
High-Complexity Questions and Their Answers for Everyday Heart Failure
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Ten Complex Key Questions About HF
3.1. Management of Recovered or Improved LVEF: Should Neurohormonal Treatment Be Continued?
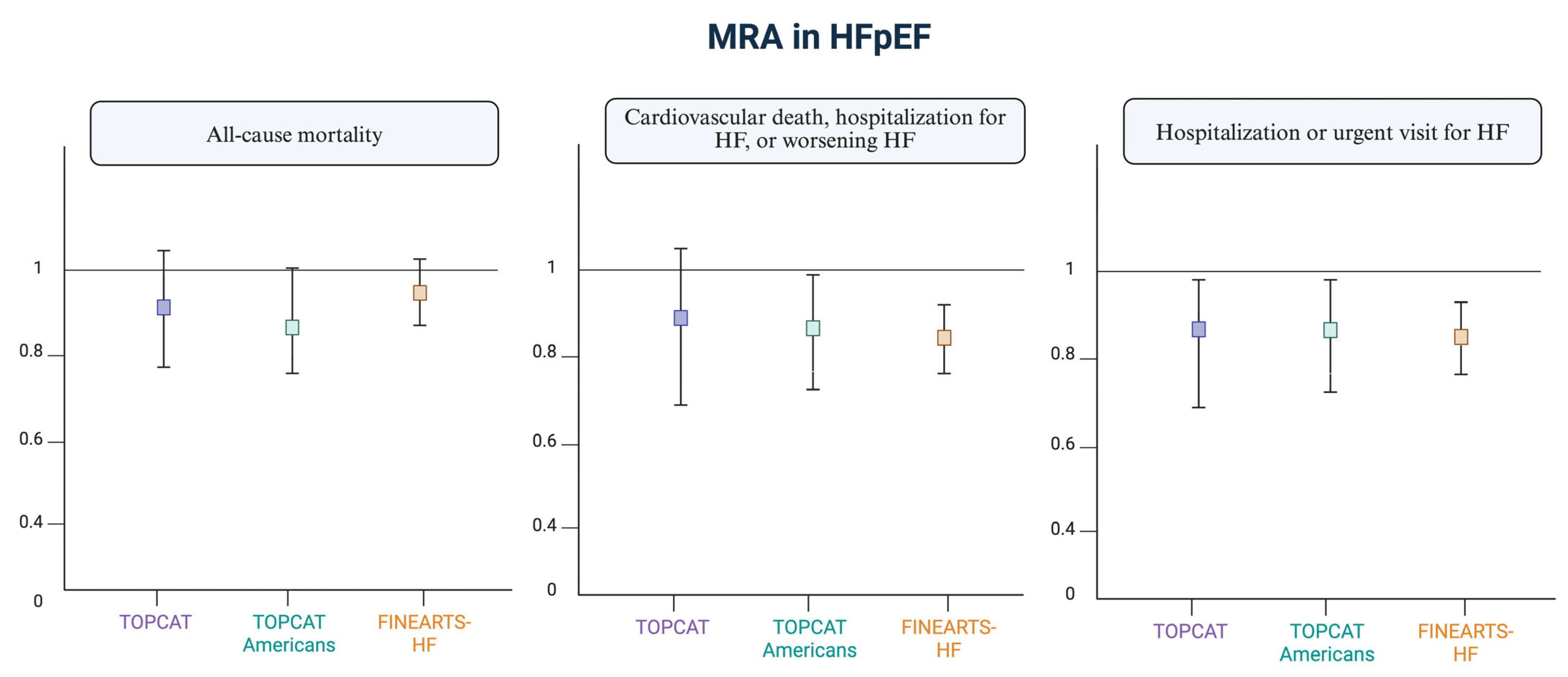
3.2. Mineralocorticoid Receptor Antagonists: Evidence and Dosage in Preserved Ejection Fraction HF
- Spironolactone: An initial dose of 12.5 mg/24 h, targeting 25–50 mg/24 h, provided there are no limitations due to hyperkalemia, renal impairment, or hypotension.
- Eplerenone: An initial dose of 25 mg/24 h, targeting 50 mg/24 h as tolerated.
- Finerenone: An initial dose of 20 mg/24 h, increased to 40 mg/24 h if the eGFR > 60 mL/min. If the eGFR is lower, start at 10 mg/24 h, increasing to 20 mg/24 h if tolerated.
- TOPCAT [3]: A clinical trial in which patients with symptomatic HF and LVEF of 45% or higher were randomly assigned to spironolactone vs. placebo. The study did not show statistical significance regarding mortality, but it did show significance for hospitalization due to HF. A subsequent subgroup analysis demonstrated statistical significance in the primary outcome (a combined event of cardiovascular death and hospitalization for HF) in the North American and Western European groups, but not in the Eastern European group. It also showed greater efficacy in patients with a LVEF < 60% and in women, where the reduction in events was similar across all EF ranges.
- FINEARTS [5,6,7]: The recent FINEARTS-HF study evaluated the effect of finerenone in HF with preserved or mildly reduced EF (EF ≥ 40%). Finerenone, compared to placebo, reduced the occurrence of the combined event of cardiovascular death and HF hospitalization. The dose was adjusted according to the patients’ eGFR according to the guidelines and the product label: → For patients with an eGFR > 60 mL/min/1.73 m2, treatment started with 20 mg daily, which could be increased to 40 mg if no adverse effects occurred. → For patients with an eGFR ≤ 60 mL/min/1.73 m2, treatment started with 10 mg daily, which could be increased to 20 mg if well tolerated. → For an eGFR < 25 mL/min/1.73 m2, the treatment was contraindicated. → This dosing regimen aimed to minimize the risk of hyperkalemia. The target dose was 20 mg daily, adjusted based on serum potassium levels after 4 weeks.
