
The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on the Consecutive Stages of Labour and Perinatal Outcomes—A Retrospective Cohort Study
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nori, W.; Kassim, M.A.K.; Helmi, Z.R.; Pantazi, A.C.; Brezeanu, D.; Brezeanu, A.M.; Penciu, R.C.; Serbanescu, L. Non-Pharmacological Pain Management in Labor: A Systematic Review. J. Clin. Med. 2023, 12, 7203. [Google Scholar] [CrossRef]
- Zuarez-Easton, S.; Erez, O.; Zafran, N.; Carmeli, J.; Garmi, G.; Salim, R. Pharmacologic and nonpharmacologic options for pain relief during labor: An expert review. Am. J. Obstet. Gynecol. 2023, 228, 1246–1259. [Google Scholar] [CrossRef]
- Whitburn, L.Y.; Jones, L.E.; Davey, M.A.; McDonald, S. The nature of labour pain: An updated review of the literature. Women Birth J. Aust. Coll. Midwives 2023, 32, 28–38. [Google Scholar] [CrossRef]
- Navarro-Prado, S.; Sánchez-Ojeda, M.A.; Marmolejo-Martín, J.; Kapravelou, G.; Fernández-Gómez, E.; Martín-Salvador, A. Cultural influence on the expression of labour-associated pain. BMC Pregnancy Childbirth 2022, 22, 836. [Google Scholar] [CrossRef]
- Janowski, J. Labor anesthesia—The current state of knowledge. J. Educ. Health Sport. 2022, 12, 184–197. [Google Scholar] [CrossRef]
- Elgzar, W.T.; Alshahrani, M.S.; Ibrahim, H.A. Non-pharmacological labor pain relive methods: Utilization and associated factors among midwives and maternity nurses in Najran, Saudi Arabia. Reprod. Health 2024, 21, 11. [Google Scholar] [CrossRef]
- Waller-Wise, R. Transcutaneous Electrical Nerve Stimulation: An Overview. J. Perinat. Educ. 2022, 31, 49–57. [Google Scholar] [CrossRef]
- Yu, M.; Qian, H.; Gan, M. Comparison of different interventions for the reduction of labor pain: A systematic review and network meta-analysis. Medicine 2023, 103, e37047. [Google Scholar] [CrossRef]
- De Santana, J.M.; Walsh, D.M.; Vance, C.; Rakel, B.A.; Sluka, K.A. Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain. Curr. Rheumatol. Rep. 2008, 10, 492–499. [Google Scholar] [CrossRef]
- Thuvarakan, K.; Zimmermann, H.; Mikkelsen, M.K.; Gazerani, P. Transcutaneous Electrical Nerve Stimulation as a Pain-Relieving Approach in Labor Pain: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Neuromodul. J. Int. Neuromodul. Soc. 2023, 23, 732–746. [Google Scholar] [CrossRef]
- Reis, C.C.S.D.; Dias, L.D.C.; Carvalho, L.B.; Junior, L.B.A.; Imoto, A.M. Transcutaneous Nerve Electrostimulation (TENS) in Pain Relief During Labor: A Scope Review. Eletroestimulação nervosa transcutânea (TENS) no alívio da dor durante o trabalho de parto: Uma revisão de escopo. Rev. Bras. Ginecol. Obstet. 2022, 44, 187–193. [Google Scholar] [CrossRef]
- Dowswell, T.; Bedwell, C.; Lavender, T.; Neilson, J.P. Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database Syst. Rev. 2009, CD007214. [Google Scholar] [CrossRef]
