

Current Trends and Future Directions in Lumbar Spine Surgery: A Review of Emerging Techniques and Evolving Management Paradigms

 , , , and
, , , and 
Abstract
1. Introduction
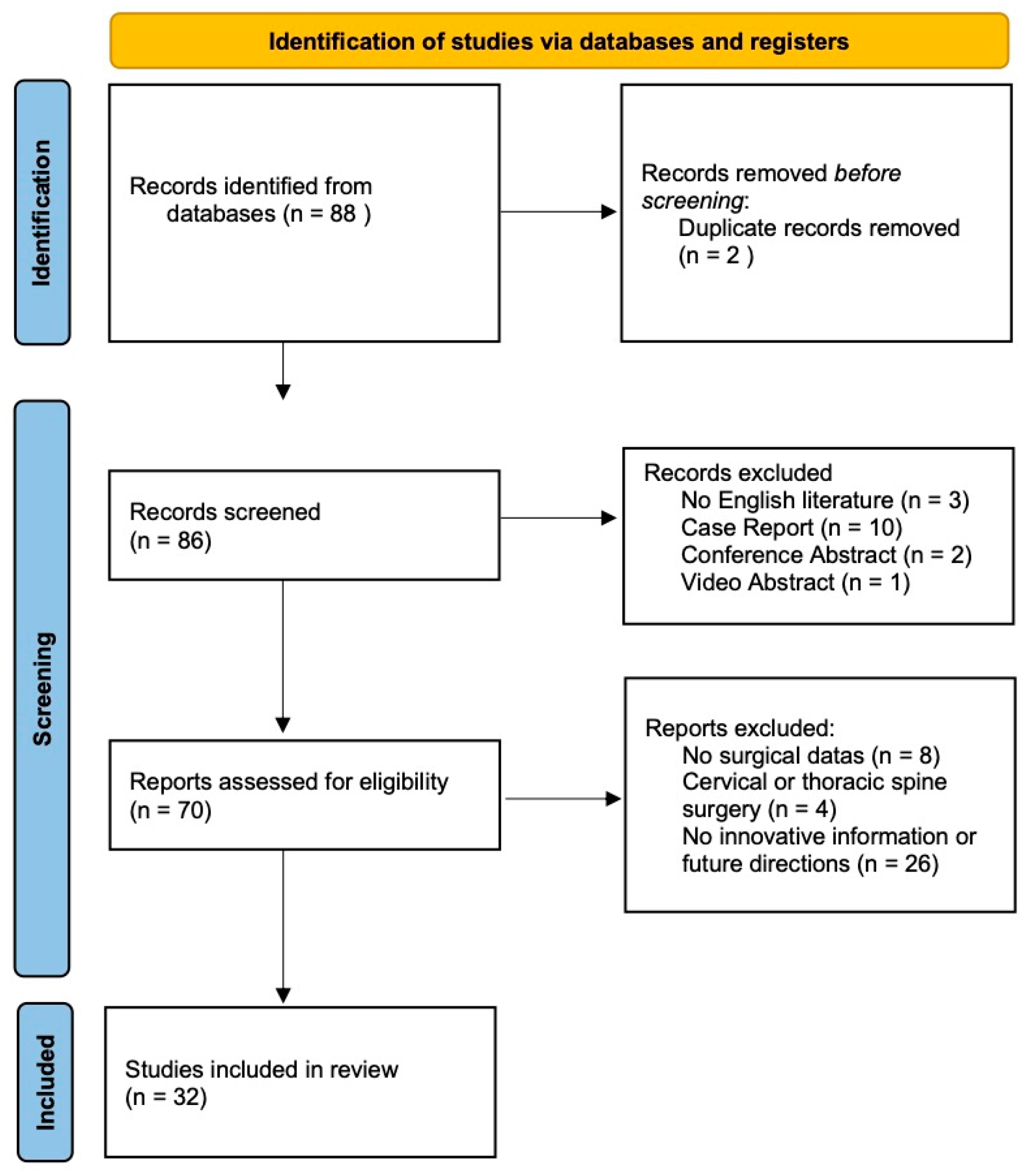
2. Materials and Methods
2.1. Study Design and Search Strategy
2.2. Inclusion Criteria
- -
- Published in a peer-reviewed journal indexed in PubMed from February 2020 onward.
- -
- Focused on lumbar spine surgery, addressing degenerative conditions, deformity correction, or other lumbar pathologies.
- -
- Utilized advanced technologies, including robotic-assisted surgery, computer navigation, AR, AI, or MIS techniques such as full-endoscopic discectomy, percutaneous instrumentation, and lateral/oblique lumbar interbody fusion (XLIF/OLIF).
- -
- Reported relevant clinical and surgical outcomes, such as accuracy of instrumentation, perioperative metrics (operative time, blood loss, and hospital stay), complication rates, and functional outcomes (pain scores, disability indices, and fusion rates).
- -
- Study types: randomized controlled trials (RCTs), prospective or retrospective comparative studies, systematic reviews, meta-analyses, and large case series were included if higher-level evidence was lacking (e.g., for AR or AI applications where RCT data remain sparse).
2.3. Exclusion Criteria
- -
- Were case reports or small case series without comparative data.
- -
- Were conference abstracts or non-peer-reviewed sources.
- -
- Focused on cervical or thoracic spine surgery, unless findings were generalizable to lumbar procedures.
- -
- Were review papers that did not provide new data (these were used for background information only).
- -
- Contained overlapping patient cohorts—in such cases, the most comprehensive or recent study was selected to avoid duplication.
- -
- Non-English-language publications.
