
Endoscopic Bridging Stent Placement Improves Bile Leaks After Hepatic Surgery
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
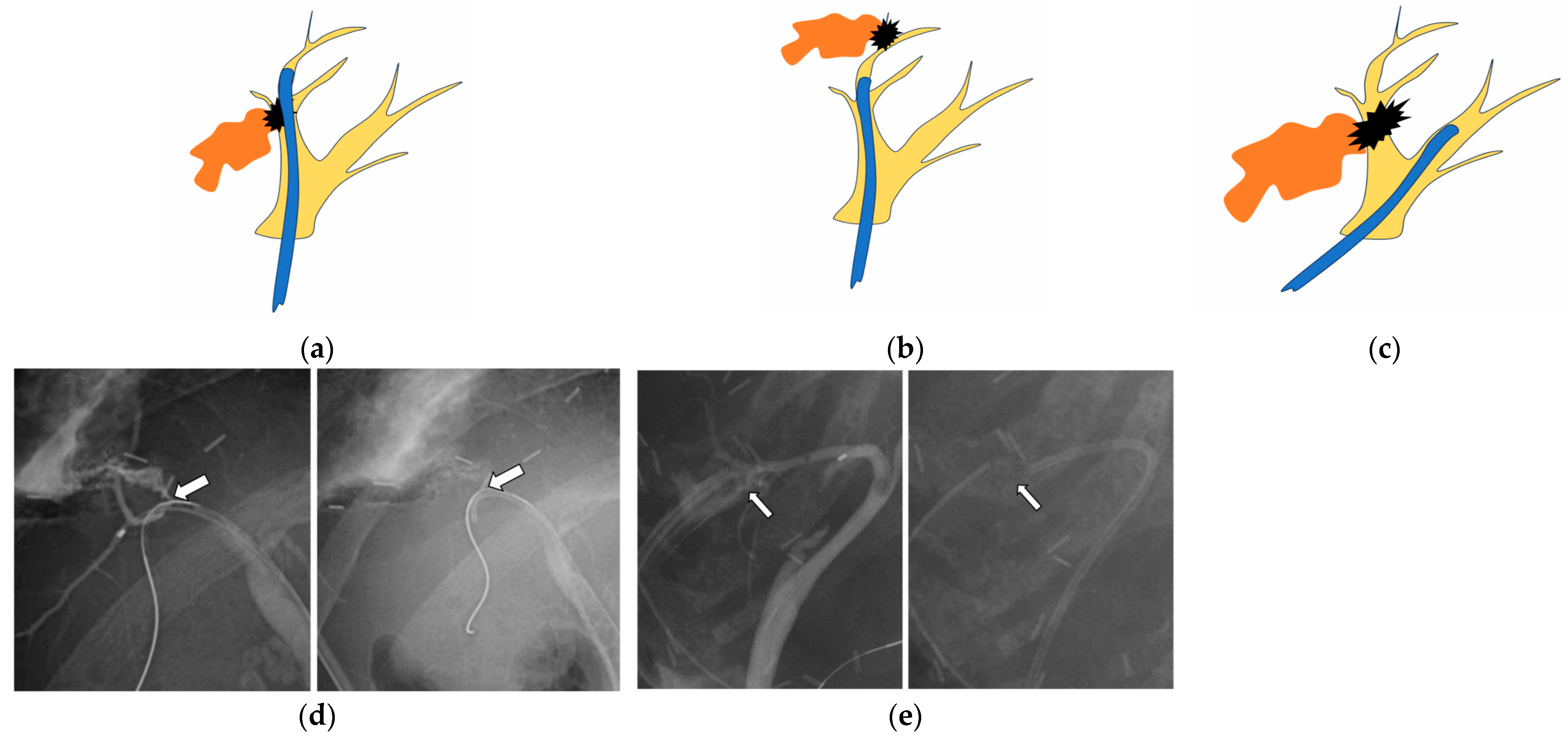
2.2. Endoscopic Procedure
2.3. Follow-Up After Stent Placement by ERC
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
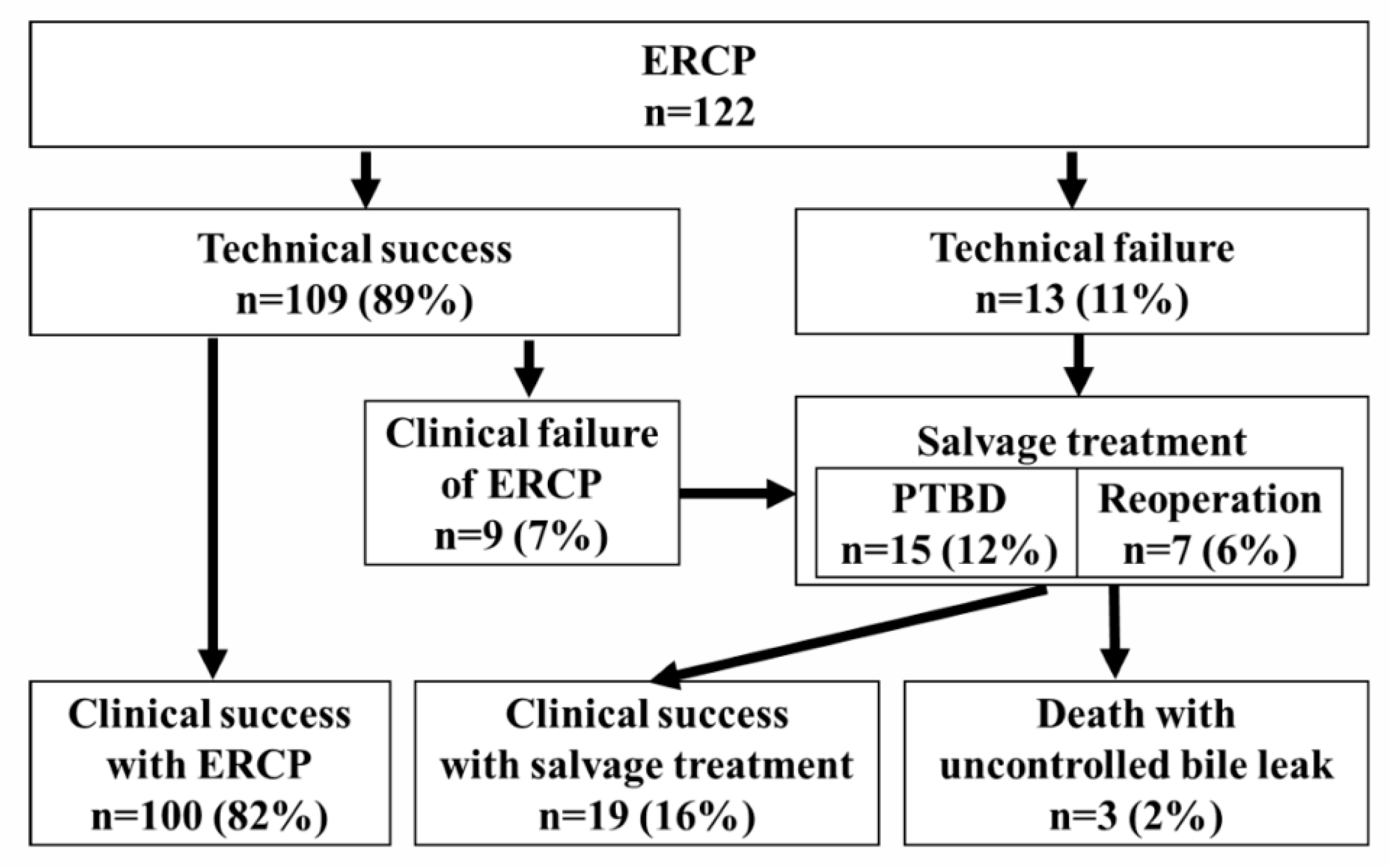
3.2. Results of ERCP
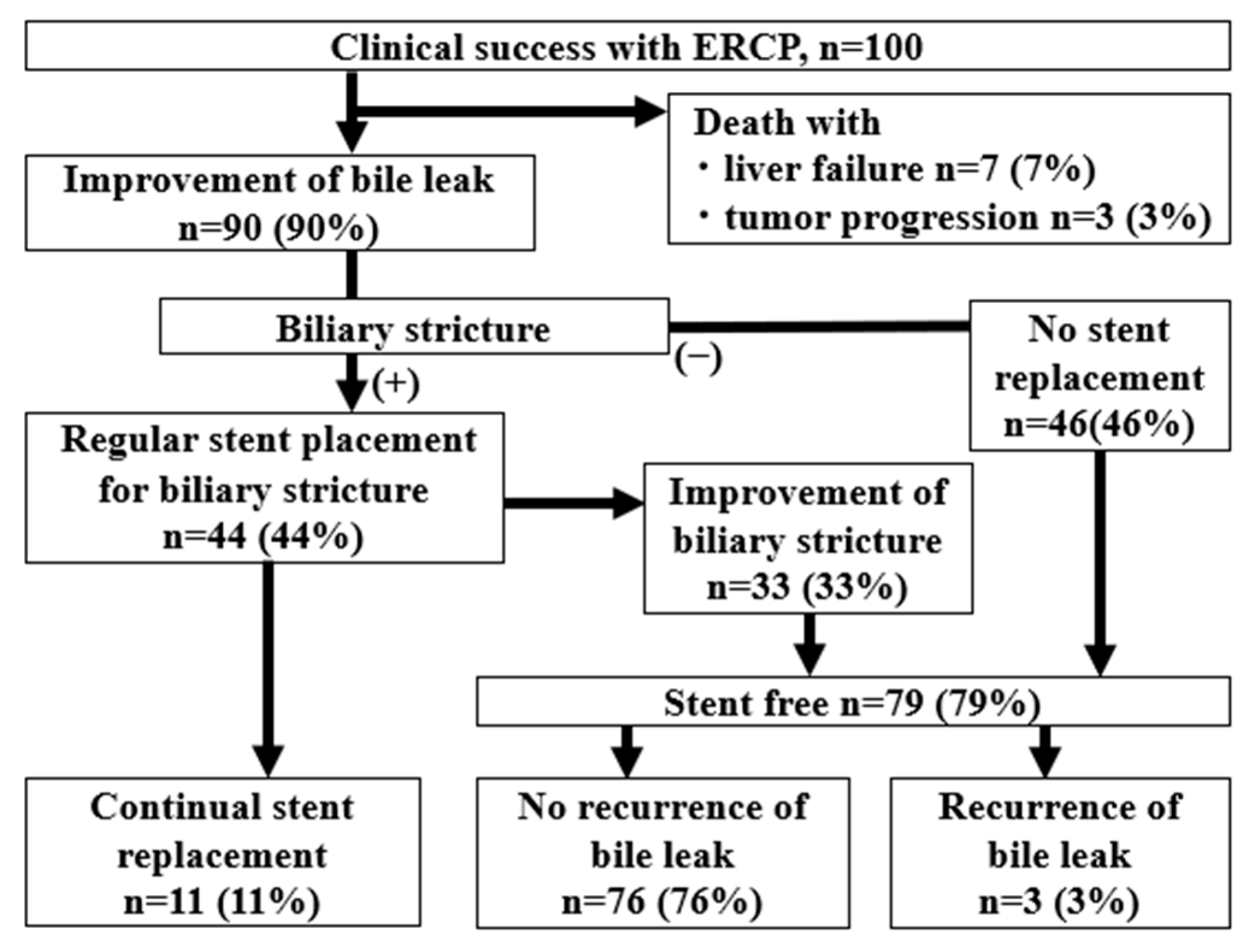
3.3. Long-Term Outcomes
3.4. Factors Related to Clinical Success of Endoscopic Treatments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASGE | American Society for Gastrointestinal Endoscopy |
| BTC | Biliary tract cancer |
| CT | Computed tomography |
| DDLT | Deceased donor living transplantation |
| ERC | Endoscopic retrograde cholangiography |
| ERCP | Endoscopic retrograde cholangiopancreatography |
| EST | Endoscopic sphincterotomy |
| HCC | Hepatocellular carcinoma |
| HR | Hepatic resection |
| IQR | Interquartile range |
| LDLT | Living donor liver transplantation |
| LT | Liver transplantation |
| PS | Plastic stent |
| PTBD | Percutaneous transhepatic biliary drainage |
| QOL | Quality of life |
| SEMS | Self-expanding metallic stents |
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.-Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemel, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Israni, A.K.; Zaun, D.A.; Martinez, A.; Schaffhausen, C.R.; Lozano, C.; McKinney, W.T.; Miller, J.M.; Snyder, J.J. OPTN/SRTR 2023 Annual Data Report: Deceased Organ Donation. Am. J. Transplant. 2025, 25, S490–S517. [Google Scholar] [CrossRef]
- Yildirim, A.C., IV; Zeren, S.; Ekici, M.F.; Yaylak, F.; Algin, M.C.; Arik, O. Comparison of Fenestrating and Reconstituting Subtotal Cholecystectomy Techniques in Difficult Cholecystectomy. Cureus 2022, 14, e22441. [Google Scholar] [CrossRef]
- Kokas, B.; Ulmann, L.; Rozman, P.; Farkas, N.; Szijártó, A.; Szücs, Á. Postoperative bile leak after hepa-to-pancreato-biliary surgery in malignant biliary obstruction: Rates, treatments, and outcomes in a high-volume tertiary referral center. BMC Surg. 2024, 24, 410. [Google Scholar] [CrossRef]
