4.2. Factors Contributing to SPMS Progression
The progression from RRMS to SPMS is influenced by various clinical, radiological, genetic, environmental, and molecular factors. Understanding these contributors is critical for identifying patients at high risk and tailoring early therapeutic strategies.
One of the most robust clinical predictors of disease progression is the rate of early disability accumulation. Patients who reach an Expanded Disability Status Scale (EDSS) score of 3.0 within five years of onset or 4.0 within ten years have a significantly higher likelihood of transitioning to SPMS earlier than those with a more indolent disease course [
3]. Rapid disability progression in the early years of RRMS suggests a more aggressive inflammatory burden and limited compensatory mechanisms [
3]. MRI biomarkers also provide critical prognostic information about the disease. A high lesion burden on T2-weighted imaging, early presence of T1-hypointense lesions (“black holes”), and pronounced atrophy, especially of the thalamus and cortical gray matter, are all associated with faster progression to SPMS [
2,
6,
8]. The presence of spinal cord lesions further increases the likelihood of progression due to their direct impact on the motor pathways [
6]. Additionally, a high frequency of gadolinium-enhancing lesions in early RRMS correlates with greater inflammatory activity and is associated with a more rapid transition to SPMS [
2].
Sex and age at disease onset are important demographic factors. Although RRMS is more prevalent in females, the male sex is linked to a more aggressive disease course and earlier conversion to SPMS, possibly due to reduced neuroprotective hormonal effects [
2]. Similarly, older age at disease onset is associated with a shorter time to SPMS, likely due to diminished remyelination capacity and neuroplasticity in aging neural tissue [
2].
Lifestyle and environmental factors also modulate the disease progression. Among these, smoking is one of the most consistently reported risk factors. Smokers with MS progress to SPMS approximately five years earlier than non-smokers, and the effect is dose-dependent. Smoking is thought to exacerbate disease progression through mechanisms such as increased oxidative stress, promotion of chronic inflammation, and impaired blood–brain barrier repair [
2]. Comorbidities, especially vascular risk factors such as hypertension, diabetes, and hyperlipidemia, have also been shown to accelerate disability accumulation and cognitive decline in patients with MS. These conditions may potentiate microvascular ischemia and amplify neuroinflammatory cascades, worsening the underlying CNS pathology [
6,
7].
From a genetic perspective, carriers of the HLA-DRB1*15:01 allele not only face a higher risk of developing MS but may also experience a more severe disease phenotype and a faster transition to SPMS [
3]. Although this association is well documented, ongoing studies are investigating the roles of additional loci and polygenic risk scores in predicting disease progression.
Emerging research has identified potential molecular and immunological markers of its progression. Elevated serum neurofilament light chain (NfL) levels have been associated with axonal damage and correlated with future disability in both RRMS and SPMS [
17]. Moreover, alterations in vitamin D metabolism, often marked by deficiency, have been implicated in increased disease activity and accelerated progression, although the findings remain heterogeneous [
26]. Additionally, the gut microbiome and prior Epstein–Barr virus (EBV) infection have garnered attention as potential modulators of disease progression. While EBV is universally present in patients with MS and may trigger early autoimmunity, its direct role in SPMS progression remains poorly defined [
26]. Similarly, dysbiosis of the gut microbiota may influence neuroinflammation; however, further mechanistic studies are needed to elucidate the causal links [
26].
4.4. Cognitive Decline in SPMS
Cognitive impairment is a major aspect of SPMS progression, affecting various domains, including memory, executive function, and information-processing speed. Epidemiological data suggest that up to 70% of patients with SPMS experience significant cognitive decline, which worsens over time due to cortical and subcortical atrophy [
2]. Unlike RRMS, where cognitive dysfunction is often episodic and linked to relapses, in SPMS, cognitive dysfunction progresses steadily, reflecting ongoing neurodegeneration rather than inflammation [
3].
MRI studies have shown that brain atrophy, particularly in the frontal and temporal lobes, is a key factor in cognitive decline. Gray matter atrophy is strongly correlated with worsening memory and reduced processing speed, while subcortical atrophy, including the thalamus, is associated with executive dysfunction and attention deficits [
2]. Furthermore, the presence of chronic T1 hypointense lesions (“black holes”) has been linked to irreversible axonal damage and worsening of cognitive function [
3].
Several risk factors contribute to the accelerated cognitive decline in SPMS. Older age at SPMS onset is associated with more severe cognitive impairment, while a higher lesion load in early RRMS predicts worse cognitive outcomes in the progressive phase [
2]. Additionally, smoking and comorbid vascular diseases, such as hypertension and diabetes, have been shown to exacerbate cognitive dysfunction by increasing neuroinflammation and vascular damage [
3].
The SPMS phase represents an advanced stage of multiple sclerosis, characterized by the progressive accumulation of neurological disabilities without distinct relapses. The impact of this phase on the quality of life of patients is significant and multidimensional. Deterioration of physical function is a defining feature of SPMS and has a direct impact on the quality of life. Reduced mobility, coordination difficulties, and balance problems limit daily activities, reducing independence and social participation. Cognitive dysfunction, including problems with memory, concentration, and information processing, is common in SPMS. This affects the ability to work, maintain social relationships, and carry out recreational activities, having a negative impact on the quality of life [
1,
27].
Fatigue is a common and debilitating symptom of SPMS that is often underestimated. The persistent feeling of physical and mental exhaustion limits the ability to carry out daily and social activities, significantly affecting the quality of life. Chronic pain is another frequent problem in SPMS, with a negative impact on the quality of life. The pain can be neuropathic, muscular, or articular and can affect mobility, sleep, and emotional state [
27].
