
Efficacy and Safety of Fosfomycin Disodium in Patients with Bacterial Infections: A Single-Center, Real-Life Clinical Study

 , , , , , ,
, , , , , , 

Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Patients Included
2.2. Variables Analyzed
2.3. Clinical and Microbiological Outcomes
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients Studied
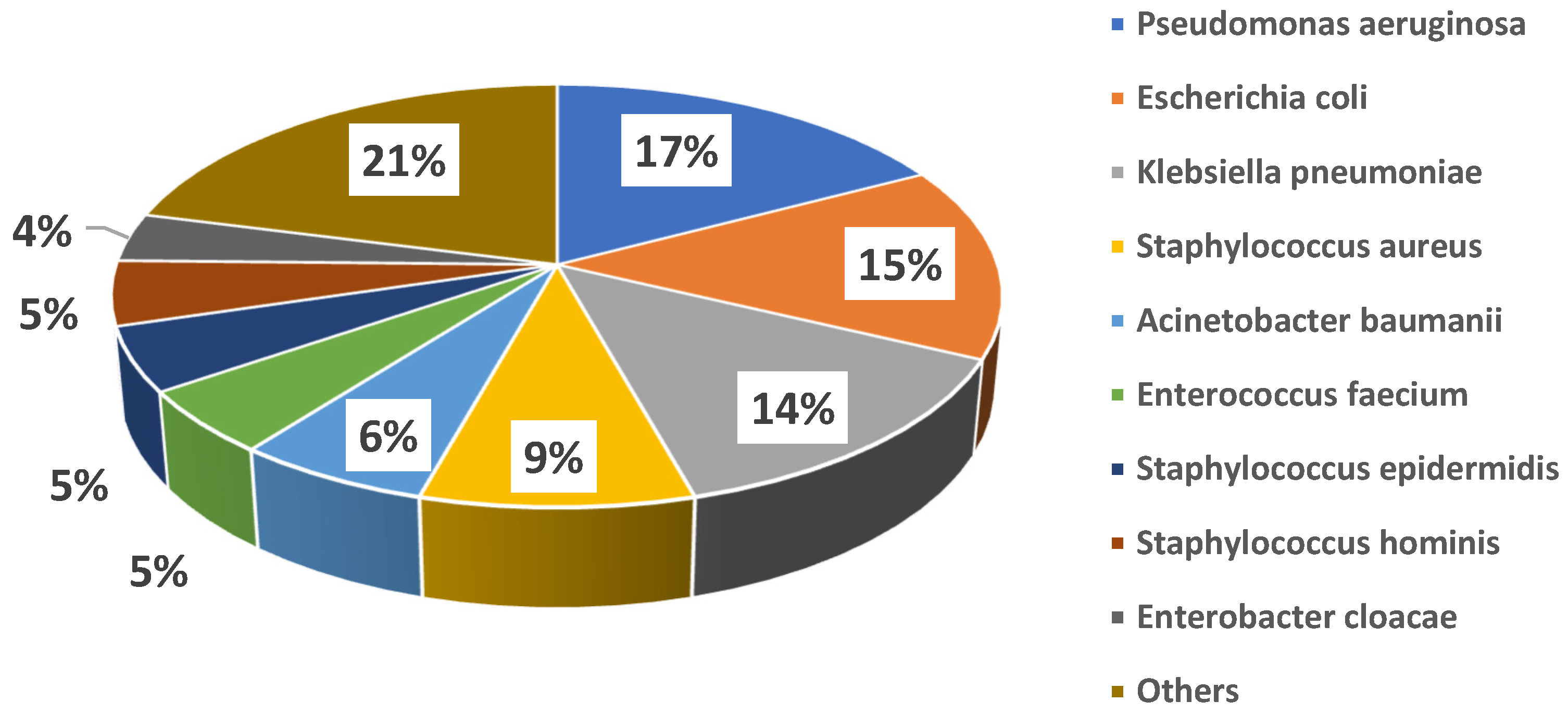
3.2. Clinical Syndromes and Microbial Etiology
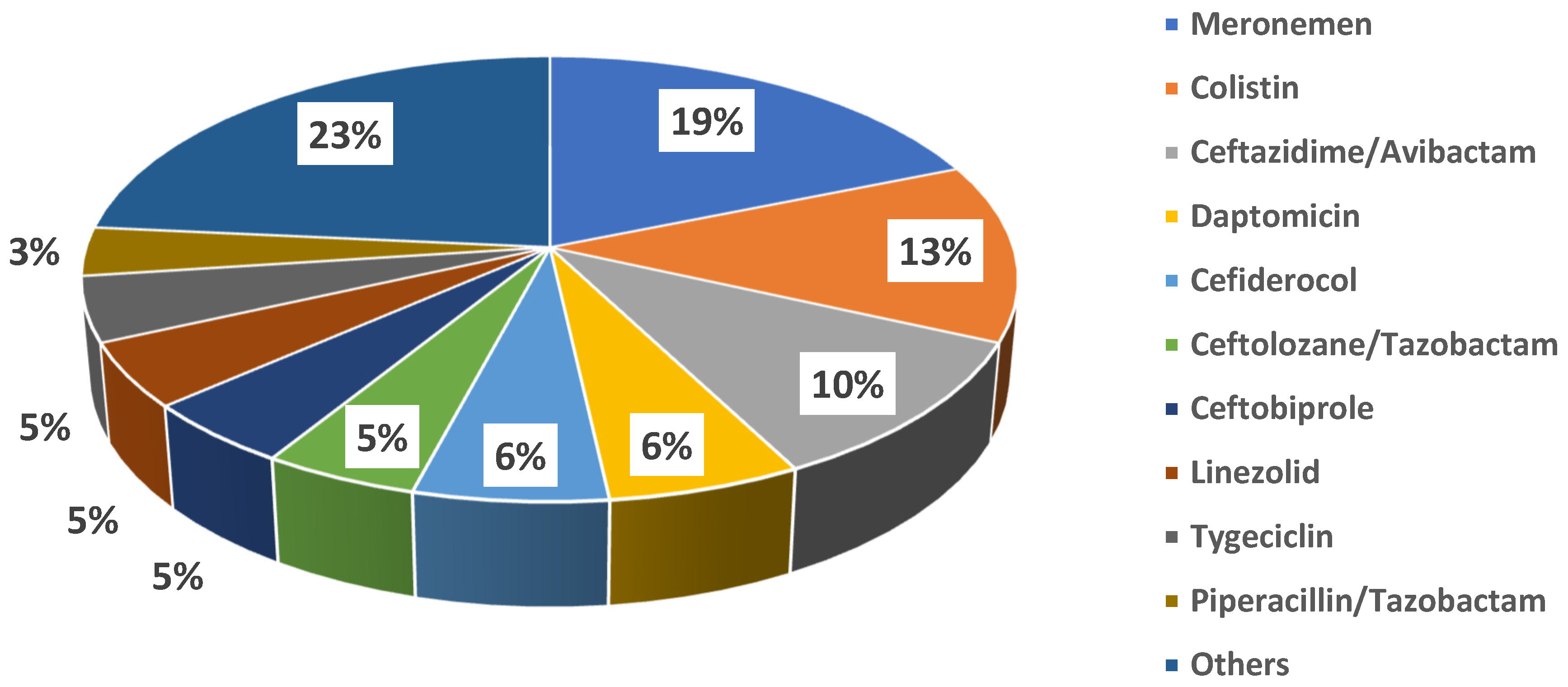
3.3. Patterns of Fosfomycin Use
3.4. Clinical Outcomes
3.5. Changes in Hematochemical Parameters
Electrolyte Imbalances
3.6. Outcomes of Hospitalization and All-Cause Mortality
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karruli, A.; Andini, R.; Corcione, A.; Durante-Mangoni, E. Prevention and control of intensive care unit-acquired carbapenem-resistant Klebsiella pneumoniae: Need for a multimodal approach. Ann. Transl. Med. 2019, 7 (Suppl. 8), S325. [Google Scholar] [CrossRef]
