
Influence of Increased Intra-Abdominal Pressure on the Validity of Ultrasound-Derived Inferior Vena Cava Measurements for Estimating Central Venous Pressure

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Outline
2.2. Patients
2.3. Ultrasound Techniques for Measuring the Inferior Vena Cava
2.4. Measurement of Intra-Abdominal Pressure
2.5. Measurement of Central Venous Pressure
2.6. Ultrasound-Guided Ascites Removal
2.7. Artificial Elevation of Intra-Abdominal Pressure
2.8. Predicting Central Venous Pressure
2.9. Correction of the Measured Inferior Vena Cava Diameters
2.10. Data Analysis
3. Results
3.1. Patients
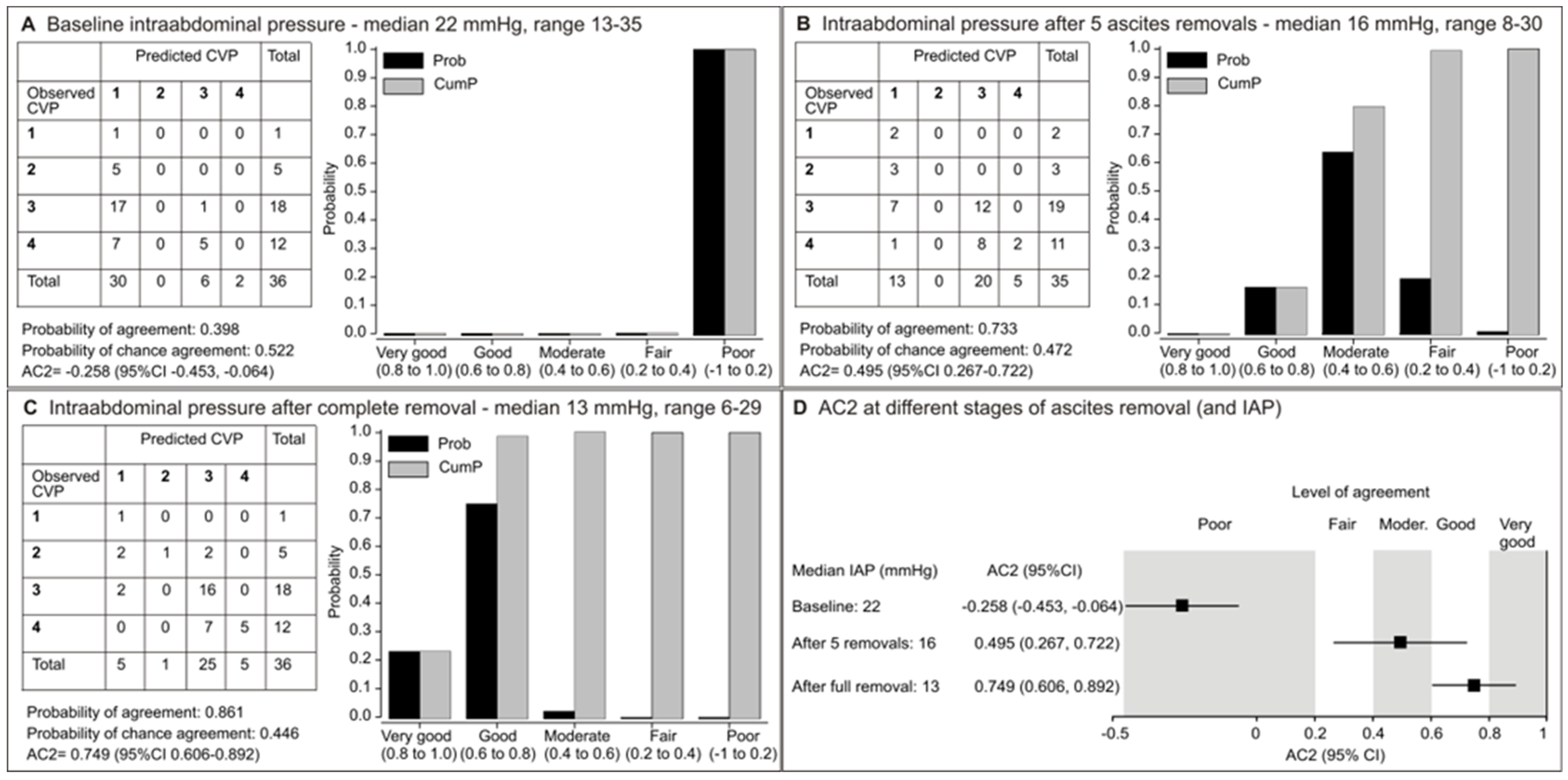
3.2. Relationship Between Decreasing Intra-Abdominal Pressure and Hemodynamic Indicators
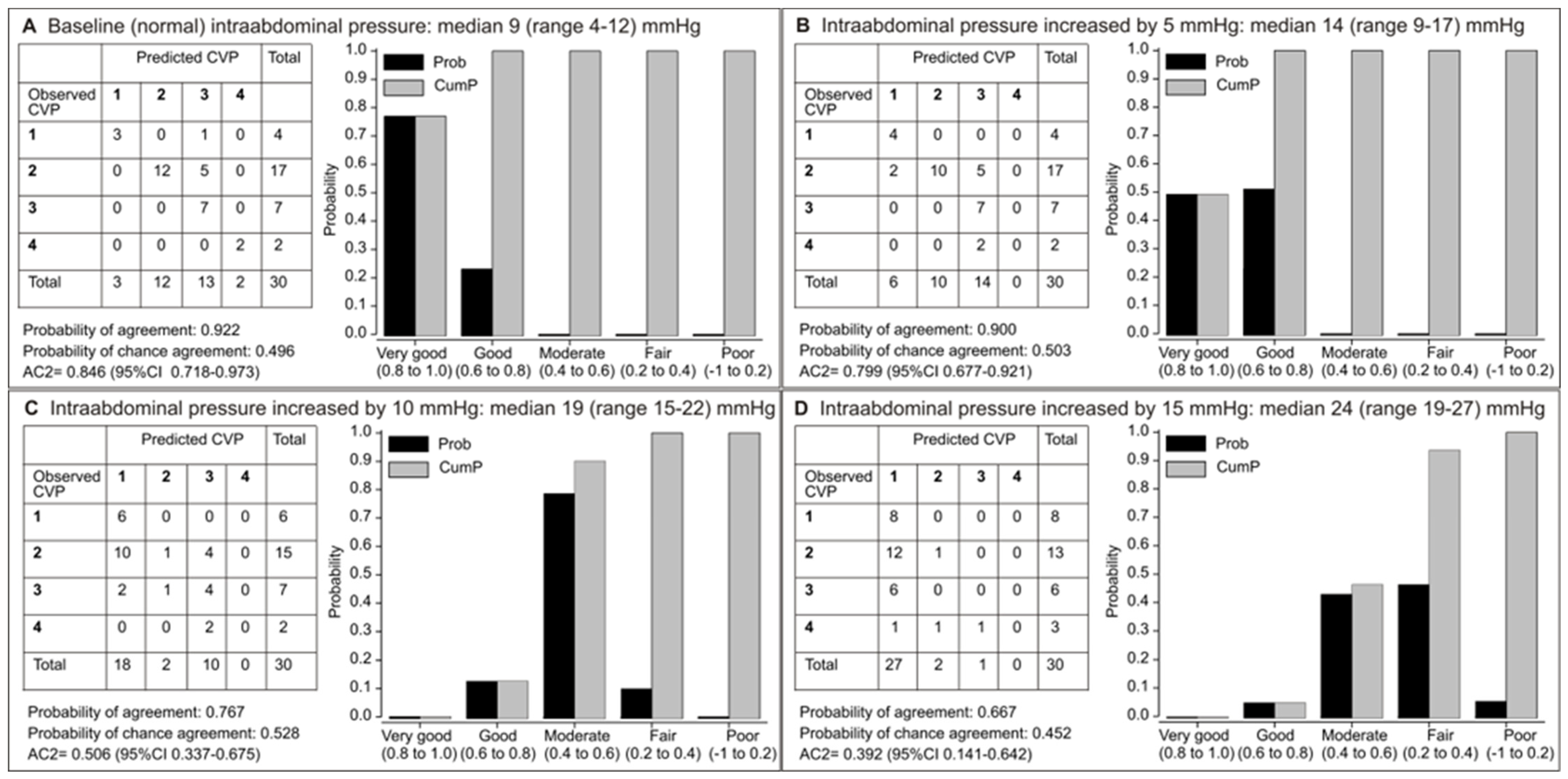
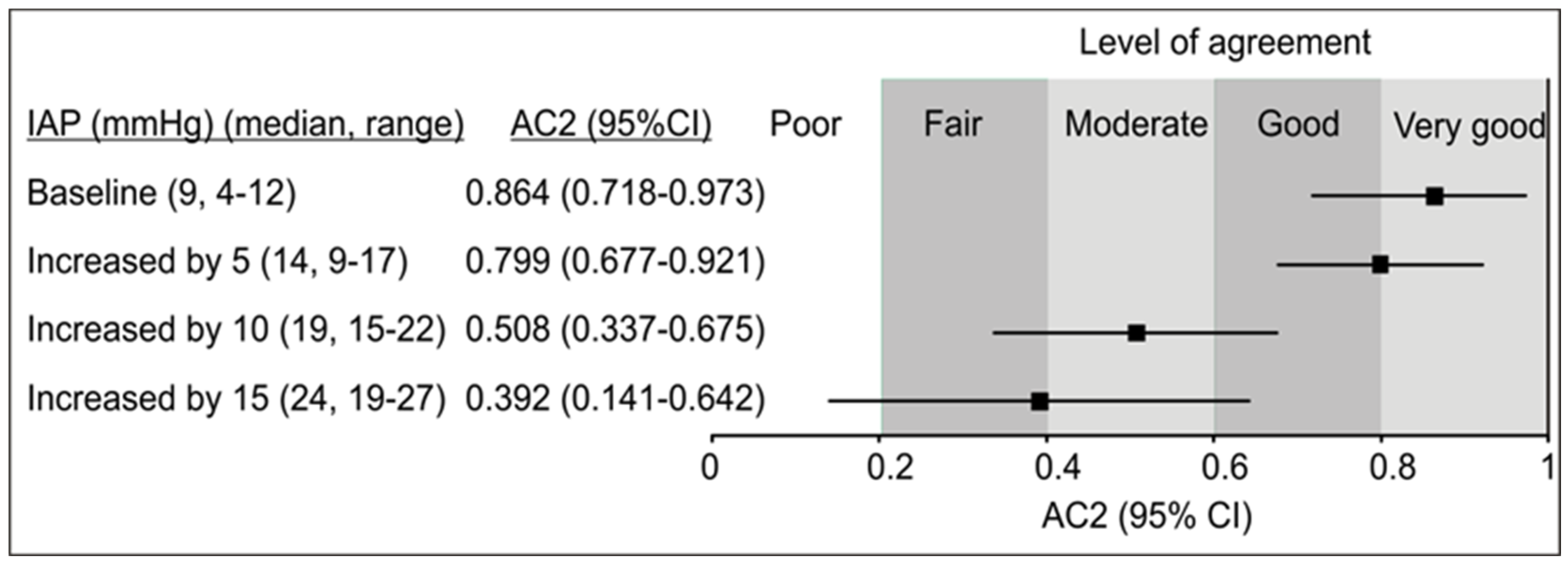
3.3. Relationship Between Increasing Intra-Abdominal Pressure and Hemodynamics Indicators
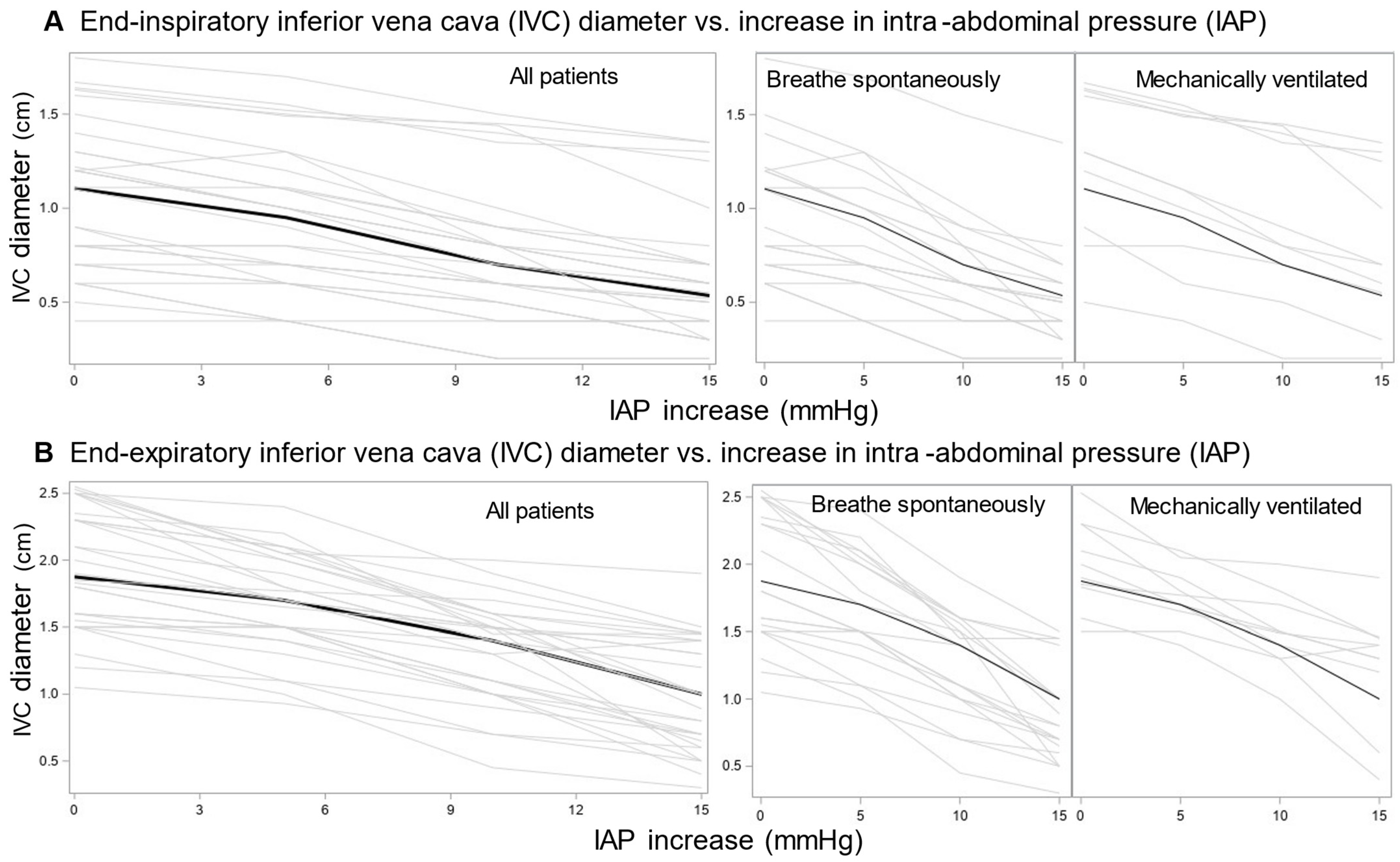
3.4. Corrected Inferior Vena Cava Diameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| AC2 | agreement coefficient |
| CVP | central venous pressure |
| ICU | intensive care unit |
| IAP | intra-abdominal pressure |
| IVC | inferior vena cava |
| IVCCI | inferior vena cava collapsibility index |
References