- van Dijk, A.H.; Donkervoort, S.C.; Lameris, W.; de Vries, E.; Eijsbouts, Q.A.J.; Vrouenraets, B.C.; Busch, O.R.; Boermeester, M.A.; de Reuver, P.R. Short- and Long-Term Outcomes after a Reconstituting and Fenestrating Subtotal Chol-ecystectomy. J. Am. Coll. Surg. 2017, 225, 371–379. [Google Scholar] [CrossRef]
- Bhattacharjya, S.; Puleston, J.; Davidson, B.R.; Dooley, J.S. Outcome of early endoscopic biliary drainage in the management of bile leaks after hepatic resection. Gastrointest. Endosc. 2003, 57, 526–530. [Google Scholar] [CrossRef]
- Rerknimitr, R.; Sherman, S.; Fogel, E.L.; Kalayci, C.; Lumeng, L.; Chalasani, N.; Kwo, P.; Lehman, G.A. Biliary tract complications after orthotopic liver transplantation with choledochocholedochostomy anastomosis: Endoscopic findings and results of therapy. Gastrointest. Endosc. 2002, 55, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Elmahi, E.; Fairclough, S.; Knifton, H. The Rate of Postoperative Bile Leak in Minimally Invasive Liver Resection in Comparison with Open Surgery: A Systematic Review. Cureus 2024, 16, e74313. [Google Scholar] [CrossRef] [PubMed]
- Thuluvath, P.J.; Atassi, T.; Lee, J. An endoscopic approach to biliary complications following orthotopic liver transplantation. Liver Int. 2003, 23, 156–162. [Google Scholar] [CrossRef]
- Kubo, N.; Shirabe, K. Treatment strategy for isolated bile leakage after hepatectomy: Literature review. Ann. Gastroenterol. Surg. 2019, 4, 47–55. [Google Scholar] [CrossRef]
- Eurich, D.; Henze, S.; Boas-Knoop, S.; Pratschke, J.; Seehofer, D. T-drain reduces the incidence of biliary leakage after liver resection. Updates Surg. 2016, 68, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Pace, R.F.; Blenkharn, J.I.; Edwards, W.J.; Orloff, M.; Blumgart, L.H.; Benjamin, I.S. Intra-abdominal sepsis after hepatic resection. Ann. Surg. 1989, 209, 302–306. [Google Scholar] [CrossRef]
