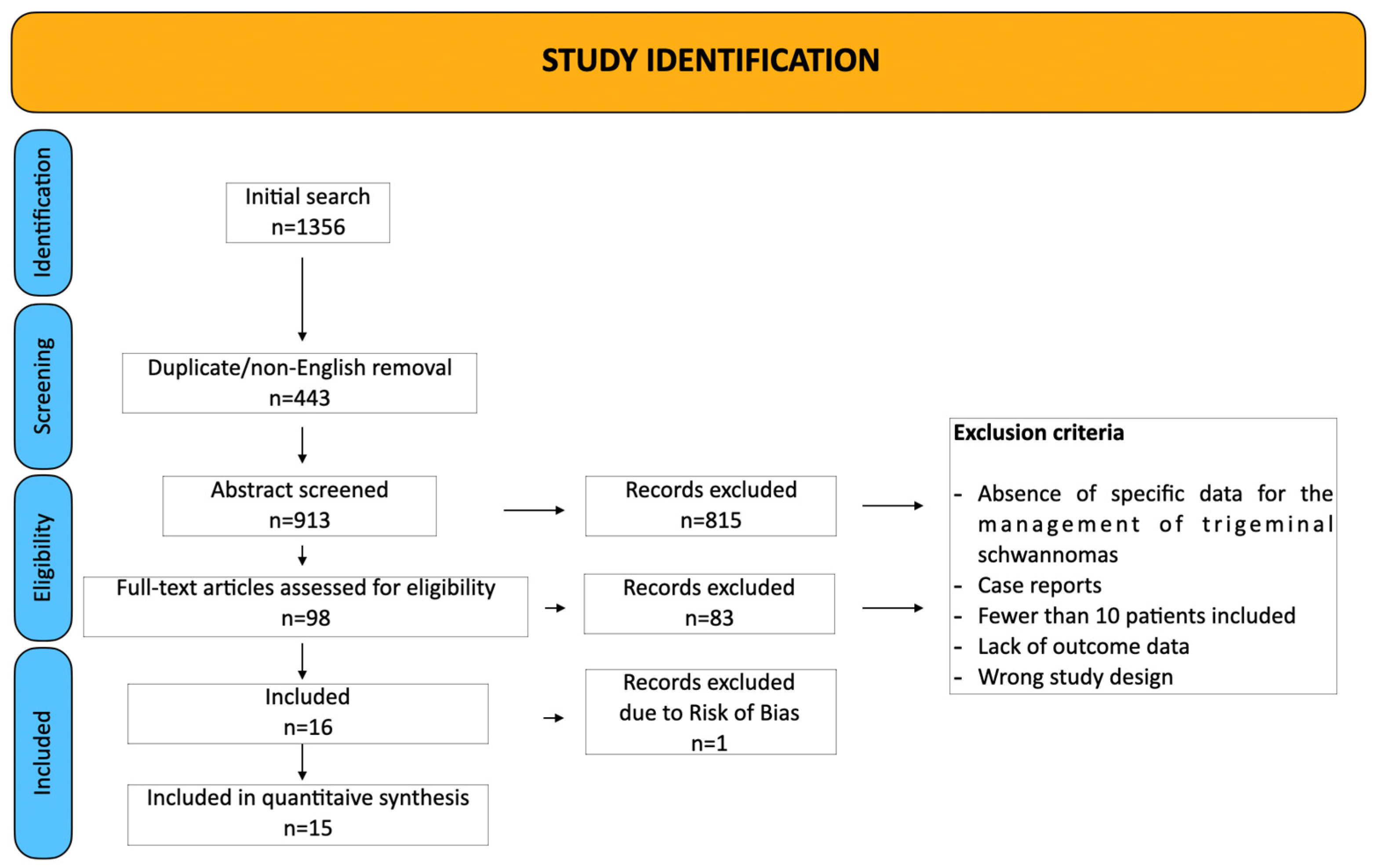
3.1. Study Selection and Characteristics
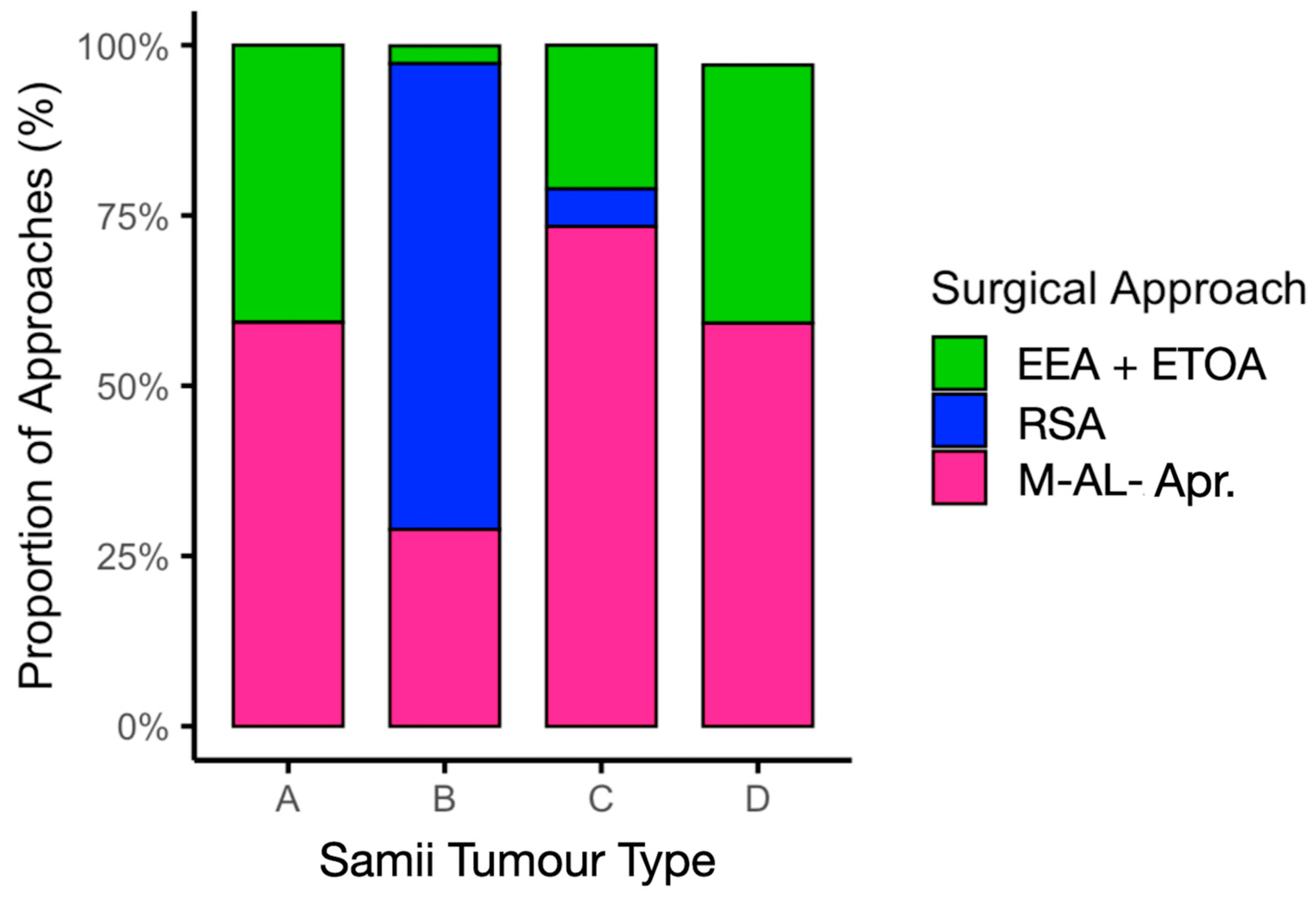
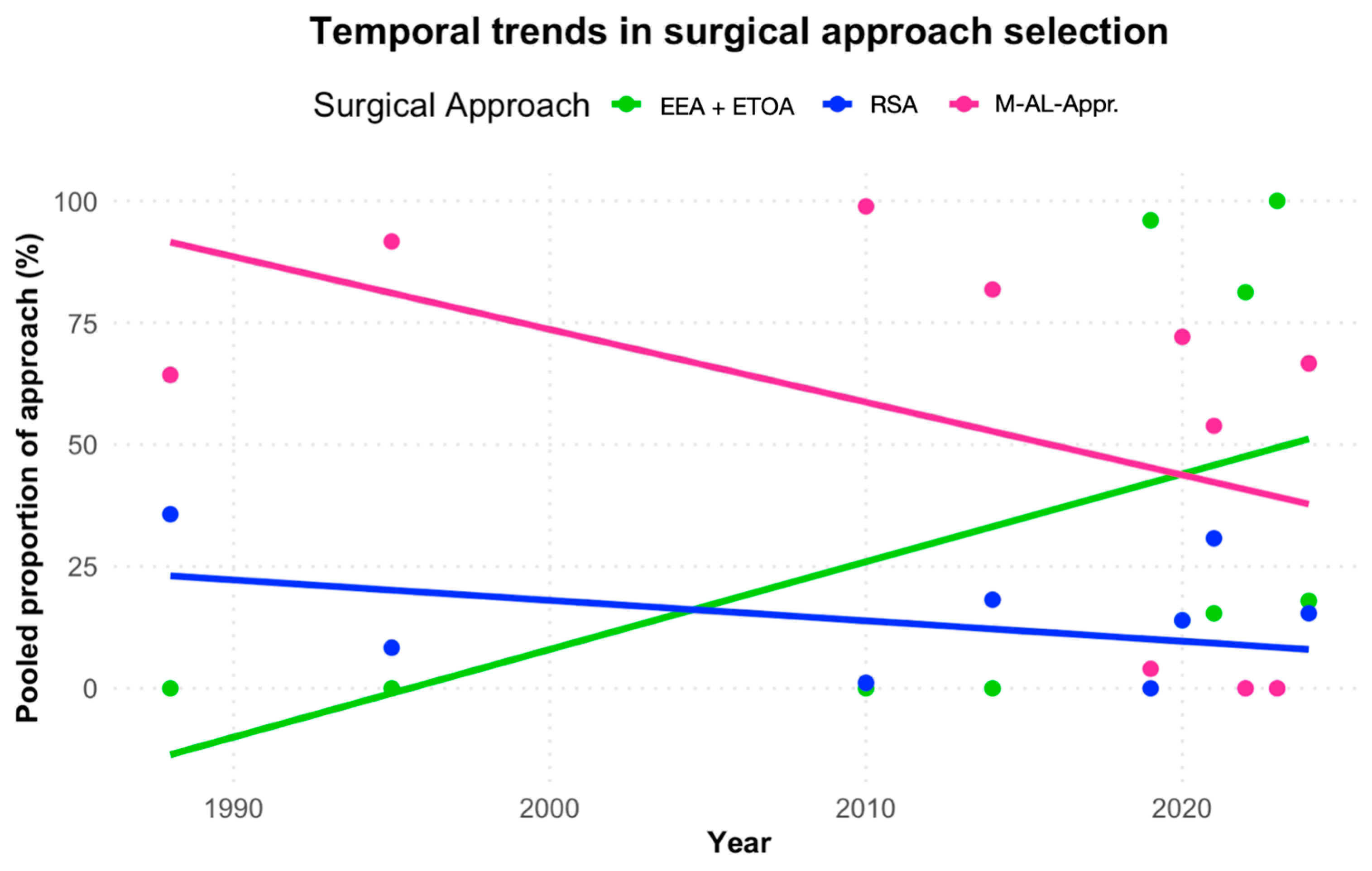
3.2. Choice of Surgical Approaches and Evolution over Time
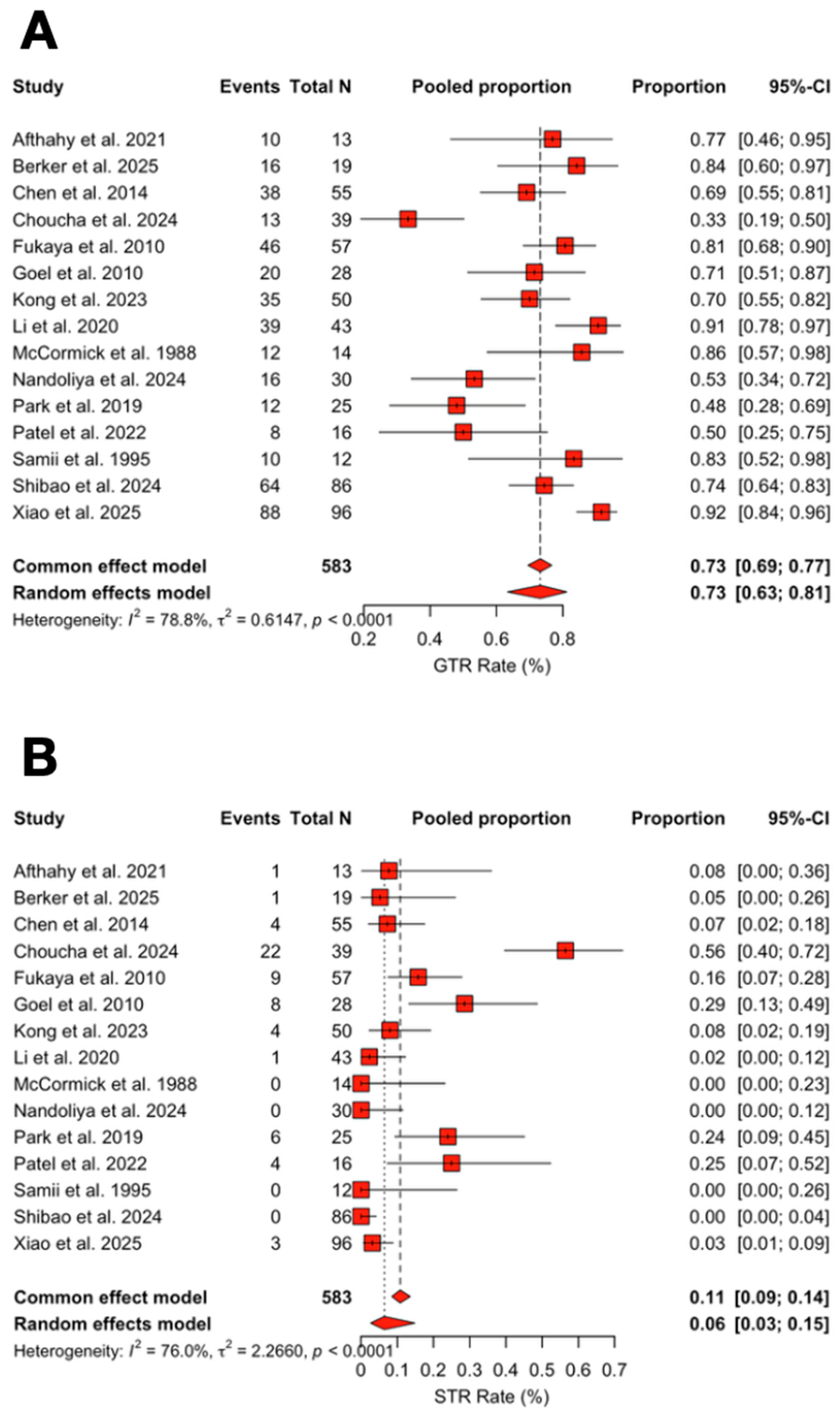
3.3. Extent of Resection Outcomes
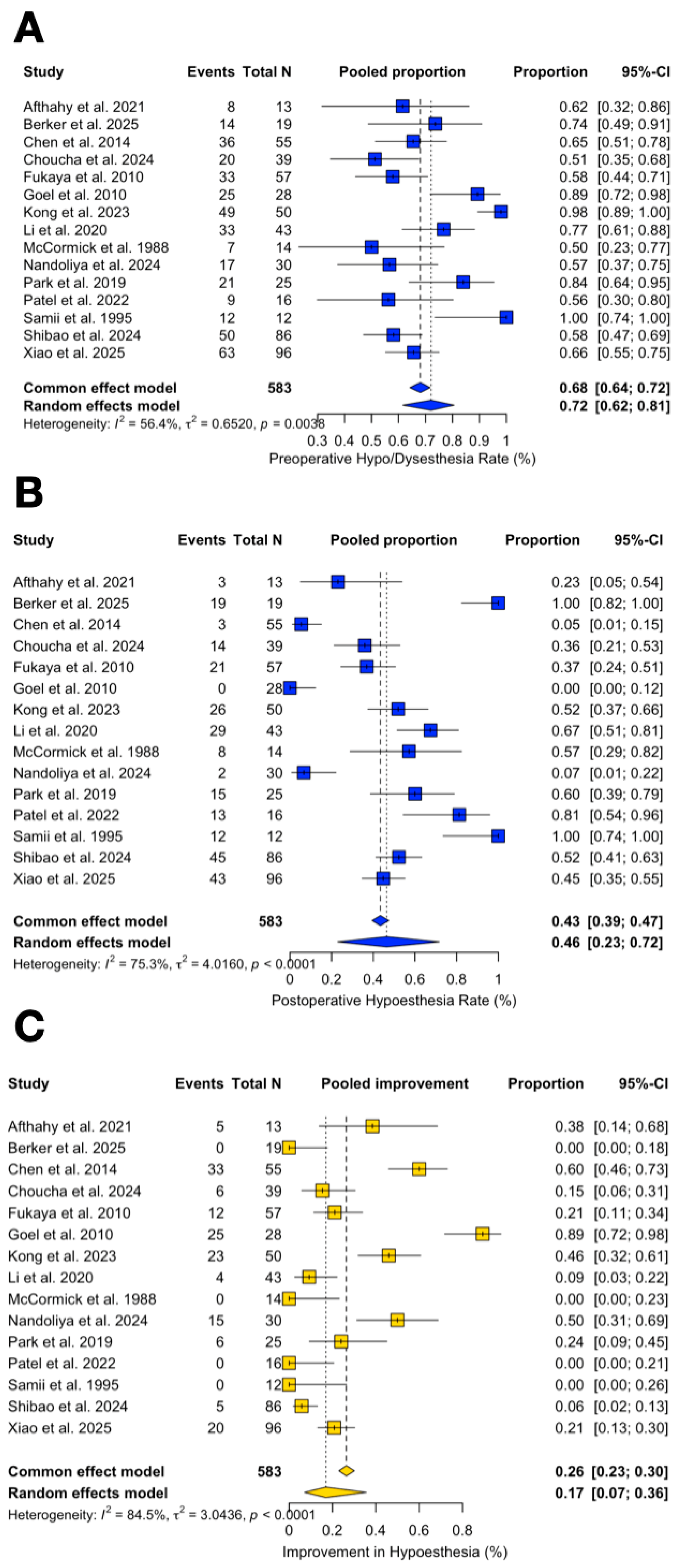
3.4. Functional Outcomes
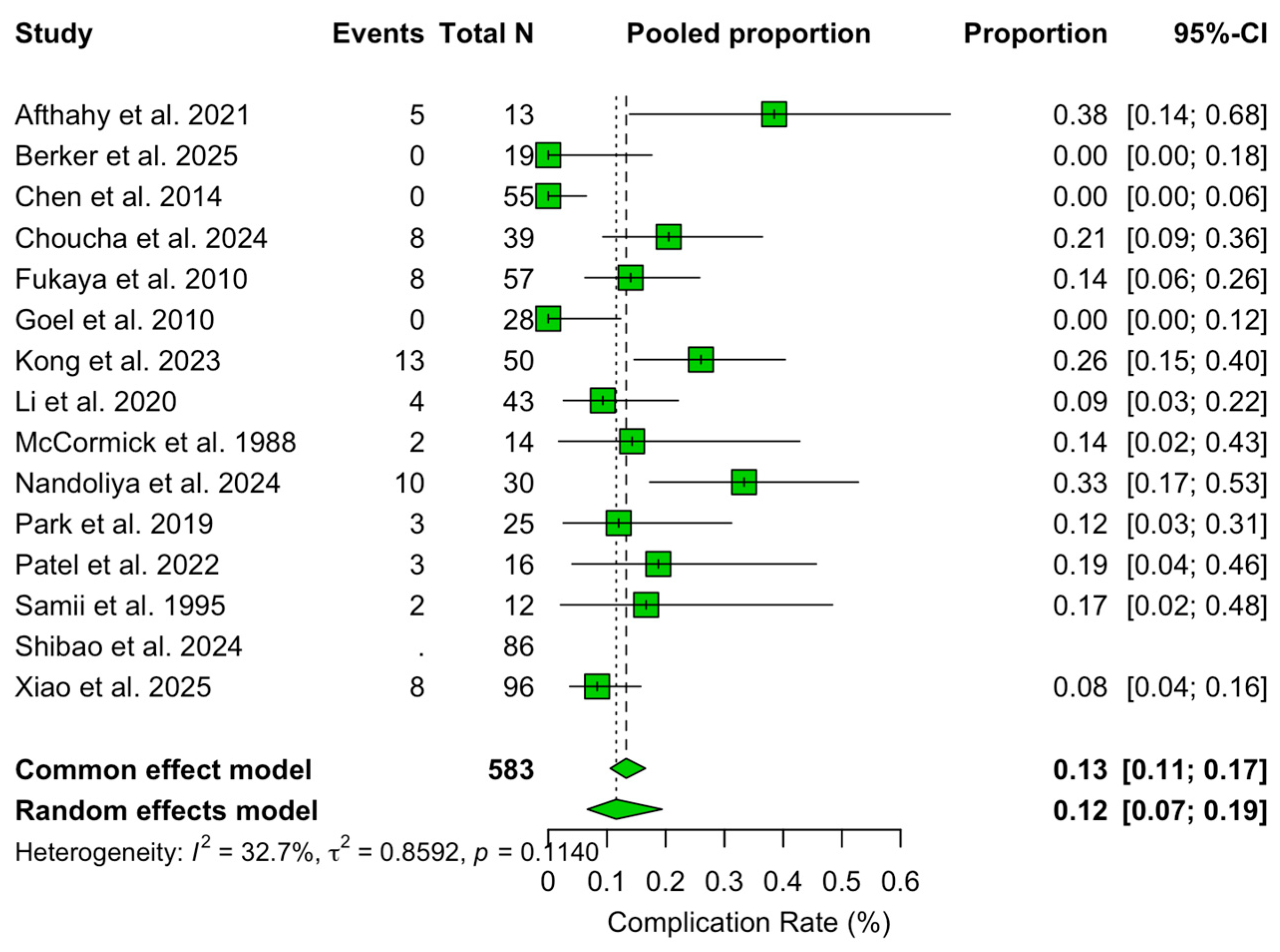
3.5. Complications
3.6. Quality Assessment
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| Comb./2sps | Combined approach or two-step surgical strategy |
| EEA | Endoscopic endonasal approach |
| ETOA | Endoscopic transorbital approach |
| FOZ | Fronto-orbitozygomatic |
| GLM | General linear model |
| GTR | Gross-total resection |
| M-AL-Appr | Microsurgical antero-lateral approaches |
| NTR | Near-total resection |
| RSA | Retrosigmoid approach |
| SRS | Stereotactic radiosurgery |
| STR | Subtotal resection |
| TMA | Trans-maxillary approach |
| TS | Trigeminal schwannoma |
References
- Srinivas, D.; Somanna, S.; Ashwathnarayana, C.B.; Bhagavatula, I.D. Multicompartmental trigeminal schwannomas: Management strategies and outcome. Skull Base 2011, 21, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Zhang, J.; Yu, X.; Qi, S.; Du, Y.; Ni, W.; Hu, Y.; Tian, Z. Stereotactic radiosurgery for trigeminal schwannoma: A clinical retrospective study in 52 cases. Stereotact. Funct. Neurosurg. 2013, 91, 236–242. [Google Scholar] [CrossRef]
- Fukaya, R.; Yoshida, K.; Ohira, T.; Kawase, T. Trigeminal schwannomas: Experience with 57 cases and a review of the literature. Neurosurg. Rev. 2010, 34, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Aftahy, A.K.; Groll, M.; Barz, M.; Wagner, A.; Lange, N.; Butenschön, V.M.; Delbridge, C.; Bernhardt, D.; Meyer, B.; Negwer, C.; et al. Surgical Outcome of Trigeminal Schwannomas. Cancers 2021, 13, 1310. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.V.; Sousa, M.P.; Palavani, L.B.; Andreão, F.F.; Neto, A.R.; Pereira, M.A.O.M.; Fukunaga, C.K.; Paleare, L.F.F.; Montecino, L.M.; Cabral, S.G.; et al. Endonasal endoscopic surgical approach for treating trigeminal schwannomas: A systematic review and meta-analysis. Neurochirurgie 2025, 71, 101676. [Google Scholar] [CrossRef]