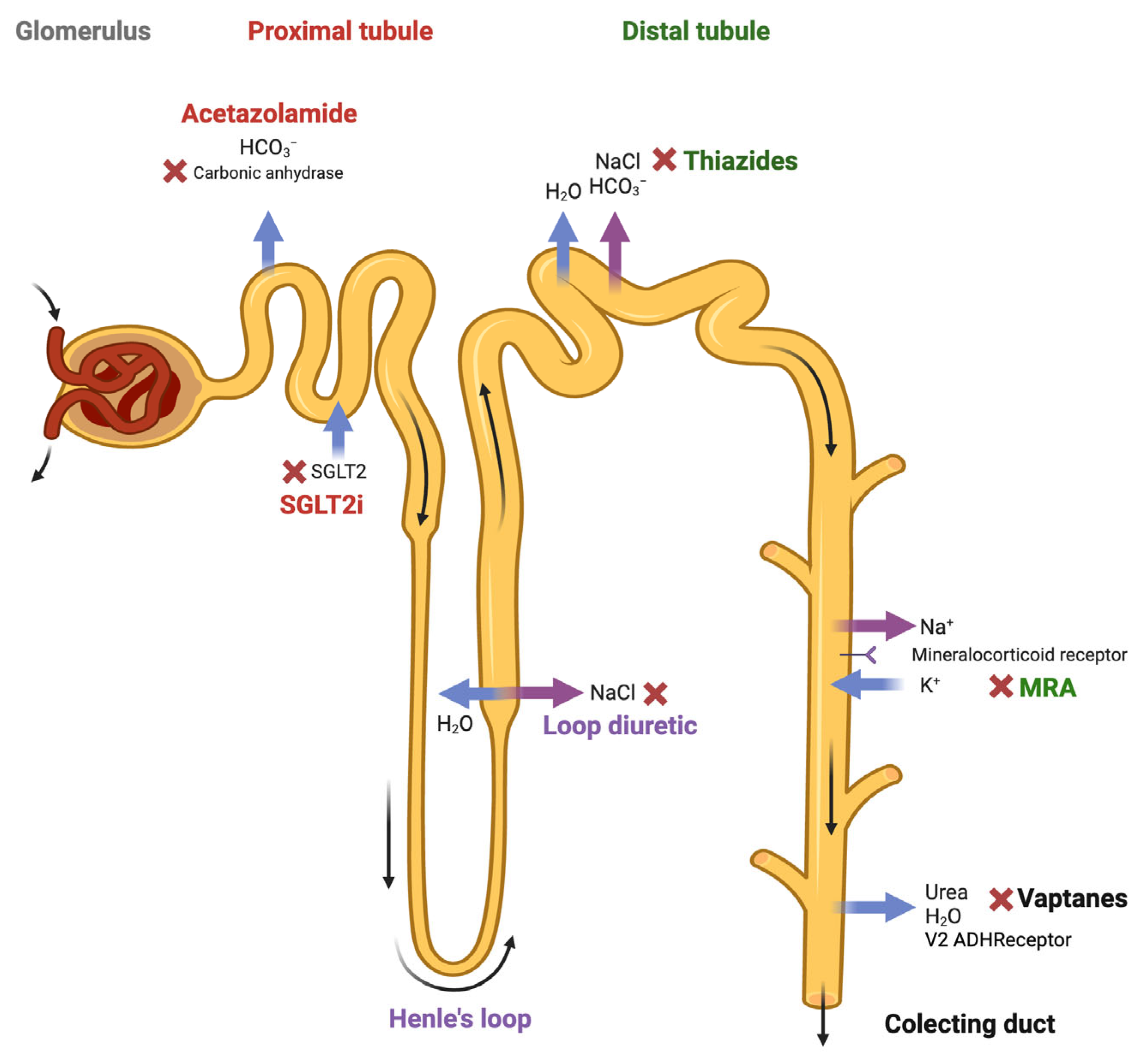
3.3. The Sequential Blockade of the Nephron: Permanent or Intermittent? What Are the Differences Between Hydrochlorothiazide and Chlorthalidone?
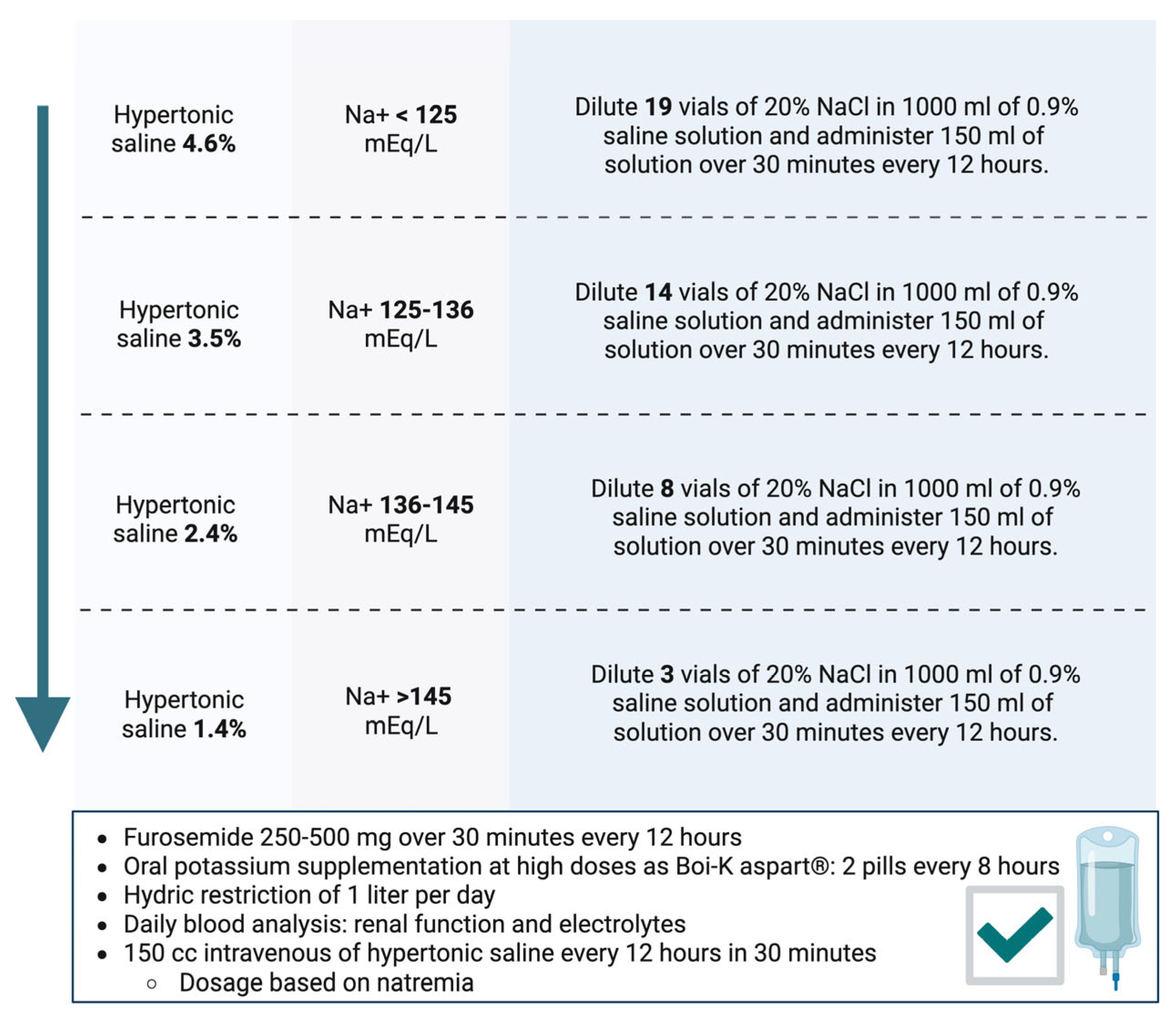
3.4. Hypertonic Saline: Evidence and Dosage
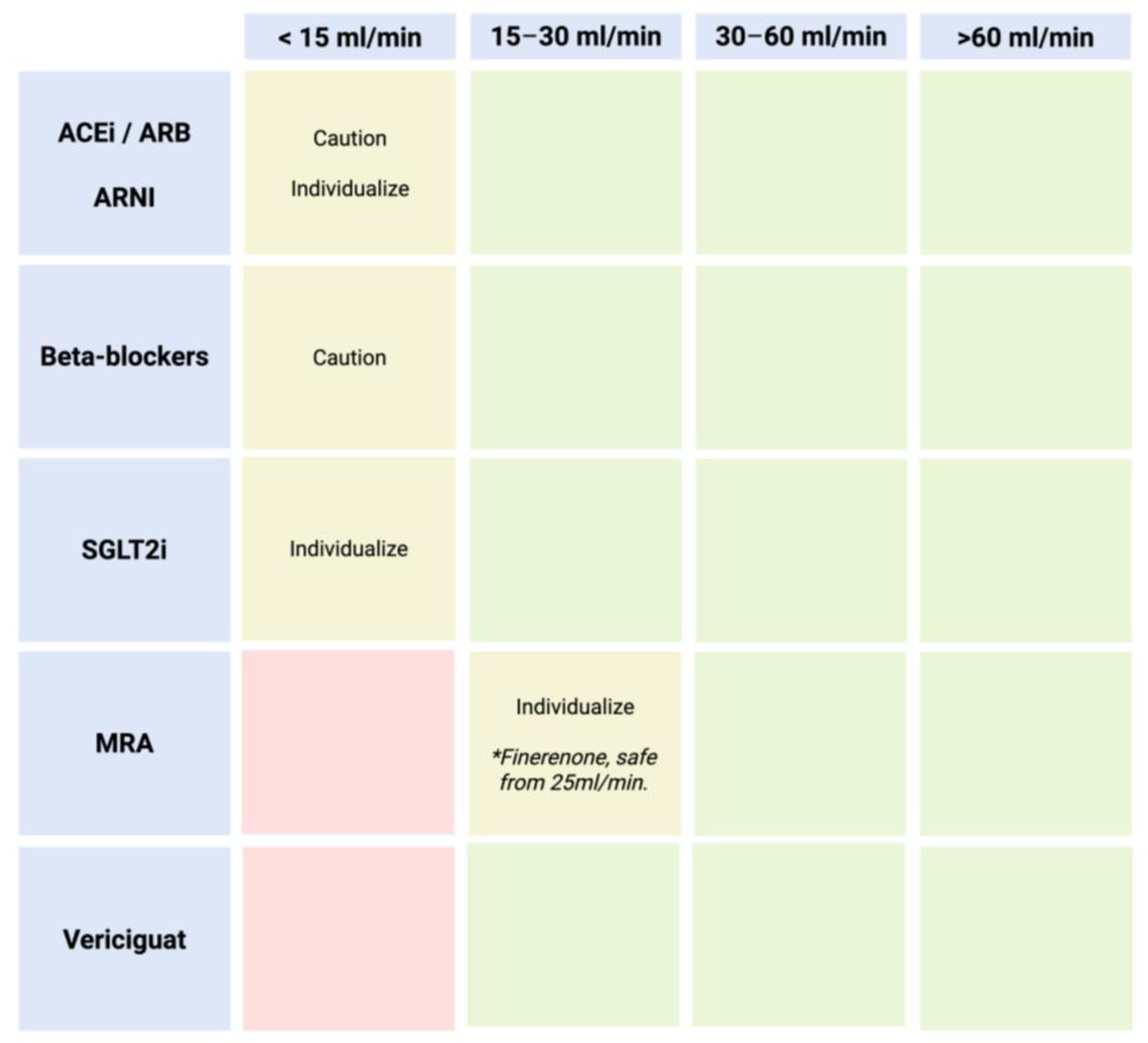
3.5. In a Cardiorenal Setting and in Patients with Low Glomerular Filtration, Should Disease-Modifying Drugs Be Discontinued?
- ACEi/ARBs/ARNIs: These are ideally used until an eGFR of 15 mL/min. Evidence supports their continuation even beyond this threshold on an individualized basis.
- SGLT2i: Indicated until an eGFR between 10 and 15 mL/min. For lower filtration rates, individualized treatment should be considered based on the patient’s clinical benefit.