2.4. Study Selection and Data Extraction
3. Results
3.1. Technological Innovations in Lumbar Spine Surgery
3.1.1. Robotic-Assisted Surgery
3.1.2. Intraoperative Navigation and Augmented Reality
3.1.3. Artificial Intelligence Applications
3.2. Minimally Invasive Techniques
3.2.1. Endoscopic and Percutaneous Spine Surgery
3.2.2. Lateral and Oblique Lumbar Interbody Fusion
3.3. Clinical and Functional Outcomes of New Techniques
3.3.1. Postoperative Pain
3.3.2. Disability and Functional Recovery
3.3.3. Fusion Rates, Radiographic Outcomes, and Infection Rates
3.3.4. Recovery Time and Return to Activity
3.3.5. Patient Satisfaction and Quality of Life
3.3.6. Durability and Reoperations
3.3.7. Learning Curve of Minimally Invasive Spine Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LSS | Lumbar Spine Surgery |
| AI | Artificial Intelligence |
| AR | Augmented Reality |
| MIS | Minimally Invasive Surgery |
| RCT | Randomized Controlled Trial |
| XLIF | Extreme Lateral Interbody Fusion |
| OLIF | Oblique Lateral Interbody Fusion |
| AMSTAR | Assessing the Methodological of Systematic Reviews |
| 3D | Three Dimensions |
| CT | Computer Tomography |
| OP | Operative Room |
| ODI | Oswestry Disability Index |
| PTED | Percutaneous Transforaminal Endoscopic Discectomy |
| TLIF | Transforaminal Lumbar Interbody Fusion |
| PLIF | Posterior Lumbar Interbody Fusion |
| ALIF | Anterior Lumbar Interbody Fusion |
| SF-36 | Short Form 36 |
| LOS | Length of Hospital Stay |
References
- Page, P.S.; Ammanuel, S.G.; Josiah, D.T. Evaluation of Endoscopic Versus Open Lumbar Discectomy: A Multi-Center Retrospective Review Utilizing the American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) Database. Cureus 2022, 14, e25202. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.X.; Huang, W.Q.; Li, H.Y.; Wang, H.S.; Guo, S.L.; Dong, J.; Chen, B.L.; Lin, Y.P. Clinical Efficacy of Robotic Spine Surgery: An Updated Systematic Review of 20 Randomized Controlled Trials. EFORT Open Rev. 2023, 8, 841–853. [Google Scholar] [CrossRef]
- Ton, A.; Hang, N.; Liu, W.; Liu, R.; Hsieh, P.C.; Wang, J.C.; Hah, R.J.; Alluri, R.K. Top 25 Most-Cited Articles on Robotic-Assisted Lumbar Spine Surgery. Int. J. Spine Surg. 2024, 18, 37–46. [Google Scholar] [CrossRef]
- Shahi, P.; Maayan, O.; Shinn, D.; Dalal, S.; Song, J.; Araghi, K.; Melissaridou, D.; Vaishnav, A.; Shafi, K.; Pompeu, Y.; et al. Floor-Mounted Robotic Pedicle Screw Placement in Lumbar Spine Surgery: An Analysis of 1050 Screws. Neurospine 2023, 20, 577–586. [Google Scholar] [CrossRef]
- Komolafe, T.E.; Zhou, L.; Zhao, W.; Guo, J.; Li, Z.; Fan, Z.; Komolafe, B.F.; Wei, W.; Samuel, O.W. Advancing Robot-Guided Techniques in Lumbar Spine Surgery: A Systematic Review and Meta-Analysis. Expert Rev. Med. Devices 2024, 21, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Guo, J.; Ma, X.; Zhang, G.; Han, S.; Zhang, H.; Liu, H.; Chen, M.; Wang, Y. The Cortical Bone Trajectory Screw Technique Assisted by the Mazor Renaissance Robotic System as a Salvage Strategy for Failed Lumbar Spine Surgery: Technical Note and Case Series. J. Pain Res. 2023, 16, 2971–2980. [Google Scholar] [CrossRef]
- Karimi, H.; Taylor, N.; Patel, J.; Wiepert, L.; Riesenburger, R.I.; Kryzanski, J. Practice Pattern Variations in the Use of Neuromonitoring, Image Guidance, and Robotics for Lumbar Pedicle Screw Placement Based on a Nationwide Neurosurgery Survey. World Neurosurg. 2024, 192, e539–e546. [Google Scholar] [CrossRef]
- Gouzoulis, M.J.; Seddio, A.E.; Winter, A.D.; Jabbouri, S.S.; Zhu, J.R.; Rubio, D.R.; Varthi, A.G.; Grauer, J.N. Robotic-Assisted Versus Navigation-Assisted Posterior Lumbar Fusion: A National Database Study. Spine 2024, 49, 1483–1487. [Google Scholar] [CrossRef] [PubMed]
- Liounakos, J.I.; Khan, A.; Eliahu, K.; Mao, J.Z.; Good, C.R.; Pollina, J.; Haines, C.M.; Gum, J.L.; Schuler, T.C.; Jazini, E.; et al. Ninety-Day Complication, Revision, and Readmission Rates for Current-Generation Robot-Assisted Thoracolumbar Spinal Fusion Surgery: Results of a Multicenter Case Series. J. Neurosurg. Spine 2022, 36, 841–848. [Google Scholar] [CrossRef]
- Good, C.R.; Orosz, L.; Schroerlucke, S.R.; Cannestra, A.; Lim, J.Y.; Hsu, V.W.; Zahrawi, F.; Villalobos, H.J.; Ramirez, P.M.; Sweeney, T.; et al. Complications and Revision Rates in Minimally Invasive Robotic-Guided Versus Fluoroscopic-Guided Spinal Fusions: The MIS ReFRESH Prospective Comparative Study. Spine 2021, 46, 1661. [Google Scholar] [CrossRef]
- Chumnanvej, S.; Ariyaprakai, K.; Pillai, B.M.; Suthakorn, J.; Gurusamy, S.; Chumnanvej, S. Cost-Effectiveness of Robotic-Assisted Spinal Surgery: A Single-Center Retrospective Study. Laparosc. Endosc. Robot. Surg. 2023, 6, 147–153. [Google Scholar] [CrossRef]
- Heydar, A.M.; Tanaka, M.; Prabhu, S.P.; Komatsubara, T.; Arataki, S.; Yashiro, S.; Kanamaru, A.; Nanba, K.; Xiang, H.; Hieu, H.K. The Impact of Navigation in Lumbar Spine Surgery: A Study of Historical Aspects, Current Techniques and Future Directions. J. Clin. Med. 2024, 13, 4663. [Google Scholar] [CrossRef] [PubMed]
