

Lung Immune Prognostic Index-Based Predictive Score in Advanced Non-Small Cell Lung Cancer with a Programmed Death Ligand-1 Tumor Proportion Score ≥ 50%

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Baseline, Tumor, and Treatment Characteristics
3.1.1. Proof-of-Concept Cohort
3.1.2. Validation Cohort
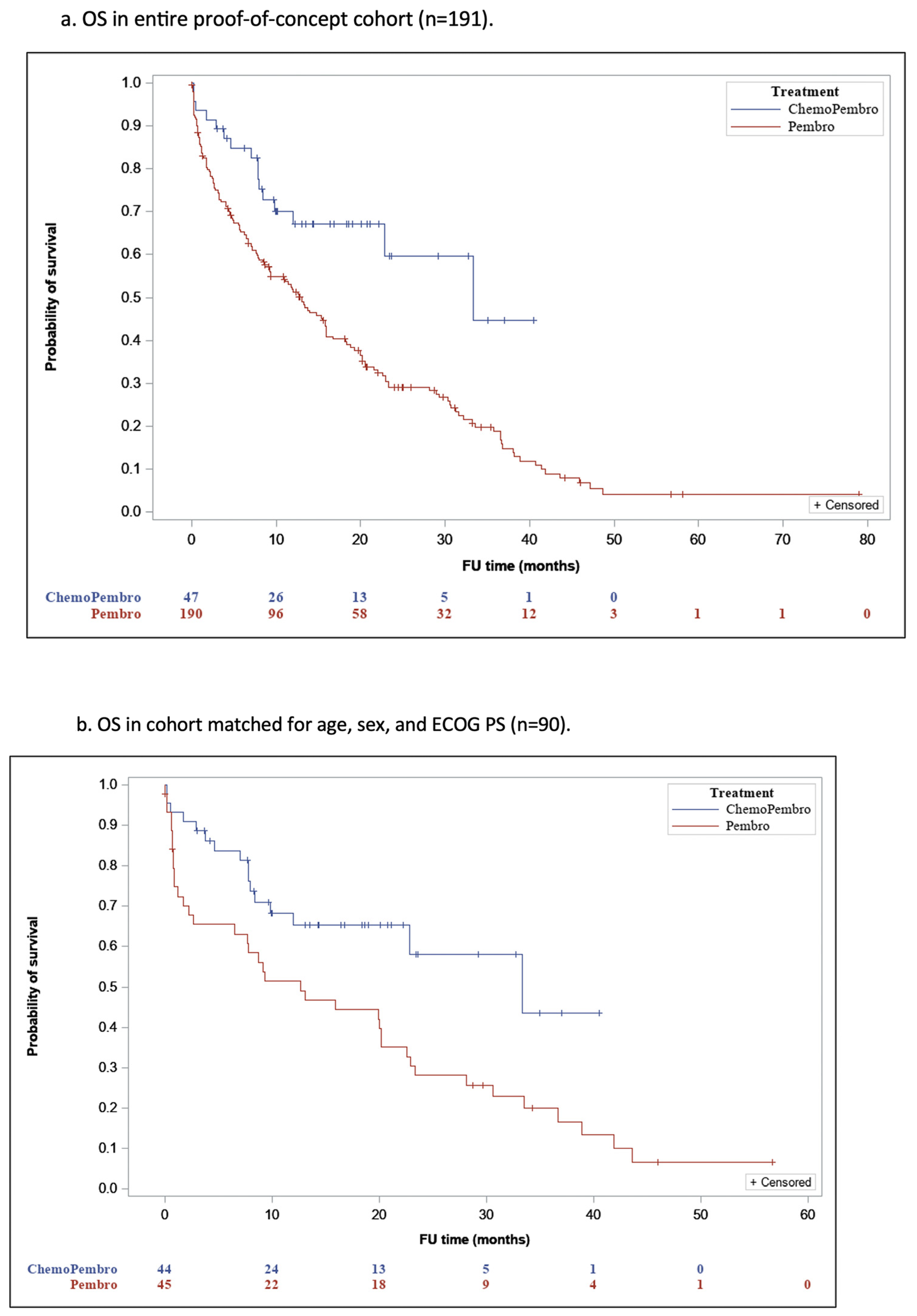
3.2. Overall Survival (OS) in the Entire and Matched Cohorts
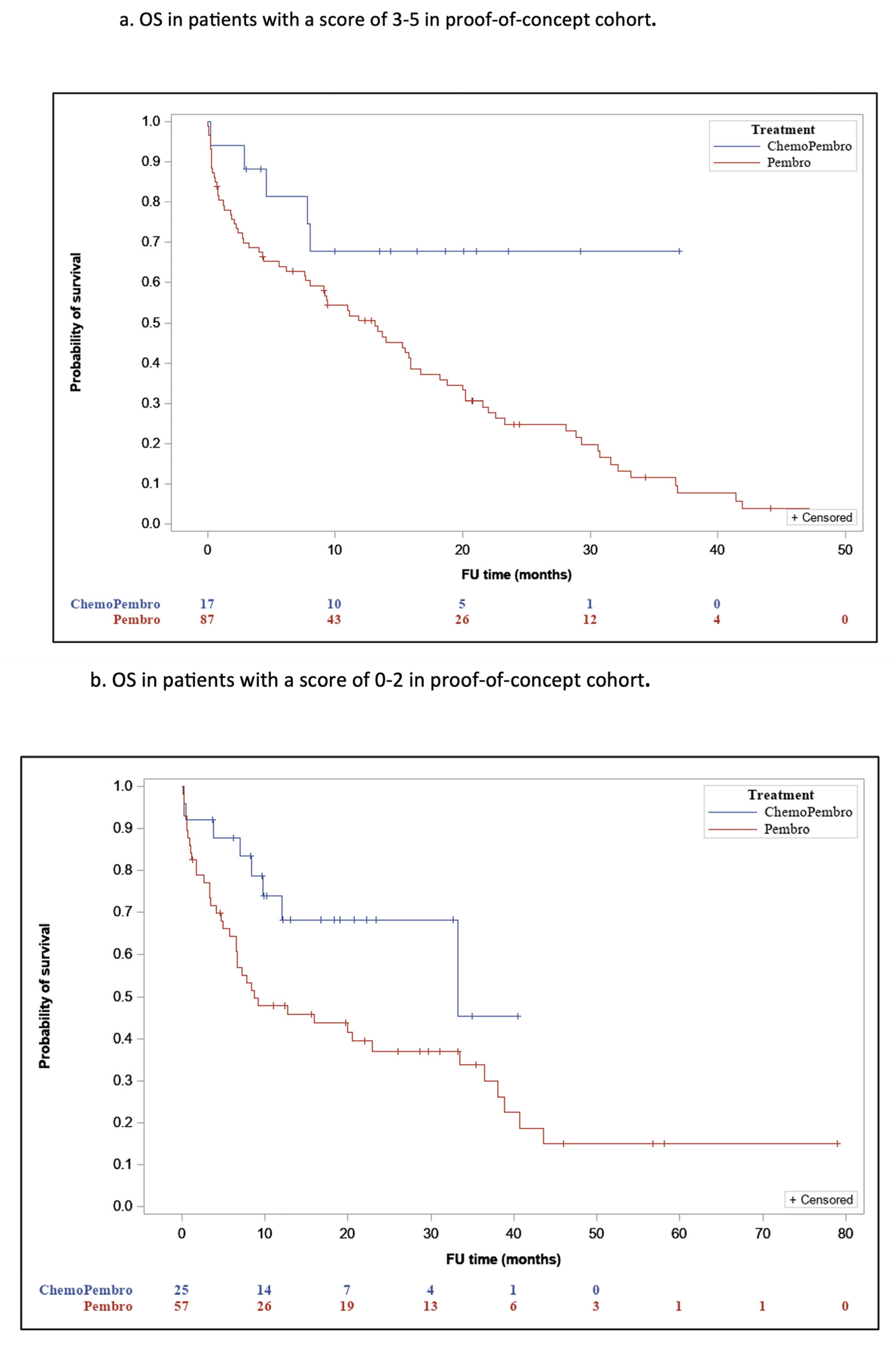
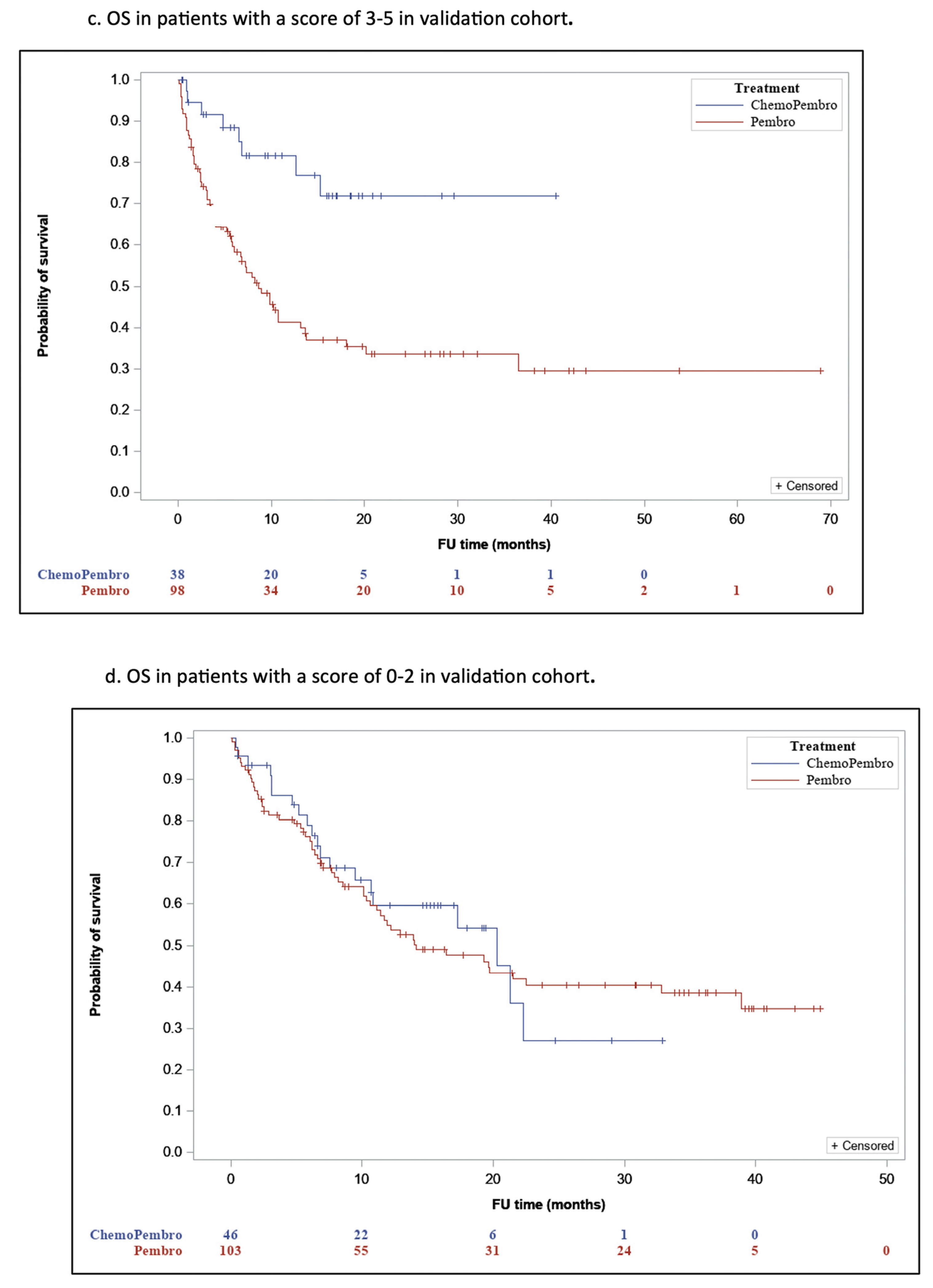
3.3. Predictive Score Development and Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aNSCLC | Advanced Non-Small Cell Lung Cancer |
| ALK | Anaplastic Lymphoma Kinase Gene |
| CI | Confidence Interval |
| ECOG PS | Eastern Cooperative Oncology Group Performance Status Score |
| EGFR | Epidermal Growth Factor Receptor Gene |
| IQR | Inter-Quartile Ranges |
| LIPI | Lung Immune Prognostic Index |
| mOS | Median Overall Survival |
| NA | Not Specified/Not Available |
| NOS | Not Otherwise Specified |
| NR | Not Reached |
| P | Pembrolizumab |
| PCT | Combination of Pembrolizumab with Platinum-Based Chemotherapy |
| PD-L1 | Programmed Death-Ligand 1 |
| Pts | Patients |
| PSM | Propensity score matching |
| ROS1 | Proto-Oncogene Tyrosine-Protein Kinase ROS1 |
| SD | Standard Deviation |
| TPS | Tumor Proportion Score |
References
- Arbour, K.C.; Riely, G.J. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA J. Am. Med. Assoc. 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Manson, G.; Norwood, J.; Marabelle, A.; Kohrt, H.; Houot, R. Biomarkers associated with checkpoint inhibitors. Ann. Oncol. 2016, 27, 1199–1206. [Google Scholar] [CrossRef]