Depression and anxiety are more common in patients with SPMS than in the general population. Coping with progressive disability, chronic pain, and fatigue can contribute to the appearance of mental health problems, affecting the quality of life. The social impact of SPMS is significant, including difficulties in maintaining a job, loss of financial independence, and social isolation. These problems can affect self-esteem, interpersonal relationships, and quality of life [
27].
Quality of life is influenced by all the factors mentioned above. Patients with SPMS often report a lower quality of life than those with other forms of MS or the general population.
4.5. Utility of MRI in Diagnosis and Monitoring
Global and regional brain volume loss is a key marker of SPMS conversion, as it strongly correlates with accumulating disability. Progressive atrophy of deep gray matter structures, particularly the thalamus, is predictive of disease worsening. Recent large cohort analyses have confirmed that early deep gray matter atrophy (notably thalamic atrophy) is a major driver of long-term disability progression and conversion to SPMS [
8].
- 2.
Cortical Lesions and Thinning
Unlike RRMS, in which white matter lesions are dominant, SPMS is characterized by more extensive cortical demyelination. Advanced imaging techniques have highlighted the importance of cortical lesion burden and leptomeningeal contrast enhancement as markers of SPMS conversion. In progressive MS, the presence of leptomeningeal enhancement on MRI—an in vivo marker of meningeal inflammation—has been associated with accelerated cortical gray matter atrophy over time [
28].
- 3.
Atrophied Lesion Volume (ALV)
A newly recognized biomarker, ALV, quantifies the transition of demyelinated lesions into cerebrospinal fluid, representing irreversible neurodegeneration. It has shown stronger correlations with clinical disability than traditional lesion counts.
- 4.
Slowly Expanding Lesions (SELs)
These smoldering lesions, which display a paramagnetic rim on susceptibility-weighted imaging, indicate chronic active inflammation and are more prevalent in patients with SPMS. SELs are associated with greater tissue destruction and long-term disability progression.
- 5.
Spinal Cord Involvement
While spinal cord atrophy is difficult to measure with standard MRI, emerging imaging protocols now allow for better assessment of spinal cord damage, which is a strong predictor of physical disability in SPMS [
20]. Indeed, pronounced spinal cord atrophy on MRI can precede the clinical onset of SPMS, serving as an early indicator of a progressive disease [
29].
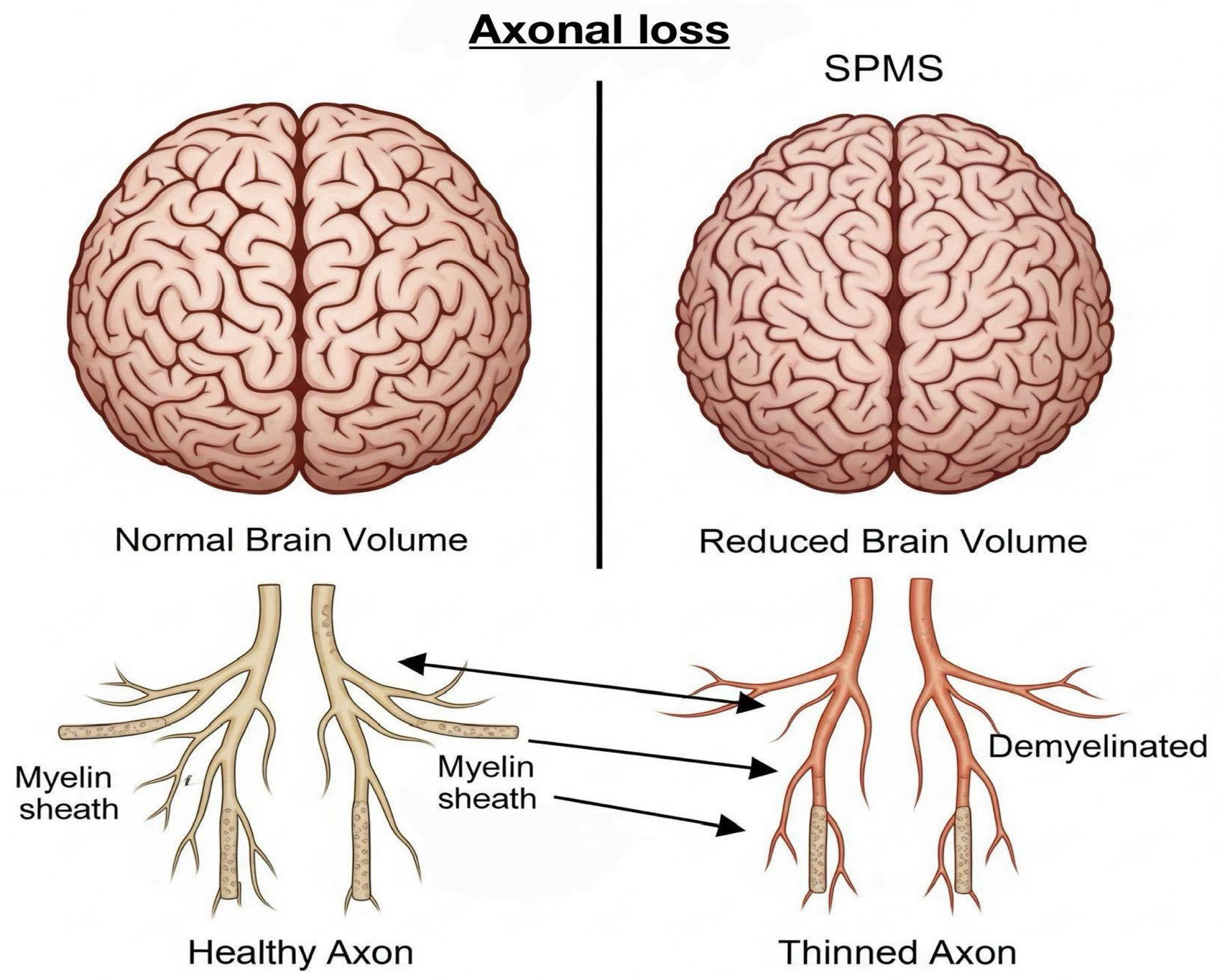
- 6.