- Çelebi Yamanoğlu, N.; Yamanoğlu, A.; Parlak, İ.; Pınar, P.; Tosun, A.; Erkuran, B.; Aydınok, G.; Torlak, F. The Role of Inferior Vena Cava Diameter in Volume Status Monitoring; the Best Sonographic Measurement Method? Am. J. Emerg. Med. 2015, 33, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Seif, D.; Perera, P.; Mailhot, T.; Riley, D.; Mandavia, D. Bedside Ultrasound in Resuscitation and the Rapid Ultrasound in Shock Protocol. Crit. Care Res. Pract. 2012, 2012, 503254. [Google Scholar] [CrossRef] [PubMed]
- Zengin, S.; Al, B.; Genc, S.; Yildirim, C.; Ercan, S.; Dogan, M.; Altunbas, G. Role of Inferior Vena Cava and Right Ventricular Diameter in Assessment of Volume Status: A Comparative Study: Ultrasound and Hypovolemia. Am. J. Emerg. Med. 2013, 31, 763–767. [Google Scholar] [CrossRef]
- Killu, K.; Coba, V.; Blyden, D.; Munie, S.; Dereczyk, D.; Kandagatla, P.; Tang, A. Sonographic Assessment of Intravascular Fluid Estimate (SAFE) Score by Using Bedside Ultrasound in the Intensive Care Unit. Crit. Care Res. Pract. 2020, 2020, 9719751. [Google Scholar] [CrossRef]
- Thanakitcharu, P.; Charoenwut, M.; Siriwiwatanakul, N. Inferior Vena Cava Diameter and Collapsibility Index: A Practical Non-Invasive Evaluation of Intravascular Fluid Volume in Critically-Ill Patients. J. Med. Assoc. Thail. 2013, 96 (Suppl. 3), S14–S22. [Google Scholar]
