
The Use of Direct Oral Anticoagulants (DOACs) in the Geriatric Population—How to Overcome the Challenges of Geriatric Syndromes

 , , ,
, , ,  ,
, 


Abstract
1. Introduction
2. Risk of Falling
3. Delayed Drug Intake
4. Accidental Overdosage
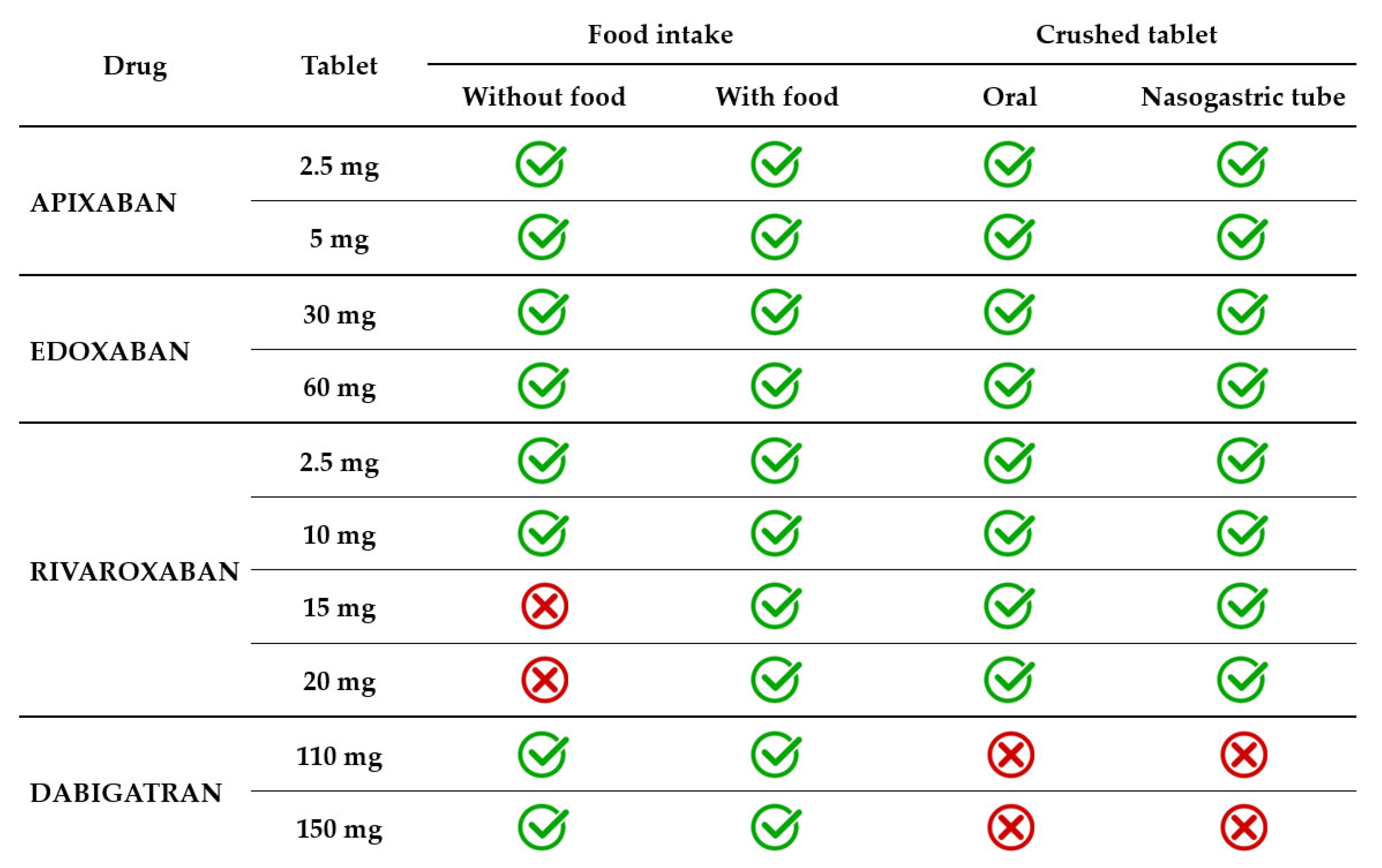
5. Swallowing Disorders
6. Polypragmasy
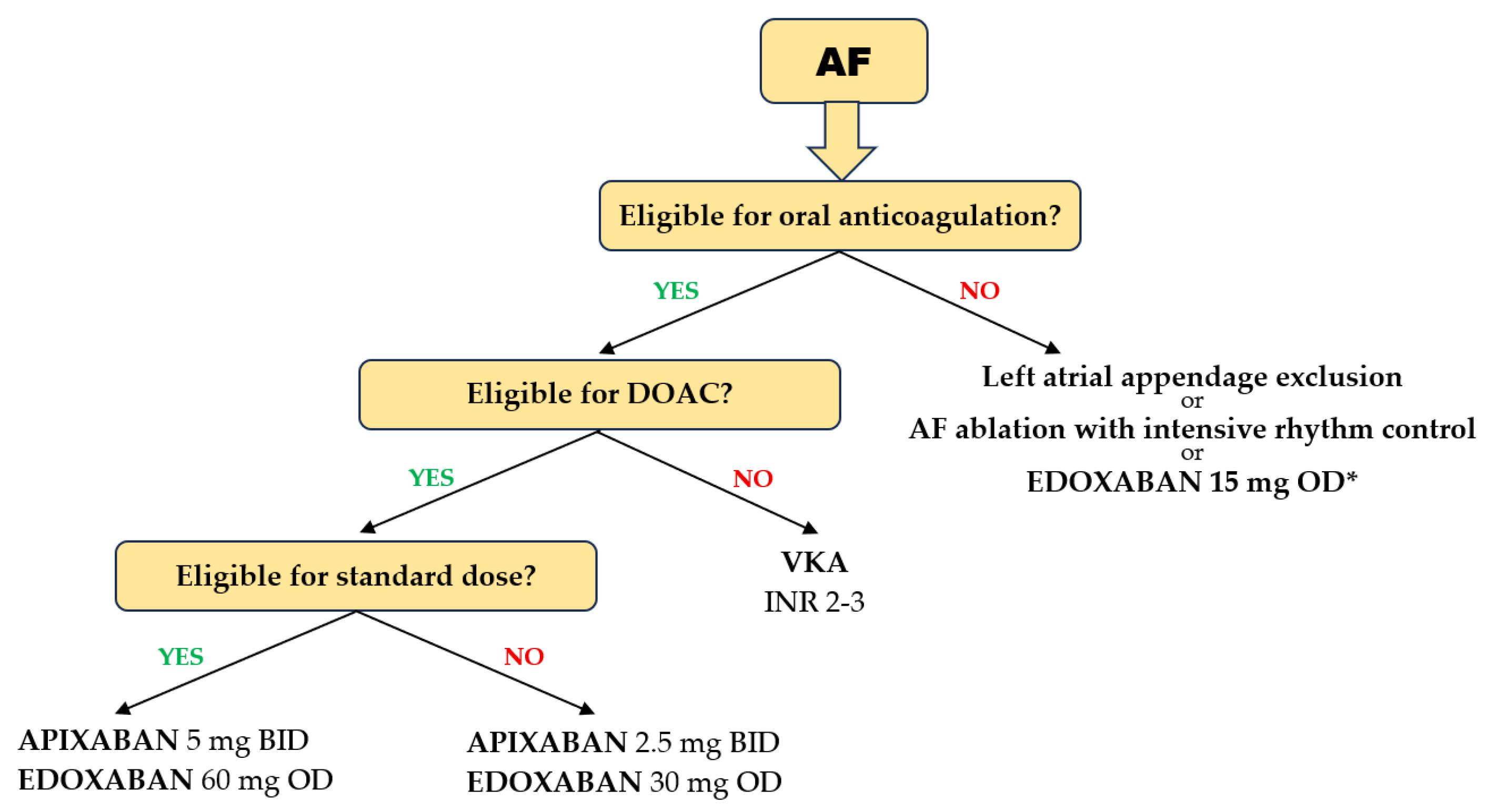
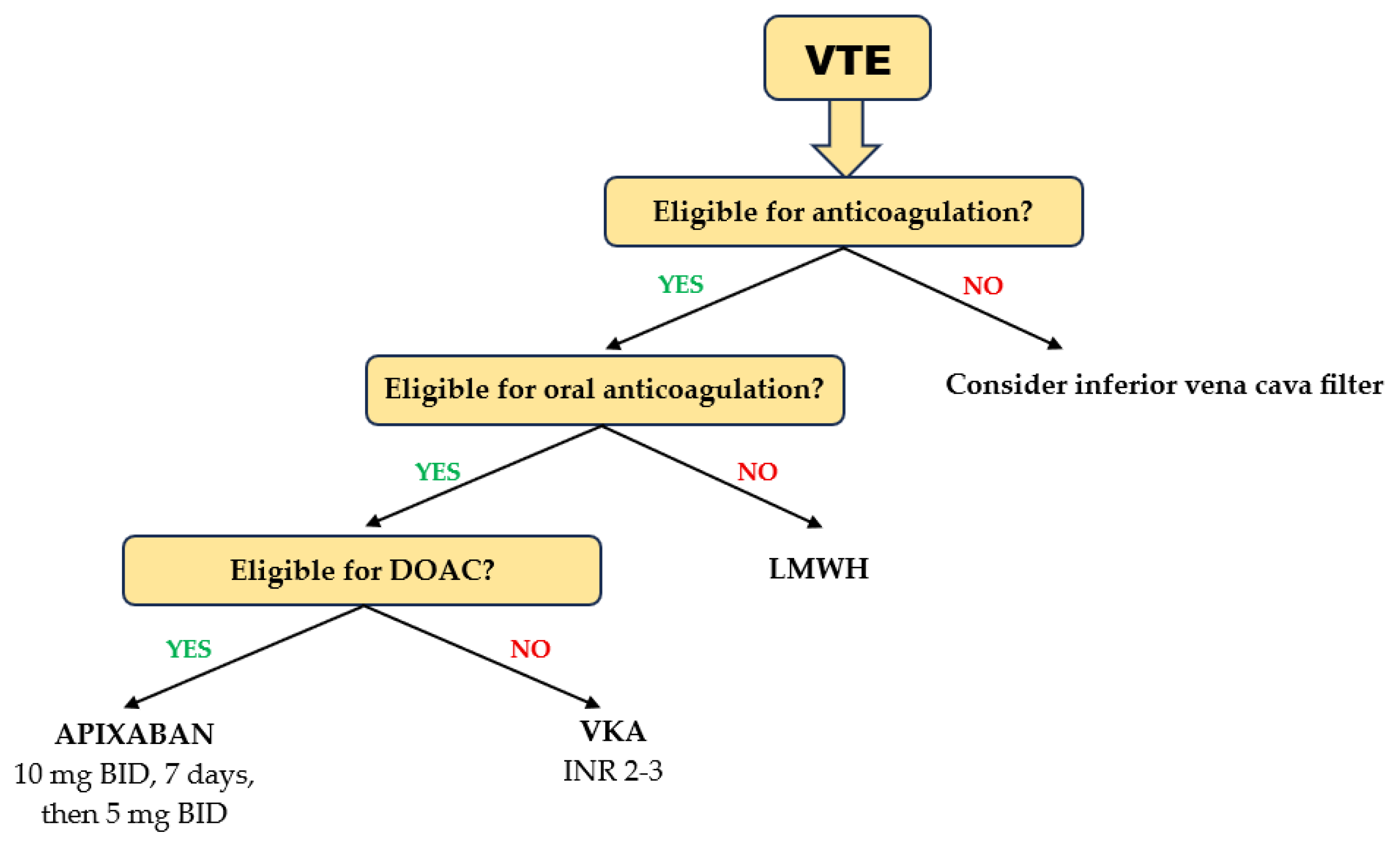
7. The Choice of Anticoagulant
8. The Choice of Anticoagulant Dose
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United States Census Bureau. 2023 National Population Projections Tables: Main Series. Available online: https://www.census.gov/data/tables/2023/demo/popproj/2023-summary-tables.html (accessed on 15 April 2025).
- Eurostat. Population Structure and Ageing. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 15 April 2025).
- Economic and Social Commission for Asia and the Pacific (ESCAP). Demographic Changes in the Asia and the Pacific. Available online: https://www.population-trends-asiapacific.org/population-ageing (accessed on 15 April 2025).
- United Nations. Departament of Economic ans Social Affairs. World Social Report 2023. Available online: https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2023/01/2023wsr-chapter1-.pdf (accessed on 15 April 2025).