- Santana, L.S.; Gallo, R.B.; Ferreira, C.H.; Duarte, G.; Quintana, S.M.; Marcolin, A.C. Transcutaneous electrical nerve stimulation (TENS) reduces pain and postpones the need for pharmacological analgesia during labour: A randomised trial. J. Physiother. 2016, 62, 29–34. [Google Scholar] [CrossRef]
- Njogu, A.; Qin, S.; Chen, Y.; Hu, L.; Luo, Y. The effects of transcutaneous electrical nerve stimulation during the first stage of labor: A randomized controlled trial. BMC Pregnancy Childbirth 2021, 21, 164. [Google Scholar] [CrossRef]
- Lindholm, A.; Hildingsson, I. Women’s preferences and received pain relief in childbirth—A prospective longitudinal study in a northern region of Sweden. Sex. Reproduct. Health 2015, 6, 74–81. [Google Scholar] [CrossRef]
- Farra, H.A.A.; Shalaby, H.S.; Fahmy, A.A.; Nawara, M. The Safety and Efficacy of Transcutaneous Nerve Stimulation (TENS) in Reducing Vaginal Delivery Labor Pain: Randomized Controlled Clinical Trial. Open J. Obstet. Gynecol. 2022, 10, 657–670. [Google Scholar] [CrossRef]
- Báez-Suárez, A.; Martín-Castillo, E.; García-Andújar, J.; García-Hernández, J.Á.; Quintana-Montesdeoca, M.P.; Loro-Ferrer, J.F. Evaluation of different doses of transcutaneous nerve stimulation for pain relief during labour: A randomized controlled trial. Trials 2018, 19, 652. [Google Scholar] [CrossRef]
- Santana, L.S.; Gallo, R.B.S.; Quintana, S.M.; Duarte, G.; Jorge, C.H.; Marcolin, A.C. Applying a physiotherapy protocol to women during the active phase of labor improves obstetrical outcomes: A randomized clinical trial. Am. J. Obstet. Gynecol. Glob. Rep. 2022, 2, 100125. [Google Scholar] [CrossRef]
- Gibson, W.; Wand, B.M.; O’Connell, N.E. Transcutaneous electrical nerve stimulation (TENS) for neuropathic pain in adults. Cochrane Database Syst. Rev. 2017, 9, CD011976. [Google Scholar] [CrossRef]
- Vance, C.G.T.; Dailey, D.L.; Chimenti, R.L.; Van Gorp, B.J.; Crofford, L.J.; Sluka, K.A. Using TENS for Pain Control: Update on the State of the Evidence. Medicina 2022, 58, 1332. [Google Scholar] [CrossRef]
- Patel, P.; Green, M.; Tram, J.; Wang, E.; Murphy, M.; Abd-Elsayed, A.A.; Chakravarthy, K. Latest Advancements in Transcutaneous Electrical Nerve Stimulation (TENS) and Electronic Muscle Stimulation (EMS): Revisiting an Established Therapy with New Possibilities. J. Pain. Res. 2025, 18, 137–153. [Google Scholar] [CrossRef]
- Buckley, S.J. Executive Summary of Hormonal Physiology of Childbearing: Evidence and Implications for Women, Babies, and Maternity Care. J. Perinat. Educ. 2015, 24, 145–153. [Google Scholar] [CrossRef]
- Shahoei, R.; Shahghebi, S.; Rezaei, M.; Naqshbandi, S. The effect of transcutaneous electrical nerve stimulation on the severity of labor pain among nulliparous women: A clinical trial. Complement. Ther. Clin. Pract. 2017, 28, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Samadzadeh, S.; Rezavand, N.; Yari, M.; Rezaei, M.; Faizmahdavi, H.; Hematti, M. Comparison of Entonox and transcutaneous electrical nerve stimulation (TENS) in labor pain. J. Med. Biomed. Sci. 2017, 6, 11–16. [Google Scholar] [CrossRef]
