

Comparison of Neurodevelopmental Therapy with Standard Therapy for the Treatment of Patients with Spasticity After Stroke

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Standards
2.2. Participants
Independent Variables
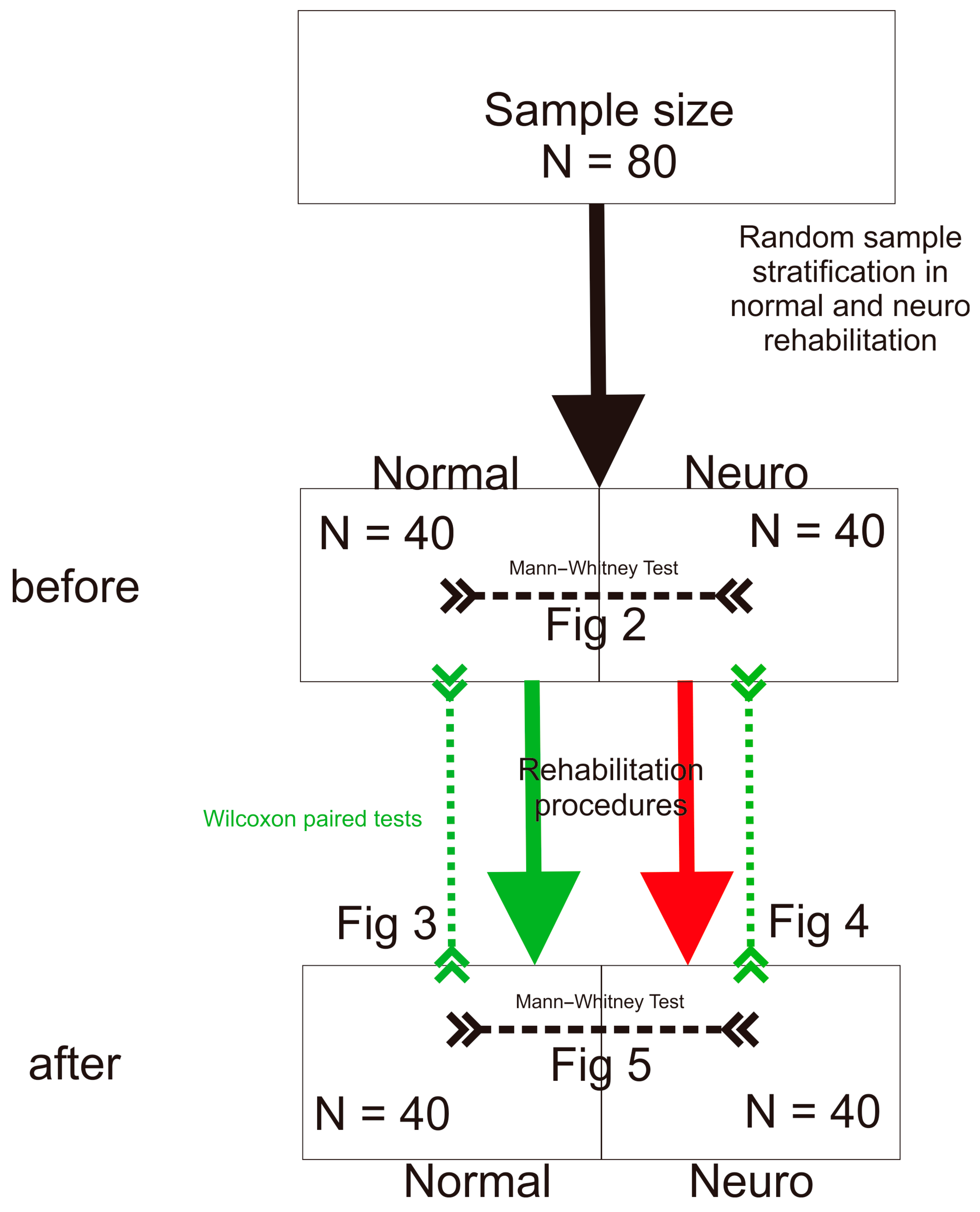
2.3. Procedures
Statistical Procedures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trompetto, C.; Marinelli, L.; Mori, L.; Pelosin, E.; Curra, A.; Molfetta, L.; Abbruzzese, G. Pathophysiology of spasticity: Implications for neurorehabilitation. BioMed Res. Int. 2014, 2014, 354906. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Cuaresma, L.; Lucena-Anton, D.; Gonzalez-Medina, G.; Martin-Vega, F.J.; Galan-Mercant, A.; Luque-Moreno, C. Effectiveness of Stretching in Post-Stroke Spasticity and Range of Motion: Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1074. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Zhang, W.; Kang, L.; Ma, Y.; Fu, L.; Jia, L.; Yu, H.; Chen, X.; Hou, L.; Wang, L.; et al. Clinical Evidence of Exercise Benefits for Stroke. Adv. Exp. Med. Biol. 2017, 1000, 131–151. [Google Scholar] [CrossRef]
- Saunders, D.H.; Sanderson, M.; Hayes, S.; Kilrane, M.; Greig, C.A.; Brazzelli, M.; Mead, G.E. Physical fitness training for stroke patients. Cochrane Database Syst. Rev. 2016, 3, Cd003316. [Google Scholar] [CrossRef] [PubMed]
- Bobath, B. Adult Hemiplegia: Evaluation and Treatment, 3rd ed.; Heinemann Medical Books: Oxford, UK, 1990. [Google Scholar]
- Wolny, T.; Saulicz, E.; Gnat, R.; Kokosz, M.; Myśliwiec, A.; Kuszewski, M. Influence of proprioceptiveneuromuscular facilitation (PNF) on the degree of spasticity in late-stage stroke patients. Fizjoterapia Pol. 2011, 11, 1–8. [Google Scholar]
- Pathak, A.; Gyanpuri, V.; Dev, P.; Dhiman, N.R. The Bobath Concept (NDT) as rehabilitation in stroke patients: A systematic review. J. Fam. Med. Prim. Care 2021, 10, 3983–3990. [Google Scholar] [CrossRef]
- Hindle, K.B.; Whitcomb, T.J.; Briggs, W.O.; Hong, J. Proprioceptive Neuromuscular Facilitation (PNF): Its Mechanisms and Effects on Range of Motion and Muscular Function. J. Hum. Kinet. 2012, 31, 105–113. [Google Scholar] [CrossRef]
- Elzib, H.; Pawloski, J.; Ding, Y.; Asmaro, K. Antidepressant pharmacotherapy and poststroke motor rehabilitation: A review of neurophysiologic mechanisms and clinical relevance. Brain Circ. 2019, 5, 62–67. [Google Scholar] [CrossRef]
- Zhang, H.; Lee, J.Y.; Borlongan, C.V.; Tajiri, N. A brief physical activity protects against ischemic stroke. Brain Circ. 2019, 5, 112–118. [Google Scholar] [CrossRef]
- Ostrowska, P.; Hansdorfer-Korzon, R.; Studnicki, R.; Spychała, D. Use of the posturography platform as a tool for quantitative assessment of imbalance and postural control in post-stroke patients in chronic phase. Fizjoter. Pol. 2023, 1, 142–163. [Google Scholar] [CrossRef]