Visualization of Axonal Loss
Axonal loss, a critical driver of disability progression in SPMS, is associated with irreversible neurological deficits in patients with SPMS. MRI indirectly detects axonal loss by evaluating brain atrophy, lesion burden, and altered diffusion patterns. Brain atrophy, reflected by reductions in brain volume, particularly in the grey matter (GM) and white matter (WM), is a hallmark of significant axonal degeneration and neuronal loss. Quantitative MRI techniques, including the normalized brain volume (NBV), normalized cortical GM volume (NCGMV), and normalized WM volume (NWMV), are used to assess this loss. It has been shown that patients with SPMS exhibit more pronounced brain volume reduction compared to those with RRMS [
6]. Furthermore, diffusion tensor imaging (DTI) offers additional insights into axonal damage through parameters such as fractional anisotropy (FA) and mean diffusivity (MD). These metrics reflect the microstructural integrity within the white matter tracts. In SPMS, decreased FA values in regions such as the fornix and medial lemniscus have been correlated with cognitive impairment and disease progression, underscoring the clinical relevance of axonal integrity as revealed by advanced imaging techniques,
Figure 1 [
7].
- 7.
Visualization of Demyelination
Demyelination, the hallmark pathological feature of multiple sclerosis (MS), can be identified using both conventional MRI sequences and specialized imaging techniques. T2-weighted MRI sequences typically reveal hyperintense lesions that correspond to regions of demyelination, edema, and inflammation. While an increased lesion load is a common finding in RRMS, in SPMS, the lesions often become more diffuse and slowly expand rather than appear as new, discrete foci [
30]. In contrast, T1-weighted sequences may show hypointense lesions, known as “black holes”, which reflect areas of severe and often irreversible demyelination and axonal loss. These T1-hypointense lesions are strongly associated with clinical disability and cognitive impairment in patients with SPMS. Their volume and persistence over time are indicative of poor prognosis [
26].
- 8.
Visualization of Chronic Lesions
Chronic lesions, especially SELs, are predominant features of SPMS and reflect the presence of ongoing low-grade inflammation and neurodegeneration. SELs are visualized on MRI as lesions with persistent, gradually expanding borders that evolve over the years, indicating continuous demyelination and axonal injury. These lesions are strongly associated with clinical progression, often independent of new inflammatory activity [
30]. Leptomeningeal enhancement (LME), which can be detected using post-contrast fluid-attenuated inversion recovery (FLAIR) sequences, serves as a marker of chronic meningeal inflammation. The presence of LME correlates with cortical demyelination and neurodegeneration, particularly in progressive forms of MS [
31].
4.6. Importance of Early MRI Detection for Patient Outcomes
Early detection of multiple sclerosis (MS) progression from the RRMS to SPMS using MRI plays a critical role in improving clinical outcomes and patients’ quality of life. Timely recognition of subtle pathological changes using advanced MRI techniques can significantly influence disease management, therapeutic decision-making, and prognosis, potentially reducing the burden of long-term disability.
MRI allows clinicians to identify patients at a higher risk of rapid progression even before the pronounced clinical manifestations. Specific MRI features, such as increased brain atrophy rates, higher lesion burden, and the presence of SELs, are critical indicators for predicting early progression to SPMS [
6,
30]. Notably, Koch et al. found that brain volume loss, especially involving gray matter, strongly correlates with physical disability and cognitive impairment, emphasizing its value as an early prognostic indicator [
6].
- 2.
Improved Therapeutic Strategies and Timely Interventions.
Early MRI detection facilitates timely therapeutic interventions, which are crucial for modifying disease progression. Identifying patients with progressive neurodegeneration allows clinicians to proactively adjust treatments, potentially delaying or preventing severe disability. For instance, the early identification of subpial demyelination or leptomeningeal inflammation, detectable through advanced MRI sequences, may guide more aggressive therapeutic strategies, including the early initiation of disease-modifying therapies (DMTs) or neuroprotective agents [
30,
31].
- 3.
Prevention or Delay of Cognitive Decline.
Early identification of MRI markers for cognitive impairment significantly enhances patient management. Progressive MS is frequently associated with substantial cognitive deficits that profoundly affect the quality of life, employment status, and social functioning. Advanced MRI techniques, such as diffusion tensor imaging (DTI), allow the detection of microstructural alterations in critical white matter tracts linked to cognition (e.g., the corpus callosum and fornix). As Mistri et al. emphasized, abnormalities in fractional anisotropy (FA) within these structures strongly correlate with cognitive impairment. Detecting these MRI biomarkers early enables tailored cognitive rehabilitation and targeted pharmacological interventions, enhancing cognitive outcomes and preserving the quality of life [
7].
- 4.
Enhanced Monitoring of Disease Activity and Treatment Efficacy.
MRI plays a crucial role in the objective monitoring of disease activity and evaluation of treatment efficacy. Through regular MRI assessments, clinicians can detect subclinical disease activity and inform therapeutic decisions. Filippi et al. highlighted the importance of imaging biomarkers, like new T2 lesions or gadolinium-enhancing lesions, as indicators of ongoing inflammatory activity. Furthermore, monitoring atrophy rates provides insight into neurodegenerative progression, allowing clinicians to evaluate the effectiveness of neuroprotective therapies and adjust treatments accordingly [
30].
- 5.
Prognostication and Patient Counseling.