- Park, H.H.; Hong, S.D.; Kim, Y.H.; Hong, C.-K.; Woo, K.I.; Yun, I.-S.; Kong, D.-S. Endoscopic transorbital and endonasal approach for trigeminal schwannomas: A retrospective multicenter analysis (KOSEN-005). J. Neurosurg. 2020, 133, 467–476. [Google Scholar] [CrossRef]
- Corrivetti, F.; de Notaris, M.; Seneca, V.; Di Nuzzo, G.; Catapano, G. Is It Time for a Paradigm Shift in the Surgical Management of Trigeminal Schwannomas? Evaluating the Role of the Transorbital Approach: An Anatomo-Clinical Study and Systematic Literature Review. World Neurosurg. 2024, 190, e1025–e1037. [Google Scholar] [CrossRef]
- de Notaris, M.; Kong, D.-S.; Di Somma, A.; Enseñat, J.; Hong, C.-K.; Moe, K.; Schwartz, T.H. Superior eyelid transorbital approaches: A modular classification system. J. Neurosurg. 2024, 141, 278–283. [Google Scholar] [CrossRef]
- Niranjan, A.; Barnett, S.; Anand, V.; Agazzi, S. Multimodality Management of Trigeminal Schwannomas. J. Neurol. Surg. B Skull Base 2016, 77, 371–378. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Samii, M.; Migliori, M.M.; Tatagiba, M.; Babu, R. Surgical treatment of trigeminal schwannomas. J. Neurosurg. 1995, 82, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Berker, B.B.; Güngör, A.; Doğruel, Y.; Rahmanov, S.; Türe, H.; Türe, U. Endoscope Assisted Microsurgical Removal of Trigeminal Schwannomas. World Neurosurg. 2025, 199, 124098. [Google Scholar] [CrossRef]
- Chen, L.-F.; Yang, Y.; Yu, X.-G.; Gui, Q.-P.; Bu, B.; Xu, B.-N.; Zhou, D.-B. Operative management of trigeminal neuromas: An analysis of a surgical experience with 55 cases. Acta Neurochir. 2014, 156, 1105–1114. [Google Scholar] [CrossRef]
- Choucha, A.; Troude, L.; Morin, L.; Fernandes, S.; Baucher, G.; De Simone, M.; Lihi, A.; Mazen, K.; Alseirihi, M.; Passeri, T.; et al. Management of large Trigeminal Schwannoma: Long-term oncologic and functional outcome from a multicentric retrospective cohort. Acta Neurochir. 2024, 166, 440. [Google Scholar] [CrossRef]
- Goel, A.; Shah, A.; Muzumdar, D.; Nadkarni, T.; Chagla, A. Trigeminal neurinomas with extracranial extension: Analysis of 28 surgically treated cases. J. Neurosurg. 2010, 113, 1079–1084. [Google Scholar] [CrossRef]