- Jardim, D.L.; Goodman, A.; de Melo Gagliato, D.; Kurzrock, R. The Challenges of Tumor Mutational Burden as an Immunotherapy Biomarker. Cancer Cell 2021, 39, 154–173. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef]
- Chen, J.; Wei, S.; Zhao, T.; Zhang, X.; Wang, Y.; Zhang, X. Clinical Significance of Serum Biomarkers in Stage IV Non-Small-Cell Lung Cancer Treated with PD-1 Inhibitors: LIPI Score, NLR, dNLR, LMR, and PAB. Dis. Markers 2022, 2022, 7137357. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Russo, A.; Franchina, T.; Ricciardi, G.R.R.; Battaglia, A.; Scimone, A.; Berenato, R.; Giordano, A.; Adamo, V. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with Nivolumab or Docetaxel. J. Cell. Physiol. 2018, 233, 6337–6343. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Hao, L.; Yang, X.; Luo, C.; Wang, G.; Lin Cai, C.; Qi, S.; Li, Z. Prognostic value of derived neutrophil-to-lymphocyte ratio (dNLR) in patients with non-small cell lung cancer receiving immune checkpoint inhibitors: A meta-analysis. BMJ Open 2021, 11, 9. [Google Scholar] [CrossRef]
- Zhang, J.; Yao, Y.H.; Li, B.G.; Yang, Q.; Zhang, P.Y.; Wang, H.T. Prognostic value of pretreatment serum lactate dehydrogenase level in patients with solid tumors: A systematic review and meta-analysis. Sci. Rep. 2015, 5, 9800. [Google Scholar] [CrossRef]
- Cona, M.S.; Lecchi, M.; Cresta, S.; Damian, S.; Del Vecchio, M.; Necchi, A.; Poggi, M.M.; Raggi, D.; Randon, G.; Ratta, R.; et al. Combination of baseline LDH, performance status and age as integrated algorithm to identify solid tumor patients with higher probability of response to anti PD-1 and PD-l1 monoclonal antibodies. Cancers 2019, 11, 223. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non-small cell lung cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Reck, M.; Remon, J.; Hellmann, M.D. First-Line Immunotherapy for Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 586–597. [Google Scholar] [CrossRef]