- Staerk, L.; Wang, B.; Preis, S.R.; Larson, M.G.; Lubitz, S.A.; Ellinor, P.T.; McManus, D.D.; Ko, D.; Weng, L.C.; Lunetta, K.L.; et al. Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: Cohort study based on longitudinal data from the Framingham Heart Study. BMJ 2018, 361, k1453. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, S.; Ashburner, J.M.; Ellinor, P.T.; McManus, D.D.; Atlas, S.J.; Singer, D.E.; Lubitz, S.A. Prevalence and Incidence of Atrial Fibrillation Among Older Primary Care Patients. JAMA Netw. Open 2023, 6, e2255838. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M.; Tsai, A.W.; White, R.H.; Heckbert, S.R.; Rosamond, W.D.; Enright, P.; Folsom, A.R. Deep vein thrombosis and pulmonary embolism in two cohorts: The longitudinal investigation of thromboembolism etiology. Am. J. Med. 2004, 117, 19–25. [Google Scholar] [CrossRef]
- Spencer, F.A.; Emery, C.; Joffe, S.W.; Pacifico, L.; Lessard, D.; Reed, G.; Gore, J.M.; Goldberg, R.J. Incidence rates, clinical profile, and outcomes of patients with venous thromboembolism. The Worcester VTE study. J. Thromb. Thrombolysis 2009, 28, 401–409. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Falls in Older People: Assessing Risk and Prevention. Available online: https://www.nice.org.uk/guidance/cg161 (accessed on 15 April 2025).
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef]
- Mitchell, A.; Snowball, J.; Welsh, T.J.; Watson, M.C.; McGrogan, A. Prescribing of direct oral anticoagulants and warfarin to older people with atrial fibrillation in UK general practice: A cohort study. BMC Med. 2021, 19, 189. [Google Scholar] [CrossRef]
- Ganetsky, M.; Lopez, G.; Coreanu, T.; Novack, V.; Horng, S.; Shapiro, N.I.; Bauer, K.A. Risk of Intracranial Hemorrhage in Ground-level Fall with Antiplatelet or Anticoagulant Agents. Acad. Emerg. Med. 2017, 24, 1258–1266. [Google Scholar] [CrossRef]
- Nederpelt, C.J.; Naar, L.; Meier, K.; van Wijck, S.F.M.; Krijnen, P.; Velmahos, G.C.; Kaafarani, H.M.A.; Rosenthal, M.G.; Schipper, I.B. Treatment and outcomes of anticoagulated geriatric trauma patients with traumatic intracranial hemorrhage after falls. Eur. J. Trauma Emerg. Surg. 2022, 48, 4297–4304. [Google Scholar] [CrossRef]
- Savioli, G.; Ceresa, I.F.; Luzzi, S.; Gragnaniello, C.; Giotta Lucifero, A.; Del Maestro, M.; Marasco, S.; Manzoni, F.; Ciceri, L.; Gelfi, E.; et al. Rates of Intracranial Hemorrhage in Mild Head Trauma Patients Presenting to Emergency Department and Their Management: A Comparison of Direct Oral Anticoagulant Drugs with Vitamin K Antagonists. Medicina 2020, 56, 308. [Google Scholar] [CrossRef]
- Kwon, H.; Kim, Y.J.; Lee, J.H.; Kim, S.; Kim, Y.J.; Kim, W.Y. Incidence and outcomes of delayed intracranial hemorrhage: A population-based cohort study. Sci. Rep. 2024, 14, 19502. [Google Scholar] [CrossRef]
- Cipriano, A.; Park, N.; Pecori, A.; Bionda, A.; Bardini, M.; Frassi, F.; Lami, V.; Leoli, F.; Manca, M.L.; Del Prato, S.; et al. Predictors of post-traumatic complication of mild brain injury in anticoagulated patients: DOACs are safer than VKAs. Intern. Emerg. Med. 2021, 16, 1061–1070. [Google Scholar] [CrossRef]
- Karamian, A.; Seifi, A.; Karamian, A.; Lucke-Wold, B. Incidence of intracranial bleeding in mild traumatic brain injury patients taking oral anticoagulants: A systematic review and meta-analysis. J. Neurol. 2024, 271, 3849–3868. [Google Scholar] [CrossRef]
- Wu, T.; Lv, C.; Wu, L.; Chen, W.; Lv, M.; Jiang, S.; Zhang, J. Risk of intracranial hemorrhage with direct oral anticoagulants: A systematic review and meta-analysis of randomized controlled trials. J. Neurol. 2022, 269, 664–675. [Google Scholar] [CrossRef]
- Silverio, A.; Di Maio, M.; Prota, C.; De Angelis, E.; Radano, I.; Citro, R.; Carrizzo, A.; Ciccarelli, M.; Vecchione, C.; Capodanno, D.; et al. Safety and efficacy of non-vitamin K antagonist oral anticoagulants in elderly patients with atrial fibrillation: Systematic review and meta-analysis of 22 studies and 440 281 patients. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, f20–f29. [Google Scholar] [CrossRef]
- Gao, X.; Huang, D.; Hu, Y.; Chen, Y.; Zhang, H.; Liu, F.; Luo, J. Direct Oral Anticoagulants vs. Vitamin K Antagonists in Atrial Fibrillation Patients at Risk of Falling: A Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 833329. [Google Scholar] [CrossRef]
- Man-Son-Hing, M.; Nichol, G.; Lau, A.; Laupacis, A. Choosing antithrombotic therapy for elderly patients with atrial fibrillation who are at risk for falls. Arch. Intern. Med. 1999, 159, 677–685. [Google Scholar] [CrossRef]
- Wei, W.; Rasu, R.S.; Hernandez-Munoz, J.J.; Flores, R.J.; Rianon, N.J.; Hernandez-Vizcarrondo, G.A.; Brown, A.T. Impact of Fall Risk and Direct Oral Anticoagulant Treatment on Quality-Adjusted Life-Years in Older Adults with Atrial Fibrillation: A Markov Decision Analysis. Drugs Aging 2021, 38, 713–723. [Google Scholar] [CrossRef]
- Mitchell, A.; Elmasry, Y.; van Poelgeest, E.; Welsh, T.J. Anticoagulant use in older persons at risk for falls: Therapeutic dilemmas-a clinical review. Eur. Geriatr. Med. 2023, 14, 683–696. [Google Scholar] [CrossRef]
- Bristol-Myers Squibb-Pfizer. Eliquis 5 mg Film-Coated Tablets. Available online: https://www.medicines.org.uk/emc/product/2878/smpc (accessed on 1 May 2025).