- Kong, D.-S.; Kim, Y.H.; Lee, W.-J.; Kim, Y.-H.; Hong, C.-K. Indications and outcomes of endoscopic transorbital surgery for trigeminal schwannoma based on tumor classification: A multicenter study with 50 cases. J. Neurosurg. 2023, 138, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, X.; Chen, G.; Liang, J.; Guo, H.; Song, G.; Bao, Y. Trigeminal schwannoma: A single-center experience with 43 cases and review of literature. Br. J. Neurosurg. 2021, 35, 49–56. [Google Scholar] [CrossRef]
- McCormick, P.C.; Bello, J.A.; Post, K.D. Trigeminal schwannoma. Surgical series of 14 cases with review of the literature. J. Neurosurg. 1988, 69, 850–860. [Google Scholar] [CrossRef]
- Nandoliya, K.R.; Vignolles-Jeong, J.; Karras, C.L.; Govind, S.; Finger, G.; Thirunavu, V.; Sonabend, A.M.; Magill, S.T.; Prevedello, D.M.; Chandler, J.P. Clinical characteristics and outcomes after trigeminal schwannoma resection: A multi-institutional experience. Neurosurg. Rev. 2024, 47, 340. [Google Scholar] [CrossRef]
- Shibao, S.; Yoshida, K.; Ueda, R.; Toda, M. Risk factors of postoperative trigeminal neuropathy in surgical treatment of trigeminal schwannomas. Acta Neurochir. 2024, 166, 387. [Google Scholar] [CrossRef]
- Xiao, Q.; Peng, H.; Tang, G.; Yuan, J.; Peng, G.; Zhang, C.; Wang, X.; Huang, W.; Qin, C.; Liu, Q. Individual surgical management of trigeminal schwannomas guided by an extended classification: A consecutive series of 96 clinical cases at a single institution. Neurosurg. Rev. 2025, 48, 289. [Google Scholar] [CrossRef]
- Patel, V.A.; Polster, S.P.; Abou-Al-Shaar, H.; Kalmar, C.L.; Zenonos, G.A.; Wang, E.W.; Gardner, P.A.; Snyderman, C.H. Trigeminal Schwannoma: A Retrospective Analysis of Endoscopic Endonasal Management, Treatment Outcomes, and Neuropathic Sequelae. J. Neurol. Surg. B Skull Base 2023, 84, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Bordi, L.; Compton, J.; Symon, L. Trigeminal neuroma. A report of eleven cases. Surg. Neurol. 1989, 31, 272–276. [Google Scholar] [CrossRef]
- Raza, S.M.; Donaldson, A.M.; Mehta, A.; Tsiouris, A.J.; Anand, V.K.; Schwartz, T.H. Surgical management of trigeminal schwannomas: Defining the role for endoscopic endonasal approaches. Neurosurg. Focus 2014, 37, E17. [Google Scholar] [CrossRef] [PubMed]
- Mariniello, G.; Cappabianca, P.; Buonamassa, S.; de Divitiis, E. Surgical treatment of intracavernous trigeminal schwannomas via a fronto-temporal epidural approach. Clin. Neurol. Neurosurg. 2004, 106, 104–109. [Google Scholar] [CrossRef]
