

Low Back Pain in South African Adolescent Field Hockey Players: Implications for Future Practice

Abstract
1. Introduction
2. Methodology
2.1. Study Design and Setting
2.2. Study Population and Sample Size
2.3. Inclusion and Exclusion Criteria
- Male adolescents (12–19 years of age) who participate in field hockey in the eThekwini municipality.
- Field hockey players who participate on an Astroturf surface.
- Participants having completed the learner assent form along with their parent/legal guardian providing consent.
- Participants who participated in the pilot study.
- Participants whose parent/legal guardian did not provide informed consent.
- Participants who did not sign the learner assent form.
- Participants residing outside the eThekwini municipality.
2.4. Measurement Tool
2.5. Expert Focus Group
- -
- The researcher;
- -
- The research supervisor/s;
- -
- Two potential participants;
- -
- A Master’s student who was conducting questionnaire research;
- -
- One lecturer and researcher with experience in quantitative research.
2.6. Data Analysis
3. Results
3.1. Descriptive Characteristics of Participants
3.2. Three-Month Period Prevalence, Point Prevalence, and Incidence of Low Back Pain
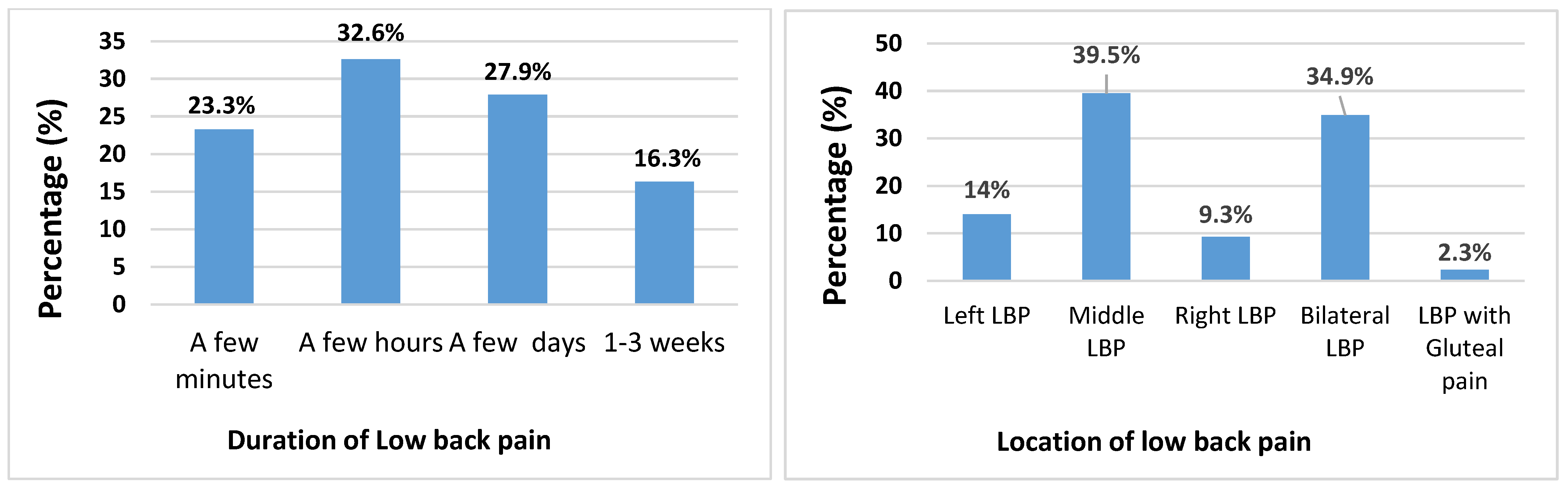
3.3. Characteristics of Low Back Pain
3.4. Associations Between Low Back Pain and Health and Lifestyle Factors
3.5. Management and Treatment of Low Back Pain
4. Discussion
4.1. Prevalence and Incidence of Low Back Pain
4.2. Characteristics of Low Back Pain
4.3. Duration of Low Back Pain and Associated Disability/Chronicity
4.4. Treatment and Management
4.5. Selected Risk Factors
4.6. Playing Position
4.7. Health and Lifestyle
4.8. Strengths of the Study
4.9. Limitations and Future Recommendations
5. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LBP | Lower back pain |
| NCAA division III | National Collegiate Athletic Association in the United States |
| SD | Standard deviation |
| BMI | Body mass index |
| EBP | Evidence-based practice |
| DOMS | Delayed onset muscle soreness |
References
- Black, A.M.; Meeuwisse, D.W.; Eliason, P.H.; Hagel, B.E.; Emery, C.A. Sport Participation and Injury Rates in High School Students: A Canadian Survey of 2029 Adolescents. J. Saf. Res. 2021, 78, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-Specific Low Back Pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Barboza, S.D.; Nauta, J.; Emery, C.; Van Mechelen, W.; Gouttebarge, V.; Verhagen, E. A Warm-Up Program to Reduce Injuries in Youth Field Hockey Players: A Quasi-Experiment. J. Athl. Train. 2019, 54, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Canepa, M.J.; San Martin, C.; Garrido, E. Youth Female Field Hockey Players Physical Condition. J. Phys. Med. Rehabil. Stud. Rep. 2023, 5, 1–9. [Google Scholar] [CrossRef]
- Cholewicki, J.; McGill, S.M.; Norman, R.W. Lumbar Spine Stability Can Be Augmented with Abdominal Muscle Coactivation. Clin. Biomech. 2000, 15, 481–488. [Google Scholar]
- Hidalgo-García, C.; Carcasona-Otal, A.; Hernández-Secorún, M.; Abenia-Benedí, H.; Brandt, L.; Krauss, J.; Tricás-Moreno, J.M.; Lucha-López, O. Effects of Contralateral Hip Flexion Angle on the Ober Test. Biomed. Res. Int. 2022, 2022, 3349940. [Google Scholar] [CrossRef] [PubMed]
- RAOSOFT. Sample Size Calculator. Available online: http://www.raosoft.com/samplesize.html (accessed on 4 July 2018).
