
Epidemiological Evidence on the Associations of Metal Exposure with Alzheimer’s Disease and Related Dementias Among Elderly Women
 ,
, 
Abstract

1. Introduction
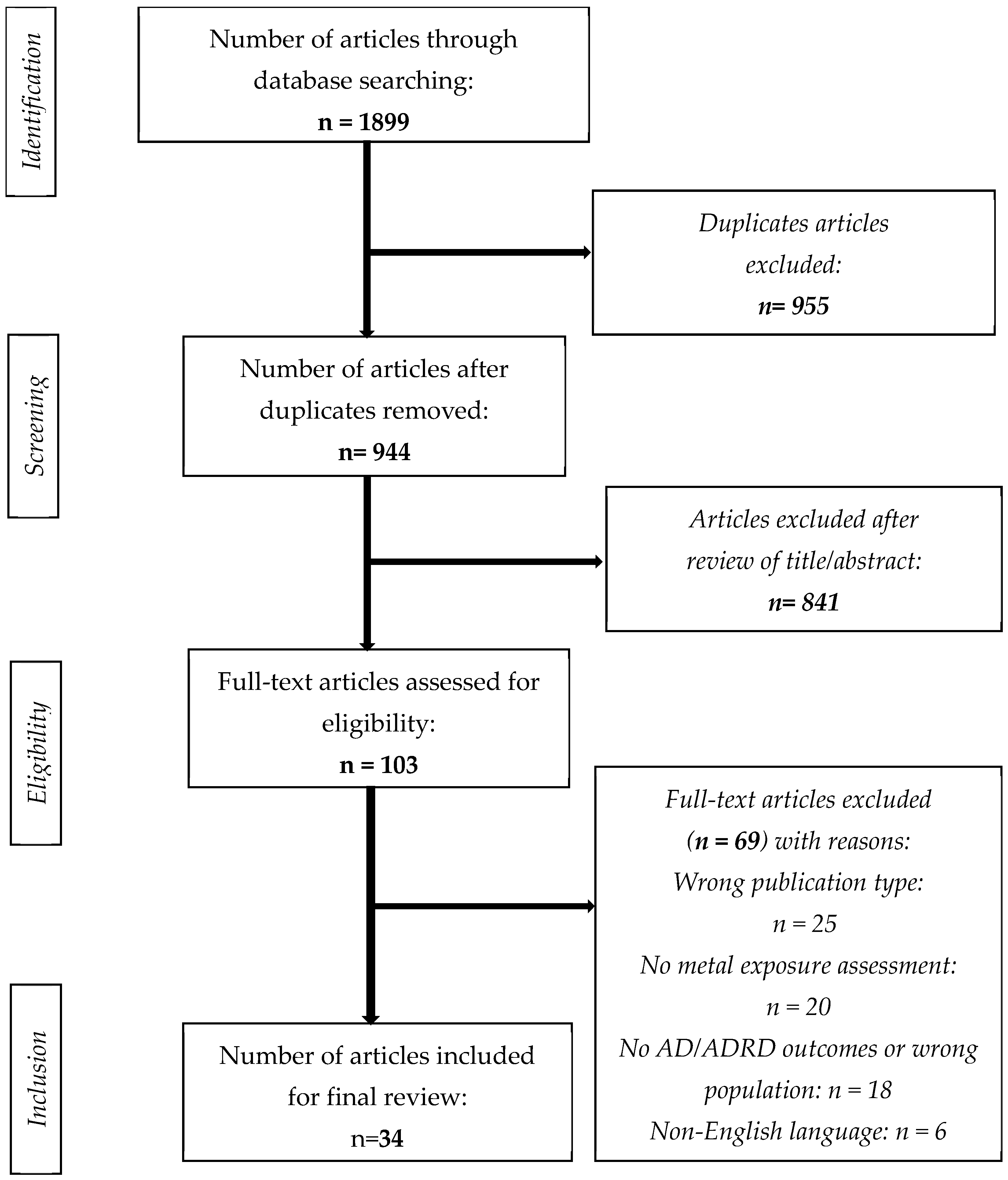
2. Methods
3. Results
3.1. Adverse Effects of Metals on AD/ADRD Outcomes Among Women
3.1.1. Lead (Pb)

{kind=link}
{kind=link}
{kind=link}
| Author and Metal(s) | Geographical Origin | Age (Mean Years ± SD) | Sample Size (Female) |
|---|---|---|---|
| Study design: Cohort | |||
| Ashraf et al. (2019) [46], Fe and Zn | United Kingdom | 77.5± 6.2 | 88 (48) |
| Giacconi et al. (2019) [47], Cu and Zn | Italy | 77.5 ± 0.05 | 179 (132) |
| Gong et al. (2021) [34], Fe | United States | 78 ± 8.6 | 3131 (1642) |
| Rembach et al. (2014) [48], Zn | Australia | 78.8 ± 8.6 | 1084(634) |
| Jinhui Yu et al. (2023) [49], Se and Zn | China | 71.70 ± 6.38 | 1025 (548) |
| Lui H et al. (2021) [15], Cd | China | 73.79 ± 5.92 | 1554 (994) |
| Liu Q et al. (2024) [44], Pb | China | 71.14 ± 5.78 | 1148 (634) |
| Power et al. (2014) [17], Pb | United States | 61 ± 6 | 584 (584) |
| Min J et al. (2016) [50], Cd | United States | 74.5 ± 8.36 | 4064 (2032) |
| Peng Q et al. (2017) [51], Cd | United States | 71.1 ± 0.24 | 2023 (971) |
| Study design: Case–control | |||
| Koseoglu et al. (2021) [52], As and Se | Turkey | 75.8 ± 5.8 | 80 (47) |
| Cardoso et al. (2017) [53], Se | Australia | 82.1 ± 1.2 | 209 (40) |
| Fathabadi et al. (2018) [38], Pb | Iran | 68.65 ± 7.39 | 81 (36) |
| Gu et al. (2021) [54] As and Se | China | 71.8 ± 6.5 | 1066 (583) |
| Huang et al. (2022) [55], Cd | United States | ≥60 years old | 1918 (964) |
| Jouini et al. (2021) [56], Fe and Ca | Tunisia | 70.538 ± 7.57 | 167 (102) |
| Zhang et al. (2022) [18], Cu and Cd | China | 67 ± 4.0 | 1667 (956) |
| Koc et al. (2015) [57], Cu, Mn, Mg, Se, and Mg | Turkey | 77.66 ± 9.28 | 78 (39) |
| Li H et al. (2018) [58], Cd | United States | 69.14 ± 10.91 | 2068 (1126) |
| Park et al. (2019) [59], Fe | Korea | 69.2 ± 8.4 | 127 (100) |
| Rozzini et al. (2018) [60], Cu | Italy | 77.1 ± 7.6 | 108 (58) |
| Socha et al. (2021) [36], Cu, Se, and Zn | Poland | 67.0 ± 7.9 | 170 (126) |
| Sternberg et al. (2017) [61], Fe | United states | 70.6 ± 7.4 | 85 (36) |
| Xu et al. (2018) [62], Mg, Ca, Fe, Cu, Zn, and Se | England | 78.2 ± 1.3 | 84 (39) |
| Yang et al. (2018) [33], As and Se | China | 76.48 ± 7.41 | 434 (244) |
| Study design: Cross-sectional | |||
| Cheng et al. (2022) [63], Se | China | 78.5 ± 10.68 | 3813 (1925) |
| Duhan et al. (2024) [64], Se and Cu | China | 72.4 ± 5.3 | 416 (208) |
| Hare et al. (2016) [65], Mn | Australia | 78 ± 8.6 | 100 (436) |
| Nascimento et al. (2021) [35], Se | Brazil | 74.41 ± 7.1 | 102 (70) |
| Wang et al. (2024) [66], Se and Cd | United States | 69.16 ± 6.68 | 1460 (675) |
| Wang X et al. (2021) [19], As | China | 57.0 ± 11.5 | 1556 (754) |
| Wang et al. (2024) [67], As, Fe, and Zn | China | 97.10 ± 4.92 | 408 (322) |
| Qing et al. (2024) [16], Pb and Cd | China | 70.55 ± 6.3 | 836 (485) |