- Takahashi, T. Sensory Stimulation of Oxytocin Release Is Associated With Stress Management and Maternal Care. Front. Psychol. 2021, 11, 588068. [Google Scholar] [CrossRef]
- Berta, M.; Lindgren, H.; Christensson, K.; Mekonnen, S.; Adefris, M. Effect of maternal birth positions on duration of second stage of labor: Systematic review and meta-analysis. BMC Pregnancy Childbirth 2019, 19, 466. [Google Scholar] [CrossRef]
- Sulu, R.; Akbas, M.; Cetiner, S. Effects of transcutaneous electrical nerve stimulation applied at different frequencies during labor on hormone levels, labor pain perception, and anxiety: A randomized placebo-controlled single-blind clinical trial. Eur. J. Integr. Med. 2022, 52, 102124. [Google Scholar] [CrossRef]
- Sluka, K.A.; Walsh, D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J. Pain. 2003, 4, 109–121. [Google Scholar] [CrossRef]
- Johnson, M.I.; Jones, G.; Paley, C.A.; Wittkopf, P.G. The clinical efficacy of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain: A protocol for a meta-analysis of randomised controlled trials (RCTs). BMJ Open 2019, 9, e029999. [Google Scholar] [CrossRef]
- Enomoto, Y.; He, S.; Huang, S.Y.; Yu, W. Effect of changes in Skin Thickness on pain-relief Transcutaneous Electrical Nerve Stimulation (TENS). In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 6504–6510. [Google Scholar] [CrossRef]
- Alizadeh-Dibazari, Z.; Abdolalipour, S.; Mirghafourvand, M. The effect of prenatal education on fear of childbirth, pain intensity during labour and childbirth experience: A scoping review using systematic approach and meta-analysis. BMC Pregnancy Childbirth 2023, 23, 541. [Google Scholar] [CrossRef]
- Olza, I.; Uvnas-Moberg, K.; Ekström-Bergström, A.; Leahy-Warren, P.; Karlsdottir, S.I.; Nieuwenhuijze, M.; Villarmea, S.; Hadjigeorgiou, E.; Kazmierczak, M.; Spyridou, A.; et al. Birth as a neuro-psycho-social event: An integrative model of maternal experiences and their relation to neurohormonal events during childbirth. PLoS ONE 2020, 15, e0230992. [Google Scholar] [CrossRef]
- Jones, L.; Othman, M.; Dowswell, T.; Alfirevic, Z.; Gates, S.; Newburn, M.; Jordan, S.; Lavender, T.; Neilson, J.P. Pain management for women in labour: An overview of systematic reviews. Cochrane Database Syst. Rev. 2012, 5, CD009234. [Google Scholar] [CrossRef]
- Cluett, E.R.; Burns, E.; Cuthbert, A. Immersion in water during labour and birth. Cochrane Database Syst. Rev. 2018, 5, CD000111. [Google Scholar] [CrossRef]
- Ergin, A.; Aşci, Ö.; Bal, M.D.; Öztürk, G.G.; Karaçam, Z. The use of hydrotherapy in the first stage of labour: A systematic review and meta-analysis. Int. J. Nurs. Pract. 2024, 30, e13192. [Google Scholar] [CrossRef]