- Sefidbakht, S.; Assadsangabi, R.; Abbasi, H.R.; Nabavizadeh, A. Sonographic Measurement of the Inferior Vena Cava as a Predictor of Shock in Trauma Patients. Emerg. Radiol. 2007, 14, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Corl, K.A.; George, N.R.; Romanoff, J.; Levinson, A.T.; Chheng, D.B.; Merchant, R.C.; Levy, M.M.; Napoli, A.M. Inferior Vena Cava Collapsibility Detects Fluid Responsiveness among Spontaneously Breathing Critically-Ill Patients. J. Crit. Care 2017, 41, 130–137. [Google Scholar] [CrossRef]
- Long, E.; Oakley, E.; Duke, T.; Babl, F.E. Does Respiratory Variation in Inferior Vena Cava Diameter Predict Fluid Responsiveness: A Systematic Review and Meta-Analysis. Shock 2017, 47, 550–559. [Google Scholar] [CrossRef]
- Ruge, M.; Marhefka, G.D. IVC Measurement for the Noninvasive Evaluation of Central Venous Pressure. J. Echocardiogr. 2022, 20, 133–143. [Google Scholar] [CrossRef]
- Ilyas, A.; Ishtiaq, W.; Assad, S.; Ghazanfar, H.; Mansoor, S.; Haris, M.; Qadeer, A.; Akhtar, A. Correlation of IVC Diameter and Collapsibility Index With Central Venous Pressure in the Assessment of Intravascular Volume in Critically Ill Patients. Cureus 2017, 9, e1025. [Google Scholar] [CrossRef]
