

Volume Change Measurements of the Heart and Lungs After Pectus Excavatum Repair


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
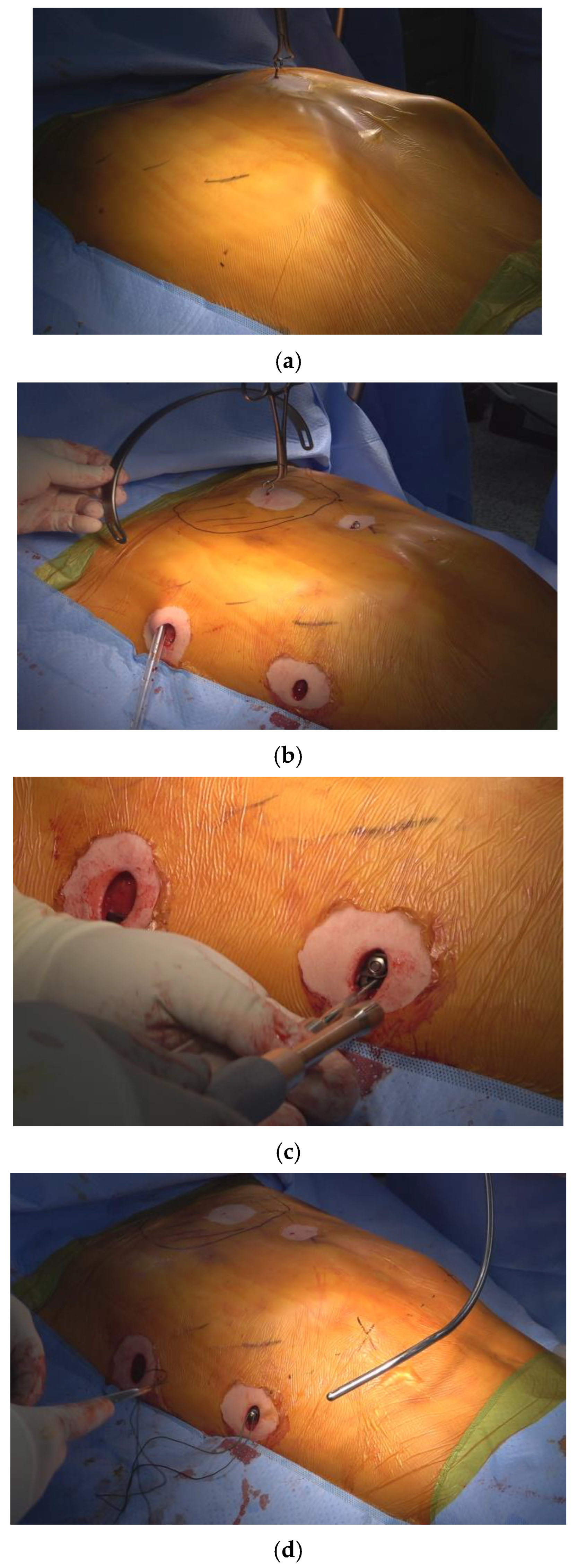
2.2. Surgical Procedures
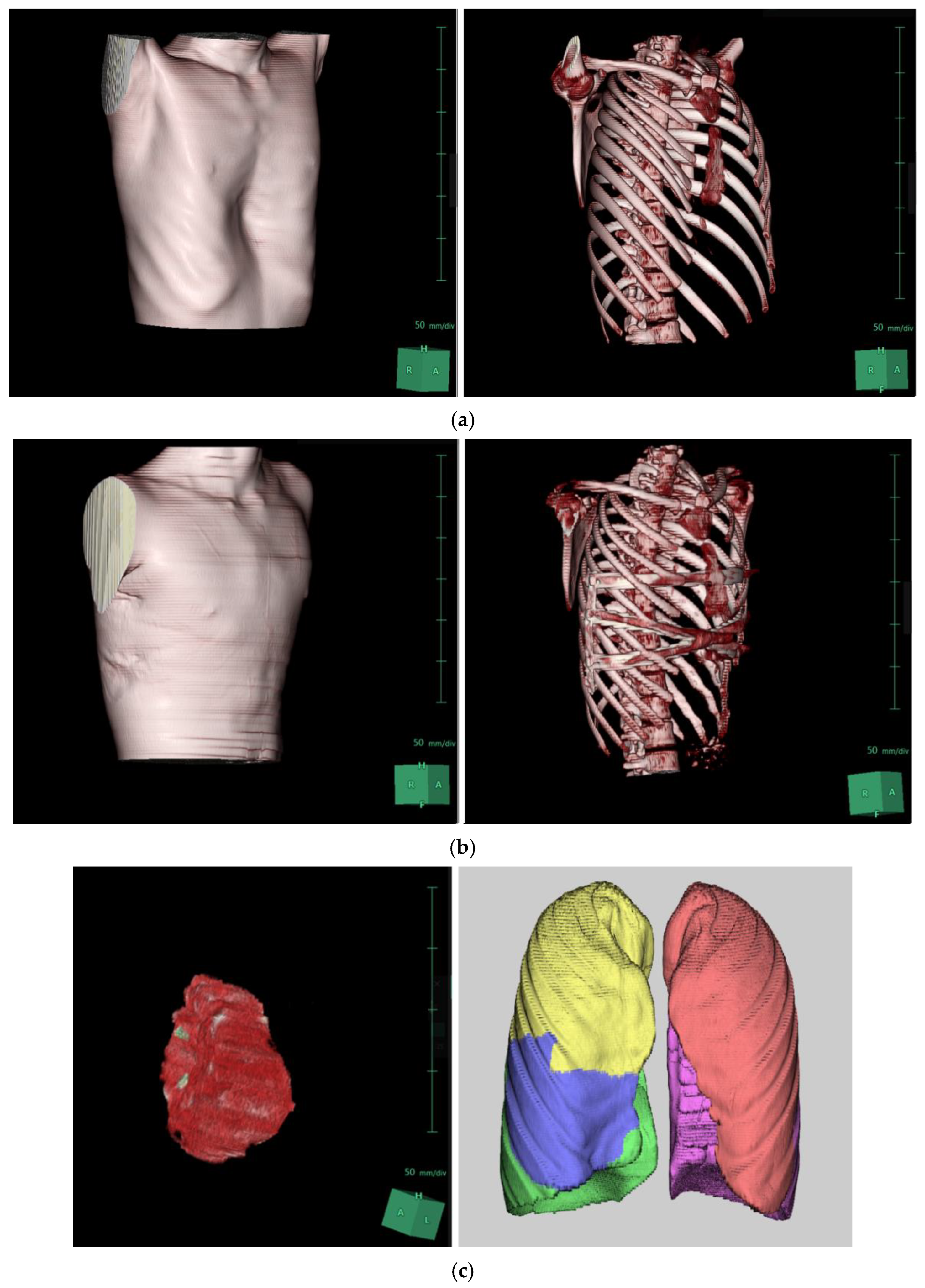
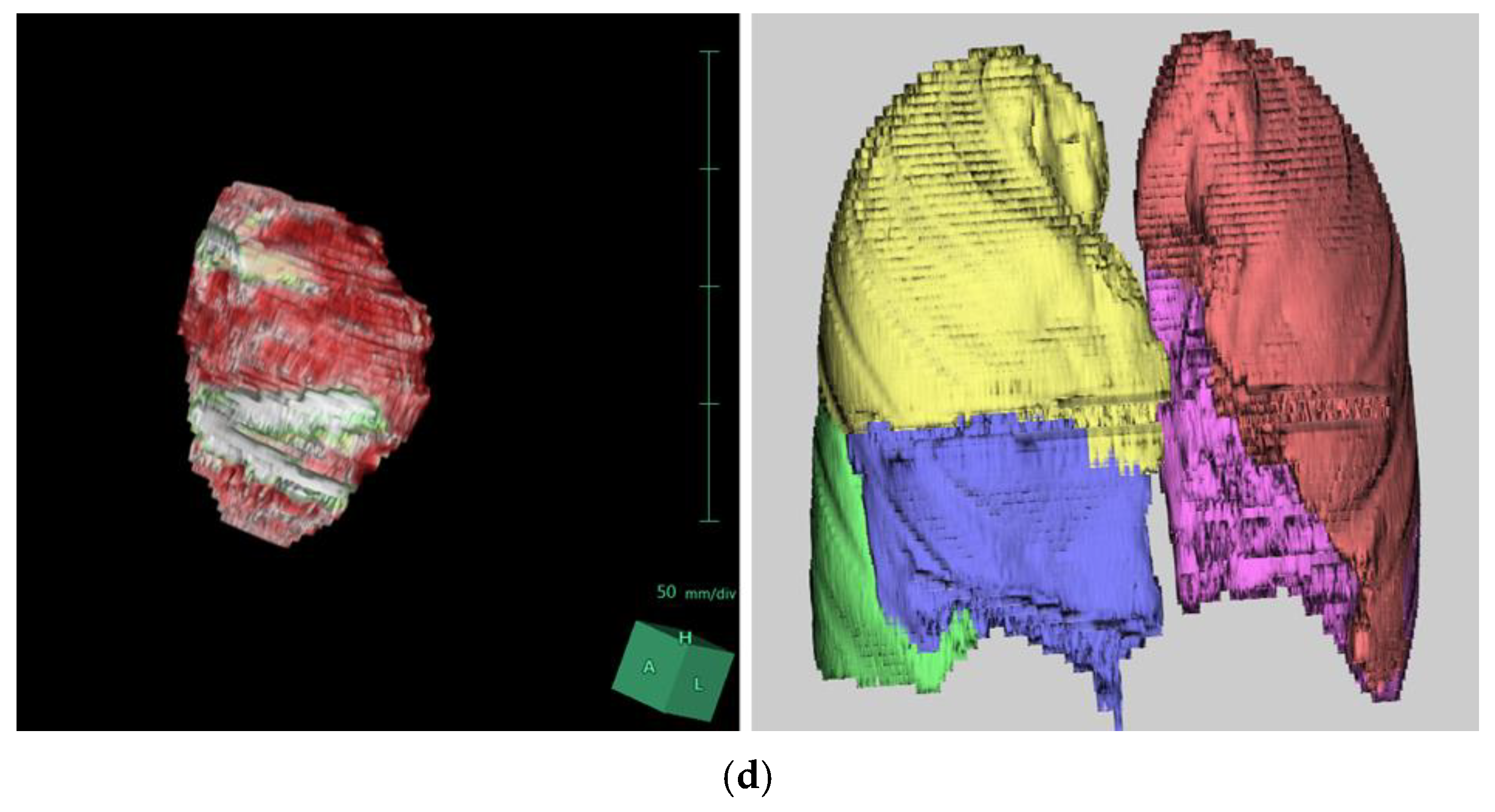
2.3. Three-Dimensional Synapse Program and Volumetric Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
References
- Janssen, N.; Coorens, N.A.; Franssen, A.J.; Daemen, J.H.; Michels, I.L.; Hulsewé, K.W.; Vissers, Y.L.; de Loos, E.R. Pectus excavatum and carinatum: A narrative review of epidemiology, etiopathogenesis, clinical features, and classification. J. Thorac. Dis. 2024, 16, 1687–1701. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Park, I.K.; Kim, Y.T.; Kim, W.S.; Kang, C.H. Classification of Pectus Excavatum According to Objective Parameters From Chest Computed Tomography. Ann. Thorac. Surg. 2016, 102, 1886–1891. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Lee, S.Y.; Lee, C.S.; Youm, W.; Lee, K.R. The Nuss procedure for pectus excavatum: Evolution of techniques and early results on 322 patients. Ann. Thorac. Surg. 2004, 77, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Rim, G.; Yoon, S.K. Recent Advancements in Pectus Surgery: Crane Lifting, Multiple-Bar Approach, Bridge Stabilization, and Sandwich Technique. J. Pediatr. Surg. 2024, 59, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Jeong, J.Y.; Jo, W.M.; Shin, J.S.; Lee, I.S.; Kim, K.T.; Choi, Y.H. Minimally invasive repair of pectus excavatum: A novel morphology-tailored, patient-specific approach. J. Thorac. Cardiovasc. Surg. 2010, 139, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rim, G.; Park, H.J. Technical Advances in Pectus Bar Stabilization in Chest Wall Deformity Surgery: 10-Year Trends and an Appraisal with 1500 Patients. J. Chest Surg. 2023, 56, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Haecker, F.M.; Krebs, T.F.; Kleitsch, K.U. Current Development of Minimally Invasive Repair of Pectus Excavatum (MIRPE). Children 2022, 9, 478. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Rim, G.; Yoon, S.K. Crane-powered pectus excavatum repair: The NeoPectus surgery. Front. Surg. 2023, 10, 1267009. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Rim, G.M. Development of a Screw-Crane System for Pre-Lifting the SternalDepression in Pectus Excavatum Repair: A Test of Mechanical Properties for the Feasibility of a New Concept. J. Chest Surg. 2021, 54, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Haecker, F.M.; Krebs, T.; Kocher, G.J.; Schmid, R.A.; Sesia, S.B. Sternal elevation techniques during the minimally invasive repair of pectus excavatum. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, K.S.; Moon, Y.K.; Lee, S. The bridge technique for pectus bar fixation: A method to make the bar un-rotatable. J. Pediatr. Surg. 2015, 50, 1320–1322. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, K.S. The sandwich technique for repair of pectus carinatum and excavatum/carinatum complex. Ann. Cardiothorac. Surg. 2016, 5, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J. A technique for complex pectus excavatum repair: The cross-bar technique for grand canyon type deformity (Park classification). Ann. Cardiothorac. Surg. 2016, 5, 526–527. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, A.; Kato, M.; Motoki, M.; Sugai, H.; Okubo, N. Quantified Aortic Luminal Irregularity as a Predictor of Complications and Prognosis After Endovascular Aneurysm Repair. Medicine 2016, 95, e2863. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Ishikawa, M.; Yamamoto, K. Comparison of CSF Distribution between Idiopathic Normal Pressure Hydrocephalus and Alzheimer Disease. AJNR Am. J. Neuroradiol. 2016, 37, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Jaroszewski, D.E.; Farina, J.M.; Gotway, M.B.; Stearns, J.D.; Peterson, M.A.; Pulivarthi, V.S.; Bostoros, P.; Abdelrazek, A.S.; Gotimukul, A.; Majdalany, D.S.; et al. Cardiopulmonary Outcomes After the Nuss Procedure in Pectus Excavatum. J. Am. Heart Assoc. 2022, 11, e022149. [Google Scholar] [CrossRef] [PubMed]
- Abu-Tair, T.; Turial, S.; Hess, M.; Wiethoff, C.M.; Staatz, G.; Lollert, A.; Kampmann, C. Impact of Pectus Excavatum on Cardiopulmonary Function. Ann. Thorac. Surg. 2018, 105, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Malek, M.H.; Berger, D.E.; Marelich, W.D.; Coburn, J.W.; Beck, T.W.; Housh, T.J. Pulmonary function following surgical repair of pectus excavatum: A meta-analysis. Eur. J. Cardio-Thorac. Surg. 2006, 30, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Lawson, M.L.; Mellins, R.B.; Tabangin, M.; Kelly, R.E., Jr.; Croitoru, D.P.; Goretsky, M.J.; Nuss, D. Impact of pectus excavatum on pulmonary function before and after repair with the Nuss procedure. J. Pediatr. Surg. 2005, 40, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Neviere, R.; Montaigne, D.; Benhamed, L.; Catto, M.; Edme, J.L.; Matran, R.; Wurtz, A. Cardiopulmonary response following surgical repair of pectus excavatum in adult patients. Eur. J. Cardiothorac. Surg. 2011, 40, e77–e82. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| XI Repair (n = 63) | |
|---|---|
| Age, years (range) | 16.95 (11–37) |
| Height, cm (range) | 169.35 (146–185) |
| Weight, kg (range) | 53.20 (32–87) |
| BMI, kg/m2 (range) | 18.26 (14.2–25.1) |
| Male sex (percentage) | 52 (82.54) |
| Race, Asian (percentage) | 61 (96.82) |
| ASA class (percentage) | |
| ASA I | 61 (96.82) |
| ASA II | 2 (3.18) |
| XI Repair (n = 63) | p Value | |
|---|---|---|
| Depression index (DI) | ||
| Pre (range) | 1.87 (1.39–3.3) | |
| Post (range) | 1.02 (1.00–1.09) | |
| Δ DI | 0.85 (0.3–2.23) | <0.01 |
| Haller index (HI) | ||
| Pre | 4.07 (3.02–7.67) | |
| Post | 2.38 (1.39–3.37) | |
| Δ HI | 1.65 (0.53–4.3) | <0.01 |
| Morphological type | ||
| PE, symmetric type | 40 (63.50) | |
| PE, asymmetric type | 23 (36.50) | |
| Operative time, min | 98.57 (65–150) | |
| Intraoperative transfusion | 0 (0) | |
| Pectus bar size, inch | 13.49 (11–15) | |
| Pectus bar shape | ||
| XI | 63 (100) | |
| Number of pectus bars | ||
| 3 | 63 (100) | |
| Pectus bar stabilization | ||
| Bridge plate | 63 (100) | |
| Crane application | 63 (100) | |
| Pectoscope | 63 (100) | |
| Flare buster | 63 (100) | |
| Magic string | 63 (100) |
| XI Repair (n = 63) | |
|---|---|
| Length of stay, days | 4.52 (4–7) |
| Complications | |
| Pneumothorax | 8 (12.70) |
| Hemothorax | 1 (1.6) |
| Pneumonia | 2 (3.2) |
| Wound complications | 1 (1.6) |
