
A Comparison of Ultra-Widefield Imaging Quality Obtained with Zeiss Clarus and Optos for Virtual Medical Retina Services
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
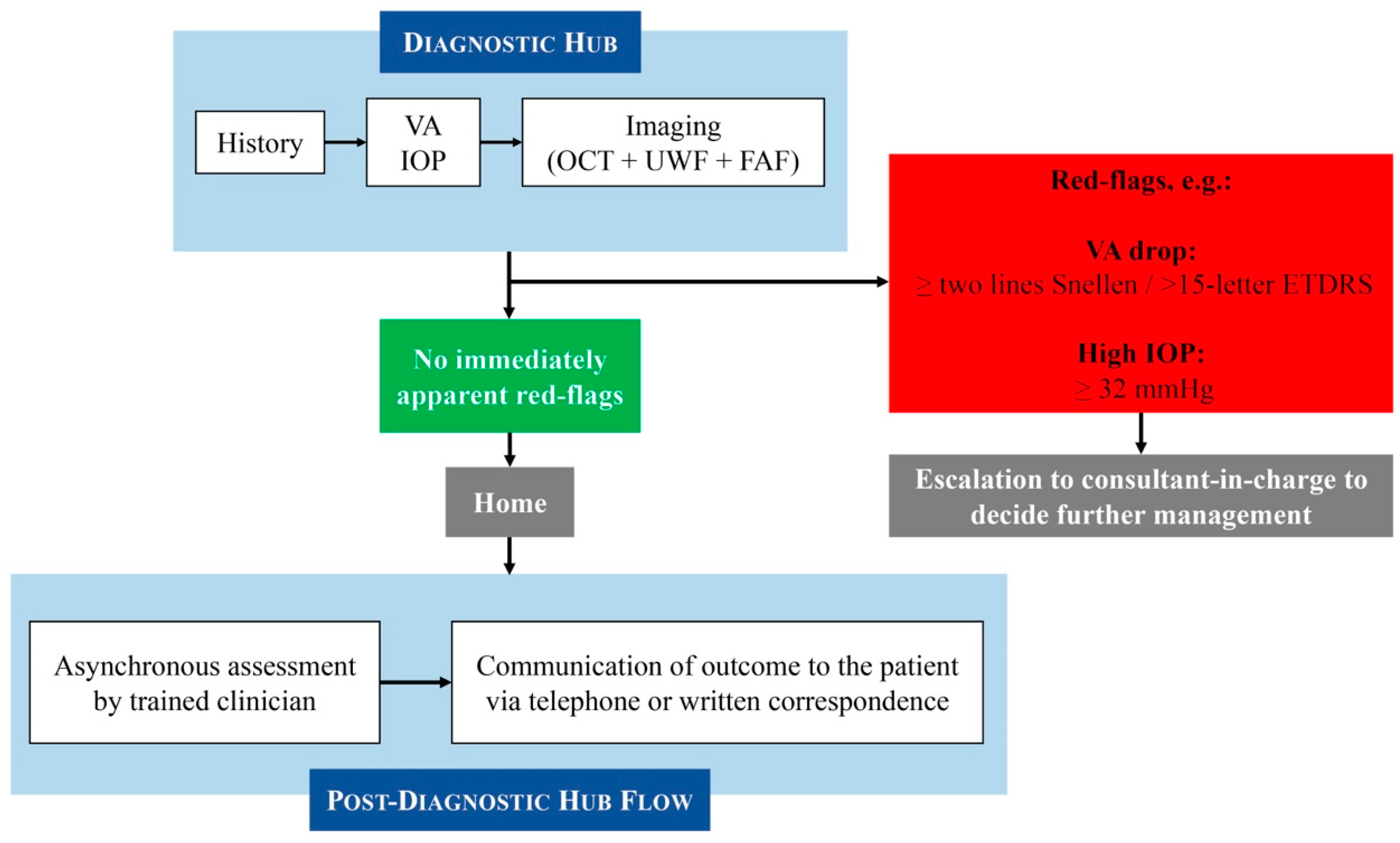
2.2. Moorfields Medical Retina Virtual Clinic Pathway
2.3. Ultrawide-Field Imaging
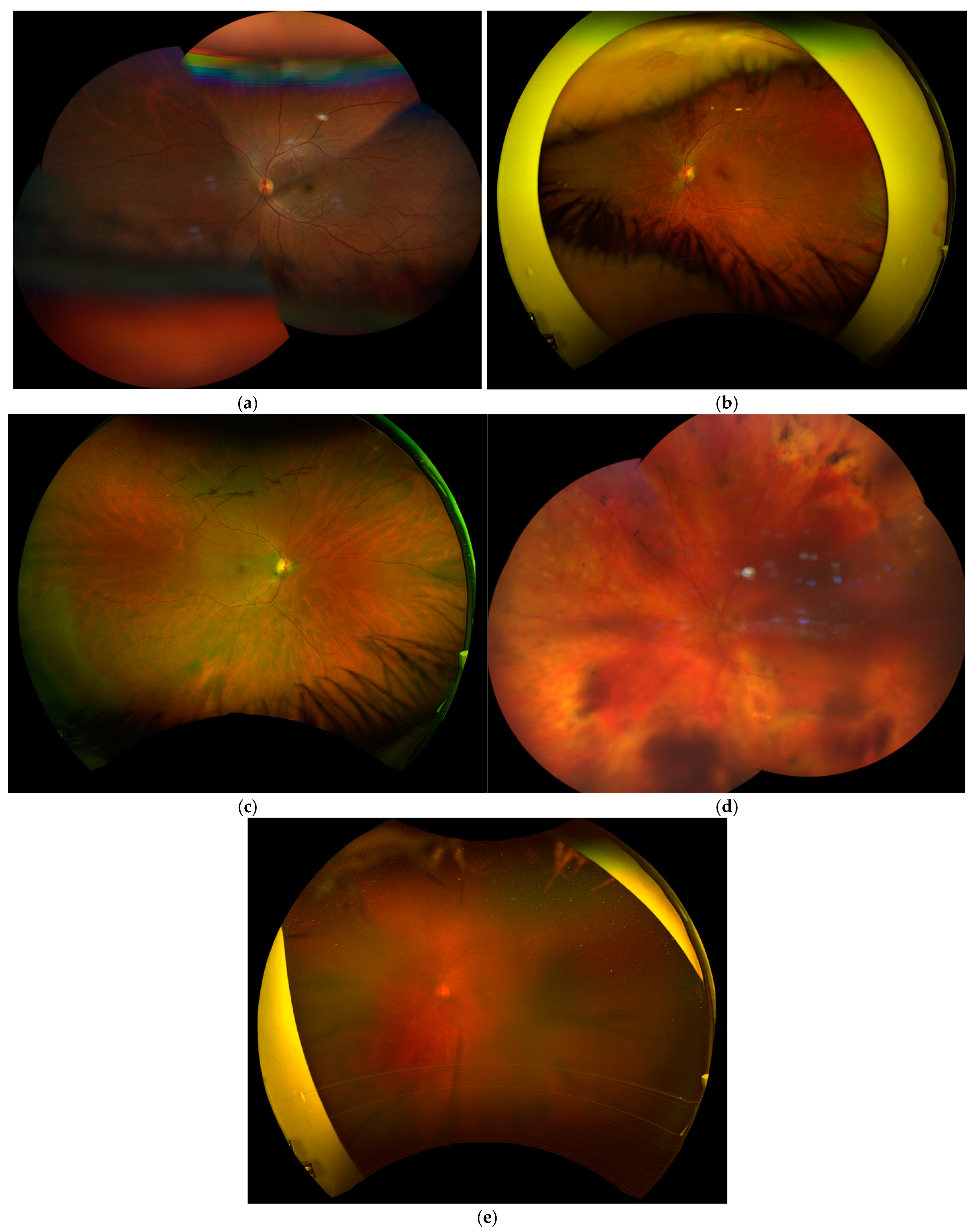