- Shahzad, H.; Saade, A.; Tse, S.; Simister, S.; Anthony Viola, I.; Muthu, S.; Singh, H.; Ambrosio, L.; Tavakoli, J.; Vetter, S.Y.; et al. Advancements and Challenges in Computer-Assisted Navigation for Cervical Spine Surgery: A Comprehensive Review of Perioperative Integration, Complications, and Emerging Technologies. Glob. Spine J. 2025, 21925682251329340. [Google Scholar] [CrossRef] [PubMed]
- La Rocca, G.; Mazzucchi, E.; Pignotti, F.; Nasto, L.A.; Galieri, G.; Rinaldi, P.; De Santis, V.; Pola, E.; Sabatino, G. Navigated, Percutaneous, Three-Step Technique for Lumbar and Sacral Screw Placement: A Novel, Minimally Invasive, and Maximally Safe Strategy. J. Orthop. Traumatol. 2023, 24, 32. [Google Scholar] [CrossRef]
- Burström, G.; Persson, O.; Edström, E.; Elmi-Terander, A. Augmented Reality Navigation in Spine Surgery: A Systematic Review. Acta Neurochir. 2021, 163, 843–852. [Google Scholar] [CrossRef]
- La Rocca, G.; Mazzucchi, E.; Pignotti, F.; Nasto, L.A.; Galieri, G.; Olivi, A.; De Santis, V.; Rinaldi, P.; Pola, E.; Sabatino, G. Intraoperative CT-Guided Navigation versus Fluoroscopy for Percutaneous Pedicle Screw Placement in 192 Patients: A Comparative Analysis. J. Orthop. Traumatol. 2022, 23, 44. [Google Scholar] [CrossRef]
- Heath, D.C.; Chang, H.K.; Chang, C.C.; Yang, H.C.; Tu, T.H.; Hsu, B.H.; Lin, M.C.; Wu, J.C.; Lin, C.M.; Huang, W.C.; et al. Comparison between Robot-Assisted and Navigation-Guided Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Multicenter Study. Neurosurg. Focus 2024, 57, E12. [Google Scholar] [CrossRef]
- Paramasivam Meenakshi Sundaram, P.; Peh, D.Y.Y.; Poh, J.W.; Kalanchiam, G.P.; Yap, W.M.Q.; Kaliya-Perumal, A.K.; Oh, J.Y.L. Does Robotic Spine Surgery Add Value to Surgical Practice over Navigation-Based Systems? A Study on Operating Room Efficiency. Medicina 2024, 60, 2112. [Google Scholar] [CrossRef]
- Shahi, P.; Vaishnav, A.; Araghi, K.; Shinn, D.; Song, J.; Dalal, S.; Melissaridou, D.; Mai, E.; Dupont, M.; Sheha, E.; et al. Robotics Reduces Radiation Exposure in Minimally Invasive Lumbar Fusion Compared with Navigation. Spine 2022, 47, 1279–1286. [Google Scholar] [CrossRef]
- Prabhu, M.C.; Jacob, K.C.; Patel, M.R.; Pawlowski, H.; Vanjani, N.; Singh, K. Is Intraoperative Navigation in Minimally Invasive Spine Surgery Cost-Effective? Mini-Invasive Surg. 2022, 6, 31. [Google Scholar] [CrossRef]
- Tovar, M.A.; Dowlati, E.; Zhao, D.Y.; Khan, Z.; Pasko, K.B.D.; Sandhu, F.A.; Voyadzis, J.M. Robot-Assisted and Augmented Reality-Assisted Spinal Instrumentation: A Systematic Review and Meta-Analysis of Screw Accuracy and Outcomes over the Last Decade. J. Neurosurg. Spine 2022, 37, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, A.; Alexander, T.; Mengaliyeva, A.; Kota, N.; Koneru, M. Augmented Reality in Minimally Invasive Spinal Interventions: Current Use and Future Directions. Cureus 2025, 17, e80119. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.Q.; Hsieh, C.T.; Hsu, W.E.; Tseng, C.S.; Chang, C.J. Two-Dimensional C-Arm Robotic Navigation System (i-Navi) in Spine Surgery: A Pilot Study. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 2281–2290. [Google Scholar] [CrossRef]
- Lee, N.J.; Lombardi, J.M.; Lehman, R.A. Artificial Intelligence and Machine Learning Applications in Spine Surgery. Int. J. Spine Surg. 2023, 17, S18–S25. [Google Scholar] [CrossRef]
- Wirries, A.; Geiger, F.; Hammad, A.; Oberkircher, L.; Blümcke, I.; Jabari, S. Artificial Intelligence Facilitates Decision-Making in the Treatment of Lumbar Disc Herniations. Eur. Spine J. 2021, 30, 2176–2184. [Google Scholar] [CrossRef]
- Liawrungrueang, W.; Cho, S.T.; Sarasombath, P.; Kim, I.; Kim, J.H. Current Trends in Artificial Intelligence-Assisted Spine Surgery: A Systematic Review. Asian Spine J. 2024, 18, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Purohit, G.; Choudhary, M.; Sinha, V.D. Use of Artificial Intelligence for the Development of Predictive Model to Help in Decision-Making for Patients with Degenerative Lumbar Spine Disease. Asian J. Neurosurg. 2022, 17, 274–279. [Google Scholar] [CrossRef]
- Davidar, A.D.; Jiang, K.; Weber-Levine, C.; Bhimreddy, M.; Theodore, N. Advancements in Robotic-Assisted Spine Surgery. Neurosurg. Clin. N. Am. 2024, 35, 263–272. [Google Scholar] [CrossRef]
- Saravi, B.; Zink, A.; Ülkümen, S.; Couillard-Despres, S.; Hassel, F.; Lang, G. Performance of Artificial Intelligence-Based Algorithms to Predict Prolonged Length of Stay after Lumbar Decompression Surgery. J. Clin. Med. 2022, 11, 4050. [Google Scholar] [CrossRef]
- Dietz, N.; Alkin, V.; Lieberman, I.; Manista, A.; Kim, T.; Johnson, J.P.; Drazin, D. Scoping Review of Robotics Technology in Spinal Surgery with Highlights of the Annual Seattle Science Foundation Course. Ann. Transl. Med. 2024, 12, 118. [Google Scholar] [CrossRef]