- Di Somma, A.; Andaluz, N.; Cavallo, L.M.; Topczewski, T.E.; Frio, F.; Gerardi, R.M.; Pineda, J.; Solari, D.; Enseñat, J.; Prats-Galino, A.; et al. Endoscopic transorbital route to the petrous apex: A feasibility anatomic study. Acta Neurochir. 2018, 160, 707–720. [Google Scholar] [CrossRef]
- Shin, S.S.; Gardner, P.A.; Stefko, S.T.; Madhok, R.; Fernandez-Miranda, J.C.; Snyderman, C.H. Endoscopic endonasal approach for nonvestibular schwannomas. Neurosurgery 2011, 69, 1046–1057; discussion 1057. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Park, H.H.; Yun, I.S.; Hong, C.K. Clinical applications of the endoscopic transorbital approach for various lesions. Acta Neurochir. 2021, 163, 2269–2277. [Google Scholar] [CrossRef]
- Kassam, A.B.; Prevedello, D.M.; Carrau, R.L.; Snyderman, C.H.; Gardner, P.; Osawa, S.; Seker, A.; Rhoton, A.L. The front door to meckel’s cave: An anteromedial corridor via expanded endoscopic endonasal approach- technical considerations and clinical series. Neurosurgery 2009, 64 (Suppl. S3), ons71–ons82; discussion ons82–ons83. [Google Scholar] [CrossRef]
- Dolenc, V.V.; Rogers, L. Microsurgical Anatomy and Surgery of the Central Skull Base; Springer: Wien, Austria, 2003. [Google Scholar]
- Dolenc, V.; Rogers, L. Cavernous Sinus: Developments and Future Perspectives; Springer: New York, NY, USA, 2009; pp. 1–227. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Features | Approaches | Samii Classification % | Clinical Features % | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Type of Studies | Cases | Surgeries | Mean age | ETOA % | EEA % | M-AL Apr. % | RSA % | Comb./2sps % | TMA % | A | B | C | D | Pre Trig. Imp. | Post Trig. Imp. | CSF Leak | Other Compl. | Recurrence | GTR | NTR | STR |
| Aftahy et al. [4] | 2021 | RS | 13 | 13 | 57.50 | 0 | 15.38 | 46.15 | 23.08 | 15.38 | 0 | 46.15 | 15.38 | 30.77 | 7.69 | 61.54 | 23.08 | 0 | 38.46 | 0 | 76.92 | 23.08 | 7.69 |
| Berker et al. [13] | 2025 | RS | 19 | 19 | 37.5 | 0 | 0 | 68.42 | 31.58 | 0 | 0 | 26.32 | 5.26 | 68.42 | 0 | 73.68 | 100 | 0 | 0 | 0 | 84.21 | 10.53 | 5.26 |
| Chen et al. [14] | 2014 | RS | 55 | 55 | 36 | 0 | 0 | 80 | 18.18 | 1.82 | 0 | 23.64 | 18.18 | 38.18 | 20 | 65.45 | 5.45 | 0 | 0 | 1.82 | 69.09 | 23.64 | 7.27 |
| Choucha et al. [15] | 2024 | RS | 39 | 39 | 42 | 0 | 15.38 | 69.23 | 15.38 | 0 | 0 | 15.38 | 5.13 | 46.15 | 33.33 | 51.28 | 35.90 | 7.69 | 20.51 | 7.69 | 33.33 | 10.26 | 56.41 |