2.4. Imaging Quality Indices: Definitions and Examples
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics and Baseline Characteristics
3.2. Primary Retinal Diagnoses
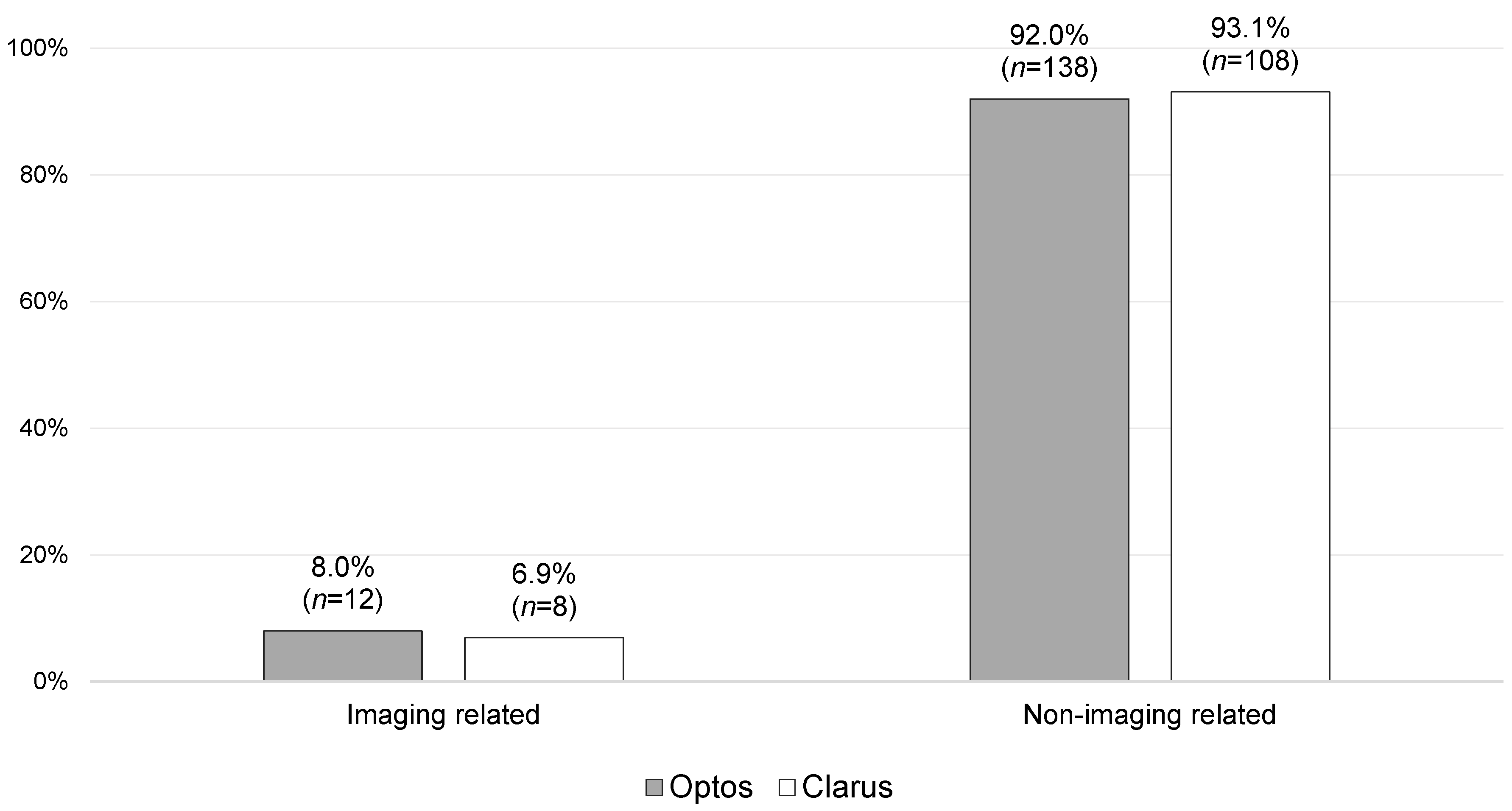
3.3. Primary Results
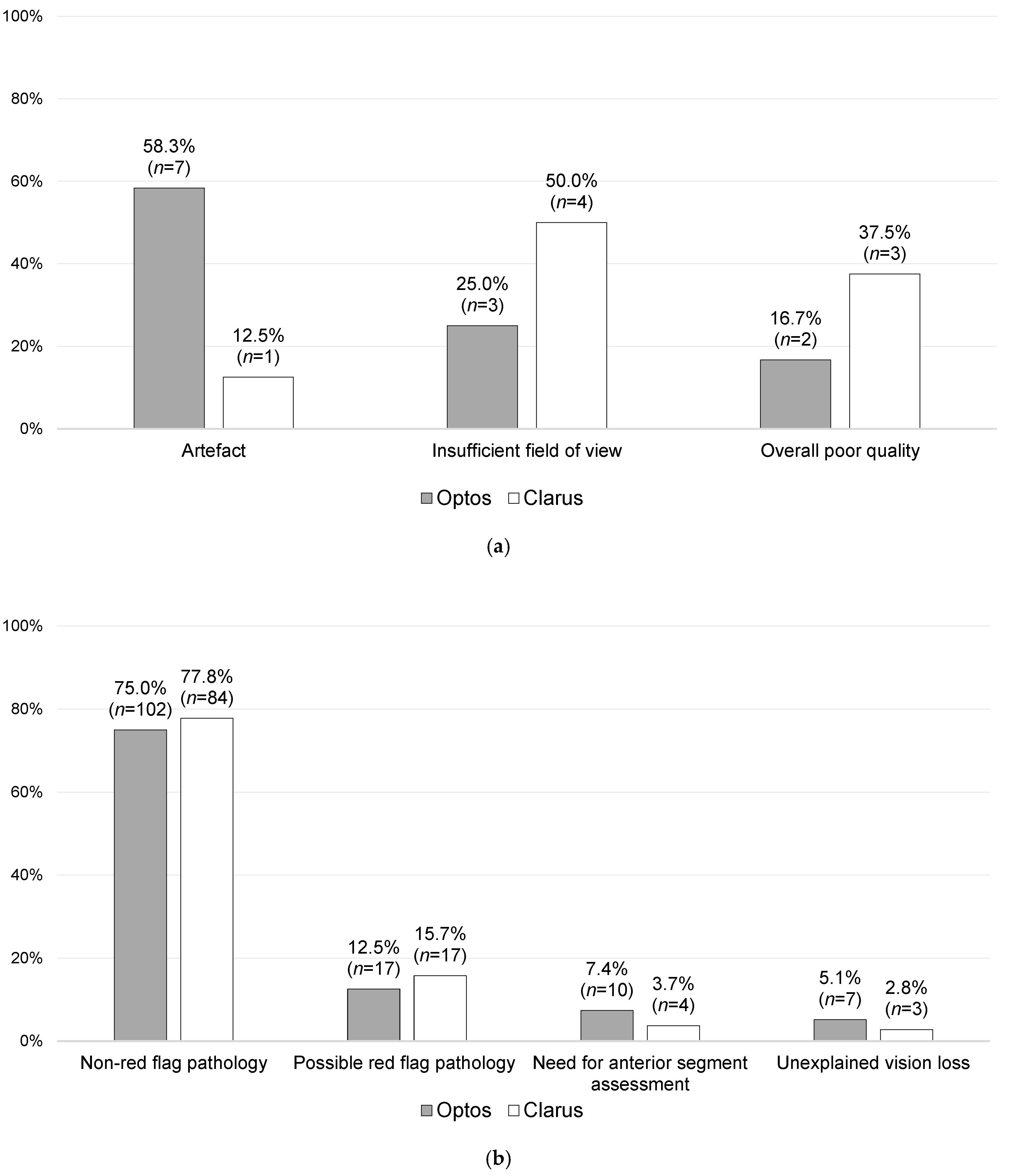
3.4. Secondary Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NHS England. Hospital Outpatient Activity 2023-24. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/hospital-outpatient-activity/2023-24 (accessed on 10 December 2024).
- Davis, A.; Baldwin, A.; Hingorani, M.; Dwyer, A.; Flanagan, D. A review of 145 234 ophthalmic patient episodes lost to follow-up. Eye 2017, 31, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Getting It Right First Time. Ophthalmology: GIRFT Programme National Specialty Report. Available online: https://gettingitrightfirsttime.co.uk/wp-content/uploads/2019/12/OphthalmologyReportGIRFT19P-FINAL.pdf (accessed on 10 December 2024).