- Berg, B.; Gorosito, M.A.; Fjeld, O.; Haugerud, H.; Storheim, K.; Solberg, T.K.; Grotle, M. Machine Learning Models for Predicting Disability and Pain Following Lumbar Disc Herniation Surgery. JAMA Netw. Open 2024, 7, E2355024. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jung, J.Y.; Mahatthanatrakul, A.; Kim, J.S. Artificial Intelligence in Spinal Imaging and Patient Care: A Review of Recent Advances. Neurospine 2024, 21, 474–486. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Dong, H.; Xia, Q.; Wang, Y.; Zhu, L.; Hu, Z.; Xia, J.; Mao, Q.; Weng, Z.; Yi, J.; et al. A New Strategy for Intervertebral Disc Regeneration: The Synergistic Potential of Mesenchymal Stem Cells and Their Extracellular Vesicles with Hydrogel Scaffolds. Biomed. Pharmacother. 2024, 172, 116238. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Liu, X.; Wang, J.; Suo, M.; Zhang, J.; Sun, T.; Zhang, W.; Li, Z. Umbilical Cord Mesenchymal Stem Cells for Regenerative Treatment of Intervertebral Disc Degeneration. Front. Cell Dev. Biol. 2023, 11, 1215698. [Google Scholar] [CrossRef]
- Farag, M.; Rezk, R.; Hutchinson, H.; Zankevich, A.; Lucke-Wold, B. Intervertebral Disc Degeneration and Regenerative Medicine. Clin. Transl. Discov. 2024, 4, e289. [Google Scholar] [CrossRef]
- Munda, M.; Velnar, T. Stem Cell Therapy for Degenerative Disc Disease: Bridging the Gap between Preclinical Promise and Clinical Potential. Biomol. Biomed. 2024, 24, 210. [Google Scholar] [CrossRef]
- Croft, A.J.; Chanbour, H.; Chen, J.W.; Young, M.W.; Stephens, B.F. Implant Surface Technologies to Promote Spinal Fusion: A Narrative Review. Int. J. Spine Surg. 2023, 17, S35. [Google Scholar] [CrossRef]
- Smith, W.R.; Hudson, P.W.; Ponce, B.A.; Rajaram Manoharan, S.R. Nanotechnology in Orthopedics: A Clinically Oriented Review. BMC Musculoskelet. Disord. 2018, 19, 67. [Google Scholar] [CrossRef]
- Wu, B.; Tang, Y.; Wang, K.; Zhou, X.; Xiang, L. Nanostructured Titanium Implant Surface Facilitating Osseointegration from Protein Adsorption to Osteogenesis: The Example of TiO2 NTAs. Int. J. Nanomed. 2022, 17, 1865. [Google Scholar] [CrossRef]
- Noh, S.H.; Sung, K.; Byeon, H.E.; Kim, S.E.; Kim, K.N. Lactoferrin-Anchored Tannylated Mesoporous Silica Nanomaterials-Induced Bone Fusion in a Rat Model of Lumbar Spinal Fusion. Int. J. Mol. Sci. 2023, 24, 15782. [Google Scholar] [CrossRef]
- Wen, J.; Cai, D.; Gao, W.; He, R.; Li, Y.; Zhou, Y.; Klein, T.; Xiao, L.; Xiao, Y. Osteoimmunomodulatory Nanoparticles for Bone Regeneration. Nanomaterials 2023, 13, 692. [Google Scholar] [CrossRef] [PubMed]
- Momin, A.A.; Steinmetz, M.P. Evolution of Minimally Invasive Lumbar Spine Surgery. World Neurosurg. 2020, 140, 622–626. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.T. A Narrative Review of Development of Full-Endoscopic Lumbar Spine Surgery. Neurospine 2020, 17, S20–S33. [Google Scholar] [CrossRef] [PubMed]
- Pertile, M.E.; de Assunção Bicca, Y.; Maccari, P.M.; Neto, O.R.; Quintas, D.P.; Bertani, R.; Batista, S.; Koester, S.W.; Rusafa, E.; Flores de Barros Vasconcelos Fernandes Serra, M.V. Advancing Education in Endoscopic Spinal Navigation: Novel Methods and Technical Note. Cureus 2023, 15, e37017. [Google Scholar] [CrossRef]
- Liawrungrueang, W.; Cho, S.T.; Sharma, A.; Cholamjiak, W.; Wu, M.H.; Yau, L.C.; Park, H.J.; Lee, H.J. Clinical Outcomes and Patient Perspectives in Full Endoscopic Cervical Surgery: A Systematic Review. Neurospine 2025, 22, 81. [Google Scholar] [CrossRef]
- Persaud-Sharma, D.; Gunaratne, C.; Talati, J.; Philips, W.; Sohel, A.; Blake, A.; Vasilopoulos, T.; Kumar, S. Efficacy of Endoscopic Decompression Surgery for Treatment of Lumbar Spinal Stenosis. Interv. Pain Med. 2024, 3, 100391. [Google Scholar] [CrossRef] [PubMed]
- Shinn, D.; Mok, J.K.; Vaishnav, A.S.; Louie, P.K.; Sivaganesan, A.; Shahi, P.; Dalal, S.; Song, J.; Araghi, K.; Melissaridou, D.; et al. Recovery Kinetics after Commonly Performed Minimally Invasive Spine Surgery Procedures. Spine 2022, 47, 1489. [Google Scholar] [CrossRef]
- Balain, B.; Bhachu, D.S.; Gadkari, A.; Ghodke, A.; Kuiper, J.H. 2nd and 3rd Generation Full Endoscopic Lumbar Spine Surgery: Clinical Safety and Learning Curve. Eur. Spine J. 2023, 32, 2796–2804. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Phan, K. Minimally Invasive Spine. J. Spine Surg. 2020, 6, E1. [Google Scholar] [CrossRef]
- Gadjradj, P.S.; Harhangi, B.S.; Amelink, J.; Van Susante, J.; Kamper, S.; Van Tulder, M.; Peul, W.C.; Vleggeert-Lankamp, C.; Rubinstein, S.M. Percutaneous Transforaminal Endoscopic Discectomy Versus Open Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Spine 2021, 46, 538–549. [Google Scholar] [CrossRef]
- Jitpakdee, K.; Liu, Y.; Heo, D.H.; Kotheeranurak, V.; Suvithayasiri, S.; Kim, J. sung Minimally Invasive Endoscopy in Spine Surgery: Where Are We Now? Eur. Spine J. 2023, 32, 2755–2768. [Google Scholar] [CrossRef] [PubMed]