| Fukaya et al. [3] | 2010 | RS | 57 | 57 | 42.8 | 0 | 0 | 100 | 0 | 0 | 0 | 14.04 | 21.05 | 57.89 | 12.28 | 57.89 | 36.84 | 3.51 | 14.04 | 8.77 | 80.70 | 3.51 | 15.79 |
| Goel et al. [16] | 2010 | RS | 28 | 28 | 0 | 0 | 100 | 0 | 0 | 0 | 0.00 | 0 | 0 | 100 | 89.29 | 0 | 0 | 0 | 7.14 | 71.43 | 0 | 28.57 | |
| Kong et al. [17] | 2023 | RS | 50 | 50 | 46.9 | 100 | 0 | 0 | 0 | 0 | 0 | 34.00 | 0 | 40 | 26 | 98 | 52 | 0 | 26 | 0 | 70 | 18 | 8 |
| Li et al. [18] | 2020 | RS | 43 | 43 | 45.3 | 0 | 13.95 | 60.47 | 13.95 | 11.63 | 0 | 18.60 | 13.95 | 44.19 | 23.26 | 76.74 | 67.44 | 0 | 9.30 | 2.33 | 90.70 | 6.98 | 2.33 |
| McCormick et al. [19] | 1988 | RS | 14 | 14 | 40 | 0 | 0 | 50 | 35.71 | 14.29 | 0 | 57.14 | 35.71 | 0 | 7.14 | 50 | 57.14 | 14.29 | 14.29 | 28.57 | 85.71 | 14.29 | 0 |
| Nandoliya et al. [20] | 2024 | RS | 30 | 30 | 43 | 0 | 46.67 | 30 | 3.33 | 20 | 0 | 20.00 | 10 | 50 | 20 | 56.67 | 6.67 | 6.67 | 33.33 | 13.33 | 53.33 | 46.67 | 0 |
| Park et al. [6] | 2019 | RS | 25 | 25 | 48.8 | 44 | 52 | 0 | 0 | 4 | 0 | 36.00 | 0 | 32 | 32 | 84 | 60 | 0 | 12 | 4 | 48 | 28 | 24 |
| Patel et al. [23] | 2022 | RS | 16 | 16 | 44 | 0 | 81.25 | 0 | 0 | 0 | 18.75 | 37.50 | 0 | 0 | 62.50 | 56.25 | 81.25 | 37.50 | 18.75 | 6.25 | 50 | 25 | 25 |
| Samii et al. [11] | 1995 | RS | 12 | 12 | 44 | 0 | 0 | 50 | 8.33 | 41.67 | 0 | 41.67 | 8.33 | 41.67 | 8.33 | 100 | 100 | 16.67 | 16.67 | 16.67 | 83.33 | 16.67 | 0 |
| Shibao et al. [21] | 2024 | RS | 86 | 86 | 45 | 0 | 2.33 | 96.51 | 1.16 | 0 | 0 | 16.28 | 19.77 | 40.70 | 23.26 | 58.14 | 52.33 | 0 | 0 | 2.33 | 74.42 | 25.58 | 0 |
| Xiao et al. [22] | 2025 | RS | 96 | 96 | 46.3 | 0 | 0 | 70.83 | 28.13 | 1.04 | 0 | 15.63 | 8.33 | 55.21 | 20.83 | 65.63 | 44.79 | 1.04 | 8.33 | 1.04 | 91.67 | 5.21 | 3.13 |
| Author | Samii Type | Number of Patients | ETOA | EEA | M-AL Approaches | RSA | Comb./2-steps | TMA |
|---|---|---|---|---|---|---|---|---|
| Aftahy et al., 2021 [4] | A | 6 | 0 | 1 | 5 | 0 | 0 | 0 |
| Chen et al., 2014 [14] | A | 13 | 0 | 0 | 13 | 0 | 0 | 0 |
| Choucha et al., 2024 [15] | A | 6 | 0 | 2 | 4 | 0 | 0 | 0 |
| Fukaya et al., 2010 [3] | A | 8 | 0 | 0 | 8 | 0 | 0 | 0 |
| Goel et al., 2010 [16] | A | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Kong et al., 2023 [17] | A | 17 | 17 | 0 | 0 | 0 | 0 | 0 |