- MRAs: These should be initiated with an eGFR ≥30 mL/min (except for finerenone: ≥25 mL/min) [25]. However, if the eGFR declines and potassium levels are within normal limits, they should be maintained, as they continue to improve prognosis. Regarding the initiation of these drugs, they are not recommended if the eGFR is below 30 mL/min/1.73 m2. It is important to note that this recommendation is based on the lack of clinical trials including patients with severe renal insufficiency. However, once started, a rise in serum creatinine up to 50% of baseline values is acceptable, as long as it is <266 μmol/L (3 mg/dL), and a reduction in eGFR of up to 10% from baseline is acceptable, as long as the eGFR remains >25 mL/min/1.73 m2.
- Beta-blockers: Similarly to other medications, there is no evidence for their use in patients with severe renal insufficiency (eGFR < 30 mL/min/1.73 m2). However, they should generally be maintained based on blood pressure and heart rate, as they have been shown to reduce mortality in moderate renal dysfunction (eGFR 45–59 mL/min/1.73 m2) as well as moderately severe renal dysfunction (eGFR 30–44 mL/min/1.73 m2).
- Vericiguat: Indicated until eGFR < 15 mL/min.
3.6. Beta-Blockers, Should They Be Discontinued in Acute Heart Failure?
3.7. Patients with Atrial Fibrillation and Heart Failure: Should I Opt for Digoxin or Beta-Blockers?
- In the clinical trial “RATE-AF” [32] (evaluation of treatment used for heart rate control in patients with symptomatic permanent AF), there were no differences between low-dose digoxin and bisoprolol in terms of quality of life scales at 6 months after initiating treatment. However, digoxin showed advantages in secondary outcomes: fewer adverse effects, fewer subjective symptoms (according to the NYHA scale), and a reduction in NT-proBNP.
- In the “ESC–EHRA EORP AF Long-Term General Registry” [33], the impact of using digoxin versus beta-blockers in AF patients was compared regarding quality of life, hospitalizations, and mortality. Higher mortality was observed with digoxin, not due to the drug itself but due to the baseline characteristics of the patients. No significant differences were found in terms of hospitalizations and quality of life.