- Daiichi Sankyo UK Limited. Lixiana 60 mg Film-Coated Tablets. Available online: https://www.medicines.org.uk/emc/product/6905/smpc (accessed on 1 May 2025).
- Bayer PLC. Xarelto 20 mg Film-Coated Tablets. Available online: https://www.medicines.org.uk/emc/product/2793/smpc (accessed on 1 May 2025).
- Mabley, J.; Scutt, G.; Lang, K.J.; Patel, J.P.; Arya, R. Rrivaroxaban-mediated vascular relaxation as a potential cause of headaches and dizziness. Blood 2015, 126, 2334. [Google Scholar] [CrossRef]
- Chung, C.C.; Lin, Y.K.; Chen, Y.C.; Kao, Y.H.; Yeh, Y.H.; Chen, Y.J. Factor Xa inhibition by rivaroxaban regulates fibrogenesis in human atrial fibroblasts with modulation of nitric oxide synthesis and calcium homeostasis. J. Mol. Cell. Cardiol. 2018, 123, 128–138. [Google Scholar] [CrossRef]
- Villari, A.; Giurdanella, G.; Bucolo, C.; Drago, F.; Salomone, S. Apixaban Enhances Vasodilatation Mediated by Protease-Activated Receptor 2 in Isolated Rat Arteries. Front. Pharmacol. 2017, 8, 480. [Google Scholar] [CrossRef]
- Mabley, J.; Patel, J.P.; Sayed, A.; Arya, R.; Scutt, G. Direct oral anticoagulant (DOAC)-mediated vasodilation: Role of nitric oxide. Thromb. Res. 2019, 176, 36–38. [Google Scholar] [CrossRef]
- Hindley, B.; Lip, G.Y.H.; McCloskey, A.P.; Penson, P.E. Pharmacokinetics and pharmacodynamics of direct oral anticoagulants. Expert Opin. Drug Metab. Toxicol. 2023, 19, 911–923. [Google Scholar] [CrossRef]
- Ieko, M.; Naitoh, S.; Yoshida, M.; Takahashi, N. Profiles of direct oral anticoagulants and clinical usage-dosage and dose regimen differences. J. Intensive Care 2016, 4, 19. [Google Scholar] [CrossRef]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- SAVAYSA [Package Insert]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/206316s017lbl.pdf (accessed on 20 April 2025).
- Lixiana [Product Information]. Available online: https://www.ema.europa.eu/en/documents/product-information/lixiana-epar-product-information_en.pdf (accessed on 20 April 2025).
- Yin, Y.W.; Liu, X.Q.; Gu, J.Q.; Li, Z.R.; Jiao, Z. How to handle a delayed or missed dose of edoxaban in patients with non-valvular atrial fibrillation? A model-informed remedial strategy. Br. J. Clin. Pharmacol. 2023, 89, 2066–2075. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef]
- Xarelto [Package Insert]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/215859s000lbl.pdf (accessed on 20 April 2025).
- Xarelto [Package Insert]. Available online: https://www.ema.europa.eu/en/documents/product-information/xarelto-epar-product-information_en.pdf (accessed on 20 April 2025).
- Liu, X.Q.; Yin, Y.W.; Wang, C.Y.; Li, Z.R.; Zhu, X.; Jiao, Z. How to handle the delayed or missed dose of rivaroxaban in patients with non-valvular atrial fibrillation: Model-informed remedial dosing. Expert Rev. Clin. Pharmacol. 2021, 14, 1153–1163. [Google Scholar] [CrossRef]
- Pradaxa [Package Insert]. Available online: https://www.ema.europa.eu/en/documents/product-information/pradaxa-epar-product-information_en.pdf (accessed on 20 April 2025).
- Pradaxa [Package Insert]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022512s047lbl.pdf (accessed on 20 April 2025).
- Frost, C.; Shenker, A.; Jhee, S.; Yu, Z.; Wang, J.; Bragat, A.; Pursley, J.; LaCreta, F. Evaluation of the single-dose pharmacokinetics and pharmacodynamics of apixaban in healthy Japanese and Caucasian subjects. Clin. Pharmacol. 2018, 10, 153–163. [Google Scholar] [CrossRef]
- Leikin, S.M.; Patel, H.; Welker, K.L.; Leikin, J.B. The X factor: Lack of bleeding after an acute apixaban overdose. Am. J. Emerg. Med. 2017, 35, 801.e5–801.e6. [Google Scholar] [CrossRef]
- Barton, J.; Wong, A.; Graudins, A. Anti-Xa activity in apixaban overdose: A case report. Clin. Toxicol. 2016, 54, 871–873. [Google Scholar] [CrossRef]
- Mast, L.; Verheul, R.J.; Reijnen, R.; van Rossen, R.; Overdiek, J.; Wilms, E.B. Apixaban Auto-intoxication: Toxicokinetics and Coagulation Tests. Thromb. Haemost. 2017, 117, 2209–2211. [Google Scholar] [CrossRef]
- Franck, B.; Dulaurent, S.; El Balkhi, S.; Monchaud, C.; Picard, N.; Couderc, S.; Marquet, P.; Saint-Marcoux, F.; Woillard, J.B. Self-poisoning with 60 tablets of Apixaban, a pharmacokinetics case report. Br. J. Clin. Pharmacol. 2019, 85, 270–272. [Google Scholar] [CrossRef]
- Guadarrama, D.S.; DeMarinis, S.M.; Sweeney, J.D. Coagulation assays in a case of apixaban overdose. Blood Coagul. Fibrinolysis 2018, 29, 231–235. [Google Scholar] [CrossRef]