- Leighl, N.B.; Laurie, S.A.; Goss, G.D.; Hughes, B.G.; Stockler, M.R.; Tsao, M.S.; Kulkarni, S.; Blais, N.; Joy, A.A.; Mates, M.; et al. CCTG BR.34: A randomized trial of durvalumab and tremelimumab +/− platinum-based chemotherapy in patients with metastatic (Stage IV) squamous or nonsquamous non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2020, 38 (Suppl. S15), 9502. [Google Scholar] [CrossRef]
- Holtzman, L.; Moskovitz, M.; Urban, D.; Nechushtan, H.; Keren, S.; Reinhorn, D.; Wollner, M.; Daher, S.; Rottenberg, Y.; Rovitzky, Y.; et al. dNLR-Based Score Predicting Overall Survival Benefit for The Addition of Platinum-Based Chemotherapy to Pembrolizumab in Advanced NSCLC with PD-L1 Tumor Proportion Score ≥ 50%. Clin. Lung Cancer 2022, 23, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ≥ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Gainor, J.F.; Rizvi, H.; Aguilar, E.J.; Skoulidis, F.; Yeap, B.Y.; Naidoo, J.; Khosrowjerdi, S.; Mooradian, M.; Lydon, C.; Illei, P.; et al. Clinical activity of programmed cell death 1 (PD-1) blockade in never, light, and heavy smokers with non-small-cell lung cancer and PD-L1 expression ≥ 50%. Ann. Oncol. 2020, 31, 404–411. [Google Scholar] [CrossRef]
- Cao, R.; Ma, J.T.; Zhang, S.L.; Sun, L.; Liu, Y.; Zhang, X.Y.; Jing, W.; Huang, L.T.; Han, C.B. Rational application of the first-line chemotherapy and immune checkpoint inhibitors in advanced nonsmall cell lung cancer: A meta-analysis. Cancer Med. 2019, 8, 5033–5046. [Google Scholar] [CrossRef]