- Mosconi, C.; Calandri, M.; Mirarchi, M.; Vara, G.; Breatta, A.D.; Cappelli, A.; Brandi, N.; Paccapelo, A.; De Benedittis, C.; Ricci, C.; et al. Percutaneous management of postoperative Bile leak after hepato-pancreato-biliary surgery: A multi-center experience. HPB 2021, 23, 1518–1524. [Google Scholar] [CrossRef]
- Pedicini, V.; Poretti, D.; Mauri, G.; Trimboli, M.; Brambilla, G.; Sconfienza, L.M.; Cornalba, G.; Sardanelli, F. Management of post-surgical biliary leakage with percutaneous transhepatic biliary drainage (PTBD) and occlusion balloon (OB) in patients without dilatation of the biliary tree: Preliminary results. Eur. Radiol. 2010, 20, 1061–1068. [Google Scholar] [CrossRef]
- Patel, I.J.; Rahim, S.; Davidson, J.C.; Hanks, S.E.; Tam, A.L.; Walker, T.G.; Wilkins, L.R.; Sarode, R.; Weinberg, I. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions-Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2019, 30, 1168.e1–1184.e1. [Google Scholar]
- Houghton, E.J.; Uribe, A.K.; De Battista, J.M.; Finger, C.; Acquafresca, P.; Palermo, M.; Giménez, M.E. Risk Factors for Hemorrhagic Adverse Events in Percutaneous Transhepatic Biliary Drainage: A Prospective Multicenter Study. J. Vasc. Interv. Radiol. 2022, 33, 919.e2–925.e2. [Google Scholar] [CrossRef]
- Veitch, A.M.; Radaelli, F.; Alikhan, R.; Dumonceau, J.M.; Eaton, D.; Jerrome, J.; Lester, W.; Nylander, D.; Thoufeeq, M.; Vanbiervliet, G.; et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Gut 2021, 70, 1611–1628. [Google Scholar] [CrossRef]
- Binmoeller, K.F.; Katon, R.M.; Shneidman, R. Endoscopic management of postoperative biliary leaks: Review of 77 cases and report of two cases with biloma formation. Am. J. Gastroenterol. 1991, 86, 227–231. [Google Scholar] [PubMed]
- Carannante, F.; Mazzotta, E.; Miacci, V.; Bianco, G.; Mascianà, G.; D’Agostino, F.; Caricato, M.; Capolupo, G.T. Identification and management of subvesical bile duct leakage after laparoscopic cholecystectomy: A systematic review. Asian J. Surg. 2023, 46, 4161–4168. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Murali, A.R.; Masadeh, M.; Silverman, W.B.; Johlin, F.C. Comparison of Biliary Stent versus Biliary Sphincterotomy Alone in the Treatment of Bile Leak. Dig. Dis. 2020, 38, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Rio-Tintoa, R.; Canena, J. Endoscopic Treatment of Post Cholecystectomy Biliary Leaks. GE Port. J. Gastroenterol. 2021, 28, 265–273. [Google Scholar] [CrossRef]
- Sandha, G.S.; Bourke, M.J.; Haber, G.B.; Kortan, P.P. Endoscopic therapy for bile leak based on a new classification: Results in 207 patients. Gastrointest. Endosc. 2004, 60, 567–574. [Google Scholar] [CrossRef]
- Desai, A.; Twohig, P.; Trujillo, S.; Dalal, S.; Kochhar, G.S.; Sandhu, D.S. Clinical efficacy, timing, and outcomes of ERCP for management of bile duct leaks: A nationwide cohort study. Endosc. Int. Open. 2021, 9, E247–E252. [Google Scholar]
- Gawlik, C.; Carneval, M. A Review of the Management of Bile Leaks. Cureus 2021, 13, e14937. [Google Scholar] [CrossRef]
- Vlaemynck, K.; Lahousse, L.; Vanlander, A.; Piessevaux, H.; Hindryckx, P. Endoscopic management of biliary leaks: A systematic review with meta-analysis. Endoscopy 2019, 51, 1074–1081. [Google Scholar] [CrossRef]
- Schaible, A.; Schemmer, P.; Hackert, T.; Rupp, C.; Schleithoff, A.E.S.; Gotthardt, D.N.; Büchler, M.W.; Sauer, P. Location of a biliary leak after liver resection determines success of endoscopic treatment. Surg. Endosc. 2017, 31, 1814–1820. [Google Scholar] [CrossRef]
- Moy, B.T.; Birk, J.W. A review on the Management of Biliary Complications after Orthotopic Liver Transplantation. J. Clin. Transl. Hepatol. 2019, 7, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Nagra, N.; Klair, J.S.; Jayaraj, M.; Murali, A.R.; Singh, D.; Law, J.; Larsen, M.; Irani, S.; Kozarek, R.; Ross, A.; et al. Biliary Sphincterotomy Alone versus Biliary Stent with or without Biliary Sphincterotomy for the Management of Post-Cholecystectomy Bile Leak: A Systematic Review and Meta-Analysis. Dig. Dis. 2022, 40, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.-W.; Lee, S.K.; Song, T.J.; Park, D.H.; Lee, S.S.; Seo, D.-W.; Kim, M.-H. Endoscopic Management of Bile Leakage after Liver Transplantation. Gut Liver 2015, 9, 417–423. [Google Scholar] [CrossRef]
