

Comparison of Intraocular Pressure Measurements with Goldmann Applanation Tonometry, iCare, and Tono-Pen in Young Children with Anterior Segment Abnormalities Under General Anesthesia


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Devices and Measurement Methods
2.3. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Leske, M.C.; Heijl, A.; Hyman, L.; Bengtsson, B. Early Manifest Glaucoma Trial: Design and baseline data. Ophthalmology 1999, 106, 2144–2153. [Google Scholar] [CrossRef] [PubMed]
- Chagny, M.; Stolowy, N.; Denis, D.; Sauvan, L. Comparison of the iCare rebound tonometer and the Perkins applanation tonometer in children under general anesthesia. J. Français D’ophtalmologie 2023, 46, 1005–1012. [Google Scholar] [CrossRef]
- Ko, F.; Papadopoulos, M.; Khaw, P.T. Primary congenital glaucoma. Prog. Brain Res. 2015, 221, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Yassin, S.A. Long-Term Visual Outcomes in Children with Primary Congenital Glaucoma. Eur. J. Ophthalmol. 2017, 27, 705–710. [Google Scholar] [CrossRef]
- Strzalkowska, A.; Pirlich, N.; Stingl, J.V.; Schuster, A.K.; Rezapour, J.; Wagner, F.M.; Buse, J.; Hoffmann, E.M. Intraocular Pressure Measurement in Childhood Glaucoma under Standardized General Anaesthesia: The Prospective EyeBIS Study. J. Clin. Med. 2022, 11, 2846. [Google Scholar] [CrossRef]
- Feng, C.S.; Jin, K.W.; Yi, K.; Choi, D.G. Comparison of Intraocular Pressure Measurements Obtained by Rebound, Noncontact, and Goldmann Applanation Tonometry in Children. Am. J. Ophthalmol. 2015, 160, 937–943 e931. [Google Scholar] [CrossRef]
- Krieglstein, G.K.; Waller, W.K. Goldmann applanation versus hand-applanation and .schiotz indentation tonometry. Albrecht Graefes Arch. Klin. Exp. Ophthalmol. 1975, 194, 11–16. [Google Scholar] [CrossRef]
- Browning, A.C.; Bhan, A.; Rotchford, A.P.; Shah, S.; Dua, H.S. The effect of corneal thickness on intraocular pressure measurement in patients with corneal pathology. Br. J. Ophthalmol. 2004, 88, 1395–1399. [Google Scholar] [CrossRef]
- McKee, E.C.; Ely, A.L.; Duncan, J.E.; Dosunmu, E.O.; Freedman, S.F. A comparison of Icare PRO and Tono-Pen XL tonometers in anesthetized children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2015, 19, 332–337. [Google Scholar] [CrossRef]
- Hsiao, Y.C.; Dzau, J.R.; Flemmons, M.S.; Asrani, S.; Jones, S.; Freedman, S.F. Home assessment of diurnal intraocular pressure in healthy children using the Icare rebound tonometer. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Boothe, W.A.; Lee, D.A.; Panek, W.C.; Pettit, T.H. The Tono-Pen. A manometric and clinical study. Arch. Ophthalmol. 1988, 106, 1214–1217. [Google Scholar] [CrossRef]