- Zhou, Y.; Lin, Z.; Zhang, X.; Chen, C.; Zhao, H.; Hong, S.; Zhang, L. First-line treatment for patients with advanced non-small cell lung carcinoma and high PD-L1 expression: Pembrolizumab or pembrolizumab plus chemotherapy. J. Immunother. Cancer 2019, 7, 120. [Google Scholar] [CrossRef] [PubMed]
- Dudnik, E.; Moskovitz, M.; Rottenberg, Y.; Lobachov, A.; Mandelboim, R.; Shochat, T.; Urban, D.; Wollner, M.; Nechushtan, H.; Rotem, O.; et al. Pembrolizumab as a monotherapy or in combination with platinum-based chemotherapy in advanced non-small cell lung cancer with PD-L1 tumor proportion score (TPS) ≥ 50%: Real-world data. Oncoimmunology 2021, 10, 1865653. [Google Scholar] [CrossRef] [PubMed]
- Perol, M.; Felip, E.; Dafni, U.; Polito, L.; Pal, N.; Tsourti, Z.; Ton, T.G.N.; Merritt, D.; Morris, S.; Stahel, R.; et al. Effectiveness of PD-(L)1 inhibitors alone or in combination with platinum doublet chemotherapy in first-line (1L) non-squamous non-small-cell lung cancer (Nsq-NSCLC) with PD-L1-high expression using real-world data. Ann. Oncol. 2022, 33, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Franco, A.; Hodgson, C.; Raja, H.; Carter, M.; Lindsay, C.; Hughes, S.; Cove-Smith, L.; Taylor, P.; Summers, Y.; Blackhall, F.; et al. Real-World Data on Pembrolizumab for Pretreated Non-Small-Cell Lung Cancer: Clinical Outcome and Relevance of the Lung Immune Prognostic Index. Target. Oncol. 2022, 17, 453–465. [Google Scholar] [CrossRef]
- Sorich, M.J.; Rowland, A.; Karapetis, C.S.; Hopkins, A.M. Evaluation of the Lung Immune Prognostic Index for Prediction of Survival and Response in Patients Treated with Atezolizumab for NSCLC: Pooled Analysis of Clinical Trials. J. Thorac. Oncol. 2019, 14, 1440–1446. [Google Scholar] [CrossRef]