- Kobayashi, T.; Saito, S.; Takada, M.; Sakaguchi, K.; Takahashi, K.; Tanaka, K.; Kawamae, K.; Nakane, M. Massive Intoxication with 70 Tablets of Apixaban: A Case Report. Case Rep. Acute Med. 2023, 6, 13–18. [Google Scholar] [CrossRef]
- Ogata, K.; Mendell-Harary, J.; Tachibana, M.; Masumoto, H.; Oguma, T.; Kojima, M.; Kunitada, S. Clinical safety, tolerability, pharmacokinetics, and pharmacodynamics of the novel factor Xa inhibitor edoxaban in healthy volunteers. J. Clin. Pharmacol. 2010, 50, 743–753. [Google Scholar] [CrossRef]
- Adachi, K.; Tuchiya, J.; Beppu, S.; Nishiyama, K.; Shimizu, M.; Yamazaki, H. Pharmacokinetics of anticoagulant edoxaban in overdose in a Japanese patient transported to hospital. J. Pharm. Health Care Sci. 2020, 6, 20. [Google Scholar] [CrossRef]
- Kubitza, D.; Becka, M.; Voith, B.; Zuehlsdorf, M.; Wensing, G. Safety, pharmacodynamics, and pharmacokinetics of single doses of BAY 59-7939, an oral, direct factor Xa inhibitor. Clin. Pharmacol. Ther. 2005, 78, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Kubitza, D.; Becka, M.; Roth, A.; Mueck, W. Dose-escalation study of the pharmacokinetics and pharmacodynamics of rivaroxaban in healthy elderly subjects. Curr. Med. Res. Opin. 2008, 24, 2757–2765. [Google Scholar] [CrossRef] [PubMed]
- Ghodsi, A.; Etemad, L.; Dadpour, B.; Mostafazadeh, B.; Moshiri, M. Conservative management of massive rivaroxaban overdose: A case report and literature review. Clin. Case Rep. 2021, 9, e05023. [Google Scholar] [CrossRef]
- Lehmann, T.; Hofer, K.E.; Baumann, M.; Hasler, K.; Ceschi, A.; Kupferschmidt, H.; Rohde, G.; Korte, W. Massive human rivaroxaban overdose. Thromb. Haemost. 2014, 112, 834–836. [Google Scholar] [CrossRef]
- Repplinger, D.J.; Hoffman, R.S.; Nelson, L.S.; Hines, E.Q.; Howland, M.; Su, M.K. Lack of significant bleeding despite large acute rivaroxaban overdose confirmed with whole blood concentrations. Clin. Toxicol. 2016, 54, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Casey, B., III; Daniels, A.; Bahekar, A.; Patel, D.; Chapa-Rodriguez, A. Management of Massive Rivaroxaban Overdose with Acetaminophen and Isosorbide Mononitrate Overdose. Cureus 2023, 15, e34019. [Google Scholar] [CrossRef]
- Stangier, J.; Rathgen, K.; Stahle, H.; Gansser, D.; Roth, W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br. J. Clin. Pharmacol. 2007, 64, 292–303. [Google Scholar] [CrossRef]
- Vlad, I.; Armstrong, J.; Ridgley, J.; Pascu, O. Dabigatran deliberate overdose: Two cases and suggestions for laboratory monitoring. Clin. Toxicol. 2016, 54, 286–289. [Google Scholar] [CrossRef]
- Peetermans, M.; Pollack, C., Jr.; Reilly, P.; Liesenborghs, L.; Jacquemin, M.; Levy, J.H.; Weitz, J.I.; Verhamme, P. Idarucizumab for dabigatran overdose. Clin. Toxicol. 2016, 54, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, J.W.; Minns, A.B.; Smollin, C.; Albertson, T.E.; Cantrell, F.L.; Tomaszewski, C.; Clark, R.F. An observational case series of dabigatran and rivaroxaban exposures reported to a poison control system. Am. J. Emerg. Med. 2014, 32, 1077–1084. [Google Scholar] [CrossRef]
- Conway, S.E.; Schaeffer, S.E.; Harrison, D.L. Evaluation of dabigatran exposures reported to poison control centers. Ann. Pharmacother. 2014, 48, 354–360. [Google Scholar] [CrossRef]
- Spiller, H.A.; Mowry, J.B.; Aleguas, A., Jr.; Griffith, J.R.; Goetz, R.; Ryan, M.L.; Bangh, S.; Klein-Schwartz, W.; Schaeffer, S.; Casavant, M.J. An Observational Study of the Factor Xa Inhibitors Rivaroxaban and Apixaban as Reported to Eight Poison Centers. Ann. Emerg. Med. 2016, 67, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; Beuhler, M.C.; Pizon, A.; Cantrel, F.L.; Spyres, M.B.; LoVecchio, F.; Skolnik, A.B.; Brooks, D.E. Assessing Bleeding Risk in Patients with Intentional Overdoses of Novel Antiplatelet and Anticoagulant Medications. Ann. Emerg. Med. 2018, 71, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Thiyagalingam, S.; Kulinski, A.E.; Thorsteinsdottir, B.; Shindelar, K.L.; Takahashi, P.Y. Dysphagia in Older Adults. Mayo Clin. Proc. 2021, 96, 488–497. [Google Scholar] [CrossRef]
- Bayer PLC. Xarelto 15 mg & 20 mg Film-Coated Tablets Treatment Initiation Pack. Available online: https://www.medicines.org.uk/emc/product/8419/smpc#gref (accessed on 25 April 2025).
- Boehringer Ingelheim Ltd. Pradaxa 150 mg Hard Capsules. Available online: https://www.medicines.org.uk/emc/product/4703/smpc (accessed on 25 April 2025).