- Yildiz, M.B.; Kose, A.O.; Celik, G.; Kizilay, O.; Imamoglu, S.; Yildiz, E. Agreement among Goldmann Applanation Tonometer, Easyton Transpalpebral Tonometer, Tonopen, and Icare in Patients with Keratoconus. Beyoglu Eye J. 2023, 8, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Tayar, A.; Grossjohann, R.; Stahl, A.; Tost, F. Comparing Different Self-Tonometry Devices against Goldmann Applanation Tonometry—Special Focus on Biomechanical Properties of the Cornea. Klin. Monbl. Augenheilkd 2025, 242, 137–145. [Google Scholar] [CrossRef]
- Kontiola, A.; Puska, P. Measuring intraocular pressure with the Pulsair 3000 and Rebound tonometers in elderly patients without an anesthetic. Graefes Arch. Clin. Exp. Ophthalmol. 2004, 242, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Hernandez, C.; Arribas-Pardo, P.; Sanchez Jean, R.; Garcia-Feljoo, J. Influence of Axial Length on Intraocular Pressure Measurement With Three Tonometers in Childhood Glaucoma. J. Pediatr. Ophthalmol. Strabismus 2020, 57, 27–32. [Google Scholar] [CrossRef]
- Karhanova, M.; Kalitova, J.; Maluskova, M.; Schovanek, J.; Zapletalova, J.; Mlcak, P.; Maresova, K. Comparison of Three Methods of Tonometry in Patients with Inactive Thyroid-Associated Orbitopathy. Cesk Slov. Oftalmol. 2023, 79, 318–323. [Google Scholar] [CrossRef]
- Grigorian, F.; Grigorian, A.P.; Olitsky, S. The Effect of Introduction of iCare Tonometer in the Pediatric Ophthalmology Clinic on Number of Examinations Under Anesthesia. Investig. Ophthalmol. Vis. Sci. 2011, 52, 679. [Google Scholar]
- Duran, M. Comparison of intraocular pressure measurements obtained by icare pro tonometer, non-contact tonometer and Goldmann applanation tonometer in healthy individuals. J. Français D’ophtalmologie 2023, 46, 1195–1203. [Google Scholar] [CrossRef]
- Liu, J.; Roberts, C.J. Influence of corneal biomechanical properties on intraocular pressure measurement: Quantitative analysis. J. Cataract. Refract. Surg. 2005, 31, 146–155. [Google Scholar] [CrossRef]
- Lambert, S.R.; Melia, M.; Buffenn, A.N.; Chiang, M.F.; Simpson, J.L.; Yang, M.B. Rebound tonometry in children: A report by the American Academy of Ophthalmology. Ophthalmology 2013, 120, e21–e27. [Google Scholar] [CrossRef]
- Borrego Sanz, L.; Morales-Fernandez, L.; Martinez de-la-Casa, J.M.; Saenz-Frances, F.; Fuentes, M.; Garcia-Feijoo, J. The Icare-Pro Rebound Tonometer Versus the Hand-held Applanation Tonometer in Congenital Glaucoma. J. Glaucoma 2016, 25, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Martinez-de-la-Casa, J.M.; Garcia-Feijoo, J.; Saenz-Frances, F.; Vizzeri, G.; Fernandez-Vidal, A.; Mendez-Hernandez, C.; Garcia-Sanchez, J. Comparison of rebound tonometer and Goldmann handheld applanation tonometer in congenital glaucoma. J. Glaucoma 2009, 18, 49–52. [Google Scholar] [CrossRef]