| Thoracic outlet syndrome (TOS) | 1 (1.6) |
| Bar dislocation | 0 |
| Re-operation | 0 |
| Readmission in 30 days | 0 |
| XI Repair (n = 63) | p Value | |
|---|---|---|
| Lung volume | ||
| Total | ||
| Pre (range) | 4371.31 (2034.1–6447.6) | |
| Post (range) | 4266.87 (2385.3–6446.8) | |
| Δ volume | −104.42 (−569.6–712.3) | 0.52 |
| Left | ||
| Pre (range) | 2052.51 (929.5–3004.6) | |
| Post (range) | 2022.61 (1111.1–3048.2) | |
| Δ volume | −29.90 (−713.2–347.3) | 0.64 |
| Right | ||
| Pre (range) | 2318.77 (1104.5–3443) | |
| Post (range) | 2310.86 (1268.4–3418.6) | |
| Δ volume | −7.90 (443.2–395.6) | 0.70 |
| Heart volume | ||
| Pre | 458.25 (289.8–647.4) | |
| Post | 499.13 (332.7–726.5) | |
| Δ volume | 40.89 (−35–170.35) | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rim, G.; Hyun, K.; Park, H.J. Volume Change Measurements of the Heart and Lungs After Pectus Excavatum Repair. J. Clin. Med. 2025, 14, 4250. https://doi.org/10.3390/jcm14124250
Rim G, Hyun K, Park HJ. Volume Change Measurements of the Heart and Lungs After Pectus Excavatum Repair. Journal of Clinical Medicine. 2025; 14(12):4250. https://doi.org/10.3390/jcm14124250
Chicago/Turabian StyleRim, Gongmin, Kwanyong Hyun, and Hyung Joo Park. 2025. "Volume Change Measurements of the Heart and Lungs After Pectus Excavatum Repair" Journal of Clinical Medicine 14, no. 12: 4250. https://doi.org/10.3390/jcm14124250
APA StyleRim, G., Hyun, K., & Park, H. J. (2025). Volume Change Measurements of the Heart and Lungs After Pectus Excavatum Repair. Journal of Clinical Medicine, 14(12), 4250. https://doi.org/10.3390/jcm14124250