- Sendino, O.; Fernández-Simon, A.; Law, R.; Dayyeh, B.A.; Leise, M.; Chavez-Rivera, K.; Cordova, H.; Colmenero, J.; Crespo, G.; de Miguel, C.R.; et al. Endoscopic management of bile leaks after liver transplantation: An analysis of two high-volume transplant centers. United Eur. Gastroenterol. J. 2018, 6, 89–96. [Google Scholar] [CrossRef]
- Wu, G.; Li, W.-Y.; Gong, Y.-X.; Lin, F.; Sun, C. Impact of open hepatectomy on postoperative bile leakage in patients with biliary tract cancer. World J. Gastrointest. Surg. 2024, 16, 67–75. [Google Scholar] [CrossRef]
- Çelik, M.; Yilmaz, H.; Akbudak, İ.H.; Kılıç, M.C.; Ozban, M.; Yılmaz, M.; Soykan, M. Efficacy and safety of endoscopic retrograde cholangiopancreatography with endoscopic sphincterotomy and biliary stenting in post-operative bile leaks. Ulus. Travma. Acil. Cerrahi. Derg. 2023, 29, 904–908. [Google Scholar] [CrossRef]
- Tewani, S.K.; Turner, B.G.; Chuttani, R.; Pleskow, D.K.; Sawhney, M.S. Location of bile leak predicts the success of ERCP performed for postoperative bile leaks. Gastrointest. Endosc. 2013, 77, 601–608. [Google Scholar] [CrossRef]
- Koch, M.; Garden, O.J.; Padbury, R.; Rahbari, N.N.; Adam, R.; Capussotti, L.; Fan, S.T.; Yokoyama, Y.; Crawford, M.; Makuuchi, M.; et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011, 149, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef]
- Canena, J.; Horta, D.; Coimbra, J.; Meireles, L.; Russo, P.; Marques, I.; Ricardo, L.; Rodrigues, C.; Capela, T.; Carvalho, D.; et al. Outcomes of endoscopic management of primary and refractory postcholecystectomy biliary leaks in a multicentre review of 178 patients. BMC Gastroenterol. 2015, 15, 105. [Google Scholar] [CrossRef]