- Angmo, D.; Ramesh, P.; Mahalingam, K.; Azmira, K.; Pandey, S.; Gupta, V.; Sihota, R.; Dada, T. Comparative Evaluation of Rebound and Perkins Tonometers in Pediatric Glaucoma With Varied Corneal Characteristics. J. Glaucoma 2021, 30, 312–316. [Google Scholar] [CrossRef]
- Umfress, A.C.; Glaser, T.S.; Ploysangam, P.; Freedman, S.F. Rebound tonometry by iCare 200 (IC200): Comparison with Tono-Pen in the operating room and Goldmann applanation in the clinic. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2021, 25, 329 e321–329 e326. [Google Scholar] [CrossRef] [PubMed]
- Stoddard-Bennett, T.; Jackson, N.J.; Robbins, L.; Villanueva, P.; Suh, S.Y.; Demer, J.L.; Pineles, S.L.; Fung, S.S.M. Agreement of iCare IC200 tonometry with Perkins applanation tonometry in healthy children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, 235 e231–235 e235. [Google Scholar] [CrossRef] [PubMed]
- Poostchi, A.; Mitchell, R.; Nicholas, S.; Purdie, G.; Wells, A. The iCare rebound tonometer: Comparisons with Goldmann tonometry, and influence of central corneal thickness. Clin. Exp. Ophthalmol. 2009, 37, 687–691. [Google Scholar] [CrossRef]
- Esmael, A.; Ismail, Y.M.; Elhusseiny, A.M.; Fayed, A.E.; Elhilali, H.M. Agreement profiles for rebound and applanation tonometry in normal and glaucomatous children. Eur. J. Ophthalmol. 2019, 29, 379–385. [Google Scholar] [CrossRef]
- Bayoumi, N.H.; El Shakankiri, N.M. Central Corneal Thickness in Aphakic Children With Microcornea-Microphthalmia. J. Glaucoma 2016, 25, 497–500. [Google Scholar] [CrossRef]
- Yulia, D.E.; Tan, S. Intraocular pressure measurements in paediatric glaucoma: A narrative review on accuracy, tolerability, and ease of use. Med. J. Malays. 2024, 79, 206–211. [Google Scholar]
- Munkwitz, S.; Elkarmouty, A.; Hoffmann, E.M.; Pfeiffer, N.; Thieme, H. Comparison of the iCare rebound tonometer and the Goldmann applanation tonometer over a wide IOP range. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Sung, V.; Lascaratos, G.; Nagi, H.; Holder, R. Intraocular pressures after ketamine and sevoflurane in children with glaucoma undergoing examination under anaesthesia. Br. J. Ophthalmol. 2010, 94, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, D.; Congdon, N.; Jampel, H.; Gilbert, D.; Elliott, R.; Rivers, R.; Munoz, B.; Quigley, H. The effects of sevoflurane and ketamine on intraocular pressure in children during examination under anesthesia. Am. J. Ophthalmol. 2007, 143, 494–499. [Google Scholar] [CrossRef]
- Oatts, J.T.; Shen, S.; Zhu, H.; Gong, Q.; Yu, Y.; Ying, G.S.; Han, Y.; Liu, H. A Prospective Study of the Effects of General Anesthesia on Intraocular Pressure in Healthy Children. Ophthalmol. Sci. 2024, 4, 100455. [Google Scholar] [CrossRef] [PubMed]