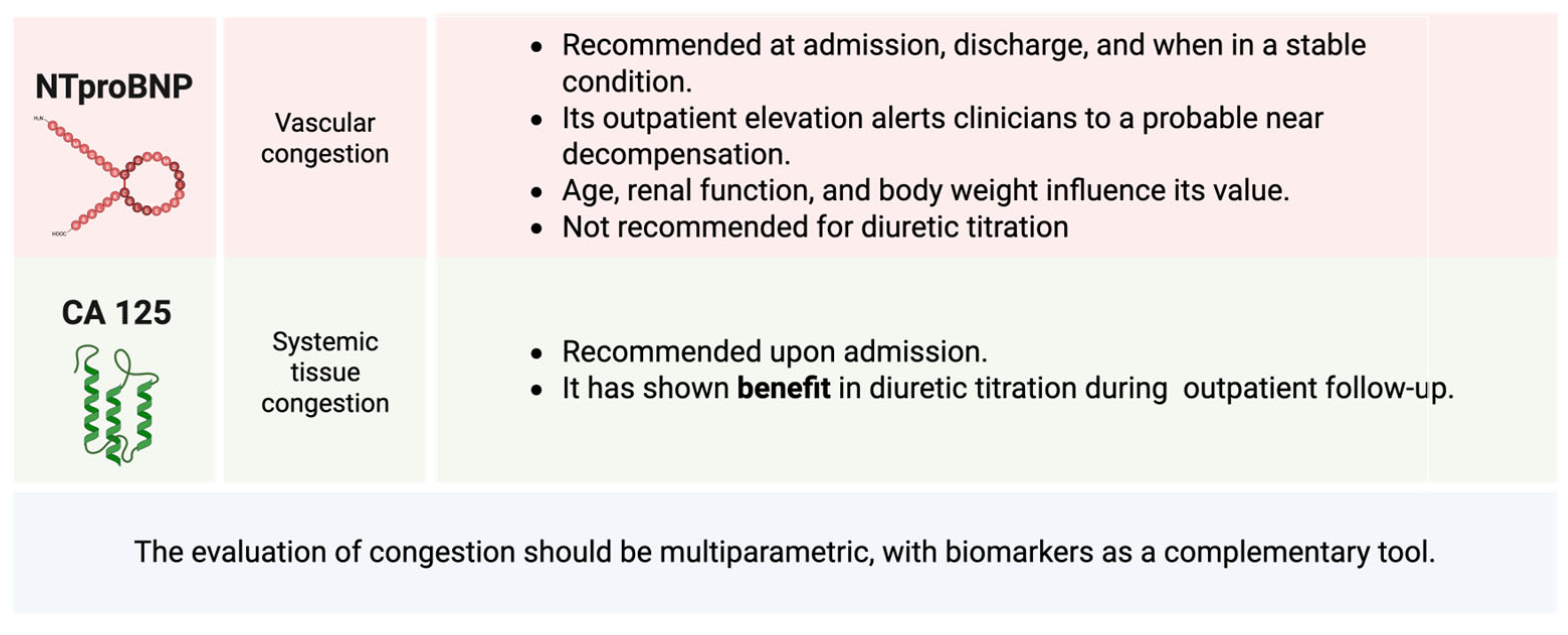
3.8. The Utility of Biomarkers for Pharmacological Titration: When Should They Be Repeated?
3.9. NTproBNP False Negatives: Does Obesity Really Influence Them?
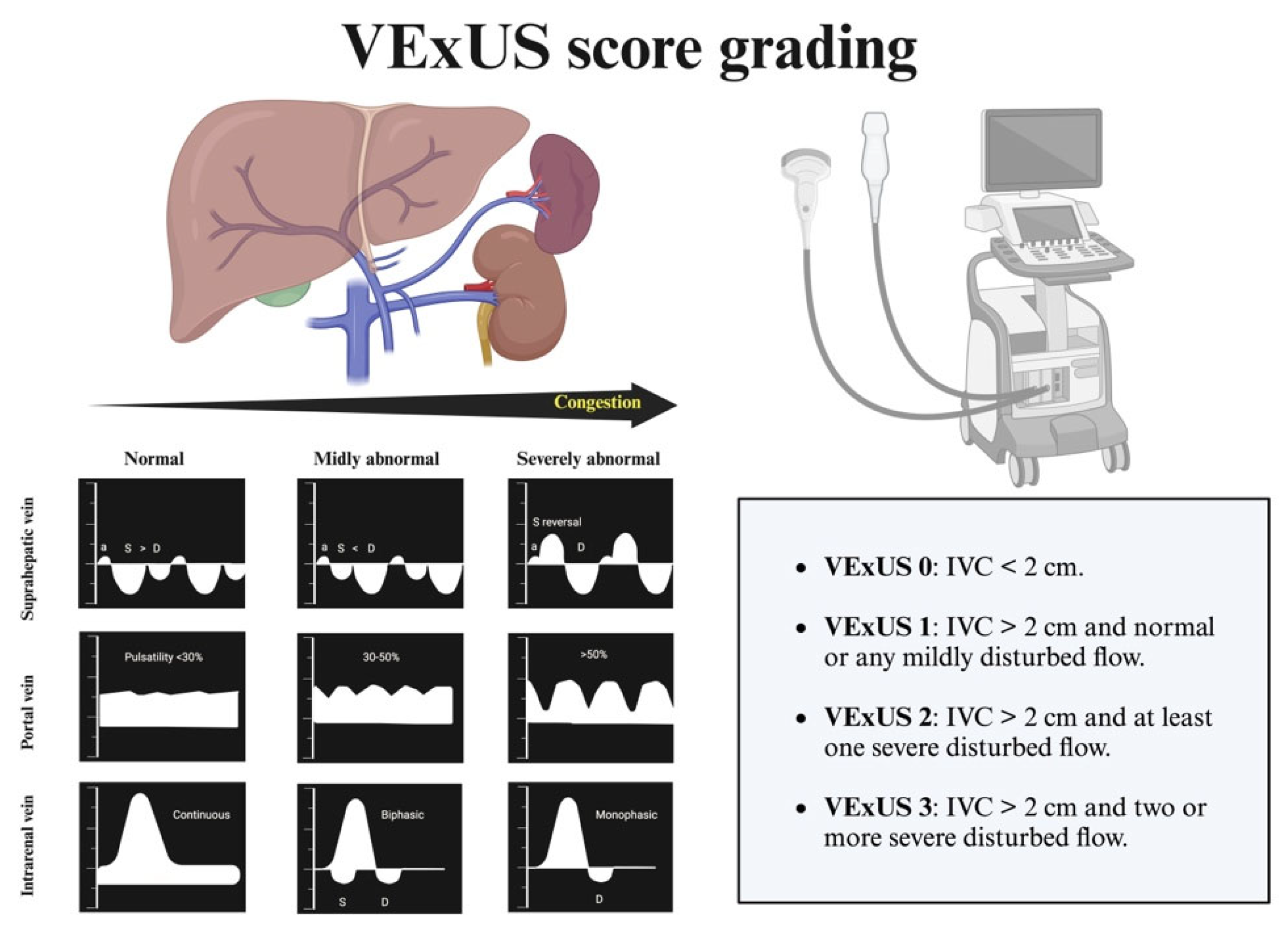
3.10. Clinical Echocardiography and Heart Failure: The Interpretation of Inferior Vena Cava Dimensions and the Role of VExUS in Patients with Suspected Pulmonary Hypertension
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEI | Angiotensin-converting enzyme inhibitor |
| AF | Atrial fibrillation |
| AHF | Acute heart failure |
| ARB | AngiotensinII receptor blocker |
| ARNI | Angiotensin–neprilysin receptor inhibitor |
| BMI | Body mass index |
| CA125 | Carbohydrate antigen 125 |
| CKD | Chronic kidney disease |
| CVRF | Cardiovascular risk factors |
| DM | Diabetes mellitus |
| eGFR | Estimated glomerular filtration rate |
| GLP-1 RA | Glucagon-like peptide-1 receptor agonist |
| HF | Heart failure |
| HSS | Hypertonic saline solution |
| IVC | Inferior vena cava |
| LVEF | Left ventricular ejection fraction |
| MRA | Mineralocorticoid receptor antagonist |
| mrLVEF | Moderately reduced left ventricular ejection fraction (40–50%) |
| NT-proBNP | N-terminal pro-brain natriuretic peptide |
| NYHA | New York Heart Association |
| pLVEF | Preserved left ventricular ejection fraction (>50%) |
| PH | Pulmonary hypertension |
| rLVEF | Reduced left ventricular ejection fraction (<40%) |
| SGLT2i | Sodium-glucose cotransporter-2 inhibitor |
| VExUS | Venous excess ultrasound protocol. |
References
- Wilcox, J.E.; Fang, J.C.; Margulies, K.B.; Mann, D.L. Heart failure with recovered left ventricular ejection fraction. J. Am. Coll. Cardiol. 2020, 76, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Halliday, B.P.; Wassall, R.; Lota, A.S.; Khalique, Z.; Gregson, J.; Newsome, S.; Jackson, R.; Rahneva, T.; Wage, R.; Smith, G.; et al. Withdrawal of pharmacological treatment for heart failure in patients with recovered dilated cardiomyopathy (TRED-HF): An open-label, pilot, randomised trial. Lancet 2018, 393, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone in heart failure with preserved ejection fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef]
- Pardo-Martínez, P.; Barge-Caballero, E.; Bouzas-Mosquera, A.; Barge-Caballero, G.; Couto-Mallón, D.; Paniagua-Martín, M.J.; Sagastagoitia-Fornie, M.; Prada-Delgado, Ó.; Muñiz, J.; Almenar-Bonet, L.; et al. Real world comparison of spironolactone and eplerenone in patients with heart failure. Eur. J. Intern. Med. 2022, 97, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.; Vaduganathan, M.; Claggett, B.; Jhund, P.S.; Desai, A.S.; Henderson, A.D.; Lam, C.S.; Pitt, B.; Senni, M.; et al. Finerenone in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2024, 391, 1475–1485. [Google Scholar] [CrossRef]
- Bonnesen, K.; Korsholm, K.; Andersen, A.; Pedersen, L.; Simonsen, C.Z.; Nielsen-Kudsk, J.E.; Schmidt, M. Risk of Ischemic Stroke After Patent Foramen Ovale Closure. JACC 2024, 84, 1424–1433. [Google Scholar] [CrossRef]
- Packer, M.; Zile, M.R.; Kramer, C.M.; Baum, S.J.; Litwin, S.E.; Menon, V.; Ge, J.; Weerakkody, G.J.; Ou, Y.; Bunck, M.C.; et al. Tirzepatide for Heart Failure with Preserved Ejection Fraction and Obesity. N. Engl. J. Med. 2025, 392, 427–437. [Google Scholar] [CrossRef]
- Pitt, B.; Filippatos, G.; Agarwal, R.; Anker, S.D.; Bakris, G.L.; Rossing, P.; Joseph, A.; Kolkhof, P.; Nowack, C.; FIGARO-DKD Investigators; et al. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 2252–2263. [Google Scholar] [CrossRef]
- Filippatos, G.; Anker, S.D.; Agarwal, R.; Pitt, B.; Ruilope, L.M.; Rossing, P. Finerenone and cardiovascular outcomes in patients with chronic kidney disease and type 2 diabetes. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- McDonagh, T.A. FINEARTS-HF—The Latest Masterpiece for MRAs in Heart Failure. N. Engl. J. Med. 2024, 391, 1540–1541. [Google Scholar] [CrossRef]