- Haidar, H.; Manasa, E.; Yassin, K.; Suissa, A.; Kluger, Y.; Khamaysi, I. Endoscopic treatment of post-cholecystectomy bile leaks: A tertiary center experience. Surg. Endosc. 2021, 35, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Dechêne, A.; Jochum, C.; Fingas, C.; Paul, A.; Heider, D.; Syn, W.-K.; Gerken, G.; Canbay, A.; Zöpf, T. Endoscopic management is the treatment of choice for bile leaks after liver resection. Gastrointest. Endosc. 2014, 80, 626–633.e1. [Google Scholar] [CrossRef]
- Bjorkman, D.J.; Carr-Locke, D.L.; Lichtenstein, D.R.; Ferrari, A.P.; Slivka, A.; Van Dam, J.; Brooks, D.C. Postsurgical bile leaks: Endoscopic obliteration of the transpapillary pressure gradient is enough. Am. J. Gastroenterol. 1995, 90, 2128–2133. [Google Scholar]
- Baron, T.H.; Poterucha, J.J. Insertion and Removal of Covered Expandable Metal Stents for Closure of Complex Biliary Leaks. Clin. Gastroenterol. Hepatol. 2006, 4, 381–386. [Google Scholar]
- Macías-Gómez, C.; Dumonceau, J.-M. Endoscopic management of biliary complications after liver transplantation: An evidence-based review. World J. Gastrointest. Endosc. 2015, 7, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Mavrogiannis, C.; Liatsos, C.; Papanikolaou, I.S.; Karagiannis, S.; Galanis, P.; Romanos, A. Biliary stenting alone versus biliary stenting plus sphincterotomy for the treatment of post-laparoscopic cholecystectomy biliary leaks: A prospective randomized study. Eur. J. Gastroenterol. Hepatol. 2006, 18, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Yabe, S.; Kato, H.; Mizukawa, S.; Akimoto, Y.; Uchida, D.; Seki, H.; Tomoda, T.; Matsumoto, K.; Yamamoto, N.; Horiguchi, S.; et al. Predictive factors for outcomes of patients undergoing endoscopic therapy for bile leak after hepatobiliary surgery. Dig. Endosc. 2017, 29, 353–361. [Google Scholar] [CrossRef]
- Canena, J.; Liberato, M.; Horta, D.; Romão, C.; Coutinho, A. Short-term stenting using fully covered self-expandable metal stents for treatment of refractory biliary leaks, postsphincterotomy bleeding, and perforations. Surg. Endosc. 2013, 27, 313–324. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 122 | Surgery Type, n (%) | |
| Sex, male, n (%) | 89 (73) | LDLT | 48 (39) |