- Giurazza, R.; Mazza, M.C.; Andini, R.; Sansone, P.; Pace, M.C.; Durante-Mangoni, E. Emerging Treatment Options for Multi-Drug-Resistant Bacterial Infections. Life 2021, 11, 519. [Google Scholar] [CrossRef]
- Nelson, R.E.; Hyun, D.; Jezek, A.; Samore, M.H. Mortality, Length of Stay, and Healthcare Costs Associated with Multidrug-Resistant Bacterial Infections Among Elderly Hospitalized Patients in the United States. Clin. Infect. Dis. 2022, 74, 1070–1080. [Google Scholar] [CrossRef]
- Dijkmans, A.C.; Zacarías, N.V.O.; Burggraaf, J.; Mouton, J.W.; Wilms, E.B.; Van Nieuwkoop, C.; Touw, D.J.; Stevens, J.; Kamerling, I.M.C. Fosfomycin: Pharmacological, Clinical and Future Perspectives. Antibiotics 2017, 6, 24. [Google Scholar] [CrossRef]
- Grabein, B.; Graninger, W.; Rodriguez-Bano, J.; Dinh, A.; Liesenfeld, D. Intravenous Fosfomycin: Back to the future. Systematic review and meta-analysis of the clinical literature. Clin. Microbiol. Infect. 2017, 23, 363–372. [Google Scholar] [CrossRef]
- Pontikis, K.; Karaiskos, I.; Bastani, S.; Dimopoulos, G.; Kalogirou, M.; Katsiari, M.; Oikonomou, A.; Poulakou, G.; Roilides, E.; Giamarellou, H. Outcomes of critically ill intensive care unit patients treated with Fosfomycin for infections due to pandrug-resistant and extensively drug-resistant carbapenemase-producing Gram-negative bacteria. Int. J. Antimicrob. Agents 2014, 43, 52–59. [Google Scholar] [CrossRef]
- Kollef, M.H.; Shorr, A.F.; Bassetti, M.; Timsit, J.-F.; Micek, S.T.; Michelson, A.P.; Garnacho-Montero, J. Timing of antibiotic therapy in the ICU. Crit. Care 2021, 25, 360. [Google Scholar] [CrossRef]
- Fosfomycin SmPC, EMA, 2017 April 6. Available online: https://www.ema.europa.eu/en/documents/psusa/fosfomycin-iv-formulation-list-nationally-authorised-medicinal-products-psusa00010336201607_en.pdf (accessed on 16 June 2025).