| Zixuan Fu et al. (2024) [45], Pb, Cu, and Cd | United States | ≥60 | 811 (421) |
3.1.2. Cadmium (Cd)
3.1.3. Arsenic (As)
3.1.4. Multiple Metals (Adverse Effects and/or No Effects)
3.2. Beneficial Effects of Metals on AD/ADRD Outcomes Among Women
3.2.1. Zinc (Zn)
3.2.2. Selenium (Se)
3.2.3. Multiple Metals (Beneficial Effects)
4. Discussion
4.1. Adverse Effects of Metal Exposure on AD/ADRD
4.2. Neuroprotective and Essential Roles of Metals
4.3. Women’s Vulnerability in Other Neurodegenerative Diseases
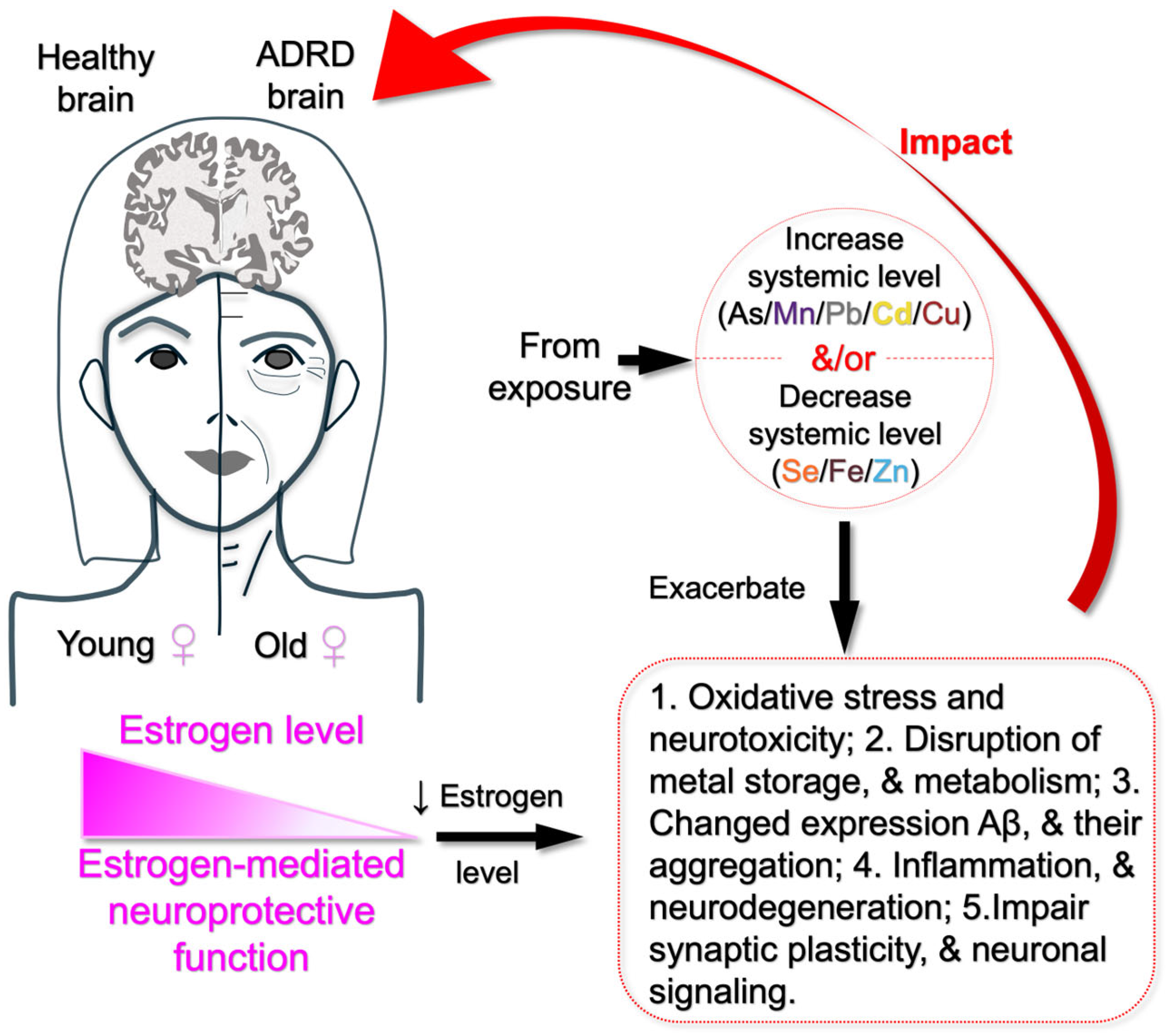
4.4. Possible Mechanisms Linking Metal Exposure, Sex Differences, and Cognitive Impairment
4.4.1. Neurotoxicity and Oxidative Stress
4.4.2. Hormonal Influence on Metal Metabolism
4.4.3. Inflammatory Pathways and Neurodegeneration
4.4.4. Metal-Induced Protein Aggregation
4.4.5. Potential Protective Roles of Zn and Se
4.5. Limitations
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| ADL | Activities of daily living scales |
| AFT | Animal Fluency Test |
| AIBL | Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing |
| AD/ADRD | Alzheimer’s disease and related dementias |
| APOE4 | Apolipoprotein E4 |
| BLL | Blood lead level |
| CI | Cognitive impaired |
| CN | Cognitive normal |
| CDR | Clinical Dementia Rating |
| CDR-SOB | Clinical Dementia Rating—Sum of Boxes |
| CERAD | Consortium to Establish and Registry for AD Test |
| CERAD-DR | Consortium to Establish and Registry for AD Test—Delayed Recall |
| CERAD-WL | Consortium to Establish and Registry for AD Test—Word Learning |
| CSF | Cerebrospinal fluid |
| DSST | Digit Symbol Substitution Test |
| DRT | Delayed Recall Test |
| GDS | Geriatric Depression Scale |
| HC | Healthy control |
| HE | Healthy elderly |
| HICs | High-income countries |
| IRT | Item response theory |
| LCP | Low cognitive performance |
| LMICs | Low- and middle-income countries |
| MCI | Mild cognitive impairment |
| MMSE | The Mini-Mental State Examination |
| MRI | Magnetic resonance imaging of the brain |
| MoCA | Montreal Cognitive Assessment |
| NHANES | National Health and Nutrition Examination Survey |
| NINCDS | National Institute of Neurological and Communicative Disorders and Stroke |
| RCTs | Randomized controlled trials |
| ROS | Reactive oxygen species |
References
- Ahmed, G.; Rahaman, M.S.; Perez, E.; Khan, K.M. Associations of Environmental Exposure to Arsenic, Manganese, Lead, and Cadmium with Alzheimer’s Disease: A Review of Recent Evidence from Mechanistic Studies. J. Xenobiot. 2025, 15, 47. [Google Scholar] [CrossRef] [PubMed]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef]
- Bott, N.T.; Sheckter, C.C.; Milstein, A.S. Dementia care, women’s health, and gender equity: The value of well-timed caregiver support. JAMA Neurol. 2017, 74, 757–758. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Research UK. Prevalence and Incidence of Dementia. Available online: https://www.dementiastatistics.org/about-dementia/prevalence-and-incidence/ (accessed on 10 March 2025).