| Li et al., 2020 [18] | A | 8 | 0 | 0 | 8 | 0 | 0 | 0 |
| McCormick et al., 1988 [19] | A | 8 | 0 | 0 | 6 | 0 | 2 | 0 |
| Park et al., 2019 [6] | A | 9 | 5 | 4 | 0 | 0 | 0 | 0 |
| Patel et al., 2022 [23] | A | 6 | 0 | 6 | 0 | 0 | 0 | 0 |
| Samii et al., 1995 [11] | A | 5 | 0 | 0 | 5 | 0 | 0 | 0 |
| Aftahy et al., 2021 [4] | B | 2 | 0 | 0 | 0 | 2 | 0 | 0 |
| Chen et al., 2014 [14] | B | 10 | 0 | 0 | 0 | 10 | 0 | 0 |
| Choucha et al., 2024 [15] | B | 2 | 0 | 1 | 0 | 1 | 0 | 0 |
| Fukaya et al., 2010 [3] | B | 12 | 0 | 0 | 11 | 1 | 0 | 0 |
| Goel et al., 2010 [16] | B | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Kong et al., 2023 [17] | B | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Li et al., 2020 [18] | B | 6 | 0 | 0 | 0 | 6 | 0 | 0 |
| McCormick et al., 1988 [19] | B | 5 | 0 | 0 | 0 | 5 | 0 | 0 |
| Park et al., 2019 [6] | B | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Patel et al., 2022 [23] | B | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Samii et al., 1995 [11] | B | 1 | 0 | 0 | 0 | 1 | 0 | 0 |
| Aftahy et al., 2021 [4] | C | 4 | 0 | 0 | 1 | 2 | 1 | 0 |
| Chen et al., 2014 [14] | C | 21 | 0 | 0 | 20 | 0 | 1 | 0 |
| Choucha et al., 2024 [15] | C | 18 | 0 | 0 | 13 | 5 | 0 | 0 |
| Fukaya et al., 2010 [3] | C | 33 | 0 | 0 | 33 | 0 | 0 | 0 |
| Goel et al., 2010 [16] | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Kong et al., 2023 [17] | C | 20 | 20 | 0 | 0 | 0 | 0 | 0 |
| Li et al., 2020 [18] | C | 19 | 0 | 0 | 17 | 0 | 2 | 0 |
| McCormick et al., 1988 [19] | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Park et al., 2019 [6] | C | 8 | 4 | 3 | 0 | 0 | 1 | 0 |
| Patel et al., 2022 [23] | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Samii et al., 1995 [11] | C | 5 | 0 | 0 | 0 | 0 | 5 | 0 |
| Aftahy et al., 2021 [4] | D | 1 | 0 | 1 | 0 | 0 | 0 | 0 |
| Chen et al., 2014 [14] | D | 11 | 0 | 0 | 11 | 0 | 0 | 0 |
| Choucha et al., 2024 [15] | D | 13 | 0 | 4 | 9 | 0 | 0 | 0 |
| Fukaya et al., 2010 [3] | D | 7 | 0 | 0 | 6 | 0 | 1 | 0 |
| Goel et al., 2010 [16] | D | 28 | 0 | 0 | 28 | 0 | 0 | 0 |
| Kong et al., 2023 [17] | D | 13 | 13 | 0 | 0 | 0 | 0 | 0 |
| Li et al., 2020 [18] | D | 10 | 0 | 6 | 1 | 0 | 3 | 0 |
| McCormick et al., 1988 [19] | D | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Park et al., 2019 [6] | D | 8 | 2 | 6 | 0 | 0 | 0 | 0 |