Early detection of progressive MRI features enables accurate prognostication, facilitating informed discussions between clinicians and patients regarding the expected disease trajectory and outcomes. A clear MRI-based understanding of disease status empowers patients by setting realistic expectations, guiding lifestyle adaptations, and optimizing psychological preparedness for potential disease progression. Koch et al. found correlations between MRI features, including lesion burden and brain atrophy, and significant clinical outcomes, underscoring their importance in patient counseling and management [
6].
- 6.
Economic and Social Implications.
Early and accurate detection using MRI can significantly impact healthcare resource utilization and societal costs associated with MS. By delaying the progression of disability, patients maintain higher functional independence, reducing direct healthcare costs (e.g., hospitalization and supportive care) and indirect costs (e.g., loss of productivity and caregiver burden). Thus, early identification of at-risk patients through MRI-based assessments yields substantial economic benefits alongside improved patient outcomes [
30].
4.7. Imaging Biomarkers in SPMS
MRI has become an indispensable tool for the diagnosis, monitoring, and prognostication of multiple sclerosis (MS). In the context of SPMS, where neurodegeneration gradually overtakes inflammatory activity, the role of MRI extends far beyond the detection of active lesions. Instead, it facilitates the visualization of chronic pathological processes—many of which may not be clinically apparent until substantial disability has accumulated. As such, MRI biomarkers are increasingly used to characterize the underlying tissue damage that drives irreversible neurological decline in patients with SPMS [
4,
5,
6]. Several classes of MRI biomarkers are now recognized for their relevance to SPMS. Structural MRI remains foundational, with T2-weighted imaging used to quantify the total lesion burden and T1-weighted imaging revealing hypointense “black holes” that correspond to areas of severe axonal loss. These traditional measures are useful for tracking the long-term disease burden, although they lack specificity for progressive pathology. In SPMS, progressive brain atrophy—particularly of the cortical gray matter and deep gray matter nuclei such as the thalamus—has emerged as a highly predictive marker of sustained disability. Cortical thinning and regional atrophy strongly correlate with both physical impairment and cognitive decline, often preceding visible clinical deterioration [
6,
9]. Recently, advanced imaging biomarkers have become the focus of SPMS research and clinical practice. SELs, which represent chronically active white matter plaques with ongoing inflammation at their margins, are now considered the hallmarks of smoldering disease activity. These lesions typically lack gadolinium enhancement but show peripheral expansion over time on follow-up imaging, reflecting the persistent microglial activation and progressive demyelination. Their presence is significantly associated with future disability and brain volume loss [
4,
17]. Similarly, iron rim lesions—characterized by paramagnetic borders visible on susceptibility-weighted imaging (SWI) or quantitative susceptibility mapping (QSM)—are indicative of iron-laden activated microglia and macrophages. These lesions offer a promising window into compartmentalized inflammation and correlate with aggressive disease progression [
18,
32]. Quantitative approaches have also refined the characterization of lesions. The concept of atrophied lesion volume (ALV), which refers to the transformation of demyelinated lesions into cerebrospinal fluid-filled cavities, offers a biomarker for irreversible tissue destruction. ALV has shown stronger correlations with clinical disability than lesion counts alone and provides a clearer index of cumulative neurodegeneration [
8]. In addition to structural imaging, several microstructural and metabolic MRI techniques have been integrated into SPMS evaluation. Diffusion tensor imaging (DTI) assesses the integrity of white matter tracts by measuring the diffusion of water molecules. Reductions in fractional anisotropy (FA) and elevations in mean diffusivity (MD) are indicative of axonal loss and have been linked to both motor and cognitive deficits [
7,
33]. Magnetization transfer imaging (MTI) quantifies the interaction between macromolecules and water protons, thereby reflecting myelin density. Decreased magnetization transfer ratios (MTR) have been observed in both lesions and normal-appearing brain tissue in SPMS, suggesting a more diffuse pathology than that visible on standard scans [
18,
34]. Magnetic resonance spectroscopy (MRS) provides metabolic insights and reveals changes in brain biochemistry that parallel clinical decline. For example, reduced levels of N-acetyl aspartate (NAA), a marker of neuronal integrity, and elevated choline, associated with membrane turnover, have been observed in patients with SPMS and correlate with disease severity (
Table 2) [
34].