- Cahill, S. WHO’s global action plan on the public health response to dementia: Some challenges and opportunities. Aging Ment. Health 2020, 24, 197–199. [Google Scholar] [CrossRef]
- Prince, M.; Albanese, E.; Guerchet, M.; Prina, M. World Alzheimer Report 2014. Dementia and Risk Reduction: An Analysis of Protective and Modifiable Risk Factors; Alzheimer’s Disease International: London, UK, 2014. [Google Scholar]
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Tran, T.A.; Mattap, S.M.; Warren, N.; Teng, J.H.J.; Duong, M.D.; Hoang, V.M.; Yasin, S.; Mohan, D. Caregiver burden among dementia caregivers in low-and middle-income countries in Asia: A systematic review. Aging Ment. Health 2025, 29, 579–590. [Google Scholar] [CrossRef]
- Wainberg, M.; Andrews, S.J.; Tripathy, S.J. Shared genetic risk loci between Alzheimer’s disease and related dementias, Parkinson’s disease, and amyotrophic lateral sclerosis. Alzheimer’s Res. Ther. 2023, 15, 113. [Google Scholar] [CrossRef]
- Bakulski, K.M.; Seo, Y.A.; Hickman, R.C.; Brandt, D.; Vadari, H.S.; Hu, H.; Park, S.K. Heavy metals exposure and Alzheimer’s disease and related dementias. J. Alzheimer’s Dis. 2020, 76, 1215–1242. [Google Scholar] [CrossRef]
- Wang, H.-X.; MacDonald, S.W.; Dekhtyar, S.; Fratiglioni, L. Association of lifelong exposure to cognitive reserve-enhancing factors with dementia risk: A community-based cohort study. PLoS Med. 2017, 14, e1002251. [Google Scholar] [CrossRef]
- Besser, L. Outdoor green space exposure and brain health measures related to Alzheimer’s disease: A rapid review. BMJ Open 2021, 11, e043456. [Google Scholar] [CrossRef]
- Shi, L.; Steenland, K.; Li, H.; Liu, P.; Zhang, Y.; Lyles, R.H.; Requia, W.J.; Ilango, S.D.; Chang, H.H.; Wingo, T. A national cohort study (2000–2018) of long-term air pollution exposure and incident dementia in older adults in the United States. Nat. Commun. 2021, 12, 6754. [Google Scholar] [CrossRef] [PubMed]
- Adani, G.; Filippini, T.; Garuti, C.; Malavolti, M.; Vinceti, G.; Zamboni, G.; Tondelli, M.; Galli, C.; Costa, M.; Vinceti, M. Environmental risk factors for early-onset Alzheimer’s dementia and frontotemporal dementia: A case-control study in northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 7941. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Su, L.; Chen, X.; Wang, S.; Cheng, Y.; Lin, S.; Ding, L.; Liu, J.; Chen, C.; Unverzagt, F.W. Higher blood cadmium level is associated with greater cognitive decline in rural Chinese adults aged 65 or older. Sci. Total Environ. 2021, 756, 144072. [Google Scholar] [CrossRef]
- Qing, Y.; Zheng, J.; Luo, Y.; Li, S.; Liu, X.; Yang, S.; Du, J.; Li, Y. The impact of metals on cognitive impairment in the elderly and the mediating role of oxidative stress: A cross-sectional study in Shanghai, China. Ecotoxicol. Environ. Saf. 2024, 286, 117152. [Google Scholar] [CrossRef]
- Power, M.C.; Korrick, S.; Tchetgen, E.J.T.; Nie, L.H.; Grodstein, F.; Hu, H.; Weuve, J.; Schwartz, J.; Weisskopf, M.G. Lead exposure and rate of change in cognitive function in older women. Environ. Res. 2014, 129, 69–75. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Q.; Xu, M.; Cai, J.; Wei, Y.; Lin, Y.; Mo, X.; Huang, S.; Liu, S.; Mo, C. Associations between plasma metals and cognitive function in people aged 60 and above. Biol. Trace Elem. Res. 2022, 200, 3126–3137. [Google Scholar] [CrossRef]
- Wang, X.; Huang, X.; Zhou, L.; Chen, J.; Zhang, X.; Xu, K.; Huang, Z.; He, M.; Shen, M.; Tang, B. Association of arsenic exposure and cognitive impairment: A population-based cross-sectional study in China. Neurotoxicology 2021, 82, 100–107. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2017 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2017, 13, 325–373. [Google Scholar] [CrossRef]
- Mielke, M.M. Sex and gender differences in Alzheimer’s disease dementia. Psychiatr. Times 2018, 35, 14. [Google Scholar]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef]
- Beam, C.R.; Kaneshiro, C.; Jang, J.Y.; Reynolds, C.A.; Pedersen, N.L.; Gatz, M. Differences between women and men in incidence rates of dementia and Alzheimer’s disease. J. Alzheimer’s Dis. 2018, 64, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Gilsanz, P.; Mayeda, E.R.; Glymour, M.M.; Quesenberry, C.P.; Mungas, D.M.; DeCarli, C.; Dean, A.; Whitmer, R.A. Female sex, early-onset hypertension, and risk of dementia. Neurology 2017, 89, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McGonagle, K.A.; Swartz, M.; Blazer, D.G.; Nelson, C.B. Sex and depression in the National Comorbidity Survey I: Lifetime prevalence, chronicity and recurrence. J. Affect. Disord. 1993, 29, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Goveas, J.S.; Espeland, M.A.; Woods, N.F.; Wassertheil-Smoller, S.; Kotchen, J.M. Depressive symptoms and incidence of mild cognitive impairment and probable dementia in elderly women: The Women’s Health Initiative Memory Study. J. Am. Geriatr. Soc. 2011, 59, 57–66. [Google Scholar] [CrossRef]
- Karp, A.; Kåreholt, I.; Qiu, C.; Bellander, T.; Winblad, B.; Fratiglioni, L. Relation of education and occupation-based socioeconomic status to incident Alzheimer’s disease. Am. J. Epidemiol. 2004, 159, 175–183. [Google Scholar] [CrossRef]
- Russ, T.C.; Stamatakis, E.; Hamer, M.; Starr, J.M.; Kivimaeki, M.; Batty, G.D. Socioeconomic status as a risk factor for dementia death: Individual participant meta-analysis of 86 508 men and women from the UK. Br. J. Psychiatry 2013, 203, 10–17. [Google Scholar] [CrossRef]
- Rocca, W.A.; Grossardt, B.R.; Shuster, L.T. Oophorectomy, menopause, estrogen treatment, and cognitive aging: Clinical evidence for a window of opportunity. Brain Res. 2011, 1379, 188–198. [Google Scholar] [CrossRef]
- Mishra, S.; Singh, G.; Gupta, A.; Tiwari, R.K. Heavy metal/metalloid contamination: Their sources in environment and accumulation in food chain. In Heavy Metal Toxicity: Environmental Concerns, Remediation and Opportunities; Springer: Berlin/Heidelberg, Germany, 2023; pp. 19–47. [Google Scholar]
- Gordon, S.; Lee, J.S.; Scott, T.M.; Bhupathiraju, S.; Ordovas, J.; Kelly, R.S.; Tucker, K.L.; Palacios, N. Metabolites and cognitive decline in a Puerto Rican cohort. J. Alzheimer’s Dis. 2024, 99, S345–S353. [Google Scholar] [CrossRef]
- Yadav, J.; Verma, A.K.; Ahmad, M.K.; Garg, R.K.; Shiuli; Mahdi, A.A.; Srivastava, S. Metals toxicity and its correlation with the gene expression in Alzheimer’s disease. Mol. Biol. Rep. 2021, 48, 3245–3252. [Google Scholar] [CrossRef]