| Patel et al., 2022 [23] | D | 10 | 0 | 7 | 0 | 0 | 0 | 3 |
| Samii et al., 1995 [11] | D | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| Author | Year | CSF Leak Overall % | CSF Leak in EEA % | CSF Leak in Other Non-Endoscopic Approaches % | Oculomotor Dysfunction % | Facial Palsy % | Retraction Related Complications % | Infections % |
|---|---|---|---|---|---|---|---|---|
| McCormick et al. [19] | 1988 | 14.29 | 100 | 7.14 | 7.14 | |||
| Samii et al. [11] | 1995 | 16.67 | 100 | 16.67 | ||||
| Fukaya et al. [3] | 2010 | 3.51 | 100 | 14.04 | ||||
| Goel et al. [16] | 2010 | |||||||
| Chen et al. [14] | 2014 | |||||||
| Park et al. [6] | 2019 | 4 | 4 | 4 | ||||
| Li et al. [18] | 2020 | 2.33 | 2.33 | 4.65 | ||||
| Aftahy et al. [4] | 2021 | 15.38 | 15.38 | 7.69 | ||||
| Patel et al. [23] | 2022 | 37.50 | 83.33 | 16.67 | 12.50 | 6.25 | ||
| Kong et al. [17] | 2023 | 22 | 4 | |||||
| Choucha et al. [15] | 2024 | 7.69 | 100 | 10.26 | 10.26 | |||
| Nandoliya et al. [20] | 2024 | 6.67 | 100 | 26.67 | 3.33 | 3.33 | ||
| Shibao et al. [21] | 2024 | |||||||
| Berker et al. [13] | 2025 | |||||||
| Xiao et al. [22] | 2025 | 1.04 | 100 | 2.08 | 2.08 | 4.17 |
| Study | Year | 1. Were There Clear Criteria for Inclusion in the Case Series? | 2. Was the Condition Measured in a Standard, Reliable Way for All Participants Included in the Case Series? | 3. Were Valid Methods Used for Identification of the Condition for All Participants Included in the Case Series? | 4. Did the Case Series Have Consecutive Inclusion of Participants? | 5. Did the Case Series Have Complete Inclusion of Participants? | 6. Was There Clear Reporting of the Demographics of the Participants in the Study? | 7. Was There Clear Reporting of Clinical Information of the Participants? | 8. Were the Outcomes or Follow-up Results of Cases Clearly Reported? | 9. Was There Clear Reporting of the Presenting site(s)/Clinic(s) Demographic Information? | 10. Was Statistical Analysis Appropriate? | Include |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aftahy et al. [4] | 2021 | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Berker et al. [13] | 2025 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Bordi et al. | 1989 | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✕ |