- Paolucci, T.; Agostini, F.; Mussomeli, E.; Cazzolla, S.; Conti, M.; Sarno, F.; Bernetti, A.; Paoloni, M.; Mangone, M. A rehabilitative approach beyond the acute stroke event: A scoping review about functional recovery perspectives in the chronic hemiplegic patient. Front. Neurol. 2023, 14, 1234205. [Google Scholar] [CrossRef] [PubMed]
- Guiu-Tula, F.X.; Cabanas-Valdes, R.; Sitja-Rabert, M.; Urrutia, G.; Gomara-Toldra, N. The Efficacy of the proprioceptive neuromuscular facilitation (PNF) approach in stroke rehabilitation to improve basic activities of daily living and quality of life: A systematic review and meta-analysis protocol. BMJ Open 2017, 7, e016739. [Google Scholar] [CrossRef]
- Wang, R.Y.; Chen, H.I.; Chen, C.Y.; Yang, Y.R. Efficacy of Bobath versus orthopaedic approach on impairment and function at different motor recovery stages after stroke: A randomized controlled study. Clin. Rehabil. 2005, 19, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Krukowska, J.; Bugajski, M.; Sienkiewicz, M.; Czernicki, J. The influence of NDT-Bobath and PNF methods on the field support and total path length measure foot pressure (COP) in patients after stroke. Neurol. Neurochir. Pol. 2016, 50, 449–454. [Google Scholar] [CrossRef]
- Gunning, E.; Uszynski, M.K. Effectiveness of the Proprioceptive Neuromuscular Facilitation Method on Gait Parameters in Patients With Stroke: A Systematic Review. Arch. Phys. Med. Rehabil. 2019, 100, 980–986. [Google Scholar] [CrossRef]
- Nguyen, P.T.; Chou, L.W.; Hsieh, Y.L. Proprioceptive Neuromuscular Facilitation-Based Physical Therapy on the Improvement of Balance and Gait in Patients with Chronic Stroke: A Systematic Review and Meta-Analysis. Life 2022, 12, 882. [Google Scholar] [CrossRef] [PubMed]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- McKnight, P.E.; Najab, J. Mann-Whitney U Test. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010; p. 1. [Google Scholar]
- Wilcoxon Test. The Concise Encyclopedia of Statistics; Springer: New York, NY, USA, 2008; pp. 575–578. [Google Scholar]
- Smith, G.V.; Silver, K.H.; Goldberg, A.P.; Macko, R.F. “Task-oriented” exercise improves hamstring strength and spastic reflexes in chronic stroke patients. Stroke 1999, 30, 2112–2118. [Google Scholar] [CrossRef]
- Studnicki, R.; Studzińska, K.; Adamczewski, T.; Hansdorfer-Korzon, R.; Krawczyk, M. Analyzing the Impact of Rehabilitation Utilizing Neurofunctional Exercises on the Functional Status of Stroke Patients. J. Clin. Med. 2024, 13, 6271. [Google Scholar] [CrossRef]
- Ada, L.; Dorsch, S.; Canning, C.G. Strengthening interventions increase strength and improve activity after stroke: A systematic review. Aust. J. Physiother. 2006, 52, 241–248. [Google Scholar] [CrossRef]
- Allison, R.; Shenton, L.; Bamforth, K.; Kilbride, C.; Richards, D. Incidence, Time Course and Predictors of Impairments Relating to Caring for the Profoundly Affected arm After Stroke: A Systematic Review. Physiother. Res. Int. 2016, 21, 210–227. [Google Scholar] [CrossRef]