- Yang, Y.-W.; Liou, S.-H.; Hsueh, Y.-M.; Lyu, W.-S.; Liu, C.-S.; Liu, H.-J.; Chung, M.-C.; Hung, P.-H.; Chung, C.-J. Risk of Alzheimer’s disease with metal concentrations in whole blood and urine: A case–control study using propensity score matching. Toxicol. Appl. Pharmacol. 2018, 356, 8–14. [Google Scholar] [CrossRef]
- Gong, Z.; Song, W.; Gu, M.; Zhou, X.; Tian, C. Association between serum iron concentrations and cognitive impairment in older adults aged 60 years and older: A dose-response analysis of National Health and Nutrition Examination Survey. PLoS ONE 2021, 16, e0255595. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, C.Q.d.; Barros-Neto, J.A.; Vieira, N.F.L.; Menezes-Filho, J.A.; Neves, S.J.F.; Lima, S.O. Selenium concentrations in elderly people with Alzheimer’s disease: A cross-sectional study with control group. Rev. Bras. Enferm. 2021, 74, e20200984. [Google Scholar] [CrossRef] [PubMed]
- Socha, K.; Klimiuk, K.; Naliwajko, S.K.; Soroczyńska, J.; Puścion-Jakubik, A.; Markiewicz-Żukowska, R.; Kochanowicz, J. Dietary habits, selenium, copper, zinc and total antioxidant status in serum in relation to cognitive functions of patients with Alzheimer’s disease. Nutrients 2021, 13, 287. [Google Scholar] [CrossRef]
- Sukumaran, P.; Nascimento Da Conceicao, V.; Sun, Y.; Ahamad, N.; Saraiva, L.R.; Selvaraj, S.; Singh, B.B. Calcium signaling regulates autophagy and apoptosis. Cells 2021, 10, 2125. [Google Scholar] [CrossRef]
- Fathabadi, B.; Dehghanifiroozabadi, M.; Aaseth, J.; Sharifzadeh, G.; Nakhaee, S.; Rajabpour-Sanati, A.; Amirabadizadeh, A.; Mehrpour, O. Comparison of blood lead levels in patients with Alzheimer’s disease and healthy people. Am. J. Alzheimer’s Dis. Other Dement. 2018, 33, 541–547. [Google Scholar] [CrossRef]
- Botturi, A.; Ciappolino, V.; Delvecchio, G.; Boscutti, A.; Viscardi, B.; Brambilla, P. The role and the effect of magnesium in mental disorders: A systematic review. Nutrients 2020, 12, 1661. [Google Scholar] [CrossRef]
- Kornblith, E.; Casey, S.L.; Lobdell, D.T.; Colledge, M.A.; Bowler, R.M. Environmental exposure to manganese in air: Tremor, motor and cognitive symptom profiles. Neurotoxicology 2018, 64, 152–158. [Google Scholar] [CrossRef]
- Ye, Q.; Park, J.E.; Gugnani, K.; Betharia, S.; Pino-Figueroa, A.; Kim, J. Influence of iron metabolism on manganese transport and toxicity. Metallomics 2017, 9, 1028–1046. [Google Scholar] [CrossRef]
- Coad, J.; Pedley, K. Iron deficiency and iron deficiency anemia in women. Scand. J. Clin. Lab. Investig. 2014, 74, 82–89. [Google Scholar] [CrossRef]
- Yang, Q.; Jian, J.; Katz, S.; Abramson, S.B.; Huang, X. 17β-Estradiol inhibits iron hormone hepcidin through an estrogen responsive element half-site. Endocrinology 2012, 153, 3170–3178. [Google Scholar] [CrossRef]
- Liu, Q.; Li, J.; Cheng, X.; Chen, G.; Zhang, Y.; Tian, Z.; Wang, Y.; Wang, H.; Guo, X.; Li, H. APOE ε4 allele modifies the associations of toxic metals and their mixture with cognitive impairment among older adults. Environ. Res. 2024, 255, 119148. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Xu, X.; Cao, L.; Xiang, Q.; Gao, Q.; Duan, H.; Wang, S.; Zhou, L.; Yang, X. Single and joint exposure of Pb, Cd, Hg, Se, Cu, and Zn were associated with cognitive function of older adults. Sci. Rep. 2024, 14, 28567. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.; Stosnach, H.; Parkes, H.G.; Hye, A.; Powell, J.; So, P.-W. Pattern of altered plasma elemental phosphorus, calcium, zinc, and iron in Alzheimer’s disease. Sci. Rep. 2019, 9, 3147. [Google Scholar] [CrossRef] [PubMed]
- Giacconi, R.; Giuli, C.; Casoli, T.; Balietti, M.; Costarelli, L.; Provinciali, M.; Basso, A.; Piacenza, F.; Postacchini, D.; Galeazzi, R. Acetylcholinesterase inhibitors in Alzheimer’s disease influence Zinc and Copper homeostasis. J. Trace Elem. Med. Biol. 2019, 55, 58–63. [Google Scholar] [CrossRef]
- Rembach, A.; Hare, D.J.; Doecke, J.D.; Burnham, S.C.; Volitakis, I.; Fowler, C.J.; Cherny, R.A.; McLean, C.; Grimm, R.; Martins, R. Decreased serum zinc is an effect of ageing and not Alzheimer’s disease. Metallomics 2014, 6, 1216–1219. [Google Scholar] [CrossRef]
- Yu, J.; He, Y.; Yu, X.; Gu, L.; Wang, Q.; Wang, S.; Tao, F.; Sheng, J. Associations between mild cognitive impairment and whole blood zinc and selenium in the elderly cohort. Biol. Trace Elem. Res. 2023, 201, 51–64. [Google Scholar] [CrossRef]
- Min, J.-Y.; Min, K.-B. Blood cadmium levels and Alzheimer’s disease mortality risk in older US adults. Environ. Health 2016, 15, 69. [Google Scholar] [CrossRef]
- Peng, Q.; Bakulski, K.M.; Nan, B.; Park, S.K. Cadmium and Alzheimer’s disease mortality in US adults: Updated evidence with a urinary biomarker and extended follow-up time. Environ. Res. 2017, 157, 44–51. [Google Scholar] [CrossRef]
- Koseoglu, E.; Kutuk, B.; Nalbantoglu, O.U.; Koseoglu, R.; Kendirci, M. Arsenic and selenium measurements in nail and hair show important relationships to Alzheimer’s disease in the elderly. J. Trace Elem. Med. Biol. 2021, 64, 126684. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Hare, D.J.; Bush, A.I.; Li, Q.-X.; Fowler, C.J.; Masters, C.L.; Martins, R.N.; Ganio, K.; Lothian, A.; Mukherjee, S. Selenium levels in serum, red blood cells, and cerebrospinal fluid of Alzheimer’s disease patients: A report from the Australian Imaging, Biomarker & Lifestyle Flagship Study of Ageing (AIBL). J. Alzheimer’s Dis. 2017, 57, 183–193. [Google Scholar]
- Gu, L.; Yu, J.; Fan, Y.; Wang, S.; Yang, L.; Liu, K.; Wang, Q.; Chen, G.; Zhang, D.; Ma, Y. The association between trace elements exposure and the cognition in the elderly in China. Biol. Trace Elem. Res. 2021, 199, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Ren, G. Interaction between ω-6 fatty acids intake and blood cadmium on the risk of low cognitive performance in older adults from National Health and Nutrition Examination Survey (NHANES) 2011–2014. BMC Geriatr. 2022, 22, 292. [Google Scholar] [CrossRef] [PubMed]
- Jouini, N.; Saied, Z.; Ben Sassi, S.; Nebli, F.; Messaoud, T.; Hentati, F.; Belal, S. Impacts of iron metabolism dysregulation on Alzheimer’s disease. J. Alzheimer’s Dis. 2021, 80, 1439–1450. [Google Scholar] [CrossRef]