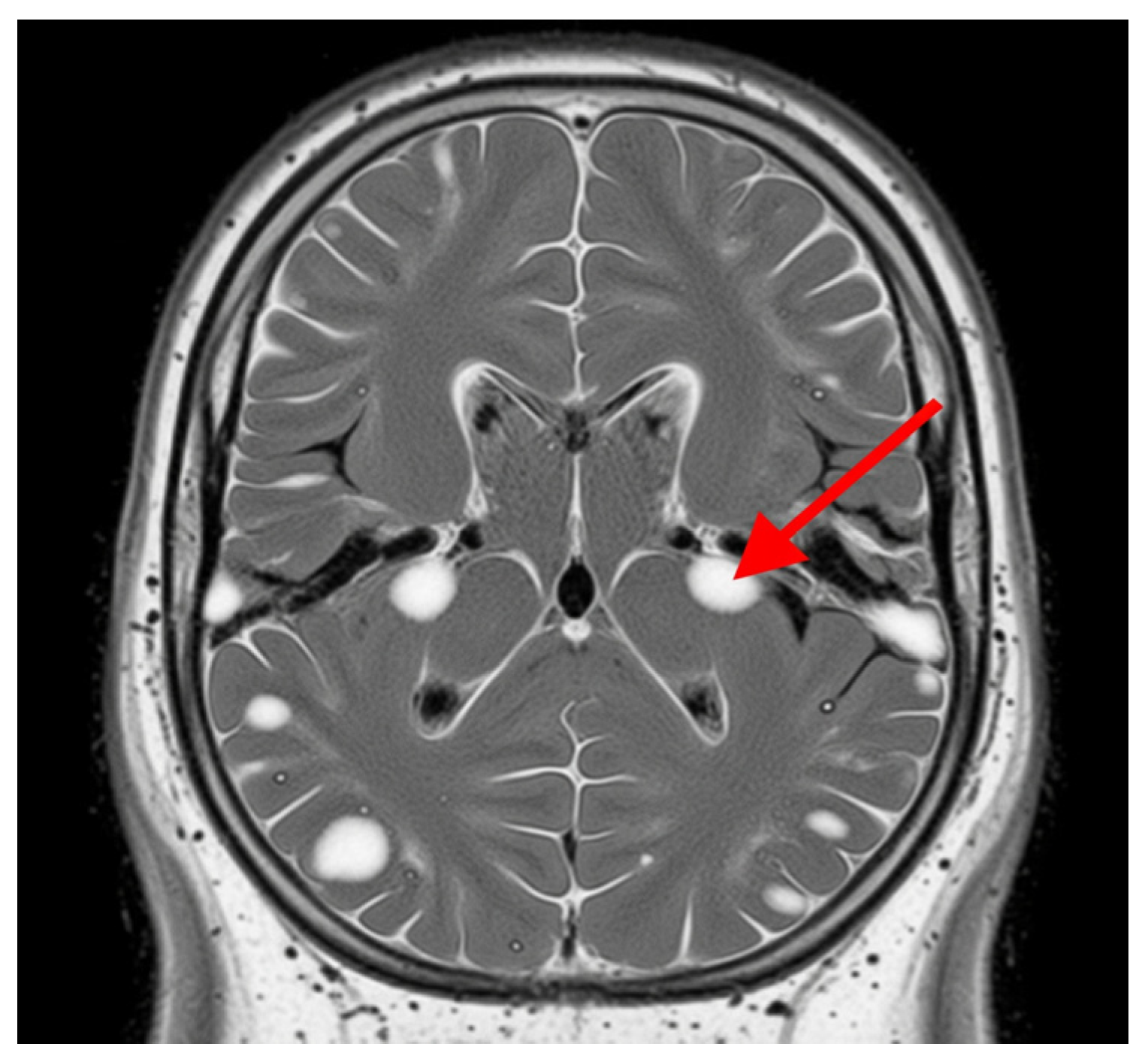
4.8. MRI Lesion Types in SPMS
In SPMS, MRI is an essential tool for characterizing disease progression by identifying and monitoring white matter lesions. These lesions typically manifest as hyperintense areas on T2-weighted MRI scans, representing areas of demyelination, axonal loss, and gliosis. T2 hyperintense lesions are a hallmark of multiple sclerosis and serve as critical biomarkers for evaluating disease burden and progression.
White matter lesions in SPMS are characterized by their initial presentation as active lesions that may be enhanced with gadolinium contrast on T1-weighted imaging, indicating blood-brain barrier disruption and acute inflammatory activity. However, over time, these active lesions typically transition into chronic demyelinated plaques, identifiable as non-enhancing stable lesions that persistently appear hyperintense on T2-weighted MRI and hypointense on T1-weighted MRI [
35].
Chronic white matter lesions in SPMS can become (SELs), which represent a significant proportion of the total lesion volume and are specifically associated with progressive neurological disability. SELs exhibit gradual expansion without evidence of acute inflammatory activity, such as gadolinium enhancement, and their volume is strongly correlated with clinical deterioration, as measured by the Expanded Disability Status Scale (EDSS) and other functional assessments [
35].
Histopathologically, chronic lesions often display ongoing neurodegeneration and axonal loss despite the absence of marked inflammation. This suggests that the pathology underlying these chronic lesions includes mechanisms independent of acute inflammatory processes, potentially involving innate immune system activation, neurodegenerative processes, and persistent tissue damage mediated by activated microglia and macrophages [
36].
Moreover, the accumulation of white matter lesion volume has been consistently correlated with increasing levels of physical disability in patients with SPMS. Higher lesion loads are indicative of more severe neurological deficits and predict worse clinical outcomes [
37].
Advanced MRI techniques have enhanced the capacity to identify and characterize these lesions, providing valuable insights into their evolution and their relationship with clinical outcomes. The persistent and expanding nature of white matter lesions highlights their central role in SPMS pathophysiology and underscores the importance of longitudinal MRI studies for monitoring disease progression and therapeutic response,
Figure 2 [
38].
- 2.
Gray Matter Lesions.
Gray matter (GM) lesions, particularly in the cortical and subcortical regions, significantly contribute to the pathology of SPMS, presenting distinctive challenges for detection and clinical interpretation.
Importance of cortical and subcortical gray matter involvement.
Gray matter atrophy, particularly affecting the cortical gray matter (cGM) and deep gray matter structures like the thalamus, is strongly linked to disability accumulation and cognitive decline in patients with SPMS. Studies such as Arnold et al. have demonstrated that cortical gray matter and thalamic volume loss correlate significantly with the progression of neurodegeneration, independent of inflammatory lesions typical of relapsing forms of the disease. These changes reflect the ongoing neurodegenerative processes that dominate the pathology in the progressive stages of MS beyond the inflammation-driven damage observed in relapsing MS [
9].
Involvement of the cortical regions and thalamus not only correlates with physical disability but also cognitive impairment, highlighting their prognostic significance in SPMS. Specifically, cortical atrophy is associated with a progressive decline in cognitive functions, such as processing speed and executive functions [
39]. Furthermore, resting-state functional connectivity studies have emphasized the role of gray matter changes in altering brain network dynamics, further contributing to cognitive and motor impairments [
17].