- Gallo, R.B.S.; Santana, L.S.; Marcolin, A.C.; Duarte, G.; Quintana, S.M. Sequential application of non-pharmacological interventions reduces the severity of labour pain, delays use of pharmacological analgesia, and improves some obstetric outcomes: A randomised trial. J. Physiother. 2018, 64, 33–40. [Google Scholar] [CrossRef]
- Elbohoty, A.E.; Abd-Elrazek, H.; Abd-El-Gawad, M.; Salama, F.; El-Shorbagy, M.; Abd-El-Maeboud, K.H. Intravenous infusion of paracetamol versus intravenous pethidine as an intrapartum analgesic in the first stage of labor. Int. J. Gynaecol. Obstet. 2012, 118, 7–10. [Google Scholar] [CrossRef]
- Kaur Makkar, J.; Jain, K.; Bhatia, N.; Jain, V.; Mal Mithrawal, S. Comparison of analgesic efficacy of paracetamol and tramadol for pain relief in active labor. J. Clin. Anesth. 2015, 27, 159–163. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Range; Mean (SD)/(n%) |
|---|---|
| Maternal age (years) | 18–44; 30.58 (4.45) |
| Gestational age (weeks) | 35–41; 39.04 (1.16) |
| Gravidity | 1–6; 1.706 (0.965) |
| Parity | 1–4; 1.517 (0.739) |
| Primiparous | 372 (61.08) |
| Multiparous | 237 (38.92) |
| GDM * | 45 (7.39) |
| PROM ** | 124 (20.36) |
| Spontaneous delivery | 222 (36.45) |
| Induced delivery | 387 (63.55) |
| Vacuum extraction | 20 (3.28) |
| VBAC *** | 5 (0.82) |
| Oxytocin | 314 (51.56) |
| Entonox (N2O + O2) | 319 (52.38) |
| Water immersion | 290 (47.62) |
| TENS | 203 (33.33) |
| Duration 1st stage (minutes) | 35–770; 230.25 (115.03) |
| Duration 2nd stage (minutes) | 2–158; 36.22 (29.07) |
| Delivery at night | 145 (23.81) |
| Delivery during the day | 464 (76.19) |
| Episiotomy | 349 (57.30) |
| Perineal tearing (I–IV) | 129 (21.19) |
| Intact perineum | 131 (21.51) |
| Birth weight (grams) | 2650–4750; 3384.58 (400.47) |
| Umbilical cord blood pH | 7.045–7.535; 7.35 (0.07) |
| Variable | Non-TENS (n = 406) | TENS (n = 203) | p | Statistical Test * | |
|---|---|---|---|---|---|
| Maternal age (years) | 30.55 (4.48 SD) | 30.65 (4.41 SD) | 0.792 | T | |
| Gestational age (weeks) | 39.03 (1.15 SD) | 39.08 (1.19 SD) | 0.415 | W | |
| Parity | 1.52 (0.75 SD) | 1.51 (0.71 SD) | 0.994 | C | |
| Primiparous | No | 157 (38.67%) | 80 (39.41%) | 0.93 | C |
| Yes | 249 (61.33%) | 123 (60.59%) | |||
| GDM | No | 377 (92.86%) | 187 (92.12%) | 0.869 | C |
| Yes | 29 (7.14%) | 16 (7.88%) | |||
| PROM | No | 336 (82.76%) | 149 (73.40%) | 0.009 | C |
| Yes | 70 (17.24%) | 54 (26.60%) | |||
| Spontaneous delivery | No | 262 (65.76%) | 125 (64.04%) | 0.741 | C |
| Yes | 144 (34.24%) | 78 (35.96%) | |||
| Vacuum extraction | No | 392 (96.55%) | 197 (97.04%) | 0.936 | C |
| Yes | 14 (3.45%) | 6 (2.96%) | |||
| VBAC | No | 403 (99.26%) | 201 (99.01%) | 1 | C |
| Yes | 3 (0.74%) | 2 (0.99%) | |||
| Entonox (N2O + O2) | No | 246 (60.59%) | 44 (21.67%) | <0.001 | C |