- Tanaka, S.; Uchino, J.; Yokoi, T.; Kijima, T.; Goto, Y.; Suga, Y.; Katayama, Y.; Nakamura, R.; Morimoto, K.; Nakao, A.; et al. Prognostic Nutritional Index and Lung Immune Prognostic Index as Prognostic Predictors for Combination Therapies of Immune Checkpoint Inhibitors and Cytotoxic Anticancer Chemotherapy for Patients with Advanced Non-Small Cell Lung Cancer. Diagnostics 2022, 12, 423. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Entire Cohort (n = 241) | Patients Matched for Age, Sex, ECOG PS (n = 90) | |||||
|---|---|---|---|---|---|---|
| Patients Treated with P (n = 191) | Patients Treated with PCT (n = 50) | p Value | Patients Treated with P (n = 45) | Patients Treated with PCT (n = 45) | p Value | |
| Age, years—mean (SD) | 70.4 (10) | 64.7 (7.6) | 0.00 | 66.5 (6.9) | 65.5 (9.8) | 0.37 |
| Sex, n (%) | 1.00 | 1.00 | ||||
| Female | 70 (36.6) | 18 (36) | 17 (37.8) | 17 (37.8) | ||
| Male | 121 (63.4) | 32 (64) | 28 (62.2) | 28 (62.2) | ||
| Smoking history, n (%) | 0.06 | 0.28 | ||||
| Current/past smoker | 140 (73.3) | 43 (86) | 34 (75.6) | 39 (86.7) | ||
| Never smoker | 51 (26.7) | 7 (14) | 11 (24.4) | 6 (13.3) | ||
| Histological subtype, n (%) | 0.39 | 0.32 | ||||
| Adenocarcinoma | 141 (73.8) | 40 (80) | 31 (68.9) | 37 (82.2) | ||
| Squamous cell | 40 (20.9) | 6 (12) | 11 (24.4) | 5 (11.1) | ||
| NSCLC NOS/other | 10 (5.3) | 4 (8) | 3 (6.6) | 3 (6.6) | ||
| Stage, n (%) | ||||||
| IV | 189 (99) | 48 (96) | 45 (100) | 43 (95) | ||
| NA | 2 (1) | 2 (4) | 0 (0) | 2 (5) | ||
| ECOG PS at diagnosis, n (%) | 0.01 | 1.00 | ||||
| 0/1 | 138 (72.2) | 44 (88) | 39 (86.6) | 39 (86.6) | ||
| 2/3/4/5 | 52 (27.3) | 6 (12) | 6 (13.3) | 6 (13.3) | ||
| NA | 1 (0.5) | 0 (0) | 0 (0) | 0 (0) | ||
| Brain metastases, n (%) | 1.00 | 0.30 | ||||