- Sivakanthan, S.; Hasan, S.; Hofstetter, C. Full-Endoscopic Lumbar Discectomy. Neurosurg. Clin. N. Am. 2020, 31, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.X.; Guo, S.J.; Meng, H.; Lin, J.S.; Yang, Y.; Fei, Q. Unilateral Biportal Endoscopic Spine Surgery for Lumbar Spinal Stenosis: A Systematic Review and Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 4998–5012. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.W.; Chang, K.E.; Shen, J.; Telfeian, A.E. Biportal Versus Uniportal Lumbar Decompression-Indications and Efficacy: A Review With Case Examples. Neurosurgery 2025, 96, S63–S68. [Google Scholar] [CrossRef]
- La Rocca, G.; Galieri, G.; Mazzucchi, E.; Pignotti, F.; Orlando, V.; Pappalardo, S.; Olivi, A.; Sabatino, G. The Three-Step Approach for Lumbar Disk Herniation with Anatomical Insights Tailored for the Next Generation of Young Spine Surgeons. J. Clin. Med. 2024, 13, 3571. [Google Scholar] [CrossRef]
- Enache, A.V.; Toader, C.; Onciul, R.; Costin, H.P.; Glavan, L.A.; Covache-Busuioc, R.A.; Corlatescu, A.D.; Ciurea, A.V. Surgical Stabilization of the Spine: A Clinical Review of Spinal Fractures, Spondylolisthesis, and Instrumentation Methods. J. Clin. Med. 2025, 14, 1124. [Google Scholar] [CrossRef]
- Sarikonda, A.; Sivaganesan, A.; Qureshi, S. Advanced Visualization in Minimally Invasive Spine Surgery: The Ergonomics, Economics, and Evolution of Camera-Based Tubes and Retractors. Int. J. Spine Surg. 2024, 18, S64–S70. [Google Scholar] [CrossRef]
- Ambrosio, L.; Muthu, S.; Cho, S.K.; Virk, M.S.; Cabrera, J.P.; Hsieh, P.C.; Demetriades, A.K.; Ćorluka, S.; Yoon, S.T.; Vadalà, G.; et al. Open Versus Minimally Invasive Spine Surgery in the Treatment of Single-Level Degenerative Lumbar Spondylolisthesis: An AO Spine Global Cross-Sectional Study. Neurospine 2025, 22, 40. [Google Scholar] [CrossRef]
- Miller, L.E.; Bhattacharyya, S.; Pracyk, J. Minimally Invasive Versus Open Transforaminal Lumbar Interbody Fusion for Single-Level Degenerative Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2020, 133, 358–365.e4. [Google Scholar] [CrossRef]
- Jacob, K.C.; Patel, M.R.; Hartman, T.J.; Nie, J.W.; Parsons, A.W.; Ribot, M.A.; Prabhu, M.; Pawlowski, H.; Vanjani, N.; Singh, K. Minimally Invasive Transforaminal Versus Lateral Lumbar Interbody Fusion for Degenerative Spinal Pathology Clinical Outcome Comparison in Patients with Predominant Back Pain. Clin. Spine Surg. 2024, 37, E441–E447. [Google Scholar] [CrossRef]
- Zhou, S.; Yang, Z.; Zhang, W.; Liu, S.; Xiao, Q.; Hou, G.; Chen, R.; Han, N.; Guo, J.; Liang, M.; et al. Development and Validation of a Predictive Model and Tool for Functional Recovery in Patients after Postero-Lateral Interbody Fusion. J. Orthop. Surg. Res. 2025, 20, 38. [Google Scholar] [CrossRef] [PubMed]
- Galieri, G.; Mazzucchi, E.; Pignotti, F.; Rinaldi, P.; De Santis, V.; La Rocca, G.; Sabatino, G. Lumbo-Sacral Pedicular Aplasia Diagnosis and Treatment: A Systematic Literature Review and Case Report. Br. J. Neurosurg. 2022, 38, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.H.; Yuan, Y.F.; Gao, H.R.; Liao, B.; Qian, J.X.; Yan, X.D. Comparative Study on the Technique and Efficacy of Microscope-Assisted MI-TLIF and Naked-Eye MI-TLIF in Lumbar Revision Surgery. J. Orthop. Surg. Res. 2024, 19, 101. [Google Scholar] [CrossRef]
- Lin, G.X.; Xu, W.B.; Kotheeranurak, V.; Chen, C.M.; Deng, Z.H.; Zhu, M.T. Comparison of Oblique and Transforaminal Approaches to Lumbar Interbody Fusion for Lumbar Degenerative Disease: An Updated Meta-Analysis. Front. Surg. 2023, 9, 1004870. [Google Scholar] [CrossRef]
- Li, X.Y.; Wang, Y.L.; Yang, S.; Liao, C.S.; Li, S.F.; Han, P.Y.; Han, P.F. Efficacy of Oblique Lumbar Interbody Fusion versus Transforaminal Lumbar Interbody Fusion in the Treatment of Lumbar Degenerative Diseases: A Systematic Review and Meta-Analysis. Arch. Orthop. Trauma Surg. 2023, 143, 5657–5670. [Google Scholar] [CrossRef]
- Ricciardi, L.; Piazza, A.; Capobianco, M.; Della Pepa, G.M.; Miscusi, M.; Raco, A.; Scerrati, A.; Somma, T.; Lofrese, G.; Sturiale, C.L. Lumbar Interbody Fusion Using Oblique (OLIF) and Lateral (LLIF) Approaches for Degenerative Spine Disorders: A Meta-Analysis of the Comparative Studies. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 1–7. [Google Scholar] [CrossRef]
- Byvaltsev, V.A.; Kalinin, A.A.; Pestryakov, Y.Y.; Aliyev, M.A.; Yuldashev, R.M.; Dyussembekov, Y.K.; Riew, K.D. Effect of Different Minimally Invasive Posterior Stabilization Techniques After Direct Lateral Interbody Fusion with Long-Term Clinical and Radiological Outcomes in Railway Workers: A Retrospective Single-Center Study. Glob. Spine J. 2025, 27, 21925682251331464. [Google Scholar] [CrossRef]
- Rocca, G.L.; Galieri, G.; Mazzucchi, E.; Pignotti, F.; Orlando, V.; Pappalardo, S.; Olivi, A.; Sabatino, G. The 3-Steps Approach for Lumbar Stenosis with Anatomical Insights, Tailored for Young Spine Surgeons. J. Pers. Med. 2024, 14, 985. [Google Scholar] [CrossRef] [PubMed]