| Chen et al. [14] | 2014 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Choucha et al. [15] | 2024 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Fukaya et al. [3] | 2010 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Goel et al. [16] | 2010 | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Kong et al. [17] | 2023 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Li et al. [18] | 2020 | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ |
| McCormick et al. [19] | 1988 | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✕ | ✓ | ✓ |
| Nandoliya et al. [20] | 2024 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Park et al. [6] | 2019 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Patel et al. [23] | 2022 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Samii et al. [11] | 1995 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ |
| Shibao et al. [21] | 2024 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Xiao et al. [22] | 2025 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porto, E.; Fiore, G.; Casali, C.; Stanziano, M.; Broggi, M.; Bertani, G.A.; Marcus, H.J.; Locatelli, M.; DiMeco, F. Evolution of Surgical Approaches for Trigeminal Schwannomas: A Meta-Regression Analysis from Past to Present. J. Clin. Med. 2025, 14, 4488. https://doi.org/10.3390/jcm14134488
Porto E, Fiore G, Casali C, Stanziano M, Broggi M, Bertani GA, Marcus HJ, Locatelli M, DiMeco F. Evolution of Surgical Approaches for Trigeminal Schwannomas: A Meta-Regression Analysis from Past to Present. Journal of Clinical Medicine. 2025; 14(13):4488. https://doi.org/10.3390/jcm14134488
Chicago/Turabian StylePorto, Edoardo, Giorgio Fiore, Cecilia Casali, Mario Stanziano, Morgan Broggi, Giulio A. Bertani, Hani J. Marcus, Marco Locatelli, and Francesco DiMeco. 2025. "Evolution of Surgical Approaches for Trigeminal Schwannomas: A Meta-Regression Analysis from Past to Present" Journal of Clinical Medicine 14, no. 13: 4488. https://doi.org/10.3390/jcm14134488
APA StylePorto, E., Fiore, G., Casali, C., Stanziano, M., Broggi, M., Bertani, G. A., Marcus, H. J., Locatelli, M., & DiMeco, F. (2025). Evolution of Surgical Approaches for Trigeminal Schwannomas: A Meta-Regression Analysis from Past to Present. Journal of Clinical Medicine, 14(13), 4488. https://doi.org/10.3390/jcm14134488