- Senthil, S.; Nakka, M.; Rout, U.; Ali, H.; Choudhari, N.; Badakere, S.; Garudadri, C. Changes in intraocular pressures associated with inhalational and mixed anesthetic agents currently used in ophthalmic surgery. Indian J. Ophthalmol. 2021, 69, 1808–1814. [Google Scholar] [CrossRef]
- Rao, A.; Kumar, M.; Prakash, B.; Varshney, G. Relationship of central corneal thickness and intraocular pressure by iCare rebound tonometer. J. Glaucoma 2014, 23, 380–384. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| children (n) | 19 |
| female (n) | 11 |
| male (n) | 8 |
| age (years) | 1.8 ± 2.08 |
| eyes (n) | 38 |
| aphakia (n) | 18 |
| congenital cataract | 10 |
| congenital glaucoma | 7 |
| nystagmus and/or hyperopia | 3 |
| corneal diameter (mean ± SD; mm) | horizontal: 10.6 ± 1.4 vertical: 10.1 ± 1.5 |
| corneal thickness (mean ± SD; µm) | all eyes: 645 ± 135 aphakic eyes: 733 ± 267 phakic eyes: 604 ± 351 eyes with glaucoma: 744 ± 224 |
| IOP, all devices [mean ± SD, (range); mmHg] | 14.1 ± 7.4 (5–43) |
| Perkins | 11.1 ± 4.8 (5–34) |
| iCare | 11.6 ± 4.4 (6.4–36.4) |
| Tono-Pen | 15.2 ± 5.5 (7–37) |
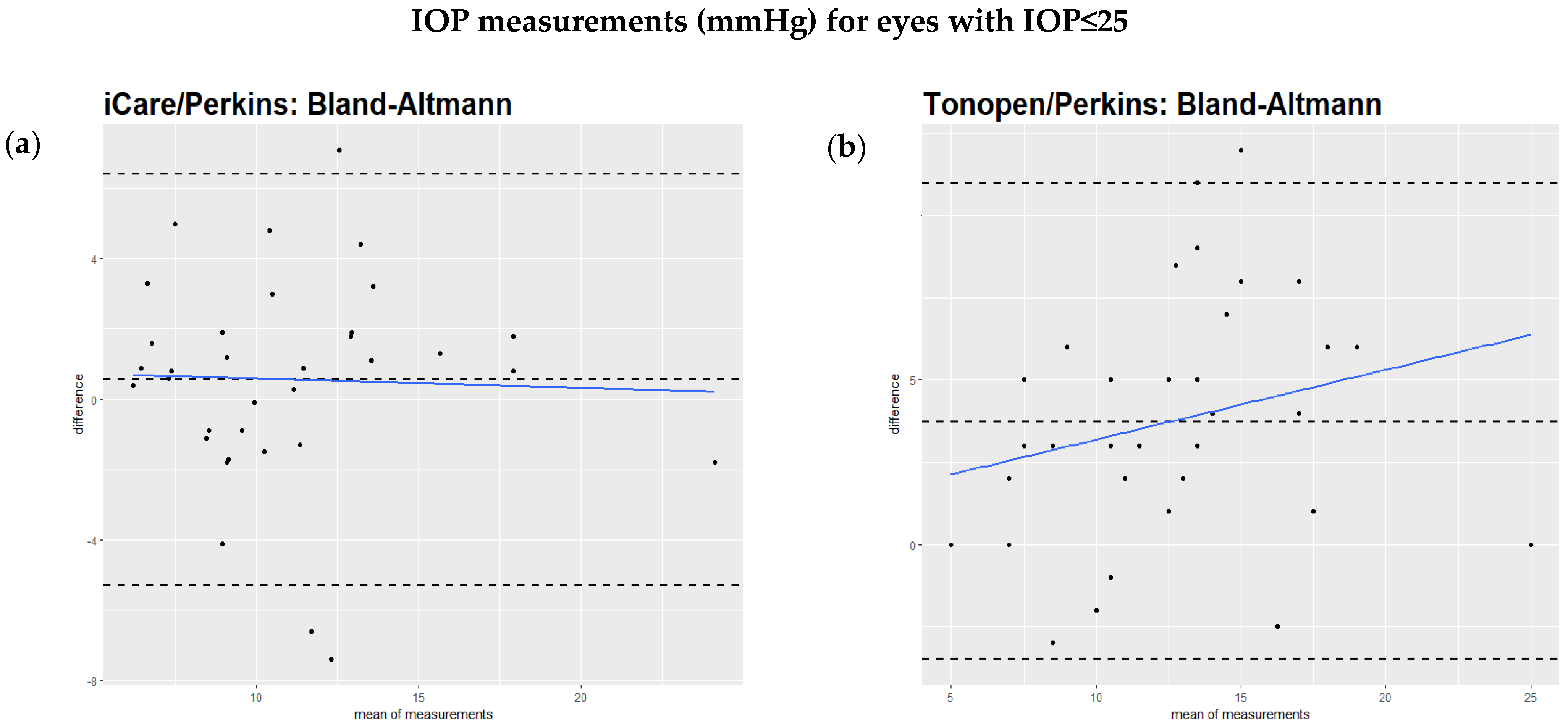
| Comparison Pair | Slope (All Values) | p-Value | Slope (IOP ≤ 25 mmHg) | p-Value |
|---|---|---|---|---|
| iCare vs. Perkins | 0.42 | <0.005 | –0.12 | 0.39 |
| Tono-Pen vs. Perkins | 0.20 | 0.04 | 0.20 | 0.24 |
| iCare vs. Tono-Pen | 0.25 | 0.02 | –0.30 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Studer, M.K.; Iliev, M.; Tappeiner, C.; Frueh, B.E.; Fraenkl, S.A. Comparison of Intraocular Pressure Measurements with Goldmann Applanation Tonometry, iCare, and Tono-Pen in Young Children with Anterior Segment Abnormalities Under General Anesthesia. J. Clin. Med. 2025, 14, 3338. https://doi.org/10.3390/jcm14103338
Studer MK, Iliev M, Tappeiner C, Frueh BE, Fraenkl SA. Comparison of Intraocular Pressure Measurements with Goldmann Applanation Tonometry, iCare, and Tono-Pen in Young Children with Anterior Segment Abnormalities Under General Anesthesia. Journal of Clinical Medicine. 2025; 14(10):3338. https://doi.org/10.3390/jcm14103338
Chicago/Turabian StyleStuder, Matias K., Milko Iliev, Christoph Tappeiner, Beatrice E. Frueh, and Stephan A. Fraenkl. 2025. "Comparison of Intraocular Pressure Measurements with Goldmann Applanation Tonometry, iCare, and Tono-Pen in Young Children with Anterior Segment Abnormalities Under General Anesthesia" Journal of Clinical Medicine 14, no. 10: 3338. https://doi.org/10.3390/jcm14103338
APA StyleStuder, M. K., Iliev, M., Tappeiner, C., Frueh, B. E., & Fraenkl, S. A. (2025). Comparison of Intraocular Pressure Measurements with Goldmann Applanation Tonometry, iCare, and Tono-Pen in Young Children with Anterior Segment Abnormalities Under General Anesthesia. Journal of Clinical Medicine, 14(10), 3338. https://doi.org/10.3390/jcm14103338