Gray matter lesions present unique challenges due to their subtle appearance on conventional MRI techniques. Traditional T2-weighted MRI, which is effective in detecting white matter lesions, is less sensitive to gray matter pathology, thus underestimating its true extent. Advanced imaging techniques, such as Magnetization Transfer Ratio (MTR), Double Inversion Recovery (DIR), and quantitative susceptibility mapping (QSM), enhance the detection and quantification of gray matter lesions. The MTR technique, for instance, has been instrumental in revealing myelin integrity changes in normal-appearing brain tissues (NABT), including cGM and normal-appearing white matter (NAWM), which are not visible on standard MRI scans [
9].
Additionally, susceptibility-based imaging methods have been increasingly used to detect cortical lesions characterized by chronic iron-containing inflammatory rims, which are significant markers of ongoing inflammation and neurodegeneration [
32]. Despite these advancements, the accurate detection and consistent quantification of gray matter lesions in clinical practice remain challenging due to the subtlety of pathological changes, technical variability between MRI scanners, and the need for specialized imaging protocols that are not universally available or standardized across clinical settings [
18].
Thus, while cortical and subcortical gray matter involvement has emerged as a critical aspect of SPMS pathology, necessitating sensitive imaging modalities for accurate detection, considerable efforts are still required to standardize these advanced imaging techniques for routine clinical applications.
- 3.
Iron Deposition.
Iron deposition, particularly in deep gray matter structures, is increasingly recognized as an important pathological feature of SPMS, reflecting chronic inflammation and neurodegeneration. Advanced MRI techniques, such as Susceptibility Weighted Imaging (SWI) and Quantitative Susceptibility Mapping (QSM), have significantly enhanced the visualization and understanding of iron accumulation in these brain regions.
Iron accumulation is commonly observed within the basal ganglia, thalamus, and at the rims of chronic active lesions and correlates strongly with disease severity and progression in SPMS [
32]. SWI effectively detects paramagnetic substances like iron, highlighting lesions with iron-containing inflammatory rims indicative of chronic microglial activation and ongoing tissue injury. QSM further refines this by providing quantitative measures of iron levels, facilitating precise monitoring of disease progression, and potentially predicting disability outcomes [
17].
These advanced imaging modalities are particularly useful in distinguishing chronic active lesions—characterized by persistent inflammation and iron-laden macrophages—from inactive lesions, thereby contributing significantly to prognosis and treatment strategies [
18]. Hence, incorporating iron-sensitive MRI techniques into routine clinical practice holds promise for more accurate assessment and management of SPMS.
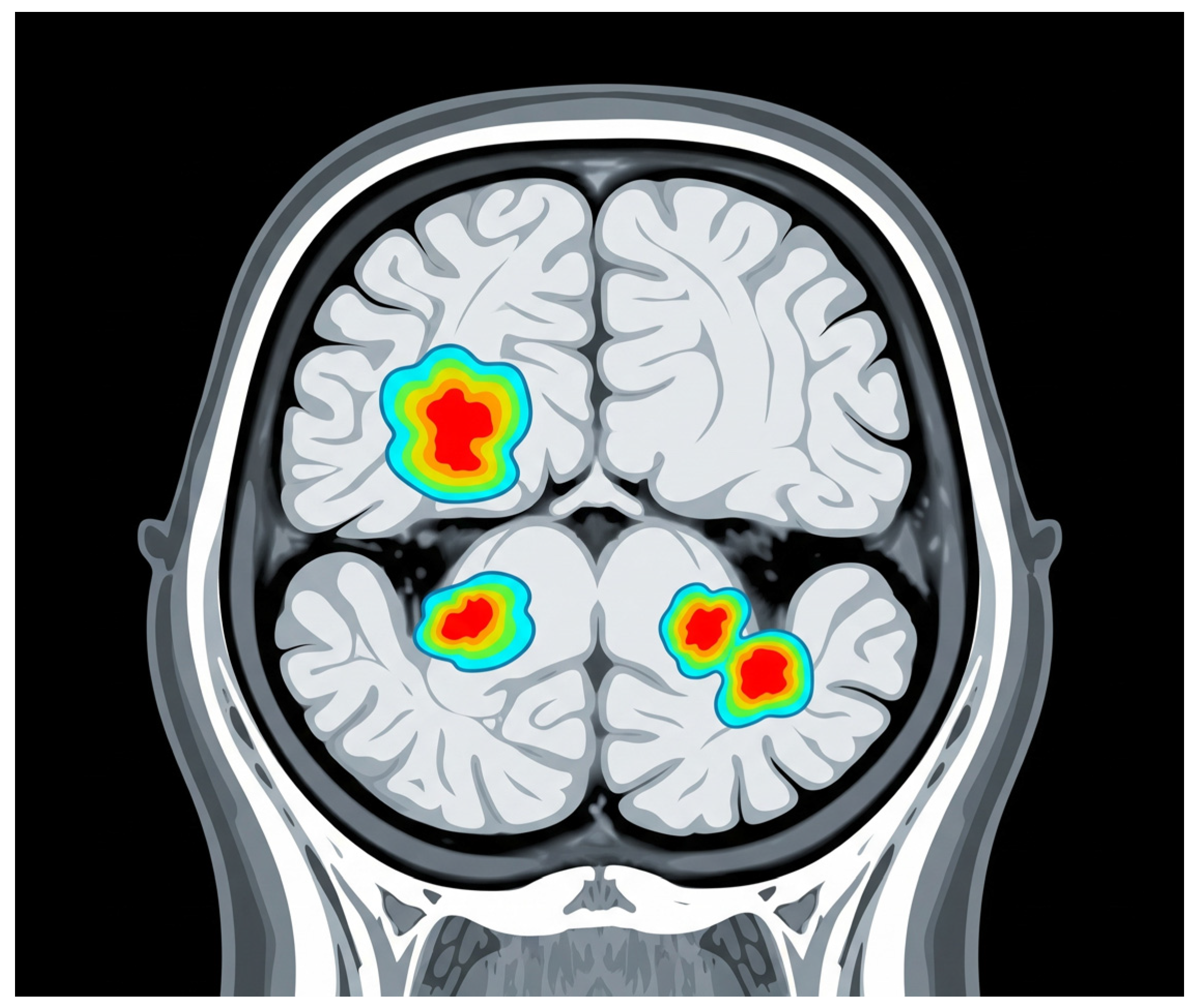
- 4.