| Median age, years (range) | 60 (21–85) | Right lobe graft | 30 (25) |
| Diagnosis, n (%) | Left lobe graft | 14 (11) | |
| Hepatocellular carcinoma | 51 (42) | Posterior segment graft | 4 (3) |
| Cholangiocarcinoma | 9 (7) | DDLT | 1 (1) |
| Other cancers/metastatic cancer | 14 (11) | Total liver graft | 1 (1) |
| Liver failure due to liver cirrhosis | 40 (33) | Hepatic resection | 73 (60) |
| Transplant donors | 5 (4) | Right lobe resection | 13 (10) |
| Other benign disease | 3 (2) | Left lobe resection | 24 (20) |
| Interval between surgery and | 41 (3–1716) | Segment resection | 36 (30) |
| First ERCP, median, days (range) | Bile leak grade (ISGLS 2010 [38]), n (%) | ||
| With external fistula at the initial ERCP | 89 (72%) | Grade B Grade C | 115 (94) 7 (6) |
| Bile Leak Location, n | Plastic Stent Placement, n (%) | ||
| HR | Bridging the leak site | 82 (67) | |
| Hilar duct | 54 | Distal of the leak site | 12 (9) |
| Peripheral duct | 18 | Another bile duct | 15 (12) |
| CHD | 6 | Median number of stents, n (range) | 1 (1–3) |
| LT | Maximum stent diameter | 7 (5–10) | |
| Anastomosis | 44 | Median, Fr (range) | |
| Cystic duct remnant | 4 | Clinical success, n (%) | 100 (82) |
| Biliary stricture, n (%) | 78 (62) | Salvage treatment, n (%) | |
| Bile leak severity, n | PTBD | 15 (12) | |
| Low grade | 61 | Reoperation | 7 (6) |
| High grade | 61 | Adverse events, n (%) | |
| Endoscopic sphincterotomy, n (%) | 65 (53) | Pancreatitis | 7 (6) |
| Technical success, n (%) | 109 (89) | Cholangitis | 2 (2) |
| Abscess | 1 (1) |
| Variable | Clinical Success | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|
| n | % | OR (95%CI) | p Value | OR (95%CI) | p Value | ||
| Sex, male | 72/89 | 81 | 0.75 (0.25–2.25) | 0.79 | |||
| Age, <median(60 y.o.) | 48/57 | 84 | 1.33 (0.52–3.40) | 0.64 | |||
| Surgery type | LT | 38/49 | 78 | 1.63 (0.64–4.13) | 0.34 | ||
| HR | 62/73 | 85 | |||||
| Days from surgery to ERCP, | 53/60 | 88 | 2.42 (0.090–6.43) | 0.1 | 1.91 (0.57–6.43) | 0.30 | |
| <Median (41 days) | |||||||