- Song, Y.; Chang, M.; Suzuki, A.; Frost, R.J.A.; Kelly, A.; LaCreta, F.; Frost, C. Evaluation of crushed tablet for oral administration and the effect of food on apixaban pharmacokinetics in healthy adults. Clin. Ther. 2016, 38, 1674–1685.e1. [Google Scholar] [CrossRef]
- Song, Y.; Wang, X.; Perlstein, I.; Wang, J.; Badawy, S.; Frost, C.; LaCreta, F. Relative Bioavailability of Apixaban Solution or Crushed Tablet Formulations Administered by Mouth or Nasogastric Tube in Healthy Subjects. Clin. Ther. 2015, 37, 1703–1712. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Li, X.; Liu, Y.; Xu, B.; Li, Y.; Yuan, F.; Zhang, P.; Tu, S.; Hu, W. Bioequivalence and Pharmacokinetic Study of 2 Edoxaban Tablets in Healthy Chinese Subjects. Clin. Pharmacol. Drug Dev. 2022, 11, 1440–1446. [Google Scholar] [CrossRef]
- Mendell, J.; Tachibana, M.; Shi, M.; Kunitada, S. Effects of food on the pharmacokinetics of edoxaban, an oral direct factor Xa inhibitor, in healthy volunteers. J. Clin. Pharmacol. 2011, 51, 687–694. [Google Scholar] [CrossRef]
- Duchin, K.; Duggal, A.; Atiee, G.J.; Kidokoro, M.; Takatani, T.; Shipitofsky, N.L.; He, L.; Zhang, G.; Kakkar, T. An Open-Label Crossover Study of the Pharmacokinetics of the 60-mg Edoxaban Tablet Crushed and Administered Either by a Nasogastric Tube or in Apple Puree in Healthy Adults. Clin. Pharmacokinet. 2018, 57, 221–228. [Google Scholar] [CrossRef]
- Cappannoli, L.; Laborante, R.; Galli, M.; Canonico, F.; Ciliberti, G.; Restivo, A.; Princi, G.; Arcudi, A.; Sabatelli, M.; De Cristofaro, R.; et al. Feasibility, effectiveness, and safety of edoxaban administration through percutaneous endoscopic gastrostomy: 12-months follow up of the ORIGAMI study. Front. Cardiovasc. Med. 2022, 9, 1052053. [Google Scholar] [CrossRef]
- Mueck, W.; Stampfuss, J.; Kubitza, D.; Becka, M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin. Pharmacokinet. 2014, 53, 1–16. [Google Scholar] [CrossRef]
- Stampfuss, J.; Kubitza, D.; Becka, M.; Mueck, W. The effect of food on the absorption and pharmacokinetics of rivaroxaban. Int. J. Clin. Pharmacol. Ther. 2013, 51, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.T.; Krook, M.A.; Vaidyanathan, S.; Sarich, T.C.; Damaraju, C.V.; Fields, L.E. Rivaroxaban crushed tablet suspension characteristics and relative bioavailability in healthy adults when administered orally or via nasogastric tube. Clin. Pharmacol. Drug Dev. 2014, 3, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Stangier, J.; Eriksson, B.I.; Dahl, O.E.; Ahnfelt, L.; Nehmiz, G.; Stahle, H.; Rathgen, K.; Svard, R. Pharmacokinetic profile of the oral direct thrombin inhibitor dabigatran etexilate in healthy volunteers and patients undergoing total hip replacement. J. Clin. Pharmacol. 2005, 45, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Heidbuchel, H. The Significance of Drug-Drug and Drug-Food Interactions of Oral Anticoagulation. Arrhythmia Electrophysiol. Rev. 2018, 7, 55–61. [Google Scholar] [CrossRef]
- Wiggins, B.S.; Dixon, D.L.; Neyens, R.R.; Page, R.L., 2nd; Gluckman, T.J. Select Drug-Drug Interactions with Direct Oral Anticoagulants: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 1341–1350. [Google Scholar] [CrossRef]
- Ferri, N.; Colombo, E.; Tenconi, M.; Baldessin, L.; Corsini, A. Drug-Drug Interactions of Direct Oral Anticoagulants (DOACs): From Pharmacological to Clinical Practice. Pharmaceutics 2022, 14, 1120. [Google Scholar] [CrossRef]
- Weng, J.; Lan, R. Does Concomitant Use of Antidepressants and Direct Oral Anticoagulants Increase the Risk of Bleeding?: A Systematic Review and Meta-Analysis. J. Clin. Psychopharmacol. 2025, 45, 140–147. [Google Scholar] [CrossRef]
- Nam, Y.H.; Brensinger, C.M.; Bilker, W.B.; Leonard, C.E.; Han, X.; Hennessy, S. Serious Hypoglycemia and Use of Warfarin in Combination with Sulfonylureas or Metformin. Clin. Pharmacol. Ther. 2019, 105, 210–218. [Google Scholar] [CrossRef]
- Manna, P.; Kalita, J. Beneficial role of vitamin K supplementation on insulin sensitivity, glucose metabolism, and the reduced risk of type 2 diabetes: A review. Nutrition 2016, 32, 732–739. [Google Scholar] [CrossRef]
- Huang, H.K.; Liu, P.P.; Lin, S.M.; Yeh, J.I.; Hsu, J.Y.; Peng, C.C.; Munir, K.M.; Loh, C.H.; Tu, Y.K. Risk of serious hypoglycaemia in patients with atrial fibrillation and diabetes concurrently taking antidiabetic drugs and oral anticoagulants: A nationwide cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 427–434. [Google Scholar] [CrossRef]
- Oh, S.H.; Cheon, S.; Choi, S.Y.; Kim, Y.S.; Choi, H.G.; Chung, J.E. Effectiveness and Safety of Dose-Specific DOACs in Patients with Atrial Fibrillation: A Systematic Review and Network Meta-Analysis. Cardiovasc. Ther. 2025, 2025, 9923772. [Google Scholar] [CrossRef]
- van der Hulle, T.; Kooiman, J.; den Exter, P.L.; Dekkers, O.M.; Klok, F.A.; Huisman, M.V. Effectiveness and safety of novel oral anticoagulants as compared with vitamin K antagonists in the treatment of acute symptomatic venous thromboembolism: A systematic review and meta-analysis. J. Thromb. Haemost. 2014, 12, 320–328. [Google Scholar] [CrossRef]