- Hesse, S.; Bertelt, C.; Jahnke, M.T.; Schaffrin, A.; Baake, P.; Malezic, M.; Mauritz, K.H. Treadmill training with partial body weight support compared with physiotherapy in nonambulatory hemiparetic patients. Stroke 1995, 26, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Yun, D.; Choi, J. Person-centered rehabilitation care and outcomes: A systematic literature review. Int. J. Nurs. Stud. 2019, 93, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Korner-Bitensky, N. When does stroke rehabilitation end? Int. J. Stroke 2013, 8, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, A.; Veluswamy, S.K.; Hombali, A.; Mullick, A.; Manikandan, N.; Solomon, J.M. Effect of Transcutaneous Electrical Nerve Stimulation on Spasticity in Adults with Stroke: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 751–768. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Pérez-Bellmunt, A.; Llurda-Almuzara, L.; Plaza-Manzano, G.; De-la-Llave-Rincón, A.I.; Navarro-Santana, M.J. Is Dry Needling Effective for the Management of Spasticity, Pain, and Motor Function in Post-Stroke Patients? A Systematic Review and Meta-Analysis. Pain Med. 2021, 22, 131–141. [Google Scholar] [CrossRef]
- Brusola, G.; Garcia, E.; Albosta, M.; Daly, A.; Kafes, K.; Furtado, M. Effectiveness of physical therapy interventions on post-stroke spasticity: An umbrella review. NeuroRehabilitation 2023, 52, 349–363. [Google Scholar] [CrossRef]
- Pollock, A.S.; Legg, L.; Langhorne, P.; Sellars, C. Barriers to achieving evidence-based stroke rehabilitation. Clin. Rehabil. 2000, 14, 611–617. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Studnicki, R.; Krawczyk, M.; Hansdorfer-Korzon, R.; Zubrzycki, I.Z.; Wiacek, M. Comparison of Neurodevelopmental Therapy with Standard Therapy for the Treatment of Patients with Spasticity After Stroke. J. Clin. Med. 2025, 14, 3450. https://doi.org/10.3390/jcm14103450
Studnicki R, Krawczyk M, Hansdorfer-Korzon R, Zubrzycki IZ, Wiacek M. Comparison of Neurodevelopmental Therapy with Standard Therapy for the Treatment of Patients with Spasticity After Stroke. Journal of Clinical Medicine. 2025; 14(10):3450. https://doi.org/10.3390/jcm14103450
Chicago/Turabian StyleStudnicki, Rafał, Maciek Krawczyk, Rita Hansdorfer-Korzon, Igor Z. Zubrzycki, and Magdalena Wiacek. 2025. "Comparison of Neurodevelopmental Therapy with Standard Therapy for the Treatment of Patients with Spasticity After Stroke" Journal of Clinical Medicine 14, no. 10: 3450. https://doi.org/10.3390/jcm14103450
APA StyleStudnicki, R., Krawczyk, M., Hansdorfer-Korzon, R., Zubrzycki, I. Z., & Wiacek, M. (2025). Comparison of Neurodevelopmental Therapy with Standard Therapy for the Treatment of Patients with Spasticity After Stroke. Journal of Clinical Medicine, 14(10), 3450. https://doi.org/10.3390/jcm14103450