- Mazzucchi, E.; La Rocca, G.; Cusumano, D.; Bazzu, P.; Pignotti, F.; Galieri, G.; Rinaldi, P.; De Santis, V.; Sabatino, G. The Role of Psychopathological Symptoms in Lumbar Stenosis: A Prediction Model of Disability after Lumbar Decompression and Fusion. Front. Psychol. 2023, 14, 1070205. [Google Scholar] [CrossRef]
- Kaye, A.D.; Edinoff, A.N.; Temple, S.N.; Kaye, A.J.; Chami, A.A.; Shah, R.J.; Dixon, B.M.; Alvarado, M.A.; Cornett, E.M.; Viswanath, O.; et al. A Comprehensive Review of Novel Interventional Techniques for Chronic Pain: Spinal Stenosis and Degenerative Disc Disease-MILD Percutaneous Image Guided Lumbar Decompression, Vertiflex Interspinous Spacer, MinuteMan G3 Interspinous-Interlaminar Fusion. Adv. Ther. 2021, 38, 4628–4645. [Google Scholar] [CrossRef]
- Galieri, G.; Orlando, V.; Mazzucchi, E.; Pignotti, F.; Cusumano, D.; Bazzu, P.; Mantini, S.; Altieri, R.; Barbarisi, M.; Olivi, A.; et al. Psychopathological Influences on Surgical and Clinical Outcomes in Lumbar Disk Herniation: Prediction Models and Literature Analysis. J. Pers. Med. 2025, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, T.F.; Shan, H.; Wan, Z.Y.; Wang, Z.; Viswanath, O.; Paladini, A.; Varrassi, G.; Wang, H.Q. Decompression Using Minimally Invasive Surgery for Lumbar Spinal Stenosis Associated with Degenerative Spondylolisthesis: A Review. Pain Ther. 2021, 10, 941. [Google Scholar] [CrossRef] [PubMed]
- Formica, M.; Vallerga, D.; Zanirato, A.; Cavagnaro, L.; Basso, M.; Divano, S.; Mosconi, L.; Quarto, E.; Siri, G.; Felli, L. Fusion Rate and Influence of Surgery-Related Factors in Lumbar Interbody Arthrodesis for Degenerative Spine Diseases: A Meta-Analysis and Systematic Review. Musculoskelet. Surg. 2020, 104, 1–15. [Google Scholar] [CrossRef]
- Kpegeol, C.K.; Jain, V.S.; Ansari, D.; Ammanuel, S.G.; Page, P.S.; Josiah, D.T. Surgical Site Infection Rates in Open versus Endoscopic Lumbar Spinal Decompression Surgery: A Retrospective Cohort Study. World Neurosurg. X 2024, 22, 100347. [Google Scholar] [CrossRef]
- Miyamoto, A.; Tanaka, M.; Flores, A.O.P.; Yu, D.; Jain, M.; Heng, C.; Komatsubara, T.; Arataki, S.; Oda, Y.; Shinohara, K.; et al. Predicting Surgical Site Infections in Spine Surgery: Association of Postoperative Lymphocyte Reduction. Diagnostics 2024, 14, 2715. [Google Scholar] [CrossRef]
- Mueller, K.; Zhao, D.; Johnson, O.; Sandhu, F.A.; Voyadzis, J.M. The Difference in Surgical Site Infection Rates between Open and Minimally Invasive Spine Surgery for Degenerative Lumbar Pathology: A Retrospective Single Center Experience of 1442 Cases. Oper. Neurosurg. 2019, 16, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Orlando, V.; Galieri, G.; Mazzucchi, E.; Pignotti, F.; Carcagnì, A.; Bazzu, P.; Altieri, R.; Barbarisi, M.; Olivi, A.; Sabatino, G.; et al. Comparative Analysis of Pedicle Screw Fixation and Interspinous Devices in Lumbar Spinal Fusion: Clinical and Surgical Outcomes in Degenerative Spine Conditions. J. Pers. Med. 2025, 15, 95. [Google Scholar] [CrossRef]
- La Rocca, G.; Orlando, V.; Galieri, G.; Mazzucchi, E.; Pignotti, F.; Cusumano, D.; Bazzu, P.; Olivi, A.; Sabatino, G. Mindfulness vs. Physiotherapy vs. Medical Therapy: Uncovering the Best Postoperative Recovery Method for Low Back Surgery Patients during the COVID-19 Pandemic-A Single Institution’s Experience. J. Pers. Med. 2024, 14, 917. [Google Scholar] [CrossRef]
- Hermansen, E.; Austevoll, I.M.; Hellum, C.; Storheim, K.; Myklebust, T.Å.; Aaen, J.; Banitalebi, H.; Anvar, M.; Rekeland, F.; Brox, J.I.; et al. Comparison of 3 Different Minimally Invasive Surgical Techniques for Lumbar Spinal Stenosis: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, E224291. [Google Scholar] [CrossRef]
- Shepard, N.; Cho, W. Recurrent Lumbar Disc Herniation: A Review. Glob. Spine J. 2019, 9, 202–209. [Google Scholar] [CrossRef]
- Bombieri, F.F.; Shafafy, R.; Elsayed, S. Complications Associated with Lumbar Discectomy Surgical Techniques: A Systematic Review. J. Spine Surg. 2022, 8, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Lee, S.; Kim, W.K.; Lee, S.G. Learning Curve for Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Systematic Review. Eur. Spine J. 2022, 31, 3551–3559. [Google Scholar] [CrossRef]
- Lee, K.H.; Yeo, W.; Soeharno, H.; Yue, W.M. Learning Curve of a Complex Surgical Technique: Minimally Invasive Transforaminal Lumbar Interbody Fusion (MIS TLIF). J. Spinal Disord. Tech. 2014, 27, E234–E240. [Google Scholar] [CrossRef]
- Wu, K.; Yun, Z.; Suvithayasiri, S.; Liang, Y.; Setiawan, D.R.; Kotheeranurak, V.; Jitpakdee, K.; Giordan, E.; Liu, Q.; Kim, J.S. Evolving Paradigms in Spinal Surgery: A Systematic Review of the Learning Curves in Minimally Invasive Spine Techniques. Neurospine 2024, 21, 1251–1275. [Google Scholar] [CrossRef] [PubMed]
- Pennington, Z.; Judy, B.F.; Zakaria, H.M.; Lakomkin, N.; Mikula, A.L.; Elder, B.D.; Theodore, N. Learning Curves in Robot-Assisted Spine Surgery: A Systematic Review and Proposal of Application to Residency Curricula. Neurosurg. Focus 2022, 52, E3. [Google Scholar] [CrossRef]