- Ciozda, W.; Kedan, I.; Kehl, D.W.; Zimmer, R.; Khandwalla, R.; Kimchi, A. The Efficacy of Sonographic Measurement of Inferior Vena Cava Diameter as an Estimate of Central Venous Pressure. Cardiovasc. Ultrasound 2016, 14, 33. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef] [PubMed]
- Porter, T.R.; Shillcutt, S.K.; Adams, M.S.; Desjardins, G.; Glas, K.E.; Olson, J.J.; Troughton, R.W. Guidelines for the Use of Echocardiography as a Monitor for Therapeutic Intervention in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2015, 28, 40–56. [Google Scholar] [CrossRef]
- Kircher, B.J.; Himelman, R.B.; Schiller, N.B. Noninvasive Estimation of Right Atrial Pressure from the Inspiratory Collapse of the Inferior Vena Cava. Am. J. Cardiol. 1990, 66, 493–496. [Google Scholar] [CrossRef]
- Kelly, N.; Esteve, R.; Papadimos, T.J.; Sharpe, R.P.; Keeney, S.A.; DeQuevedo, R.; Portner, M.; Bahner, D.P.; Stawicki, S.P. Clinician-Performed Ultrasound in Hemodynamic and Cardiac Assessment: A Synopsis of Current Indications and Limitations. Eur. J. Trauma Emerg. Surg. 2015, 41, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Akoglu, E.U.; Demir, H.; Ozturk, T.C.; Ar, A.Y.; Turan, G. Respiratory Variability of Inferior Vena Cava at Different Mechanical Ventilator Settings. Am. J. Emerg. Med. 