- Caldeira, D.; Nunes-Ferreira, A.; Rodrigues, R.; Vicente, E.; Pinto, F.J.; Ferreira, J.J. Non-vitamin K antagonist oral anticoagulants in elderly patients with atrial fibrillation: A systematic review with meta-analysis and trial sequential analysis. Arch. Gerontol. Geriatr. 2019, 81, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Pradhan, A.; Vishwakarma, P.; Di Renzo, L.; Iellamo, F.; Ali, W.; Perrone, M.A. Direct Oral Anticoagulant Use in Older Adults with Atrial Fibrillation: Challenges and Solutions. Eur. Cardiol. 2025, 20, e03. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Keshishian, A.V.; Kang, A.L.; Dhamane, A.D.; Luo, X.; Li, X.; Balachander, N.; Rosenblatt, L.; Mardekian, J.; Pan, X.; et al. Oral anticoagulants for nonvalvular atrial fibrillation in frail elderly patients: Insights from the ARISTOPHANES study. J. Intern. Med. 2021, 289, 42–52. [Google Scholar] [CrossRef]
- Carnicelli, A.P.; Hong, H.; Connolly, S.J.; Eikelboom, J.; Giugliano, R.P.; Morrow, D.A.; Patel, M.R.; Wallentin, L.; Alexander, J.H.; Cecilia Bahit, M.; et al. Direct Oral Anticoagulants Versus Warfarin in Patients with Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials with Interaction Testing by Age and Sex. Circulation 2022, 145, 242–255. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.Q.; Chen, X.H.; Tian, X.Y.; Li, L. Differences in Gastrointestinal Safety Profiles Among Novel Oral Anticoagulants: Evidence From A Network Meta-Analysis. Clin. Epidemiol. 2019, 11, 911–921. [Google Scholar] [CrossRef]
- van Es, N.; Coppens, M.; Schulman, S.; Middeldorp, S.; Buller, H.R. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: Evidence from phase 3 trials. Blood 2014, 124, 1968–1975. [Google Scholar] [CrossRef]
- Sadlon, A.H.; Tsakiris, D.A. Direct oral anticoagulants in the elderly: Systematic review and meta-analysis of evidence, current and future directions. Swiss Med. Wkly. 2016, 146, w14356. [Google Scholar] [CrossRef]
- Pessoa, R.L.; Kessler, V.G.; Becker, G.G.; Garcia, G.M.; Duarte Araldi, P.V.; Aver, P.V. Efficacy and Safety of Direct Oral Anticoagulants for Acute Treatment of Venous Thromboembolism in Older Adults: A Network Meta-Analysis of Randomised Controlled Trials. Vasc. Endovasc. Surg. 2024, 58, 633–639. [Google Scholar] [CrossRef]
- Iwai, C.; Jo, T.; Konishi, T.; Kumazawa, R.; Matsui, H.; Fushimi, K.; Yasunaga, H. Comparative Safety and Effectiveness of Direct Oral Anticoagulants and Warfarin during Chemotherapy in Cancer Patients with Venous Thromboembolism Aged 75 Years or Older: A Nationwide Inpatient Database Study. Gerontology 2023, 69, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus warfarin in patients with mechanical heart valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.Y.; Svensson, L.G.; Wen, J.; Vekstein, A.; Gerdisch, M.; Rao, V.U.; Moront, M.; Johnston, D.; Lopes, R.D.; Chavez, A.; et al. Apixaban or Warfarin in Patients with an On-X Mechanical Aortic Valve. NEJM Evid. 2023, 2, EVIDoa2300067. [Google Scholar] [CrossRef] [PubMed]
- Khairani, C.D.; Bejjani, A.; Piazza, G.; Jimenez, D.; Monreal, M.; Chatterjee, S.; Pengo, V.; Woller, S.C.; Cortes-Hernandez, J.; Connors, J.M.; et al. Direct Oral Anticoagulants vs Vitamin K Antagonists in Patients with Antiphospholipid Syndromes: Meta-Analysis of Randomized Trials. J. Am. Coll. Cardiol. 2023, 81, 16–30. [Google Scholar] [CrossRef]
- Portela, C.P.; Gautier, L.A.; Zermatten, M.G.; Fraga, M.; Moradpour, D.; Calderara, D.B.; Aliotta, A.; Veuthey, L.; De Gottardi, A.; Stirnimann, G.; et al. Direct oral anticoagulants in cirrhosis: Rationale and current evidence. JHEP Rep. 2024, 6, 101116. [Google Scholar] [CrossRef]
- Krittayaphong, R.; Chantrarat, T.; Rojjarekampai, R.; Jittham, P.; Sairat, P.; Lip, G.Y.H. Poor Time in Therapeutic Range Control is Associated with Adverse Clinical Outcomes in Patients with Non-Valvular Atrial Fibrillation: A Report from the Nationwide COOL-AF Registry. J. Clin. Med. 2020, 9, 1698. [Google Scholar] [CrossRef]
- Kosum, P.; Siranart, N.; Nissaipan, K.; Laohapiboolrattana, W.; Sowalertrat, W.; Triamamornwooth, K.; Arunphan, R.; Sriyom, A.; Rungpradubvong, V. Utility of TTR-INR guided warfarin adjustment protocol to improve time in therapeutic range in patients with atrial fibrillation receiving warfarin. Sci. Rep. 2024, 14, 11647. [Google Scholar] [CrossRef]
- Fovel, L.M.; Miller, C.D.; Seabury, R.W.; Probst, L.A.; Horvath, L. Evaluation of Warfarin Patients with Low Time in Therapeutic Range (TTR) for Transition to Non-Vitamin-K Oral Anticoagulant (NOAC) Therapy. Pharm. Ther. 2019, 44, 534. [Google Scholar]
- Pundi, K.N.; Perino, A.C.; Fan, J.; Schmitt, S.; Kothari, M.; Szummer, K.; Askari, M.; Heidenreich, P.A.; Turakhia, M.P. Direct Oral Anticoagulant Adherence of Patients with Atrial Fibrillation Transitioned from Warfarin. J. Am. Heart Assoc. 2021, 10, e020904. [Google Scholar] [CrossRef]
- Joosten, L.P.T.; van Doorn, S.; van de Ven, P.M.; Kohlen, B.T.G.; Nierman, M.C.; Koek, H.L.; Hemels, M.E.W.; Huisman, M.V.; Kruip, M.; Faber, L.M.; et al. Safety of Switching From a Vitamin K Antagonist to a Non-Vitamin K Antagonist Oral Anticoagulant in Frail Older Patients with Atrial Fibrillation: Results of the FRAIL-AF Randomized Controlled Trial. Circulation 2024, 149, 279–289. [Google Scholar] [CrossRef]