- Koç, E.R.; Ilhan, A.; Aytürk, Z.; Acar, B.; Gürler, M.; Altuntaş, A.; Karapirli, M.; Bodur, A.S. A comparison of hair and serum trace elements in patients with Alzheimer disease and healthy participants. Turk. J. Med. Sci. 2015, 45, 1034–1039. [Google Scholar] [CrossRef]
- Li, H.; Wang, Z.; Fu, Z.; Yan, M.; Wu, N.; Wu, H.; Yin, P. Associations between blood cadmium levels and cognitive function in a cross-sectional study of US adults aged 60 years or older. BMJ Open 2018, 8, e020533. [Google Scholar] [CrossRef]
- Park, M.; Moon, Y.; Han, S.-H.; Moon, W.-J. Motor cortex hypointensity on susceptibility-weighted imaging: A potential imaging marker of iron accumulation in patients with cognitive impairment. Neuroradiology 2019, 61, 675–683. [Google Scholar] [CrossRef]
- Rozzini, L.; Lanfranchi, F.; Pilotto, A.; Catalani, S.; Gilberti, M.E.; Paganelli, M.; Apostoli, P.; Padovani, A. Serum non-ceruloplasmin non-albumin copper elevation in mild cognitive impairment and dementia due to Alzheimer’s disease: A case control study. J. Alzheimer’s Dis. 2018, 61, 907–912. [Google Scholar] [CrossRef]
- Sternberg, Z.; Hu, Z.; Sternberg, D.; Waseh, S.; Quinn, J.F.; Wild, K.; Jeffrey, K.; Zhao, L.; Garrick, M. Serum hepcidin levels, iron dyshomeostasis and cognitive loss in Alzheimer’s disease. Aging Dis. 2017, 8, 215. [Google Scholar] [CrossRef]
- Xu, J.; Church, S.J.; Patassini, S.; Begley, P.; Kellett, K.A.; Vardy, E.R.; Unwin, R.D.; Hooper, N.M.; Cooper, G.J. Plasma metals as potential biomarkers in dementia: A case–control study in patients with sporadic Alzheimer’s disease. Biometals 2018, 31, 267–276. [Google Scholar] [CrossRef]
- Cheng, B.-j.; Wang, J.; Meng, X.-l.; Sun, L.; Hu, B.; Li, H.-b.; Sheng, J.; Chen, G.-m.; Tao, F.-b.; Sun, Y.-h. The association between essential trace element mixture and cognitive function in Chinese community-dwelling older adults. Ecotoxicol. Environ. Saf. 2022, 231, 113182. [Google Scholar] [CrossRef]
- Duan, L.; Su, L.; He, X.; Du, Y.; Duan, Y.; Xu, N.; Wu, R.; Zhu, Y.; Shao, R.; Unverzagt, F.W. Multi-element Exposure and Cognitive Function in Rural Elderly Chinese. Biol. Trace Elem. Res. 2024, 202, 1401–1410. [Google Scholar] [CrossRef] [PubMed]
- Hare, D.J.; Faux, N.G.; Roberts, B.R.; Volitakis, I.; Martins, R.N.; Bush, A.I. Lead and manganese levels in serum and erythrocytes in Alzheimer’s disease and mild cognitive impairment: Results from the Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing. Metallomics 2016, 8, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Guo, L.; Shi, M.; Wang, L.; Zhou, Y.; Liu, H.; Xu, X.Q. Association of single and combined effects of blood heavy metals with cognitive function in older adults of the United States: A cross-sectional study. Res. Sq. 2024. [Google Scholar] [CrossRef]
- Wang, X.; Wang, B.; Yang, F.; Shang, K.; Chen, S.; Zhang, Y. Associations between plasma metal elements and risk of cognitive impairment among Chinese older adults. Front. Aging Neurosci. 2024, 16, 1353286. [Google Scholar] [CrossRef]
- Torres-Rojas, C.; Jones, B.C. Sex differences in neurotoxicogenetics. Front. Genet. 2018, 9, 196. [Google Scholar] [CrossRef]
- Varikasuvu, S.R.; Prasad, V.S.; Kothapalli, J.; Manne, M. Brain selenium in Alzheimer’s disease (BRAIN SEAD Study): A systematic review and meta-analysis. Biol. Trace Elem. Res. 2019, 189, 361–369. [Google Scholar] [CrossRef]
- Jomova, K.; Alomar, S.Y.; Nepovimova, E.; Kuca, K.; Valko, M. Heavy metals: Toxicity and human health effects. Arch. Toxicol. 2025, 99, 153–209. [Google Scholar] [CrossRef]
- Unverzagt, F.W.; Monahan, P.O.; Moser, L.R.; Zhao, Q.; Carpenter, J.S.; Sledge, G.W.; Champion, V.L. The Indiana University telephone-based assessment of neuropsychological status: A new method for large scale neuropsychological assessment. J. Int. Neuropsychol. Soc. 2007, 13, 799–806. [Google Scholar] [CrossRef]
- Bandeen-Roche, K.; Glass, T.A.; Bolla, K.I.; Todd, A.C.; Schwartz, B.S. Cumulative lead dose and cognitive function in older adults. Epidemiology 2009, 20, 831–839. [Google Scholar] [CrossRef]
- Weisskopf, M.G.; Proctor, S.P.; Wright, R.O.; Schwartz, J.; Spiro III, A.; Sparrow, D.; Nie, H.; Hu, H. Cumulative lead exposure and cognitive performance among elderly men. Epidemiology 2007, 18, 59–66. [Google Scholar] [CrossRef]
- Khalil, N.; Morrow, L.A.; Needleman, H.; Talbott, E.O.; Wilson, J.W.; Cauley, J.A. Association of cumulative lead and neurocognitive function in an occupational cohort. Neuropsychology 2009, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Lin, X.; Zhou, J.; Li, M.; Fu, Z.; Song, D. Concurrent serum lead levels and cognitive function in older adults. Front. Neurosci. 2023, 17, 1180782. [Google Scholar] [CrossRef] [PubMed]
- Basun, H.; Forssell, L.; Wetterberg, L.; Winblad, B. Metals and trace elements in plasma and cerebrospinal fluid in normal aging and Alzheimer’s disease. J. Neural Transm. Park. Dis. Dement. Sect. 1991, 3, 231–258. [Google Scholar]
- Lui, E.; Fisman, M.; Wong, C.; Diaz, F. Metals and the Liver in Alzheimer’s Disease An Investigation of Hepatic Zinc, Copper, Cadmium, and Metallothionein. J. Am. Geriatr. Soc. 1990, 38, 633–639. [Google Scholar] [CrossRef]
- Panayi, A.; Spyrou, N.; Iversen, B.; White, M.; Part, P. Determination of cadmium and zinc in Alzheimer’s brain tissue using inductively coupled plasma mass spectrometry. J. Neurol. Sci. 2002, 195, 1–10. [Google Scholar] [CrossRef]
- Męcik-Kronenberg, T.; Kuć, A.; Kubik-Machura, D.; Kościelecka, K.; Radko, L. Interaction of Metals, Menopause and COVID-19—A Review of the Literature. Biology 2023, 12, 350. [Google Scholar] [CrossRef]
- Monrad, M.; Ersbøll, A.K.; Sørensen, M.; Baastrup, R.; Hansen, B.; Gammelmark, A.; Tjønneland, A.; Overvad, K.; Raaschou-Nielsen, O. Low-level arsenic in drinking water and risk of incident myocardial infarction: A cohort study. Environ. Res. 2017, 154, 318–324. [Google Scholar] [CrossRef]
- Malavolta, M.; Giacconi, R.; Piacenza, F.; Santarelli, L.; Cipriano, C.; Costarelli, L.; Tesei, S.; Pierpaoli, S.; Basso, A.; Galeazzi, R. Plasma copper/zinc ratio: An inflammatory/nutritional biomarker as predictor of all-cause mortality in elderly population. Biogerontology 2010, 11, 309–319. [Google Scholar] [CrossRef]
- Osredkar, J.; Sustar, N. Copper and zinc, biological role and significance of copper/zinc imbalance. J. Clin. Toxicol. S 2011, 3, 0495. [Google Scholar] [CrossRef]
- Burmistrov, D.E.; Gudkov, S.V.; Franceschi, C.; Vedunova, M.V. Sex as a determinant of age-related changes in the brain. Int. J. Mol. Sci. 2024, 25, 7122. [Google Scholar] [CrossRef]