2021, 48, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Vieillard-Baron, A. Assessment of Right Ventricular Function. Curr. Opin. Crit. Care 2009, 15, 254–260. [Google Scholar] [CrossRef]
- Via, G.; Tavazzi, G.; Price, S. Ten Situations Where Inferior Vena Cava Ultrasound May Fail to Accurately Predict Fluid Responsiveness: A Physiologically Based Point of View. Intensive Care Med. 2016, 42, 1164–1167. [Google Scholar] [CrossRef]
- Battey, T.W.K.; Dreizin, D.; Bodanapally, U.K.; Wnorowski, A.; Issa, G.; Iacco, A.; Chiu, W. A Comparison of Segmented Abdominopelvic Fluid Volumes with Conventional CT Signs of Abdominal Compartment Syndrome in a Trauma Population. Abdom. Radiol. 2019, 44, 2648–2655. [Google Scholar] [CrossRef]
- Wachsberg, R.H.; Sebastiano, L.L.; Levine, C.D. Narrowing of the Upper Abdominal Inferior Vena Cava in Patients with Elevated Intraabdominal Pressure. Abdom. Imaging 1998, 23, 99–102. [Google Scholar] [CrossRef]
- Cavaliere, F.; Cina, A.; Biasucci, D.; Costa, R.; Soave, M.; Gargaruti, R.; Bonomo, L.; Proietti, R. Sonographic Assessment of Abdominal Vein Dimensional and Hemodynamic Changes Induced in Human Volunteers by a Model of Abdominal Hypertension. Crit. Care Med. 2011, 39, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Vieillard-Baron, A.; Evrard, B.; Repessé, X.; Maizel, J.; Jacob, C.; Goudelin, M.; Charron, C.; Prat, G.; Slama, M.; Geri, G.; et al. Limited Value of End-Expiratory Inferior Vena Cava Diameter to Predict Fluid Responsiveness Impact of Intra-Abdominal Pressure. Intensive Care Med. 2018, 44, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Rangegowda, D.; Kajal, K.; Khumuckham, J.S. Noninvasive Estimation of Intravascular Volume Status in Cirrhosis by Dynamic Size and Collapsibility Indices of the Inferior Vena Cava Using Bedside Echocardiography. JGH Open 2019, 3, 322–328. [Google Scholar] [CrossRef]
- Je, B.-K.; Kim, H.K.; Horn, P.S. Abdominal Compartment Syndrome in Children: Clinical and Imaging Features. AJR Am. J. Roentgenol. 2019, 212, 655–664. [Google Scholar] [CrossRef]
- Malbrain, M.L.N.G.; Cheatham, M.L.; Kirkpatrick, A.; Sugrue, M.; Parr, M.; De Waele, J.; Balogh, Z.; Leppäniemi, A.; Olvera, C.; Ivatury, R.; et al. Results from the International Conference of Experts on Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med. 2006, 32, 1722–1732. [Google Scholar] [CrossRef]
- Gestring, M. Abdominal Compartment Syndrome in Adults. UpToDate. Available online: https://www.uptodate.com/contents/abdominal-compartment-syndrome-in-adults#H354238352 (accessed on 19 October 2024).