- Goertz, M.; Thorson, D.; Bonsell, J.; Bonte, B.; Campbell, R.; Haake, B.; Johnson, K.; Kramer, C.; Mueller, B.; Peterson, S.; et al. Adult Acute and Subacute Low Back Pain; Institute for Clinical Systems Improvement: Bloomington, MN, USA, 2012; pp. 8–9.
- Kopec, J.A.; Esdaile, J.M.; Abrahamowicz, M. The Quebec Back Pain Disability Scale: Measurement Properties. Spine 1995, 20, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Davison, M.; Keating, J.L. A Comparison of Five Low Back Disability Questionnaires: Reliability and Responsiveness. Phys. Ther. 2002, 82, 8–24. [Google Scholar] [CrossRef] [PubMed]
- Van Hilst, J.; Hilgerson, N.F.; Kuilman, M.C. Low Back Pain in Young Elite Field Hockey Players, Football Players and Speed Skaters: Prevalence and Risk Factors. J. Back Musculoskelet. Rehabil. 2015, 28, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Haydt, R.; Pheasant, S.; Lawrence, K. The Incidence of Low Back Pain in NCAA Division III Female Field Hockey Players. Int. J. Sports Phys. Ther. 2012, 7, 296–305. [Google Scholar] [PubMed]
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation, and Physical Activity; Human Kinetics: Champaign, IL, USA, 2004; Chapter 16. [Google Scholar]
- Wege, S.; Freitag, S.; Schmidt-Wiethoff, R.; Strüder, H.K. Trunk Muscle Strength in Field Hockey Players. J. Strength Cond. Res. 2006, 20, 604–609. [Google Scholar]
- Collier, D.; Blasch, C.; Elders, P.; Hunnaball, M.; Powell, K.; Renaud, A.; Sandison, D.; Youssef, A.; Smith, B. Rules of Hockey; FIH: Lausanne, Switzerland, 2016. [Google Scholar]
- Gorman, A.J.; Li, F.X.; Shum, G.L.K. The Timing and Magnitude of Muscular Activity Patterns during a Field Hockey Hit. Sports Biomech. 2013, 12, 341–350. [Google Scholar]
- McGill, S.M. Low Back Disorders: Evidence-Based Prevention and Rehabilitation, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2007. [Google Scholar]
- Rubinstein, S.M.; De Zoete, A.; Van Middelkoop, M.; Assendelft, W.J.J.; De Boer, M.R.; Van Tulder, M.W. Benefits and Harms of Spinal Manipulative Therapy for the Treatment of Chronic Low Back Pain: Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2019, 364, l689. [Google Scholar] [CrossRef] [PubMed]
- Fett, D.; Trompeter, K.; Platen, P. Back Pain in Elite Sports: A Cross-Sectional Study on 1114 Athletes. PLoS ONE 2017, 12, e0180130. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, W. Low Back Pain and Injury in Athletes; Department of Orthopaedic Surgery, Royal Melbourne Hospital: Parkville Victoria, Australia, 2012. [Google Scholar]
- Sharma, A.; Seth, M.; Koley, S. Profile of Injuries in Indian Elite Male Field Hockey Players in Relation to Playing Positions. Med. Sport. 2012, 8, 1839. [Google Scholar]
- Ellapen, T.; Bowyer, K.; Van Heerden, H. Common Acute and Chronic Musculoskeletal Injuries among Female Adolescent Field Hockey Players in KwaZulu-Natal, South Africa. S. Afr. J. Sports Med. 2014, 26, 4–8. [Google Scholar] [CrossRef]
- Lee, E.C.; Fragala, M.S.; Kavouras, S.A.; Queen, R.M.; Pryor, J.L.; Casa, D.J. Biomarkers in Sports and Exercise: Tracking Health, Performance, and Recovery in Athletes. J. Strength Cond. Res. 2017, 31, 2920–2937. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Indicator | Prevalence | n | Mean | SD | SEM | p |