- Hashemian, S.M.; Farhadi, Z.; Farhadi, T. Fosfomycin: The characteristics, activity, and use in critical care. Ther. Clin. Risk Manag. 2019, 15, 525–530. [Google Scholar] [CrossRef]
- Stengel, D.; Görzer, E.; Schintler, M. Second-line Treatment of Limb-Threatening Diabetic Foot Infections with Intravenous Fosfomycin. J. Chemother. 2005, 17, 527–535. [Google Scholar] [CrossRef]
- Biscarini, S.; Mangioni, D.; Bobbio, C.; Mela, L.; Alagna, L.; Baldelli, S.; Blasi, F.; Canetta, C.; Ceriotti, F.; Gori, A.; et al. Adverse events during intravenous fosfomycin therapy in a real-life scenario. Risk factors and the potential role of therapeutic drug monitoring. BMC Infect. Dis. 2024, 24, 650. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Florent, A.; Chichmanian, R.-M.; Cua, E.; Pulcini, C. Adverse events associated with intravenous Fosfomycin. Int. J. Antimicrob. Agents 2011, 37, 82–83. [Google Scholar] [CrossRef]
- Kaye, K.S.; Rice, L.B.; Dane, A.L.; Stus, V.; Sagan, O.; Fedosiuk, E.; Das, A.F.; Skarinsky, D.; Eckburg, P.B.; Ellis-Grosse, E.J. Fosfomycin for Injection (ZTI-01) Versus Piperacillin-tazobactam for the Treatment of Complicated Urinary Tract Infection Including Acute Pyelonephritis: ZEUS, A Phase 2/3 Randomized Trial. Clin. Infect. Dis. 2019, 69, 2045–2056. [Google Scholar] [CrossRef]
- Savaj, P.; Davda, K.; Sunavala, A.; Soman, R. Our Experience with IV Fosfomycin. Open Forum Infect. Dis. 2018, 5, S721. [Google Scholar] [CrossRef]
- Falagas, M.E.; Vouloumanou, E.K.; Samonis, G.; Vardakasa, K.Z. Fosfomycin. Clin. Microbiol. Rev. 2016, 29, 321–347. [Google Scholar] [CrossRef]
- Iarikov, D.; Wassel, R.; Farley, J.; Nambiar, S. Adverse Events Associated with Fosfomycin Use: Review of the Literature and Analyses of the FDA Adverse Event Reporting System Database. Infect. Dis. Ther. 2015, 4, 433–458. [Google Scholar] [CrossRef]
- Putensen, C.; Ellger, B.; Sakka, S.G.; Weyland, A.; Schmidt, K.; Zoller, M.; Weiler, N.; Kindgen-Milles, D.; Jaschinski, U.; Weile, J.; et al. Current clinical use of intravenous Fosfomycin in ICU patients in two European countries. Infection 2019, 47, 827–836. [Google Scholar] [CrossRef]
- Malnic, G.; Muto, S.; Giebisch, G. Regulation of Potassium Excretion. In Seldin and Giebisch’s The Kidney; Academic Press: Cambridge, MA, USA, 2008; pp. 1301–1347. [Google Scholar] [CrossRef]
- Swaminathan, R. Magnesium Metabolism and its Disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar]
- Dawson-Hughes, B.; Fowler, S.E.; Dalsky, G.; Gallagher, C. Sodium Excretion Influences Calcium Homeostasis in Elderly Men and Women. J. Nutr. 1996, 126, 2107–2112. [Google Scholar] [CrossRef]
- Canamares-Orbis, I.; Silva, J.T.; López-Medrano, F.; Aguado, J.M. Is high-dose intravenous Fosfomycin safe for the treatment of patients prone to heart failure? Enfermedades Infecc. Microbiol. Clínica 2015, 33, 294. [Google Scholar] [CrossRef]