- Vidal, M.G.; Ruiz Weisser, J.; Gonzalez, F.; Toro, M.A.; Loudet, C.; Balasini, C.; Canales, H.; Reina, R.; Estenssoro, E. Incidence and Clinical Effects of Intra-Abdominal Hypertension in Critically Ill Patients. Crit. Care Med. 2008, 36, 1823–1831. [Google Scholar] [CrossRef]
- Regueira, T.; Bruhn, A.; Hasbun, P.; Aguirre, M.; Romero, C.; Llanos, O.; Castro, R.; Bugedo, G.; Hernandez, G. Intra-Abdominal Hypertension: Incidence and Association with Organ Dysfunction during Early Septic Shock. J. Crit. Care 2008, 23, 461–467. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Ejike, J.C.; Leppäniemi, A.; De Keulenaer, B.L.; Kirkpatrick, A.W.; Roberts, D.J.; Kimball, E.; Ivatury, R.; Malbrain, M.L. Intra-Abdominal Hypertension and Abdominal Compartment Syndrome in Pancreatitis, Paediatrics, and Trauma. Anaesthesiol. Intensive Ther. 2015, 47, 219–227. [Google Scholar] [CrossRef]
- Wise, R.; Roberts, D.J.; Vandervelden, S.; Debergh, D.; De Waele, J.J.; De Laet, I.; Kirkpatrick, A.W.; De Keulenaer, B.L.; Malbrain, M.L. Awareness and Knowledge of Intra-Abdominal Hypertension and Abdominal Compartment Syndrome: Results of an International Survey. Anaesthesiol. Intensive Ther. 2015, 47, 14–29. [Google Scholar] [CrossRef]
- Cheatham, M.L.; Safcsak, K. Intraabdominal Pressure: A Revised Method for Measurement. J. Am. Coll. Surg. 1998, 186, 594–595. [Google Scholar] [CrossRef]
- Gwet, K.L. Handbook of Inter-Rater Reliability, 4th ed.; The Definitive Guide to Measuring The Extent of Agreement Among Raters; Advanced Analytics, LLC: Gaithersburg, MD, USA, 2014. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Schmidt, G.A. POINT: Should Acute Fluid Resuscitation Be Guided Primarily by Inferior Vena Cava Ultrasound for Patients in Shock? Yes. Chest 2017, 151, 531–532. [Google Scholar] [CrossRef] [PubMed]
- Barbier, C.; Loubières, Y.; Schmit, C.; Hayon, J.; Ricôme, J.-L.; Jardin, F.; Vieillard-Baron, A. Respiratory Changes in Inferior Vena Cava Diameter Are Helpful in Predicting Fluid Responsiveness in Ventilated Septic Patients. Intensive Care Med. 2004, 30, 1740–1746. [Google Scholar] [CrossRef]
- Preau, S.; Bortolotti, P.; Colling, D.; Dewavrin, F.; Colas, V.; Voisin, B.; Onimus, T.; Drumez, E.; Durocher, A.; Redheuil, A.; et al. Diagnostic Accuracy of the Inferior Vena Cava Collapsibility to Predict Fluid Responsiveness in Spontaneously Breathing Patients With Sepsis and Acute Circulatory Failure. Crit. Care Med. 2017, 45, e290–e297. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Pizzi, B. Inferior Vena Cava Distensibility as a Predictor of Fluid Responsiveness in Patients with Subarachnoid Hemorrhage. Neurocrit. Care 2010, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xu, X.; Ye, S.; Xu, L. Ultrasonographic Measurement of the Respiratory Variation in the Inferior Vena Cava Diameter Is Predictive of Fluid Responsiveness in Critically Ill Patients: Systematic Review and Meta-Analysis. Ultrasound Med. Biol. 2014, 40, 845–853. [Google Scholar] [CrossRef]
- Hill, B.; Smith, C. Central Venous Pressure Monitoring in Critical Care Settings. Br. J. Nurs. 2021, 30, 230–236. [Google Scholar] [CrossRef]