- Pinares-Garcia, P.; Stratikopoulos, M.; Zagato, A.; Loke, H.; Lee, J. Sex: A significant risk factor for neurodevelopmental and neurodegenerative disorders. Brain Sci. 2018, 8, 154. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, B.B.; Henry, J.F. Brain aging modulates the neuroprotective effects of estrogen on selective aspects of cognition in women: A critical review. Front. Neuroendocrinol. 2008, 29, 88–113. [Google Scholar] [CrossRef] [PubMed]
- Joborn, C.; Hetta, J.; Niklasson, F.; Rastad, J.; Wide, L.; Ågren, H.; Åkerström, G.; Ljunghall, S. Cerebrospinal fluid calcium, parathyroid hormone, and monoamine and purine metabolites and the blood-brain barrier function in primary hyperparathyroidism. Psychoneuroendocrinology 1991, 16, 311–322. [Google Scholar] [CrossRef]
- Breitwieser, G.E. Calcium sensing receptors and calcium oscillations: Calcium as a first messenger. Curr. Top. Dev. Biol. 2006, 73, 85–114. [Google Scholar]
- Tsien, R.W.; Wheeler, D.B. Voltage-gated calcium channels. In Calcium as a Cellular Regulator; Oxford University Press: New York, NY, USA, 1999; pp. 171–199. [Google Scholar]
- Limbrick Jr, D.; Sombati, S.; DeLorenzo, R. Calcium influx constitutes the ionic basis for the maintenance of glutamate-induced extended neuronal depolarization associated with hippocampal neuronal death. Cell Calcium 2003, 33, 69–81. [Google Scholar] [CrossRef]
- Tymianski, M.; Tator, C.H. Normal and abnormal calcium homeostasis in neurons: A basis for the pathophysiology of traumatic and ischemic central nervous system injury. Neurosurgery 1996, 38, 1176–1195. [Google Scholar]
- Park, S.; Kang, S.; Kim, D.S. Severe calcium deficiency increased visceral fat accumulation, down-regulating genes associated with fat oxidation, and increased insulin resistance while elevating serum parathyroid hormone in estrogen-deficient rats. Nutr. Res. 2020, 73, 48–57. [Google Scholar] [CrossRef]
- Lee, T.M.; Sun, D.; Leung, M.-K.; Chu, L.-W.; Keysers, C. Neural activities during affective processing in people with Alzheimer’s disease. Neurobiol. Aging 2013, 34, 706–715. [Google Scholar] [CrossRef]
- Wei, F.; Wang, D.; Li, H.; Xia, P.; Ran, Y.; You, J. Toxicogenomics provides insights to toxicity pathways of neonicotinoids to aquatic insect, Chironomus dilutus. Environ. Pollut. 2020, 260, 114011. [Google Scholar] [CrossRef]
- Moon, Y.; Han, S.-H.; Moon, W.-J. Patterns of brain iron accumulation in vascular dementia and Alzheimer’s dementia using quantitative susceptibility mapping imaging. J. Alzheimer’s Dis. 2016, 51, 737–745. [Google Scholar] [CrossRef]
- Park, M.; Moon, W.-J.; Moon, Y.; Choi, J.W.; Han, S.-H.; Wang, Y. Region-specific susceptibility change in cognitively impaired patients with diabetes mellitus. PLoS ONE 2018, 13, e0205797. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.J.; Zucca, F.A.; Duyn, J.H.; Crichton, R.R.; Zecca, L. The role of iron in brain ageing and neurodegenerative disorders. Lancet Neurol. 2014, 13, 1045–1060. [Google Scholar] [CrossRef] [PubMed]
- McClung, J.P.; Murray-Kolb, L.E. Iron nutrition and premenopausal women: Effects of poor iron status on physical and neuropsychological performance. Annu. Rev. Nutr. 2013, 33, 271–288. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Palta, P.; Rippon, B.; Soto, L.; Ceballos, F.; Pardo, M.; Laing, K.; Igwe, K.; Johnson, A.; Tomljanovic, Z. Sex differences in in vivo Alzheimer’s disease neuropathology in late middle-aged Hispanics. J. Alzheimer’s Dis. 2020, 74, 1243–1252. [Google Scholar] [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef]
- Tang, F.; Chi, I.; Dong, X. Sex differences in the prevalence and incidence of cognitive impairment: Does immigration matter? J. Am. Geriatr. Soc. 2019, 67, S513–S518. [Google Scholar] [CrossRef]
- Sussman, D.; Smith, L.M.; Anderson, M.E.; Duniho, S.; Hunter, J.H.; Kostner, H.; Miyamoto, J.B.; Nesterova, A.; Westendorf, L.; Van Epps, H.A. SGN–LIV1A: A novel antibody–drug conjugate targeting LIV-1 for the treatment of metastatic breast cancer. Mol. Cancer Ther. 2014, 13, 2991–3000. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Bandeira, V.S.; Jacob-Filho, W.; Cozzolino, S.M.F. Selenium status in elderly: Relation to cognitive decline. J. Trace Elem. Med. Biol. 2014, 28, 422–426. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Ong, T.P.; Jacob-Filho, W.; Jaluul, O.; Freitas, M.I.d.Á.; Cozzolino, S.M.F. Nutritional status of selenium in Alzheimer’s disease patients. Br. J. Nutr. 2010, 103, 803–806. [Google Scholar] [CrossRef]
- Vural, H.; Demirin, H.; Kara, Y.; Eren, I.; Delibas, N. Alterations of plasma magnesium, copper, zinc, iron and selenium concentrations and some related erythrocyte antioxidant enzyme activities in patients with Alzheimer’s disease. J. Trace Elem. Med. Biol. 2010, 24, 169–173. [Google Scholar] [CrossRef]
- Zhao, Y.; Ray, A.; Portengen, L.; Vermeulen, R.; Peters, S. Metal exposure and risk of Parkinson disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2023, 192, 1207–1223. [Google Scholar] [CrossRef]
- Baj, J.; Flieger, W.; Barbachowska, A.; Kowalska, B.; Flieger, M.; Forma, A.; Teresiński, G.; Portincasa, P.; Buszewicz, G.; Radzikowska-Büchner, E. Consequences of disturbing manganese homeostasis. Int. J. Mol. Sci. 2023, 24, 14959. [Google Scholar] [CrossRef] [PubMed]
- Antonioni, A.; Govoni, V.; Brancaleoni, L.; Donà, A.; Granieri, E.; Bergamini, M.; Gerdol, R.; Pugliatti, M. Amyotrophic lateral sclerosis and air pollutants in the province of Ferrara, Northern Italy: An ecological study. Int. J. Environ. Res. Public Health 2023, 20, 5591. [Google Scholar] [CrossRef] [PubMed]
- Kamel, F.; Umbach, D.M.; Munsat, T.L.; Shefner, J.M.; Hu, H.; Sandler, D.P. Lead exposure and amyotrophic lateral sclerosis. Epidemiology 2002, 13, 311–319. [Google Scholar] [CrossRef]
- Domingo-Relloso, A.; McGraw, K.E.; Heckbert, S.R.; Luchsinger, J.A.; Schilling, K.; Glabonjat, R.A.; Martinez-Morata, I.; Mayer, M.; Liu, Y.; Wood, A.C. Urinary metal levels, cognitive test performance, and dementia in the Multi-Ethnic Study of Atherosclerosis. JAMA Netw. Open 2024, 7, e2448286. [Google Scholar] [CrossRef]
- Eimer, W.A.; Kumar, D.K.V.; Shanmugam, N.K.N.; Rodriguez, A.S.; Mitchell, T.; Washicosky, K.J.; György, B.; Breakefield, X.O.; Tanzi, R.E.; Moir, R.D. Alzheimer’s disease-associated β-amyloid is rapidly seeded by herpesviridae to protect against brain infection. Neuron 2018, 99, 56–63.e53. [Google Scholar] [CrossRef]