- Katsuura, Y.; Colón, L.F.; Perez, A.A.; Albert, T.J.; Qureshi, S.A. A Primer on the Use of Artificial Intelligence in Spine Surgery. Clin. Spine Surg. 2021, 34, 316–321. [Google Scholar] [CrossRef]
- Passias, P.G.; Brown, A.E.; Alas, H.; Bortz, C.A.; Pierce, K.E.; Hassanzadeh, H.; Labaran, L.A.; Puvanesarajah, V.; Vasquez-Montes, D.; Wang, E.; et al. A Cost Benefit Analysis of Increasing Surgical Technology in Lumbar Spine Fusion. Spine J. 2021, 21, 193–201. [Google Scholar] [CrossRef]
- Austevoll, I.M.; Hermansen, E.; Fagerland, M.W.; Storheim, K.; Brox, J.I.; Solberg, T.; Rekeland, F.; Franssen, E.; Weber, C.; Brisby, H.; et al. Decompression with or without Fusion in Degenerative Lumbar Spondylolisthesis. N. Engl. J. Med. 2021, 385, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Gadjradj, P.S.; Basilious, M.; Goldberg, J.L.; Sommer, F.; Navarro-Ramirez, R.; Mykolajtchuk, C.; Ng, A.Z.; Medary, B.; Hussain, I.; Härtl, R. Decompression Alone versus Decompression with Fusion in Patients with Lumbar Spinal Stenosis with Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis. Eur. Spine J. 2023, 32, 1054–1067. [Google Scholar] [CrossRef]
- Tozawa, K.; Matsubayashi, Y.; Kato, S.; Doi, T.; Taniguchi, Y.; Kumanomido, Y.; Higashikawa, A.; Yosihida, Y.; Kawamura, N.; Sasaki, K.; et al. Surgical Outcomes between Posterior Decompression Alone and Posterior Decompression with Fusion Surgery among Patients with Meyerding Grade 2 Degenerative Spondylolisthesis: A Multicenter Cohort Study. BMC Musculoskelet. Disord. 2022, 23, 902. [Google Scholar] [CrossRef]
- Wei, F.L.; Zhou, C.P.; Gao, Q.Y.; Du, M.R.; Gao, H.R.; Zhu, K.L.; Li, T.; Qian, J.X.; Yan, X.D. Decompression Alone or Decompression and Fusion in Degenerative Lumbar Spondylolisthesis. EClinicalMedicine 2022, 51, 101559. [Google Scholar] [CrossRef]
- Perfetti, D.C.; Kisinde, S.; Rogers-Lavanne, M.P.; Satin, A.M.; Lieberman, I.H. Robotic Spine Surgery: Past, Present, and Future. Spine 2022, 47, 909–921. [Google Scholar] [CrossRef] [PubMed]
- Matur, A.V.; Palmisciano, P.; Duah, H.O.; Chilakapati, S.S.; Cheng, J.S.; Adogwa, O. Robotic and Navigated Pedicle Screws Are Safer and More Accurate than Fluoroscopic Freehand Screws: A Systematic Review and Meta-Analysis. Spine J. 2023, 23, 197–208. [Google Scholar] [CrossRef]

{kind=link}
| Technology | Key Advantages | Current Evidence (Last 5 Years) |
|---|---|---|
| Robotic-Assisted Surgery | High precision in pedicle screw placement (≈92–94% accuracy vs. ~70% freehand). | Accuracy: Significantly higher Grade A screw placement vs. conventional freehand. |
| Reduced intraoperative blood loss and radiation exposure in some studies. | Perioperative: Less blood loss and shorter hospital stays observed in RCT meta-analysis. No increase in overall OR time. | |
| Facilitates minimally invasive approaches (percutaneous instrumentation). | Outcomes: No improvement in 90-day or long-term clinical outcomes versus non-robotic surgery in matched comparisons. Similar pain relief and fusion rates. | |
| Limitations: High initial cost; learning curve; few studies on cost-benefit (one analysis shows cost-effectiveness if revisions are reduced). | ||
| Intraoperative Navigation (Conventional 3D navigation systems) | Improves screw placement accuracy over fluoroscopy alone. | Accuracy: Established improvement in pedicle screw accuracy vs. freehand. |
| Avoids reliance on surgeon’s anatomic estimates, enhancing safety in complex anatomy. | Workflow: Can increase setup time and requires surgeon to look away to a separate screen, which may disrupt workflow. | |
| Outcomes: Associated with reduced screw misplacement-related complications, but direct impact on long-term outcomes is unclear. Widely adopted especially in deformity and revision cases. | ||
| Augmented Reality Navigation | Projects navigation cues into surgeon’s field of view (via headsets or displays) resulting in improved ergonomics (surgeon keeps eyes on patient). | Accuracy: Non-inferior to standard navigation; AR-guided pedicle screw placement accuracy comparable to conventional navigation and far better than freehand. Early head-mounted AR studies report accuracy on par with navigation (differences not statistically significant). |
| Workflow efficiency: Easier, more intuitive instrument guidance, potentially shorter learning curve for navigation. | Workflow: Qualitatively improved; surgeons report greater ease and faster confirmation of trajectories. AR deemed a “meaningful addition” to traditional methods. | |
| May reduce need for fluoroscopy (lower radiation) by providing continuous visual guidance. | Outcomes: No clinical outcome or cost data yet. Studies so far are small; need prospective trials to confirm any reduction in operative time or complication rates. | |
| Artificial Intelligence (AI) (machine learning for planning, guidance, and decision support) | Preoperative: Automates image analysis and surgical planning (3D reconstructions and optimal screw trajectories). | Feasibility: AI-driven tools have been implemented in pilot studies with satisfactory accuracy and safety profiles (e.g., AI planning yielding proper screw placement and AI-assisted imaging matching expert readings). |