Chronic Active Lesions (“Smoldering Lesions”).
Chronic active lesions, commonly termed “smoldering lesions”, are critical pathological hallmarks of SPMS. These lesions are characterized by a persistent inflammatory rim around their edges, which is distinctively visible on SWI. The appearance of these hypointense rims on SWI is primarily due to iron accumulation within activated microglia and macrophages, signifying ongoing inflammatory activity despite the absence of typical acute inflammatory episodes [
32].
The identification of rim lesions through advanced MRI techniques, particularly SWI, has significant clinical implications, as these lesions are strongly correlated with ongoing neurodegeneration and clinical progression. Studies have demonstrated that patients with a higher burden of chronic active lesions exhibit more pronounced disability accumulation and cognitive deterioration over time [
17,
18]. Absinta et al. further showed that lesions with paramagnetic rims (indicative of chronic active inflammation) tend to persist or even expand over the years, whereas rimless lesions gradually shrink—reinforcing the link between rimmed lesions and more aggressive disease progression [
19].
Consequently, smoldering lesions are gaining recognition not only as robust biomarkers for disease progression but also as potential targets for therapeutic intervention. Monitoring their presence and evolution through routine imaging could facilitate timely clinical decision-making and enhance prognostic precision, ultimately contributing to improved patient management in SPMS patients. Overall, these findings support the view that progressive MS is driven by smoldering pathology, prompting proposals for a new framework of MS progression based on underlying mechanisms rather than relapses alone,
Figure 3 [
40].
- 5.
Spinal Cord Lesions
Spinal cord lesions are frequent and clinically significant in SPMS, manifesting distinct patterns of involvement compared with other MS phenotypes. These lesions often correlate with substantial clinical impairment due to their critical anatomical localization. Spinal cord involvement, especially when extensive, frequently correlates with severe neurological deficits, including motor weakness, sensory disturbances, and autonomic dysfunctions [
18].
Clinically, the frequency and extent of spinal cord lesions tend to increase with disease progression and are notably more prevalent and severe in SPMS than in RRMS. This increased burden contributes significantly to disease progression and disability accumulation, reflecting the chronic neurodegenerative aspect characteristic of the secondary-progressive stage [
9].
The pathological hallmarks of spinal cord lesions in SPMS include a higher prevalence of diffuse demyelination, axonal loss, and gliosis, differentiating them from lesions predominantly seen in RRMS, which typically exhibit more pronounced inflammatory features and less extensive axonal degeneration [
33]. Moreover, the spinal cord lesions observed in SPMS frequently show persistent signal abnormalities on MRI without acute gadolinium enhancement, indicating chronic degenerative rather than active inflammatory processes [
17].
4.9. Advanced MRI Techniques in SPMS
Quantitative MRI techniques, including MTI, DTI, and Magnetic Resonance Spectroscopy (MRS), are pivotal in assessing microstructural damage in SPMS. These methods provide insights beyond those of conventional MRI, enabling detailed evaluations of disease progression.
MTI utilizes the exchange of magnetization between protons bound to macromolecules (such as myelin proteins and lipids) and those in the surrounding tissue water. The Magnetization Transfer Ratio (MTR) derived from MTI sequences specifically reflects myelin integrity, although it also correlates with axonal density. Decreased MTR values indicate demyelination and axonal loss, which are prominent in patients with SPMS [
36]. Furthermore, reduced MTR values in normal-appearing white and gray matter (NAWM, NAGM) are more pronounced in SPMS than in relapsing forms, highlighting the advanced microstructural pathology characteristic of SPMS [
33].
DTI measures the diffusion of water molecules in tissues and provides fractional anisotropy (FA) and mean diffusivity (MD) metrics, both of which are indicators of microstructural integrity. DTI studies have demonstrated increased MD and decreased FA values within lesions and normal-appearing brain tissues in SPMS, reflecting widespread demyelination and axonal degeneration. These changes are significantly correlated with neurological disability and cognitive decline, further emphasizing their clinical relevance [
38,
41].
MRS assesses brain metabolism by quantifying metabolites such as N-acetyl aspartate (NAA, a marker of neuronal integrity), choline (Cho, a marker of membrane turnover and myelin breakdown), creatine (Cr, a marker of gliosis), and myoinositol (mIn, a marker of astroglial activation). Reduced NAA and elevated Cho levels, frequently observed in SPMS, underscore persistent neuronal and myelin damage. These metabolic alterations correlate closely with disease severity, highlighting the potential of this technique as a sensitive biomarker for monitoring SPMS progression [
33].
- 2.
Functional MRI.
Functional MRI (fMRI) has emerged as a valuable tool for evaluating connectivity changes in SPMS, providing insights into the functional integrity and adaptability of neural networks as the disease progresses. While conventional MRI is crucial for diagnosing and monitoring structural lesions, fMRI allows for the assessment of functional changes, specifically alterations in resting-state functional connectivity (rsFC), highlighting subtle neural network disruptions that underlie clinical deterioration.
Recent studies employing multiparametric MRI have demonstrated the significance of functional connectivity in understanding cognitive impairment in patients with SPMS. Mistri et al. reported that cognitive dysfunction in SPMS is associated with structural abnormalities and white matter tract involvement, yet interestingly, resting-state functional connectivity did not significantly contribute to global cognitive functioning. This suggests that while structural integrity is critical for cognitive performance, functional connectivity changes may be subtler and require more targeted methods of analysis to detect significant clinical correlations [
7].