- Zhdanava, M.; Ashton, V.; Korsiak, J.; Jiang, F.; Pilon, D.; Alberts, M. Out-of-pocket costs for direct oral anticoagulants and prescription abandonment among patients with nonvalvular atrial fibrillation or venous thromboembolism. J. Manag. Care Spec. Pharm. 2025, 31, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Noviyani, R.; Youngkong, S.; Nathisuwan, S.; Bagepally, B.S.; Chaikledkaew, U.; Chaiyakunapruk, N.; McKay, G.; Sritara, P.; Attia, J.; Thakkinstian, A. Economic evaluation of direct oral anticoagulants (DOACs) versus vitamin K antagonists (VKAs) for stroke prevention in patients with atrial fibrillation: A systematic review and meta-analysis. BMJ Evid. Based Med. 2022, 27, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P. Non-vitamin K antagonist oral anticoagulants in older and frail patients with atrial fibrillation. Eur. Heart J. Suppl. 2022, 24, A1–A10. [Google Scholar] [CrossRef] [PubMed]
- Shroff, G. NOAC Dosing in Atrial Fibrillation and Renal Dysfunction: What Measure Are You Using? JACC 2017, 70, 2733–2734. [Google Scholar] [CrossRef]
- Fatima, H.; Nwankwo, I.; Anam, M.; Maharjan, S.; Amjad, Z.; Abaza, A.; Vasavada, A.M.; Sadhu, A.; Valencia, C.; Khan, S. Safety and Efficacy of Apixaban vs Warfarin in Patients with Stage 4 and 5 Chronic Kidney Disease: A Systematic Review. Cureus 2022, 14, e30230. [Google Scholar] [CrossRef]
- Yao, X.; Tangri, N.; Gersh, B.J.; Sangaralingham, L.R.; Shah, N.D.; Nath, K.A.; Noseworthy, P.A. Renal Outcomes in Anticoagulated Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2017, 70, 2621–2632. [Google Scholar] [CrossRef]
- Bendayan, M.; Mardigyan, V.; Williamson, D.; Chen-Tournoux, A.; Eintracht, S.; Rudski, L.; MacNamara, E.; Blostein, M.; Afilalo, M.; Afilalo, J. Muscle Mass and Direct Oral Anticoagulant Activity in Older Adults with Atrial Fibrillation. J. Am. Geriatr. Soc. 2021, 69, 1012–1018. [Google Scholar] [CrossRef]
- Okumura, K.; Akao, M.; Yoshida, T.; Kawata, M.; Okazaki, O.; Akashi, S.; Eshima, K.; Tanizawa, K.; Fukuzawa, M.; Hayashi, T.; et al. Low-Dose Edoxaban in Very Elderly Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1735–1745. [Google Scholar] [CrossRef]
- Chan, Y.H.; Chao, T.F.; Chen, S.W.; Lee, H.F.; Li, P.R.; Yeh, Y.H.; Kuo, C.T.; See, L.C.; Lip, G.Y.H. Clinical outcomes in elderly atrial fibrillation patients at increased bleeding risk treated with very low dose vs. regular-dose non-vitamin K antagonist oral anticoagulants: A nationwide cohort study. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 681–691. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Side Effect | Frequency | Reference |
|---|---|---|---|
| Apixaban | Dizziness | Common | [26] |
| Syncope | Uncommon | ||
| Hypotension | Common | ||
| Decreased general strength and energy (incl. fatigue and asthenia) | Common | ||
| Edoxaban | Dizziness | Common | [27] |
| Rivaroxaban | Dizziness | Common | [28] |
| Syncope | Uncommon | ||
| Hypotension | Common | ||
| Decreased general strength and energy (incl. fatigue and asthenia) | Common |
| Drug | Solvent for Crushed Tablets | Reference |
|---|---|---|
| Apixaban | Orally: water, glucose 5%, apple juice or apple puree NGT: 60 mL water or glucose 5% | [26] |
| Edoxaban | Orally: water or apple puree NGT: water | [27] |
| Rivaroxaban | Orally: water or applesauce NGT: water or applesauce | [68] |
| Dabigatran | Crushing is not allowed. | [69] |
| Drug | DOAC |
|---|---|
| Amiodarone | A, E |
| Dronedarone | A |
| Diltiazem | A, E, D |
| Verapamil | A, E |
| Carbamazepine | A, E |
| Phenytoin | A, E |
| Phenobarbital | A, E, D |
| Valproic acid | Contraindicated |
| Standard Dose | Reduced Dose | Criteria for Dose Reduction | ||
|---|---|---|---|---|
| Factor Xa inhibitors | ||||
| APIXABAN | AF | 5 mg bid | 2.5 mg bid | If ≥2 of the following:
|
| VTE | 10 mg bid, 7 days, then 5 mg bid | - | - | |
| EDOXABAN | AF | 60 mg od | 30 mg od | If any of the following:
|
| VTE | LMWH ≥ 5 days, then 60 mg od | LMWH ≥ 5 days, then 30 mg od | If any of the following:
| |
| RIVAROXABAN | AF | 20 mg | 15 mg | CrCl 15–49 mL/min |
| VTE | 15 mg bid, 21 days, then 20 mg od | - | - | |
| Factor IIa inhibitor | ||||
| DABIGATRAN | AF | 150 mg bid | 110 mg bid | Recommended, if any of the following:
|
| VTE | LMWH ≥ 5 days, then 150 mg bid | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badescu, M.C.; Popescu, D.; Gosav, E.M.; Costache, A.D.; Cosău, D.E.; Chetran, A.; Duca, Ș.-T.; Cucută, S.; Șerban, I.L.; Costache Enache, I.I.; et al. The Use of Direct Oral Anticoagulants (DOACs) in the Geriatric Population—How to Overcome the Challenges of Geriatric Syndromes. J. Clin. Med. 2025, 14, 4396. https://doi.org/10.3390/jcm14134396
Badescu MC, Popescu D, Gosav EM, Costache AD, Cosău DE, Chetran A, Duca Ș-T, Cucută S, Șerban IL, Costache Enache II, et al. The Use of Direct Oral Anticoagulants (DOACs) in the Geriatric Population—How to Overcome the Challenges of Geriatric Syndromes. Journal of Clinical Medicine. 2025; 14(13):4396. https://doi.org/10.3390/jcm14134396
Chicago/Turabian StyleBadescu, Minerva Codruta, Diana Popescu, Evelina Maria Gosav, Alexandru Dan Costache, Diana Elena Cosău, Adriana Chetran, Ștefania-Teodora Duca, Sandu Cucută, Ionela Lăcrămioara Șerban, Irina Iuliana Costache Enache, and et al. 2025. "The Use of Direct Oral Anticoagulants (DOACs) in the Geriatric Population—How to Overcome the Challenges of Geriatric Syndromes" Journal of Clinical Medicine 14, no. 13: 4396. https://doi.org/10.3390/jcm14134396
APA StyleBadescu, M. C., Popescu, D., Gosav, E. M., Costache, A. D., Cosău, D. E., Chetran, A., Duca, Ș.-T., Cucută, S., Șerban, I. L., Costache Enache, I. I., & Rezus, C. (2025). The Use of Direct Oral Anticoagulants (DOACs) in the Geriatric Population—How to Overcome the Challenges of Geriatric Syndromes. Journal of Clinical Medicine, 14(13), 4396. https://doi.org/10.3390/jcm14134396