| Yes | 45 (23.6) | 11 (22) | 12 (26.7) | 10 (22.2) | ||
| No | 146 (76.4) | 38 (76) | 33 (73.3) | 34 (75.6) | ||
| NA | 0 (0) | 1 (2) | 0 (0) | 1 (2.2) | ||
| Liver metastases, n (%) | 0.41 | 0.77 | ||||
| Yes | 40 (20.9) | 7 (11) | 11 (24.4) | 6 (13.3) | ||
| No | 151 (79.1) | 42 (89) | 34 (75.6) | 38 (84.4) | ||
| NA | 0 (0) | 1 (2) | 0 (0) | 1 (2.2) | ||
| LIPI, n (%) | ||||||
| 0 | 39 (20.4) | 18 (36) | 5 (11.1) | 15 (33.3) | ||
| 1 | 59 (30.9) | 18 (36) | 16 (35.6) | 16 (35.6) | ||
| 2 | 47 (24.6) | 8 (16) | 0.10 | 21 (46.7) | 8 (17.8) | 0.00 |
| ½ | 106 (55.5) | 26 (52) | 37 (82.2) | 24 (53.3) | ||
| NA | 46 (24.1) | 6 (12) | 3 (6.7) | 6 (13.3) | ||
| Entire Cohort (n = 409) | |||
|---|---|---|---|
| Patients Treated with P (n = 295) | Patients Treated with PCT (n = 114) | p Value | |
| Age, years—mean (SD) | 69.2 (10.3) | 64.3 (9.2) | 0.00 |
| Sex, n (%) | 0.48 | ||
| Female | 100 (33.9) | 43 (37.7) | |
| Male | 195 (61.1) | 71 (62.3) | |
| Smoking history, n (%) | 0.06 | ||
| Current/past smoker | 263 (89.2) | 102 (89.5) | |
| Never smoker | 30 (10.2) | 11 (9.6) | |
| NA | 2 (0.7) | 1 (0.9) | |
| Histological subtype, n (%) | 0.39 | ||
| Adenocarcinoma | 222 (75.3) | 74 (64.9) | |
| Squamous cell | 50 (16.9) | 27 (23.7) | |
| NSCLC NOS/other | 23 (7.8) | 12 (10.5) | |
| NA | 0 (0) | 1 (0.9) | |
| Stage, n (%) | 1.00 | ||
| IV | 277 (93.9) | 106 (93) | |
| III (not amenable to definitive treatment) | 10 (3.4) | 3 (2.6) | |
| NA | 8 (2.7) | 5 (4.4) | |
| ECOG PS at diagnosis, n (%) | 0.223 | ||
| 0/1 | 197 (66.8) | 89 (78) | |
| 2/3/4/5 | 87 (29.5) | 22 (19.3) | |
| NA | 11 (3.7) | 3 (2.6) | |
| Brain metastases, n (%) | 0.53 | ||
| Yes | 82 (27.8) | 28 (24.6) | |
| No | 213 (72.2) | 86 (75.4) | |