Other studies suggest a more nuanced relationship between functional MRI changes and clinical outcomes. For instance, Preziosa et al. highlighted that altered rsFC, particularly within frontal cortico-subcortical networks involving the dorsolateral prefrontal cortex, caudate nucleus, and thalamus, correlated with fatigue and dual-task performance impairment, which is common in progressive MS phenotypes. These findings underscore the involvement of frontal networks in mediating the functional deficits seen in SPMS, supporting the hypothesis that specific functional network disruptions underlie the distinct clinical symptoms [
17].
Furthermore, Gravesteijn et al. found preliminary evidence of a potential association between higher cardiorespiratory fitness levels and improved functional connectivity within the sensorimotor network, suggesting a protective or adaptive role of physical fitness in maintaining functional brain connectivity in patients with SPMS. This emphasizes the potential therapeutic implications of enhancing physical fitness as a strategy to mitigate functional connectivity disruptions and associated clinical decline in patients with SPMS [
42].
- 3.
Brain Atrophy Measurements.
Brain atrophy is a prominent feature of MS, and its patterns and clinical implications differ significantly between SPMS and RRMS patients. Advanced MRI techniques enable the precise quantification of these atrophic changes, offering insights into disease progression and severity.
In SPMS, widespread brain atrophy predominantly affects the cortical gray matter and deep gray matter structures, such as the thalamus, more extensively than in RRMS [
6]. Gray matter atrophy in SPMS is strongly correlated with disability progression, cognitive decline, and overall poor clinical outcomes [
33]. Cortical atrophy, in particular, is associated with pronounced cognitive impairment and disability, highlighting its utility as a prognostic indicator in patients with SPMS [
18].
Comparatively, RRMS exhibits more pronounced inflammatory activity, with lesions frequently showing gadolinium enhancement, while SPMS demonstrates greater neurodegenerative pathology. As RRMS transitions into SPMS, brain volume loss accelerates, becoming more diffuse and involving multiple cortical and subcortical areas, reflecting the neurodegenerative processes underlying SPMS [
9,
18].
Clinically, measurements of brain atrophy, including whole-brain, cortical, and deep gray matter volumes, have become critical endpoints in therapeutic trials and are recommended for routine clinical monitoring in patients with SPMS. Progressive atrophy predicts disability accumulation and cognitive dysfunction, emphasizing the need for therapies targeting neurodegeneration beyond inflammatory processes alone [
34].
- 4.
Emerging Modalities.
Emerging imaging techniques, such as PET-MRI and ultra-high-field MRI (7 Tesla, 7T MRI), have significantly advanced the visualization and understanding of MS pathology, particularly in the challenging diagnosis of SPMS.
PET-MRI integrates functional, structural, and metabolic data, enabling a detailed evaluation of inflammation and neurodegeneration in SPMS. Studies utilizing PET with radioligands like [11C]TMSX and [11C]PK11195 have revealed important insights into molecular alterations in both GM and NAWM. For instance, increased binding of [11C]TMSX to adenosine A2A receptors has been demonstrated in the NAWM of patients with SPMS, correlating strongly with disability [
43]. Additionally, PET imaging using [11C]PK11195, which binds specifically to the translocator protein (TSPO) expressed in activated microglia, has allowed the detection of diffuse inflammation in the NAWM and periplaque areas of patients with SPMS, thus revealing chronic inflammatory processes that conventional MRI fails to visualize [
44].
Furthermore, PET imaging techniques enable the study of synaptic density and neuronal integrity using advanced tracers such as [11C]UCB-J, highlighting the extent of synaptic loss and dysfunction in patients with SPMS. The utilization of PET-MRI in longitudinal studies promises to elucidate dynamic changes in neuroinflammation and neurodegeneration, contributing significantly to personalized therapeutic strategies and early intervention opportunities [
25].
The advent of ultra-high-field MRI at 7 Tesla (7T MRI) has notably improved the visualization of subtle pathological features, including cortical and subcortical GM lesions, which are challenging to detect at lower field strengths. 7T MRI enhances lesion detection sensitivity, especially in cortical areas, and reveals a significantly higher number of cortical lesions than conventional MRI techniques, providing crucial insights into cortical pathology, which is a significant factor in cognitive impairment and disability progression in SPMS [
45]. Specifically, 7T MRI can detect cortical lesions with greater spatial resolution, enabling better differentiation of lesion subtypes and detailed characterization of lesion morphology, including the presence of chronic active “smoldering” lesions with inflammatory rims containing iron.
Additionally, 7T MRI facilitates the detection of leptomeningeal inflammation, a pathological feature closely linked to cortical damage and neurodegeneration in SPMS, thus potentially guiding more precise therapeutic targets [
25].
Segmentation volumetry through advanced MRI analysis has emerged as a powerful tool for quantifying GM and WM volumes, which is crucial for monitoring SPMS progression. Volumetric segmentation helps identify atrophy patterns, which are particularly extensive in the cortical and deep GM areas during the progressive phase. This technique supports both clinical prognosis and therapeutic monitoring, offering precise and quantitative assessments of the severity of neurodegeneration [
25]. Accurate volumetric segmentation can differentiate subtle regional atrophy patterns, such as thalamic and hippocampal volume loss, which are strongly associated with cognitive decline and disability progression.
Moreover, longitudinal volumetric measurements enhance our understanding of the temporal dynamics of neurodegeneration and improve the predictive capability of MRI biomarkers for disease progression. Consequently, volumetric segmentation methods have become integral to clinical trials evaluating the effectiveness of neuroprotective therapies in SPMS.

 ,
, 

{kind=link}
{kind=link}
{kind=link}