- Ko, D.; Rahman, F.; Schnabel, R.B.; Yin, X.; Benjamin, E.J.; Christophersen, I.E. Atrial fibrillation in women: Epidemiology, pathophysiology, presentation, and prognosis. Nat. Rev. Cardiol. 2016, 13, 321–332. [Google Scholar] [CrossRef]
- Semba, R.D.; Ferrucci, L.; Sun, K.; Walston, J.; Varadhan, R.; Guralnik, J.M.; Fried, L.P. Oxidative stress is associated with greater mortality in older women living in the community. J. Am. Geriatr. Soc. 2007, 55, 1421–1425. [Google Scholar] [CrossRef]
- Karri, V.; Schuhmacher, M.; Kumar, V. Heavy metals (Pb, Cd, As and MeHg) as risk factors for cognitive dysfunction: A general review of metal mixture mechanism in brain. Environ. Toxicol. Pharmacol. 2016, 48, 203–213. [Google Scholar] [CrossRef]
- Zárate, S.; Stevnsner, T.; Gredilla, R. Role of estrogen and other sex hormones in brain aging. Neuroprotection and DNA repair. Front. Aging Neurosci. 2017, 9, 430. [Google Scholar] [CrossRef]
- Mehta, S.W.; Eikum, R. Effect of estrogen on serum and tissue levels of copper and zinc. In Copper Bioavailability and Metabolism; Springer: Berlin/Heidelberg, Germany, 1989; pp. 155–162. [Google Scholar]
- Dacks, P.A. Estrogens Iron out the Details: A Novel Direct Pathway for Estrogen Control of Iron Homeostasis; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Zhou, X.; Smith, A.M.; Failla, M.L.; Hill, K.E.; Yu, Z. Estrogen status alters tissue distribution and metabolism of selenium in female rats. J. Nutr. Biochem. 2012, 23, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Henson, M.C.; Chedrese, P.J. Endocrine disruption by cadmium, a common environmental toxicant with paradoxical effects on reproduction. Exp. Biol. Med. 2004, 229, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-S.Y.; Yin, Z.; Milatovic, D.; Jiang, H.; Aschner, M. Estrogen and tamoxifen protect against Mn-induced toxicity in rat cortical primary cultures of neurons and astrocytes. Toxicol. Sci. 2009, 110, 156–167. [Google Scholar] [CrossRef]
- Maynard, C.J.; Bush, A.I.; Masters, C.L.; Cappai, R.; Li, Q.X. Metals and amyloid-β in Alzheimer’s disease. Int. J. Exp. Pathol. 2005, 86, 147–159. [Google Scholar] [CrossRef]
- Sun, R.; Wang, J.; Feng, J.; Cao, B. Zinc in cognitive impairment and aging. Biomolecules 2022, 12, 1000. [Google Scholar] [CrossRef]
- Zhou, J.; Zhang, W.; Cao, Z.; Lian, S.; Li, J.; Nie, J.; Huang, Y.; Zhao, K.; He, J.; Liu, C. Association of selenium levels with neurodegenerative disease: A systemic review and meta-analysis. Nutrients 2023, 15, 3706. [Google Scholar] [CrossRef]
- Vural, Z.; Avery, A.; Kalogiros, D.I.; Coneyworth, L.J.; Welham, S.J. Trace mineral intake and deficiencies in older adults living in the community and institutions: A systematic review. Nutrients 2020, 12, 1072. [Google Scholar] [CrossRef]
| Reference | Metal(s) and Common Source | Diagnosis | Major Findings Related to Sex Differences |
|---|---|---|---|
| Ashraf et al. (2019) [46] | Plasma Zn; Food/ processed food | MMSE, CDR, and APOEε4-positive (n, %) | Zn was higher in AD. Sex was not statistically significant. |
| Duan et al. (2024) [64] | Ca, Zn, Fe, and Pb; Not mentioned | Nine standardized cognitive tests | No significant difference in sex. Higher levels of Ca (p = 0.025) were associated with lower cognitive function. Zn, Fe, and Pb were not associated. |
| Koseoglu et al. (2021) [52] | Nail and hair As and Se; Ground water | MMSE | As and Se levels were not associated with sex. Positive correlation between As and Se levels within the AD group (p < 0.01). |
| Fathabadi et al. (2018) [38] | Blood Pb; Industrial pollutants | MMSE | BLL was significantly higher in the patients group. Sex was not statistically significant. BLL was lower in women (p = 0.01). |
| Giacconi et al. (2019) [47] | Plasma Cu; Not mentioned | MMSE | No significant differences were found for sex. Significantly higher Cu levels among AD participants. |
| Gu et al. (2021) [54] | Blood As and Se; Not mentioned | MMSE | As and Se were associated with the increased risk of CI (p < 0.05). Sex was not statistically significant. |
| Huang et al. (2022) [55] | Blood Cd; Food | AFT, CERAD, and DSST | High-level Cd significantly was associated with low cognitive performance. Sex was not correlated. |
| Yu et al. (2023) [49] | Whole-blood Zn; Drinking water | ADL and MMSE | Higher Zn increased the risk of MCI, especially among women (p < 0.05). |
| Jouini N et al. (2021) [56] | CSF Fe; Not mentioned | Brain imaging and MMSE | Fe significantly higher in the AD group (p < 0.001). No difference was observed in women. |
| Zhang et al. (2022) [18] | Plasma Cu and Cd; Food, water, and industrial pollutants | MMSE | Significant positive correlation between the risk of CI and Cu and Cd (p < 0.05). Sex was also statistically significant, and most CI participants were female. |
| Koc et al. (2015) [57] | Hair Cu, Mn, and Mg; Not mentioned | MMSE | No significant variations based on sex. Significantly higher hair Cu and Mn levels found in AD patients (p < 0.05). Mg showed no effects on AD. |
| Lui H et al. (2021) [15] | Blood Cd; Air, water, soil, and food | Nine standardized cognitive tests | Higher Cd levels were significantly associated with greater cognitive decline. Sex wasstatistically significant (p< 0.05). |
| Li H et al. (2018) [58] | Blood Cd; Not mentioned | CERAD, Word List Learning Test, the CERAD Word List Recall Test, AFT, and DSST | Higher level of blood Cd was associated with worse cognitive function. Sex was significant (p< 0.05). |
| Liu Q et al. (2024) [44] | Blood Pb; Not mentioned | MMSE | Significant association with Pb and CI (p < 0.05). Sex was significant (p < 0.001), and most CI individuals tended to be women. |
| Power et al. (2014) [17] | Bone Pb; Not mentioned | Telephone-based cognitive assessment | Long-term cumulative Pb exposure weakly associated with faster cognitive decline among women. |
| Min J et al. (2016) [50] | Blood Cd; Air and industrial pollutants | NHANES (1999–2004) | Female participants (0.50 μg/L) had higher blood Cd levels. Significant association between high Cd levels and risk of AD mortality (p = 0.0684). |
| Wang et al. (2024) [66] | Blood Cd; Air | CERAD, Word Learning Test, AFT, and DSST | Higher blood Cd was associated with lower cognitive scores. Women group did not show any association. |