| Intraoperative: Enhances robotics and navigation (e.g., adaptive trajectory adjustments and real-time tissue recognition). | Radiation/Precision: AI-assisted navigation shown to reduce reliance on fluoroscopy and maintain or improve accuracy versus standard techniques. | |
| Postoperative: Predicts outcomes and complication risks (personalized prognostics). | Clinical impact: No proven superiority in patient outcomes yet. Lacks RCTs; current evidence (11 studies review) shows no clear outcome advantage of AI assistance, although processes are improved. | |
| Can integrate with AR/VR to improve simulation and training. | Future: Rapidly evolving; expected to enhance surgeon decision-making and possibly enable semi-autonomous surgeries. |
| Procedures | Surgical Outcome Measures | Key Findings |
|---|---|---|
| Endoscopic Discectomy vs. Open Microdiscectomy | Long-term leg pain relief and functional improvement | No significant difference. Both approaches yield comparable outcomes for sciatica at 6–12 months. |
| Hospital Stay | Endoscopic shorter (e.g., ~0.8 vs. 1.1 days) with more same day discharges. | |
| Complications | Endoscopic has lower risk of adverse events (0.6% vs. 3.4% in one large series), including lower infection rates. | |
| Recovery | Faster early mobility and less postoperative pain medication reported with endoscopic technique in several studies (due to minimal muscle disruption). | |
| MIS TLIF vs. Open TLIF (single-level fusion) | Perioperative | Less blood loss with MIS (~200 mL reduction). |
| Shorter hospitalization by ~2 days (earlier ambulation and discharge). | ||
| Fluoroscopy use is higher in MIS (by ~48 s) due to percutaneous screw placement. | ||
| Complications | No significant difference in overall complication rates. MIS approach does not increase neurological or hardware-related complications when performed with navigation/experience. | |
| Fusion Rate | Equivalent between groups (~90% at 12 months). MIS does not compromise bony fusion healing. | |
| Clinical Outcomes | Similar pain scores at 1 year (both groups improve greatly). ODI slightly better in MIS group (by ~3 points), indicating a small functional benefit. Long-term outcomes (up to 5 years) show no differences in pain/disability trajectories. | |
| Lateral/Oblique Fusion (XLIF/OLIF) vs. Posterior Fusion (TLIF) | Operative Time | No significant difference (lateral approaches as efficient as TLIF for single level). |
| Blood Loss | Lower in lateral (XLIF/OLIF)—often by 150–250 mL less than TLIF. | |
| Hospital Stay | Shorter with XLIF/OLIF (mean 1–2 days shorter) due to reduced pain and quicker mobilization. | |
| Pain and Disability | Faster early improvement in OLIF vs. TLIF. Lower VAS back pain at 3 months and better ODI at 3 months and final follow-up (2–3 point advantage). Leg pain relief similar between groups. | |
| Fusion and Alignment | Fusion rates high and comparable. XLIF/OLIF yield greater disc height and foraminal height restoration, aiding indirect decompression. Similar or slightly better segmental lordosis gain vs. TLIF, depending on levels fused. | |
| Complications | Overall rates similar, but profile differs. OLIF: risk of vascular injury (~3%) higher than TLIF (near zero). XLIF: risk of lumbar plexus neuropraxia (transient thigh numbness/weakness) ~10–20% vs. much lower in TLIF. No significant difference in infection rates (both are low due to minimal incisions). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galieri, G.; Orlando, V.; Altieri, R.; Barbarisi, M.; Olivi, A.; Sabatino, G.; La Rocca, G. Current Trends and Future Directions in Lumbar Spine Surgery: A Review of Emerging Techniques and Evolving Management Paradigms. J. Clin. Med. 2025, 14, 3390. https://doi.org/10.3390/jcm14103390
Galieri G, Orlando V, Altieri R, Barbarisi M, Olivi A, Sabatino G, La Rocca G. Current Trends and Future Directions in Lumbar Spine Surgery: A Review of Emerging Techniques and Evolving Management Paradigms. Journal of Clinical Medicine. 2025; 14(10):3390. https://doi.org/10.3390/jcm14103390
Chicago/Turabian StyleGalieri, Gianluca, Vittorio Orlando, Roberto Altieri, Manlio Barbarisi, Alessandro Olivi, Giovanni Sabatino, and Giuseppe La Rocca. 2025. "Current Trends and Future Directions in Lumbar Spine Surgery: A Review of Emerging Techniques and Evolving Management Paradigms" Journal of Clinical Medicine 14, no. 10: 3390. https://doi.org/10.3390/jcm14103390
APA StyleGalieri, G., Orlando, V., Altieri, R., Barbarisi, M., Olivi, A., Sabatino, G., & La Rocca, G. (2025). Current Trends and Future Directions in Lumbar Spine Surgery: A Review of Emerging Techniques and Evolving Management Paradigms. Journal of Clinical Medicine, 14(10), 3390. https://doi.org/10.3390/jcm14103390