| Yes | 160 (39.41%) | 159 (78.33%) | |||
| Oxytocin | No | 203 (50.00%) | 92 (45.32%) | 0.316 | C |
| Yes | 203 (50.00%) | 111 (54.68%) | |||
| Water immersion | No | 226 (55.67%) | 93 (45.81%) | 0.027 | C |
| Yes | 180 (44.33%) | 110 (54.19%) | |||
| Duration 1st stage (minutes) | 222.71 (109.91 SD) | 245.33 (123.54 SD) | 0.036 | W | |
| Duration 2nd stage (minutes) | 35.52 (28.91 SD) | 37.64 (29.41 SD) | 0.260 | W | |
| Delivery at night | 95 (23.40 SD) | 50 (24.63 SD) | 0.814 | C | |
| Delivery during the day | 311 (76.60 SD) | 153 (75.37 SD) | |||
| Episiotomy | No | 166 (40.89%) | 94 (46.31%) | 0.235 | C |
| Yes | 240 (59.11%) | 109 (53.69%) | |||
| Perineal tearing (I–IV) | No | 329 (81.03%) | 151 (74.38%) | 0.083 | C |
| Yes | 77 (18.97%) | 52 (25.62%) | |||
| Intact perineum | No | 318 (78.33%) | 160 (78.82%) | 0.972 | C |
| Yes | 88 (21.67%) | 43 (21.18%) | |||
| Birth weight (grams) | 3380.15 (369.64 SD) | 3393.45 (456.78 SD) | 0.699 | T | |
| Umbilical cord blood pH | 7.35 (0.07 SD) | 7.36 (0.07 SD) | 0.697 | W | |
| Umbilical cord blood pH < 7.2 | No | 392 (96.55%) | 201 (99.01%) | 0.128 | C |
| Yes | 14 (3.45%) | 2 (0.99%) |
| Variable | Estimate | SD | T | p | 95% CI |
|---|---|---|---|---|---|
| Primiparity | 89.460 | 8.720 | 10.259 | <0.001 | 72.334 |
| Water immersion | 8.708 | 10.552 | 0.825 | 0.410 | −12.015 |
| TENS | −3.996 | 13.574 | −0.294 | 0.769 | −30.653 |
| Entonox (N2O + O2) | −0.483 | 9.225 | −0.052 | 0.958 | −18.599 |
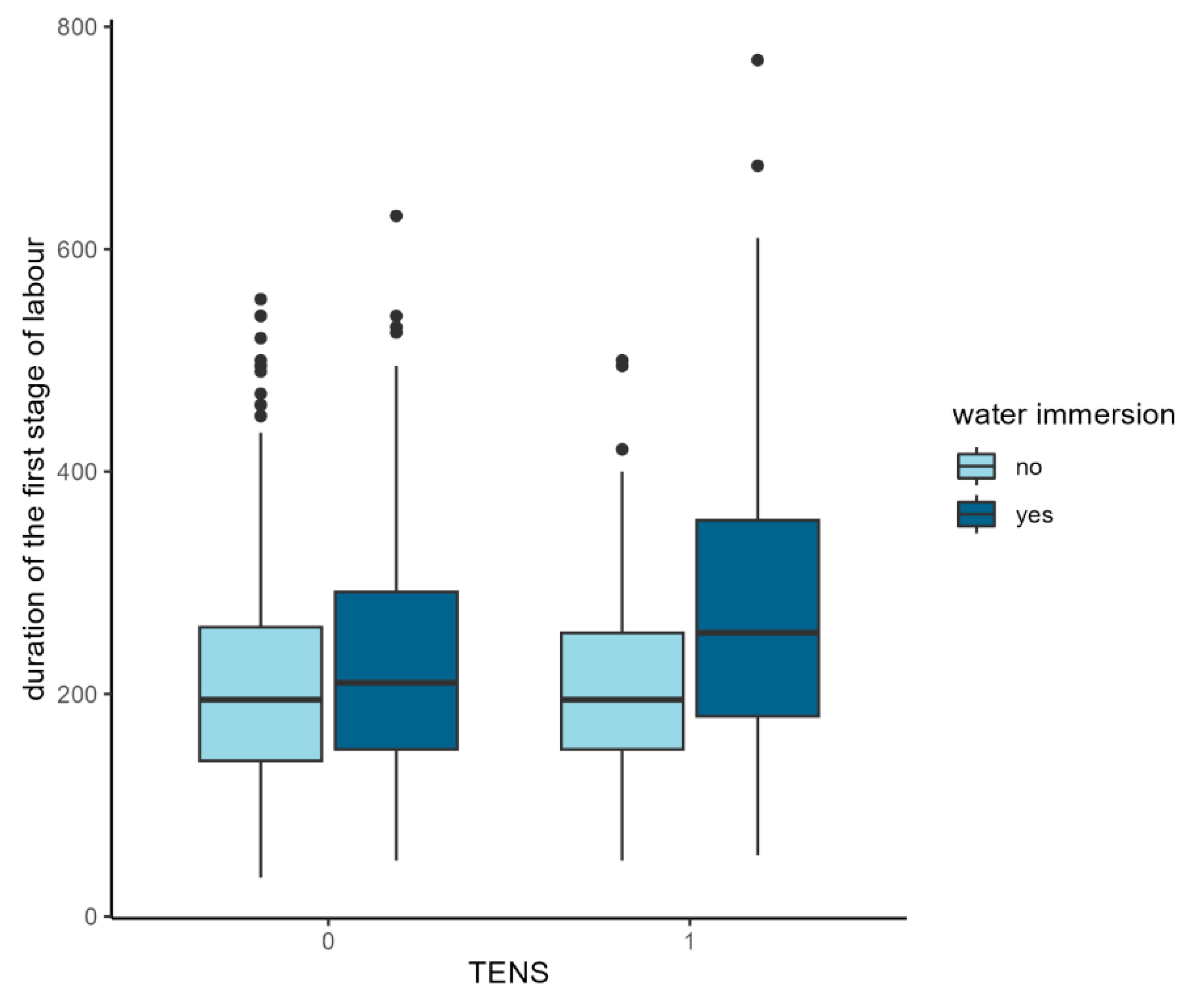
| Water immersion–TENS | 49.116 | 18.121 | 2.710 | 0.007 | 13.528 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalska, A.; Blazuk-Fortak, A.; Gladys-Jakubczyk, A.; Wolder, D.; Swiercz, G. The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on the Consecutive Stages of Labour and Perinatal Outcomes—A Retrospective Cohort Study. J. Clin. Med. 2025, 14, 3445. https://doi.org/10.3390/jcm14103445
Michalska A, Blazuk-Fortak A, Gladys-Jakubczyk A, Wolder D, Swiercz G. The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on the Consecutive Stages of Labour and Perinatal Outcomes—A Retrospective Cohort Study. Journal of Clinical Medicine. 2025; 14(10):3445. https://doi.org/10.3390/jcm14103445
Chicago/Turabian StyleMichalska, Agata, Anna Blazuk-Fortak, Aleksandra Gladys-Jakubczyk, Daniel Wolder, and Grzegorz Swiercz. 2025. "The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on the Consecutive Stages of Labour and Perinatal Outcomes—A Retrospective Cohort Study" Journal of Clinical Medicine 14, no. 10: 3445. https://doi.org/10.3390/jcm14103445
APA StyleMichalska, A., Blazuk-Fortak, A., Gladys-Jakubczyk, A., Wolder, D., & Swiercz, G. (2025). The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on the Consecutive Stages of Labour and Perinatal Outcomes—A Retrospective Cohort Study. Journal of Clinical Medicine, 14(10), 3445. https://doi.org/10.3390/jcm14103445