- Candel, F.J.; Matesanz, M.; Martín-Sánchez, F.J.; Castillo, J.M. Monitoring of high-dose Fosfomycin guided by NT-proBNP. Int. J. Cardiol. 2016, 209, 131–132. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Number | 56 |
|---|---|
| Age, median [IQR] | 62.4 [30–75] |
| Sex (M/F)—n. (%) | 38 (68)/18 (32) |
| BMI, median [IQR] | 26.7 [23.6–30] |
| Pack/years, median [IQR] | 49.9 [30–75] |
| CCI, median [IQR] | 4 [3–6] |
| Haemoglobin, g/dL, median [IQR] | 9.7 [8.1–10.75] |
| Erytrocytes, cells/μL, median [IQR] | 3460 [2850–3780] |
| Leukocytes, cells/μL, median [IQR] | 9920 [7150–14,777] |
| Neutrophils, cells/μL, median [IQR] | 8340 [6130–13,000] |
| Platelets, cells/μL, median [IQR] | 210 [115–303] |
| INR, median [IQR] | 1.2 [1.13–1.38] |
| aPTT, s, median [IQR] | 33.5 [30.95–40.45] |
| C-Reactive Protein, mg/dL, median [IQR] | 11.6 [5.7–18.35] |
| Creatinine, mg/dL, median [IQR] | 1 [0.6–1.7] |
| Estimated GFR, mL/min, median [IQR] | 78.5 [41.5–107.8] |
| Urea, mg/dL, median [IQR] | 52 [31–96.5] |
| Fasting Glucose, mg/dL, median [IQR] | 107 [88.25–137.5] |
| AST, IU/L, median [IQR] | 25 [15–39] |
| ALT, IU/L, median [IQR] | 24.5 [13.25–51.75] |
| Total Bilirubin, mg/dL, median [IQR] | 0.6 [0.4–0.98] |
| Sodium, mEq/L, median [IQR] | 138 [136–140] |
| Potassium, mEq/L, median [IQR] | 3.9 [3.7–4.3] |
| Calcium, mEq/L, median [IQR] | 8.6 [8–9] |
| Magnesium, mEq/L, median [IQR] | 1.8 [1.6–2.1] |
| Chloride, mEq/L, median [IQR] | 103 [101–106] |
| Number of Patients | 56 |
|---|---|
| Duration of treatment, median [IQR] | 10 [5–13.5] |
| Bloodstream infections | 15 [9–19.5] |
| Respiratory tract infections | 8 [5–12] |
| Urinary tract infections | 7 [5–10] |
| Bone Infections | 13 [6–26] |
| Surgical site infections | 9.5 [7.5–10.8] |
| Co-administered antibiotics, n (%) | |
| Meronemen | 16 (28.6) |
| Colistin | 11 (19.6) |
| Ceftazidime/Avibactam | 9 (16.1) |
| Daptomicin | 5 (8.9) |
| Cefiderocol | 5 (8.9) |
| Ceftolozane/Tazobactam | 4 (7.1) |
| Ceftobiprole | 4 (7.1) |
| Linezolid | 4 (7.1) |
| Tygeciclin | 4 (7.1) |
| Piperacillin/Tazobactam | 3 (5.4) |
| Amikacin | 2 (3.6) |
| Gentamicin | 2 (3.6) |
| Amoxicillin/Clavulanate | 2 (3.6) |
| Cotrimoxazole | 2 (3.6) |
| Teicoplanin | 2 (3.6) |
| Vancomycin | 2 (3.6) |
| Meropenem/vaborbactam | 2 (3.6) |
| Ertapenem | 1 (1.8) |
| Cefepime | 1 (1.8) |
| Metronidazole | 1 (1.8) |
| Ceftaroline | 1 (1.8) |
| Ampicillin/Sulbactam | 1 (1.8) |
| Cefazolina | 1 (1.8) |
| Infection onset to start of treatment, days, median [IQR] | 7 [3–25] |
| Therapeutic strategy, n (%) | |
| Empirical therapy | 29 (51.8) |
| Targeted therapy | 27 (48.2) |