|---|---|---|---|---|---|---|
| Height (cm) | No LBP | 25 | 170.8 | 10.5 | 2.1 | 0.13 |
| LBP | 43 | 174.7 | 9.8 | 1.5 | ||
| Body mass (kg) | No LBP | 25 | 62.4 | 9.8 | 2.0 | 0.12 |
| LBP | 43 | 66.0 | 8.7 | 1.3 | ||
| Age (years) | No LBP | 25 | 15.3 | 1.6 | 0.3 | 0.72 |
| LBP | 43 | 15.4 | 1.4 | 0.2 | ||
| Number of matches played during the season | No LBP | 25 | 21.7 | 7.5 | 1.5 | 0.58 |
| LBP | 43 | 23.0 | 9.7 | 1.5 | ||
| Number of times played per week (during the season) | No LBP | 25 | 4.6 | 1.1 | 0.23 | 0.5 |
| LBP | 43 | 5.0 | 1.6 | 0.2 | ||
| Number of years played | No LBP | 25 | 5.8 | 2.1 | 0.4 | 0.08 |
| LBP | 43 | 6.8 | 2.1 | 0.3 | ||
| Playing position | ||||||
| (a) Goalkeeper | No LBP | 3 (37%) | - | - | - | - |
| LBP | 5 (62.5%) | - | - | - | - | |
| (b) Defender | No LBP | 9 (33%) | - | - | - | - |
| LBP | 18 (66.7%) | - | - | - | - | |
| (c) Midfield | No LBP | 7 (43%) | - | - | - | - |
| LBP | 9 (56.3%) | - | - | - | - | |
| (d) Forward | No LBP | 5 (38.5%) | - | - | - | - |
| LBP | 8 (61.3%) | - | - | - | - | |
| (e) Defender or midfield | No LBP | 0 (0.0%) | - | - | - | - |
| LBP | 3 (100.0%) | - | - | - | - | |
| (f) Midfield or forward | No LBP | 1 (100.0%) | - | - | - | - |
| LBP | 0 (0.0%) | - | - | - | - |
| No Low Back Pain | Low Back Pain | |||
|---|---|---|---|---|
| Frequency (n) | Percentage (%) | Frequency (n) | Percentage (%) | |
| 3-month period prevalence | 25 | 36.8% | 43 | 63.2% |
| Incidence | 42 | 61.8% | 26 | 38.2% |
| Point prevalence beginning of season | 51 | 75% | 17 | 25% |
| Point prevalence mid-season | 46 | 67.6% | 22 | 32.4% |
| Point prevalence end of season | 53 | 77.9% | 15 | 22.1% |
| Risk Factor | Low Back Pain Prevalence | p Value | ||||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| n | % | n | % | |||
| Warm up before play | No | 1 | 100.0% | 0 | 0.0% | 0.186 |
| Yes | 24 | 35.8% | 43 | 64.2% | ||
| Diet/nutrition | Very healthy | 0 | 0.0% | 2 | 100.0% | 0.597 |
| Healthy | 12 | 40.0% | 18 | 60.0% | ||
| Moderately healthy | 13 | 37.1% | 22 | 62.9% | ||
| Unhealthy | 0 | 0.0% | 1 | 100.0% | ||
| Frequent hydration during training and matches | No | 0 | 0.0% | 6 | 100.0% | 0.050 |
| Yes | 25 | 40.3% | 37 | 59.7% | ||
| Aerobic fitness levels | Excellent | 6 | 50.0% | 6 | 50.0% | 0.520 |
| Good | 11 | 36.7% | 19 | 63.3% | ||
| Acceptable | 8 | 30.8% | 18 | 69.2% | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Wit, D.; Pillay, J.D. Low Back Pain in South African Adolescent Field Hockey Players: Implications for Future Practice. J. Clin. Med. 2025, 14, 3309. https://doi.org/10.3390/jcm14103309
De Wit D, Pillay JD. Low Back Pain in South African Adolescent Field Hockey Players: Implications for Future Practice. Journal of Clinical Medicine. 2025; 14(10):3309. https://doi.org/10.3390/jcm14103309
Chicago/Turabian StyleDe Wit, Dale, and Julian D. Pillay. 2025. "Low Back Pain in South African Adolescent Field Hockey Players: Implications for Future Practice" Journal of Clinical Medicine 14, no. 10: 3309. https://doi.org/10.3390/jcm14103309
APA StyleDe Wit, D., & Pillay, J. D. (2025). Low Back Pain in South African Adolescent Field Hockey Players: Implications for Future Practice. Journal of Clinical Medicine, 14(10), 3309. https://doi.org/10.3390/jcm14103309