- Marino, P.L. The ICU Book, 4th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Spontaneous | Artificial | |
|---|---|---|---|
| N | 66 | 36 | 30 |
| Age (years) | 63 (54–72; 21–86) | 58 (47–66; 34–78) | 72 (61–76; 21–86) |
| Men | 46 (69.7) | 29 (80.6) | 17 (56.7) |
| Breathe spontaneously | 38 (57.6) | 18 (50) | 20 (66.7) |
| Mechanically ventilated | 28 (42.4) | 18 (50) | 10 (33.3) |
| BIPAP | 16 (24.2) | 11 (30.5) | 5 (16.6) |
| ASB | 11 (16.7) | 6 (16.6) | 5 (16.6) |
| SIMV | 1 (1.5) | 1 (2.8) | 0 |
| Sedated (midazolam) | 8 (12.1) | 7 (19.4) | 1 (3.3) |
| Diagnosis | |||
| Liver cirrhosis | 32 (48.5) | 30 (83.3) | 2 (6.7) |
| Sepsis | 13 (19.7) | 1 (2.8) | 12 (40.0) |
| Pneumonia | 6 (9.1) | 0 | 6 (20.0) |
| Cardiorespiratory arrest | 3 (4.5) | 0 | 3 (10.0) |
| Other | 12 (18.2) | 5 (13.9) | 7 (23.3) |
| Baseline IAP (mmHg) | 15.5 (9.8–22.2; 4–35) | 22.0 (19–25; 13–25) | 9.0 (7.7–10; 4.0–12.0) |
| Baseline CVP (mmHg) | 11.5 (8–15; 4–20) | 14.5 (11–16; 5–20) | 9.0 (7.7–10; 4.0–12.0) |
| Baseline end-inspiratory IVC (cm) | 1.0 (0.6–1.3; 0–2.2) | 0.9 (0.5–1.3; 0–2.2) | 1.1 (0.7–1.3; 0.4–1.8) |
| Baseline end-expiratory IVC (cm) | 1.5 (1.0–1.9; 0–2.5) | 1.1 (0.7–1.5; 0–2.3) | 1.9 (1.5–2.3; 1.1–2.6) |
| Baseline collapsibility index (%) | 30.6 (6.3–48.4; 0–68.8) | 7.4 (2.7–22.4; 0–51.5) | 48.1 (35.4–55.2; 8.7–68.7) |
| IAP (mmHg) | End-Inspiratory IVC | End-Expiratory IVC |
|---|---|---|
| 4–10 | none | none |
| 11–12 | +0.1 | +0.24 |
| 13 | +0.15 | +0.31 |
| 14–15 | +0.2 | +0.39 |
| 16–17 | +0.32 | +0.58 |
| 18 | +0.38 | +0.65 |
| 19–20 | +0.42 | +0.72 |
| 21–22 | +0.51 | +0.86 |
| 23 | +0.57 | +0.94 |
| 24–25 | +0.63 | +1.02 |
| 26–28 | +0.73 | +1.21 |
| 29–31 | +0.82 | +1.33 |
| 32–35 | +0.90 | +1.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rora Bertović, M.; Trkulja, V.; Ćurčić Karabaić, E.; Šundalić, S.; Bielen, L.; Ivičić, T.; Radonić, R. Influence of Increased Intra-Abdominal Pressure on the Validity of Ultrasound-Derived Inferior Vena Cava Measurements for Estimating Central Venous Pressure. J. Clin. Med. 2025, 14, 3684. https://doi.org/10.3390/jcm14113684
Rora Bertović M, Trkulja V, Ćurčić Karabaić E, Šundalić S, Bielen L, Ivičić T, Radonić R. Influence of Increased Intra-Abdominal Pressure on the Validity of Ultrasound-Derived Inferior Vena Cava Measurements for Estimating Central Venous Pressure. Journal of Clinical Medicine. 2025; 14(11):3684. https://doi.org/10.3390/jcm14113684
Chicago/Turabian StyleRora Bertović, Mia, Vladimir Trkulja, Ela Ćurčić Karabaić, Sara Šundalić, Luka Bielen, Toni Ivičić, and Radovan Radonić. 2025. "Influence of Increased Intra-Abdominal Pressure on the Validity of Ultrasound-Derived Inferior Vena Cava Measurements for Estimating Central Venous Pressure" Journal of Clinical Medicine 14, no. 11: 3684. https://doi.org/10.3390/jcm14113684
APA StyleRora Bertović, M., Trkulja, V., Ćurčić Karabaić, E., Šundalić, S., Bielen, L., Ivičić, T., & Radonić, R. (2025). Influence of Increased Intra-Abdominal Pressure on the Validity of Ultrasound-Derived Inferior Vena Cava Measurements for Estimating Central Venous Pressure. Journal of Clinical Medicine, 14(11), 3684. https://doi.org/10.3390/jcm14113684