| Liver metastases, n (%) | 0.61 | ||
| Yes | 35 (11.9) | 16 (14) | |
| No | 260 (88.1) | 98 (86) | |
| LIPI, n (%) | |||
| 0 (Good) | 81 (27.5) | 29 (25.4) | |
| 1 (Intermediate) | 80 (27.1) | 43 (37.7) | |
| 2 (Poor) | 45 (15.3) | 14 (12.3) | 0.24 |
| ½ | 161 (54.6) | 72 (63.1) | |
| NA | 89 (30.1) | 28 (24.6) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raphael, A.; Kamm Feldman, A.; Lazarev, I.; Kian, W.; Peled, N.; Hod, K.; Shalata, W.; Dudnik, E. Lung Immune Prognostic Index-Based Predictive Score in Advanced Non-Small Cell Lung Cancer with a Programmed Death Ligand-1 Tumor Proportion Score ≥ 50%. J. Clin. Med. 2025, 14, 3543. https://doi.org/10.3390/jcm14103543
Raphael A, Kamm Feldman A, Lazarev I, Kian W, Peled N, Hod K, Shalata W, Dudnik E. Lung Immune Prognostic Index-Based Predictive Score in Advanced Non-Small Cell Lung Cancer with a Programmed Death Ligand-1 Tumor Proportion Score ≥ 50%. Journal of Clinical Medicine. 2025; 14(10):3543. https://doi.org/10.3390/jcm14103543
Chicago/Turabian StyleRaphael, Ari, Ayelet Kamm Feldman, Irina Lazarev, Waleed Kian, Nir Peled, Keren Hod, Walid Shalata, and Elizabeth Dudnik. 2025. "Lung Immune Prognostic Index-Based Predictive Score in Advanced Non-Small Cell Lung Cancer with a Programmed Death Ligand-1 Tumor Proportion Score ≥ 50%" Journal of Clinical Medicine 14, no. 10: 3543. https://doi.org/10.3390/jcm14103543
APA StyleRaphael, A., Kamm Feldman, A., Lazarev, I., Kian, W., Peled, N., Hod, K., Shalata, W., & Dudnik, E. (2025). Lung Immune Prognostic Index-Based Predictive Score in Advanced Non-Small Cell Lung Cancer with a Programmed Death Ligand-1 Tumor Proportion Score ≥ 50%. Journal of Clinical Medicine, 14(10), 3543. https://doi.org/10.3390/jcm14103543