- Felker, G.M.; Ellison, D.H.; Mullens, W.; Cox, Z.L.; Testani, J.M. Diuretic Therapy for Patients With Heart Failure. J. Am. Coll. Cardiol. 2020, 75, 1178–1195. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.; Bates, D. Diuretic Strategies in Acute Decompensated Heart Failure: A Narrative Review. Can. J. Hosp. Pharm. 2024, 77, e3323. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trullàs, J.C.; Morales-Rull, J.L.; Casado, J.; Carrera-Izquierdo, M.; Sánchez-Marteles, M.; Conde-Martel, A.; Dávila-Ramos, M.F.; Llácer, P.; Salamanca-Bautista, P.; Pérez-Silvestre, J.; et al. Combining loop with thiazid22e diuretics for decompensated heart failure: The CLOROTIC trial. Eur. Heart J. 2023, 44, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Paterna, S.; Fasullo, S.; Cannizzaro, S.; Vitrano, G.; Terrazzino, G.; Maringhini, G.; Ganci, F.; Scalzo, S.; Di Pasquale, P.; Parrinello, G.; et al. Short-term effects of hypertonic saline solution in acute heart failure and long-term effects of a moderate sodium restriction in patients with compensated heart failure with New York Heart Association class III (Class C) (SMAC-HF Study). Am. J. Med. Sci. 2011, 342, 27–37. [Google Scholar] [CrossRef]
- Llàcer, P.; Romero, G.; Trullàs, J.C.; de la Espriella, R.; Cobo, M.; Quiroga, B.; Casado, J.; Slon-Roblero, M.F.; Morales, J.L.; Morgado, I.; et al. Consenso multidisciplinar sobre el manejo de la sobrecarga hidrosalina en insuficiencia cardiaca aguda. Recomendaciones SEMI/SEC/S.E.N. Rev. Esp. Cardiol. 2024, 77, 556–565. [Google Scholar] [CrossRef]
- Rodríguez, J.F.; Casado, J.; Formiga, F.; Gonzalez-Franco, A.; Arevalo, J.C.; Beltrán, M.; González, J.C.; Llacer, P.; Manzano, L.; Morales-Rull, J.L.; et al. Consensus on basic conduct during the hospital admission of patients with acute heart failure. Rev. Clin. Esp. 2021, 221, 283–296. [Google Scholar] [CrossRef]
- Murad, C.M.; Marcondes-Braga, F.G. Hypertonic saline solution: How, why, and for whom? ABC Heart Fail. Cardiomyopathy 2023, 3, e20230078. [Google Scholar] [CrossRef]
- Nguyen, D.V.; Le, T.N.; Truong, B.Q.; Nguyen, H.T.T. Efficacy and safety of angiotensin receptor–neprilysin inhibition in heart failure patients with end-stage kidney disease on maintenance dialysis: A systematic review and meta-analysis. Eur. J. Heart Fail. 2024, 27, 72–84. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Wheeler, D.C.; Stefánsson, B.V.; Jongs, N.; Postmus, D.; Correa-Rotter, R.; Chertow, G.M.; Hou, F.F.; Rossing, P.; Sjöström, C.D.; et al. Effects of Dapagliflozin in Patients with Kidney Disease, With and Without Heart Failure. JACC Heart Fail. 2021, 9, 807–820, Erratum in JACC Heart Fail. 2022, 10, 446–447. [Google Scholar] [CrossRef]
- E Díaz-Domínguez, M.; Fernández-Lucas, M.; Gomis-Couto, A.; Ruiz-Roso, G.; Teruel, J.L.; Quereda, C. Effects of suspending ACE inhibitors and ARBs in advanced chronic kidney disease. Nefrologia 2012, 32, 275–418. [Google Scholar] [CrossRef]
- Anker, S.; Butler, J.; Filippatos, G.; Marx, N.; Schnaidt, S.; Ofstad, A.; Ponikowski, P.; Pocock, S.; Zannad, F.; Packer, M. Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients with Heart Failure by Baseline Diabetes Status: Results from the EMPEROR-Reduced Trial. Circulation 2021, 143, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Solomon, S.D.; Claggett, B.; Diaz, R.; McMurray, J.J.V.; Metra, M.; Anand, I.; Crespo-Leiro, M.G.; Dahlström, U.; Goncalvesova, E.; et al. Assessment of Omecamtiv Mecarbil for the Treatment of Patients with Severe Heart Failure: A Post Hoc Analysis of Data From the GALACTIC-HF Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 26–34. [Google Scholar] [CrossRef]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; Ezekowitz, J.; Hernandez, A.F.; Butler, J.; Lam, C.S.; Ponikowski, P.; Voors, A.A.; Jia, G.; et al. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2020, 382, 1883–1893. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. Guía ESC 2021 sobre el diagnóstico y tratamiento de la insuficiencia cardiaca aguda y crónica. Rev. Esp. Cardiol. 2022, 75, 523.e1–523.e114. [Google Scholar] [CrossRef]