| Dosage^ in patients with impaired renal function*, mean (SD) | |
| 3 A (eGFR 59-45 ml/min/1.73 m2) | 16 (±4.3) |
| 3 B (eGFR 44-30 ml/min/1.73 m2) | 12 (±5.9) |
| 4 (eGFR 29-15 ml/min/1.73 m2) | 12 (±7) |
| 5/5D (eGFR < 15 ml/min/1.73 and/or dialysis) | 12 (±16) |
| ALIVE (42) | DEAD (14) | p Value | ||
|---|---|---|---|---|
| Age, median [IQR] | 67.5 [56.8–70] | 58.5 [31.5–75.8] | 0.35 | |
| CCI, median [IQR] | 4 [2.5–5.5] | 5.5 [4.1–6.9] | 0.13 | |
| Admission ward, n. (%) | Cardiology Unit | 1 (2.4) | 1 (7.1) | 0.4 |
| Respiratory Medicine Unit | 1 (2.4) | 3 (21.4) | 0.04 | |
| Cardiothoracic Surgery Unit | 5 (11.9) | 1 (7.1) | 0.62 | |
| Intensive Care Unit | 8 (19.0) | 9 (64.3) | <0.01 | |
| Internal Medicine Unit | 27 (64.3) | 0 (0) | <0.01 | |
| Infective syndrome, n. (%) | Bloodstream Infections | 8 (19) | 3 (21.4) | 1 |
| Respiratory Tract Infections | 13 (31) | 10 (71) | 0.01 | |
| Urinary Tract Infections | 9 (21) | 0 (0) | 0.09 | |
| Bone Infections | 9 (21) | 0 (0) | 0.09 | |
| Surgical Site Infections | 3 (7) | 1 (7) | 1 | |
| Causative pathogen, n. (%) | Acinetobacter baumannii | 2 (4.8) | 2 (14.3) | 0.23 |
| Corynebacterium striatum | 1 (2.4) | 0 (0) | 0.76 | |
| Enterobacter aerogenes | 2 (4.8) | 0 (0) | 0.97 | |
| Enterobacter cloacae | 3 7.1) | 0 (0) | 0.75 | |
| Enterococcus faecalis | 2 (4.8) | 0 (0) | 0.97 | |
| Enterococcus faecium | 1 (2.4) | 3 (21.4) | 0.04 | |
| Enterococcus raffinosus | 1 (2.4) | 0 (0) | 0.76 | |
| Escherichia coli | 11 (26.2) | 1 (7.1) | 0.13 | |
| Haemophilus influenza | 1 (2.4) | 0 (0) | 0.76 | |
| Hafnia alvei | 1 (2.4) | 1 (7.1) | 0.4 | |
| Klebsiella pneumonia | 8 (19.0) | 4 (28.6) | 0.45 | |
| Moraxella catarrhalis | 0 (0) | 1 (7.1) | 0.1 | |
| Pseudomonas aeruginosa | 9 (21.4) | 4 (28.6) | 0.58 | |
| Pseudomonas putida | 0 (0) | 1 (7.1) | 0.1 | |
| Sphingomonas paucimobilis | 1 (2.4) | 0 (0) | 0.76 | |
| Staphylococcus aureus | 6 (14.3) | 2 (14.3) | 1 | |
| Staphylococcus epidermidis | 2 (4.8) | 2 (14.3) | 0.23 | |
| Staphylococcus haemolyticus | 0 (0) | 2 (14.3) | 0.02 | |
| Staphylococcus hominis | 4 (9.5) | 0 (0) | 0.59 | |
| Staphylococcus simulans | 1 (2.4) | 0 (0) | 0.76 | |
| Stenotrophomonas maltophilia | 1 (2.4) | 1 (7.1) | 0.4 | |
| Main comorbidities, n. (%) | Renal disease | 11 (26.2) | 6 (42.8) | 0.24 |
| Heart disease | 9 (21.4) | 6 (42.8) | 0.12 | |
| Respiratory syndromes | 9 (21.4) | 4 (28.5) | 0.58 | |
| Diabetes mellitus | 12 (28.6) | 4 (28.5) | 1 | |
| Patients’ outcomes, n.(%) | Complete resolution | 19 (45.2) | 3 (21.4) | 0.20 |
| Partial resolution | 21 (50) | 7 (50) | 1 | |
| No resolution | 0 (0) | 1 (7.1) | 0.25 | |
| Not enough data | 2 (4.7) | 3 (21.4) | - |
| Parameter | BL | EOT | p-Value |
|---|---|---|---|
| Hematochemical Parameters | Median [IQR] | Median [IQR] | |