| Park et al. (2019) [59] | Brain Fe; Not mentioned | CDR, GDS, MMSE, and brain MRI | In the motor cortex, there was higher Fe among AD patients. No difference was observed in women. |
| Peng Q et al. (2017) [51] | Blood Cd; Not mentioned | NHANES 1999–2006 | Women (0.52 ng/mL) had significantly higher blood Cd level. Increased blood Cd was associated with AD mortality (p = 0.04). |
| Rozzini et al. (2018) [60] | Serum Cu; Not mentioned | MMSE | Higher Cu in MCI and dementia was due to AD (p < 0.0001). Women showed higher total Cu levels in both groups. |
| Socha et al. (2021) [36] | Serum Cu and Zn; Food | MMSE | The Cu/Zn molar ratio was significantly higher among women with AD. |
| Sternberg et al. (2017) [61] | Serum Fe; Not mentioned | MMSE, CDR, CDR-SOB, neuroimaging, and clinical data | Fe among AD patients was significantly higher (50%) compared to controls (p = 0.004). No difference was observed in women. |
| Wang et al. (2021) [19] | Hair As; Environment | MMSE | Women had a significantly higher prevalence of CI. Positive correlation between As and CI (OR= 1.84, p < 0.05). |
| Wang et al. (2024) [67] | Plasma Ca; Environment | MMSE | Plasma Ca was positively correlated with CI risk. Women group did not show any association. |
| Qing et al. (2024) [16] | Blood Bb and urinary Cd and Pb; Food | MoCA | Pb and Cd levels were significantly correlated with MoCA score. Sex was significant (p < 0.05), but women group did not show any association. |
| Yang et al. (2018) [33] | Whole-blood Se and urine As; Drinking water | CDR and MMSE | Women were significantly more likely to have AD. Significant association with both Se and As with AD risk (OR = 1.9, p < 0.05). |
| Fu et al. (2024) [45] | Blood Pb, Cd, and Cu; Air, water, and food | IRT, DRT, AFT, and DSST | High levels of Pb, Cd, and Cu were correlated with cognitive function. Female group had higher blood Pb level (2.09 µg/dL). |
| Reference | Metal(s) and Common Source | Diagnosis | Major Findings Related to Sex Differences |
|---|---|---|---|
| Ashraf et al. (2019) [46] | Plasma Fe; Food/processed food | MMSE, CDR, and APOEε4-positive (n, %) | Fe was lower in AD. Sex was not statistically significant. |
| Cardoso et al. (2017) [53] | Erythrocytes, serum, and CSF Se; Not mentioned | GDS and MMSE | Erythrocyte Se levels were significantly lower in AD (p < 0.05). No significant differences were found for sex. |
| Cheng et al. (2022) [63] | Urine Se; Food | MMSE | Se was positively associated with MMSE scores and cognitive function. Lower MMSE scores were found in women (p < 0.01). |
| Duan et al. (2024) [64] | Se, Cu; Not mentioned | Nine standardized cognitive tests | No significant difference in sex. Higher levels of Se (p = 0.007) and Cu (p = 0.048) were associated with better cognitive function in the elderly. |
| Giacconi et al. (2019) [47] | Plasma Zn; Not mentioned | MMSE | No significant differences were found for sex. Significantly lower Zn among AD patients. |
| Gong et al. (2021) [34] | Serum Fe; Not mentioned | DSST, AF, CERAD-DR, and CERAD-WL | Sex was not significant. Inverse dose–response relationship between serum Fe and CI. |
| Hare et al. (2016) [65] | Serum and erythrocyte Mn; Not mentioned | AIBL | Lower erythrocyte Mn (p = 0.053) in women. Serum Mn was decreased in AD compared to HC (p < 0.001). |
| Yu et al. (2023) [49] | Whole-blood Se; Drinking water | ADL and MMSE | Lower Se in MCI, especially among women (p < 0.05). |
| Jouini N et al. (2021) [56] | CSF Ca; Not mentioned | Brain imaging and MMSE | Ca was significantly lower in the AD group (p < 0.001). No difference was observed in women. |
| Koc et al. (2015) [57] | Hair Se and Zn; Not mentioned | MMSE | No significant variations based on sex. Significantly lower hair Se and Zn levels were found in AD patients (p < 0.05). |
| Nascimento et al. (2021) [35] | Plasma and erythrocyte Se; Food | NINCDS criteria by geriatrician and MMSE | Elderly with AD presented lower Se concentrations (p = 0.028). Odds ratio between men and women was 0.51. |
| Wang et al. (2024) [66] | Blood Se; Air | CERAD, Word Learning test, AFT, and DSST | Se has protective effect on cognitive function. Women group did not show any association. |
| Rembach et al. (2014) [48] | Serum Zn; Not mentioned | MMSE | Non-significant lower Zn levels in AD women. Serum Zn levels were significantly lower in AD patients compared to healthy controls (p = 0.001). |
| Socha et al. (2021) [36] | Serum Se and Zn; Food | MMSE | Significantly lower serum Se and Zn in AD patients, with women showing even lower (p < 0.05). |
| Xu et al. (2018) [62] | Serum Mg, Ca, Fe, Cu, Zn, and Se; Not mentioned | MMSE | Among female patients, none of the measured serum elements of serum Mg, Ca, Fe, Cu, Zn, Se differed in their plasma concentrations between the AD and control groups. Low levels of Zn and Fe were found in women participants. |
| Wang et al. (2024) [67] | Plasma Mn, Fe, and Zn; Environment | MMSE | Plasma Mn, Fe, and Zn levels were negatively correlated with CI risk. Women’s group did not show any association. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashid, F.; Khan, K.M.; Saiprakash, S.; Ahmed, G.; Sultana, R.; Parvez, F.; Islam, Z.; Rahaman, M.S. Epidemiological Evidence on the Associations of Metal Exposure with Alzheimer’s Disease and Related Dementias Among Elderly Women. J. Clin. Med. 2025, 14, 3776. https://doi.org/10.3390/jcm14113776
Rashid F, Khan KM, Saiprakash S, Ahmed G, Sultana R, Parvez F, Islam Z, Rahaman MS. Epidemiological Evidence on the Associations of Metal Exposure with Alzheimer’s Disease and Related Dementias Among Elderly Women. Journal of Clinical Medicine. 2025; 14(11):3776. https://doi.org/10.3390/jcm14113776
Chicago/Turabian StyleRashid, Fahmida, Khalid M. Khan, Samyukthaa Saiprakash, Giasuddin Ahmed, Rasheda Sultana, Faruque Parvez, Zhahirul Islam, and Md. Shiblur Rahaman. 2025. "Epidemiological Evidence on the Associations of Metal Exposure with Alzheimer’s Disease and Related Dementias Among Elderly Women" Journal of Clinical Medicine 14, no. 11: 3776. https://doi.org/10.3390/jcm14113776
APA StyleRashid, F., Khan, K. M., Saiprakash, S., Ahmed, G., Sultana, R., Parvez, F., Islam, Z., & Rahaman, M. S. (2025). Epidemiological Evidence on the Associations of Metal Exposure with Alzheimer’s Disease and Related Dementias Among Elderly Women. Journal of Clinical Medicine, 14(11), 3776. https://doi.org/10.3390/jcm14113776