- Matsumoto, S.; Henderson, A.D.; Shen, L.; Yang, M.; Swedberg, K.; Vaduganathan, M.; van Veldhuisen, D.J.; Solomon, S.D.; Pitt, B.; Zannad, F.; et al. Mineralocorticoid Receptor Antagonists in Patients With Heart Failure and Impaired Renal Function. J. Am. Coll. Cardiol. 2024, 83, 2426–2436. [Google Scholar] [CrossRef] [PubMed]
- Psaty, B.M.; Koepsell, T.D.; Wagner, E.H.; LoGerfo, J.P.; Inui, T.S. The relative risk of incident coronary heart disease associated with recently stopping the use of beta-blockers. JAMA 1990, 263, 1653–1657. [Google Scholar] [CrossRef]
- Jondeau, G.; Neuder, Y.; Eicher, J.-C.; Jourdain, P.; Fauveau, E.; Galinier, M.; Jegou, A.; Bauer, F.; Trochu, J.N.; Bouzamondo, A.; et al. B-CONVINCED: Beta-blocker CONtinuation Vs. INterruption in patients with Congestive heart failure hospitalizED for a decompensation episode. Eur. Heart J. 2009, 30, 2186–2192. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Abraham, W.T.; Albert, N.M.; Stough, W.G.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B. Influence of beta-blocker continuation or withdrawal on outcomes in patients hospitalized with heart failure: Findings from the OPTIMIZE-HF program. J. Am. Coll. Cardiol. 2008, 52, 190–199. [Google Scholar] [CrossRef]
- A Gattis, W.; O’connor, C.M.; Leimberger, J.D.; Felker, G.; Adams, K.F.; Gheorghiade, M. Clinical outcomes in patients on beta-blocker therapy admitted with worsening chronic heart failure. Am. J. Cardiol. 2003, 91, 169–174. [Google Scholar] [CrossRef]
- Srivastava, P.K.; DeVore, A.D.; Hellkamp, A.S.; Thomas, L.; Albert, N.M.; Butler, J.; Patterson, J.H.; Spertus, J.A.; Williams, F.B.; Duffy, C.I.; et al. Heart Failure Hospitalization and Guideline-Directed Prescribing Patterns Among Heart Failure With Reduced Ejection Fraction Patients. JACC Heart Fail. 2021, 9, 28–38. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.; De Potter, T.J.; Dwight, J.; Guasti, L.; Hanke, T.; et al. ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Bunting, K.V.; Gill, S.K.; Mehta, S.; Stanbury, M.; Jones, J.C.; Haynes, S.; Calvert, M.J.; Deeks, J.J.; Steeds, R.P.; et al. Effect of Digoxin vs Bisoprolol for Heart Rate Control in Atrial Fibrillation on Patient-Reported Quality of Life: The RATE-AF Randomized Clinical Trial. JAMA 2020, 324, 2497–2508. [Google Scholar] [CrossRef] [PubMed]
- Ding, W.Y.; Boriani, G.; Marin, F.; Blomström-Lundqvist, C.; Potpara, T.S.; Fauchier, L.; Lip, G.Y. Outcomes of digoxin vs. beta blocker in atrial fibrillation: Report from ESC–EHRA EORP AF Long-Term General Registry. Eur. Heart J.-Cardiovasc. Pharmacother. 2022, 8, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, E895–E1032. [Google Scholar] [CrossRef] [PubMed]
- Anguita, M.; Bayés-Genís, A.; Cepeda, J.M.; Cinza, S.; Cosín, J.; Crespo, M.; Egocheaga, I.; Escobar, C.; Faraudo, M.; García-Pinilla, J.M.; et al. Consenso de expertos sobre la insuficiencia cardíaca aguda. Rev. Esp. Cardiol. 2020, 73, 69–77. [Google Scholar]
- Mueller, C.; McDonald, K.; de Boer, R.A.; Maisel, A.; Cleland, J.G.; Kozhuharov, N.; Coats, A.J.; Metra, M.; Mebazaa, A.; Ruschitzka, F.; et al. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur. J. Heart Fail. 2019, 21, 715–731. [Google Scholar] [CrossRef]
- Anguita, M.; Recio, A.; Castro, A.; García-Pinilla, J.M.; Cobos, M.; Núnez, J.; Peira, J.R.; Torres, J.; Vila, J.; Villar, S.; et al. Descompensaciones en Pacientes con Insuficiencia Cardíaca: Más allá de las guías. Sociedad Española de Cardiología. 2022. Available online: https://secardiologia.es/images/publicaciones/libros/descompensaciones-en-pacientes-con-IC-mas-alla-de-las-guias.pdf (accessed on 2 May 2025).