| CRP (mg/dL) | 11.6 [5.7–18.3] | 4.8 [2.7–8.7] | <0.01 |
| SOFA score (0–48/72h) | 3 [1–6] | 3 [1–5] | 0.43 |
| RBC (cells ×103/µL) | 3460 [2850–3780] | 3275 [2965–3795] | 0.79 |
| WBC (cells/µL) | 9920 [7150–14,777] | 7780 [5997–12,770] | 0.08 |
| NEUT (cells/µL)) | 8340 [6130–13,000] | 5730 [3815–9200] | 0.01 |
| PLT (cells ×103/µL) | 210 [115–303] | 233 [160–300] | 0.32 |
| HGB (g/dL) | 9.7 [8.1–10.75] | 9.1 [8.38–10.53] | 0.90 |
| CREA (mg/dL) | 1 [0.6–1.7] | 0.83 [0.6–1.2] | 0.22 |
| eGFR (mL/min/1.73m2) | 78.5 [41.5–107.8] | 92.7 [56–110] | 0.31 |
| UREA (mg/dL) | 52 [31–96.5] | 40.5 [28–70] | 0.13 |
| INR | 1.22 [1.13–1.37] | 1.25 [1.13–1.47] | 0.65 |
| aPTT (sec.) | 33.5 [30.95–40.45] | 34.55 [30.65–38.18] | 0.84 |
| AST (IU/L) | 25 [15–39] | 21 [14–35] | 0.58 |
| ALT (IU/L) | 24.5 [13.25–51.75] | 20.5 [12–42] | 0.51 |
| TOTAL BILIRUBIN (mg/dL) | 0.6 [0.4–0.98] | 0.55 [0.3–1.03] | 0.54 |
| Na+ (mEq/L) | 138 [136–140] | 140 [139–143] | <0.01 |
| K+ (mEq/L) | 3.9 [3.7–4.3] | 3.9 [3.63–4.38] | 0.76 |
| Ca2+ (mEq/L) | 8.6 [8–9] | 8.15 [7.48–8.75] | 0.10 |
| Mg2+ (mEq/L) | 1.8 [1.6–2.1] | 1.8 [1.48–1.93] | 0.61 |
| Cl− (mEq/L) | 103 [101–106] | 103 [101–105.75] | 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luciano, F.; Bertolino, L.; Patauner, F.; Boccia, F.; Gallo, R.; Sommese, P.; Peluso, A.M.C.; Infante, O.; Mercadante, S.; Delle Femine, A.; et al. Efficacy and Safety of Fosfomycin Disodium in Patients with Bacterial Infections: A Single-Center, Real-Life Clinical Study. J. Clin. Med. 2025, 14, 4386. https://doi.org/10.3390/jcm14124386
Luciano F, Bertolino L, Patauner F, Boccia F, Gallo R, Sommese P, Peluso AMC, Infante O, Mercadante S, Delle Femine A, et al. Efficacy and Safety of Fosfomycin Disodium in Patients with Bacterial Infections: A Single-Center, Real-Life Clinical Study. Journal of Clinical Medicine. 2025; 14(12):4386. https://doi.org/10.3390/jcm14124386
Chicago/Turabian StyleLuciano, Fabio, Lorenzo Bertolino, Fabian Patauner, Filomena Boccia, Raffaella Gallo, Pino Sommese, Anna Maria Carolina Peluso, Oriana Infante, Silvia Mercadante, Augusto Delle Femine, and et al. 2025. "Efficacy and Safety of Fosfomycin Disodium in Patients with Bacterial Infections: A Single-Center, Real-Life Clinical Study" Journal of Clinical Medicine 14, no. 12: 4386. https://doi.org/10.3390/jcm14124386
APA StyleLuciano, F., Bertolino, L., Patauner, F., Boccia, F., Gallo, R., Sommese, P., Peluso, A. M. C., Infante, O., Mercadante, S., Delle Femine, A., Karruli, A., Andini, R., Zampino, R., & Durante-Mangoni, E. (2025). Efficacy and Safety of Fosfomycin Disodium in Patients with Bacterial Infections: A Single-Center, Real-Life Clinical Study. Journal of Clinical Medicine, 14(12), 4386. https://doi.org/10.3390/jcm14124386