| Leak location | LT, anastomosis | 35/45 | 78 | 1.17 (0.11–12.5) | 0.99 | ||
| HR, hilar duct | 44/55 | 80 | 0.80 (0.20–3.26) | 0.99 | |||
| Target lobe | Right lobe | 72/84 | 86 | 2.22 (0.86–5.74) | 0.12 | ||
| Biliary stricture | (+) | 62/77 | 81 | 0.65 (0.23–1.83) | 0.47 | ||
| Leak severity | High grade | 44/61 | 73 | 0.23 (0.08–0.68) | 0.0085 | 0.21 (0.06–0.74) | 0.015 |
| Sphincterotomy | (+) | 52/65 | 80 | 0.75 (0.29–1.91) | 0.64 | ||
| Leak-bridging stenting | (+) | 77/82 | 84 | 8.93 (3.13–25.4) | <0.001 | 12.2 (3.49–42.5) | <0.001 |
| Maximum Stent diameter | ≥7 Fr | 38/41 | 93 | 1.90 (0.48–7.46) | 0.53 | ||
| Multiple stents | (+) | 18/18 | 100 | N.A. | 0.35 | ||
| With external fistula | (+) | 79/88 | 90 | 5.43 (2.04–14.4) | 0.0010 | 7.10 (1.99–25.3) | 0.0025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obata, T.; Matsumoto, K.; Harada, K.; Hattori, N.; Sato, R.; Matsumi, A.; Miyamoto, K.; Terasawa, H.; Fujii, Y.; Uchida, D.; et al. Endoscopic Bridging Stent Placement Improves Bile Leaks After Hepatic Surgery. J. Clin. Med. 2025, 14, 3381. https://doi.org/10.3390/jcm14103381
Obata T, Matsumoto K, Harada K, Hattori N, Sato R, Matsumi A, Miyamoto K, Terasawa H, Fujii Y, Uchida D, et al. Endoscopic Bridging Stent Placement Improves Bile Leaks After Hepatic Surgery. Journal of Clinical Medicine. 2025; 14(10):3381. https://doi.org/10.3390/jcm14103381
Chicago/Turabian StyleObata, Taisuke, Kazuyuki Matsumoto, Kei Harada, Nao Hattori, Ryosuke Sato, Akihiro Matsumi, Kazuya Miyamoto, Hiroyuki Terasawa, Yuki Fujii, Daisuke Uchida, and et al. 2025. "Endoscopic Bridging Stent Placement Improves Bile Leaks After Hepatic Surgery" Journal of Clinical Medicine 14, no. 10: 3381. https://doi.org/10.3390/jcm14103381
APA StyleObata, T., Matsumoto, K., Harada, K., Hattori, N., Sato, R., Matsumi, A., Miyamoto, K., Terasawa, H., Fujii, Y., Uchida, D., Horiguchi, S., Tsutsumi, K., & Otsuka, M. (2025). Endoscopic Bridging Stent Placement Improves Bile Leaks After Hepatic Surgery. Journal of Clinical Medicine, 14(10), 3381. https://doi.org/10.3390/jcm14103381