- Mebazaa, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; A Voors, A.; et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet 2022, 400, 1938–1952. [Google Scholar] [CrossRef]
- de la Espriella, R.; Santas, E.; Zegri Reiriz, I.; Górriz, J.L.; Cobo Marcos, M.; Núñez, J. Quantification and Treatment of Congestion in Heart Failure: A Clinical and Pathophysiological Overview. Nefrología (Engl. Ed.) 2022, 42, 145–162. [Google Scholar] [CrossRef]
- Núñez, J.; de la Espriella, R.; Miñana, G.; Santas, E.; Llácer, P.; Núñez, E.; Palau, P.; Bodí, V.; Chorro, F.J.; Sanchis, J.; et al. Antigen carbohydrate 125 as a biomarker in heart failure: A narrative review. Eur. J. Heart Fail. 2021, 23, 1445–1457. [Google Scholar] [CrossRef]
- Núñez, J.; Llàcer, P.; García-Blas, S.; Bonanad, C.; Ventura, S.; Núñez, J.M.; Sánchez, R.; Fácila, L.; de la Espriella, R.; Vaquer, J.M.; et al. CA125-Guided Diuretic Treatment Versus Usual Care in Patients With Acute Heart Failure and Renal Dysfunction. Am. J. Med. 2020, 133, 370–380.e4. [Google Scholar] [CrossRef]
- García-Blas, S.; Bonanad, C.; Llàcer, P.; Ventura, S.; Núñez, J.M.; Sánchez, R.; Chamorro, C.; Fácila, L.; de la Espriella, R.; Vaquer, J.M.; et al. Diuretic Strategies in Acute Heart Failure and Renal Dysfunction: Conventional vs Carbohydrate Antigen 125-guided Strategy. Clinical Trial Design. Rev. Esp. Cardiol. 2017, 70, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J. BNP: Biomarker Not Perfect in heart failure with preserved ejection fraction. Eur. Heart J. 2022, 43, 1952–1954. [Google Scholar] [CrossRef]
- Krauser, D.G.; Lloyd-Jones, D.M.; Chae, C.U.; Cameron, R.; Anwaruddin, S.; Baggish, A.L.; Chen, A.; Tung, R.; Januzzi, J.L. Effect of body mass index on natriuretic peptide levels in patients with acute congestive heart failure: A ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) substudy. Am. Heart J. 2005, 149, 744–750. [Google Scholar] [CrossRef]
- Kozhuharov, N.; Martin, J.; Wussler, D.; Lopez-Ayala, P.; Belkin, M.; Strebel, I.; Flores, D.; Diebold, M.; Shrestha, S.; Nowak, A.; et al. Clinical effect of obesity on N-terminal pro-B-type natriuretic peptide cut-off concentrations for the diagnosis of acute heart failure. Eur. J. Heart Fail. 2022, 24, 1545–1554. [Google Scholar] [CrossRef]
- Torres Macho, J.; Garcia de Casasola, G.; Grupo de Trabajo de Ecografía Clínica, Sociedad Española de Medicina Interna. Ecocardiografía clínica en Medicina Interna [Echocardiography in internal medicine]. Med. Clin. 2012, 12, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying systemic congestion with Point-Of-Care ultrasound: Development of the venous excess ultrasound grading system. Ultrasound J. 2020, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Beigel, R.; Cercek, B.; Luo, H.; Siegel, R.J. Noninvasive evaluation of right atrial pressure. J. Am. Soc. Echocardiogr. 2013, 26, 1033–1042. [Google Scholar] [CrossRef]
- Khan, A.A.; Saeed, H.; Haque, I.U.; Iqbal, A.; Du, D.; Koratala, A. Point-of-care ultrasonography spotlight: Could venous excess ultrasound serve as a shared language for internists and intensivists? World J. Crit. Care Med. 2024, 13, 93206. [Google Scholar] [CrossRef]
- de la Flor Merino, J.; Vaca Gallardo, M.; Rivera Gorrín, M. Score VEXUS (Venous Excess Ultrasound Score) en el síndrome cardiorrenal. In Nefrología al día; Lorenzo, V., López Gómez, J.M., Eds.; 2024; ISSN 2659-2606. Available online: https://www.nefrologiaaldia.org/593 (accessed on 1 May 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IVC (cm) | % Collapse of IVC | Central Venous Pressure (mmHg) |
|---|---|---|
| <1.5 | >50% | 0–5 |
| 1.5–2.5 | >50% | 5–10 |
| 1.5–2.5 | <50% | 10–15 |
| >2.5 | Minimum | 15–20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos-Saénz de Santamaría, A.; Pérez-Santana, J.; Croset, F.; Esterellas-Sánchez, L.K.; Lobo-Antuña, V.; Ripoll-Martínez, M.; Russo-Botero, S.; Gómez-Sacristán, H.; Pérez-Silvestre, J.; Fernández-Rodriguez, J.M.; et al. High-Complexity Questions and Their Answers for Everyday Heart Failure. J. Clin. Med. 2025, 14, 3993. https://doi.org/10.3390/jcm14113993
Campos-Saénz de Santamaría A, Pérez-Santana J, Croset F, Esterellas-Sánchez LK, Lobo-Antuña V, Ripoll-Martínez M, Russo-Botero S, Gómez-Sacristán H, Pérez-Silvestre J, Fernández-Rodriguez JM, et al. High-Complexity Questions and Their Answers for Everyday Heart Failure. Journal of Clinical Medicine. 2025; 14(11):3993. https://doi.org/10.3390/jcm14113993
Chicago/Turabian StyleCampos-Saénz de Santamaría, Amelia, Javier Pérez-Santana, François Croset, Laura Karla Esterellas-Sánchez, Victoria Lobo-Antuña, Miriam Ripoll-Martínez, Sofia Russo-Botero, Henar Gómez-Sacristán, José Pérez-Silvestre, José María Fernández-Rodriguez, and et al. 2025. "High-Complexity Questions and Their Answers for Everyday Heart Failure" Journal of Clinical Medicine 14, no. 11: 3993. https://doi.org/10.3390/jcm14113993
APA StyleCampos-Saénz de Santamaría, A., Pérez-Santana, J., Croset, F., Esterellas-Sánchez, L. K., Lobo-Antuña, V., Ripoll-Martínez, M., Russo-Botero, S., Gómez-Sacristán, H., Pérez-Silvestre, J., Fernández-Rodriguez, J. M., Sánchez-Marteles, M., Salamanca-Bautista, P., & Rubio-Gracia, J. (2025). High-Complexity Questions and Their Answers for Everyday Heart Failure. Journal of Clinical Medicine, 14(11), 3993. https://doi.org/10.3390/jcm14113993