- Foot, B.; MacEwen, C. Surveillance of sight loss due to delay in ophthalmic treatment or review: Frequency, cause and outcome. Eye 2017, 31, 771–775. [Google Scholar] [CrossRef]
- Tsaousis, K.T.; Empeslidis, T.; Konidaris, V.E.; Kapoor, B.; Deane, J. The concept of virtual clinics in monitoring patients with age-related macular degeneration. Acta Ophthalmol. 2016, 94, e353–e355. [Google Scholar] [CrossRef]
- Kern, C.; Kortuem, K.; Hamilton, R.; Fasolo, S.; Cai, Y.; Balaskas, K.; Keane, P.; Sim, D. Clinical Outcomes of a Hospital-Based Teleophthalmology Service: What Happens to Patients in a Virtual Clinic? Ophthalmol. Retin. 2019, 3, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Hanumunthadu, D.; Adan, K.; Tinkler, K.; Balaskas, K.; Hamilton, R.; Nicholson, L. Outcomes following implementation of a high-volume medical retina virtual clinic utilising a diagnostic hub during COVID-19. Eye 2022, 36, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Gale, R.; Scanlon, P.H.; Evans, M.; Ghanchi, F.; Yang, Y.; Silvestri, G.; Freeman, M.; Maisey, A.; Napier, J. Action on diabetic macular oedema: Achieving optimal patient management in treating visual impairment due to diabetic eye disease. Eye 2017, 31, S1–S20. [Google Scholar] [CrossRef]
- Kortuem, K.; Fasler, K.; Charnley, A.; Khambati, H.; Fasolo, S.; Katz, M.; Balaskas, K.; Rajendram, R.; Hamilton, R.; Keane, P.A.; et al. Implementation of medical retina virtual clinics in a tertiary eye care referral centre. Br. J. Ophthalmol. 2018, 102, 1391–1395. [Google Scholar] [CrossRef]
- Lee, J.X.; Manjunath, V.; Talks, S.J. Expanding the role of medical retina virtual clinics using multimodal ultra-widefield and optical coherence tomography imaging. Clin. Ophthalmol. 2018, 12, 2337–2345. [Google Scholar] [CrossRef]
- Hussain, G.; Chong, Y.J.; Nosrati, N.; Bennett, M.; Rossiter, J.; Sivaraj, R. Implementation of ophthalmic diagnostic hub after COVID-19 pandemic: Efficiency, DNA and attendances. Eye 2023, 37, 3506–3508. [Google Scholar] [CrossRef]
- Kotecha, A.; Baldwin, A.; Brookes, J.; Foster, P.J. Experiences with developing and implementing a virtual clinic for glaucoma care in an NHS setting. Clin. Ophthalmol. 2015, 9, 1915–1923. [Google Scholar] [CrossRef]
- Shah, V.; Jackson, T.L.; Edwards, R.T.; Attlee, J.; Kailani, O. Health economics of virtual versus face-to-face glaucoma clinics: A time-driven activity-based costing study. BMJ Open Ophthalmol. 2024, 9, e001800. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, N.; Duker, J.S.; Freund, K.B.; Kiss, S.; Querques, G.; Rosen, R.; Sarraf, D.; Souied, E.H.; Stanga, P.E.; Staurenghi, G.; et al. Classification and Guidelines for Widefield Imaging: Recommendations from the International Widefield Imaging Study Group. Ophthalmol. Retin. 2019, 3, 843–849. [Google Scholar] [CrossRef]
- Borrelli, E.; Querques, L.; Lattanzio, R.; Cavalleri, M.; Grazioli Moretti, A.; Di Biase, C.; Signorino, A.; Gelormini, F.; Sacconi, R.; Bandello, F.; et al. Nonmydriatic widefield retinal imaging with an automatic white LED confocal imaging system compared with dilated ophthalmoscopy in screening for diabetic retinopathy. Acta Diabetol. 2020, 57, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.S.; Cavallerano, J.D.; Sun, J.K.; Noble, J.; Aiello, L.M.; Aiello, L.P. Nonmydriatic ultrawide field retinal imaging compared with dilated standard 7-field 35-mm photography and retinal specialist examination for evaluation of diabetic retinopathy. Am. J. Ophthalmol. 2012, 154, 549–559.e2. [Google Scholar] [CrossRef]
- Veeramani, P.; Pilar Martin-Gutierrez, M.; Agorogiannis, E.; Hamilton, R.; Griggs, T.; Nicholson, L.; Heng, L.Z. Efficacy and Safety outcomes of a novel model to assess new medical retina referrals in a high-volume medical retina virtual clinic. Eye 2024, 38, 168–172. [Google Scholar] [CrossRef]
- Murray, D. NHS England Publishes Guidance on Reducing ‘Did Not Attends’ in Outpatient Services. Available online: https://www.rcophth.ac.uk/news-views/nhs-england-publishes-guidance-on-reducing-did-not-attends-in-outpatient-services/ (accessed on 6 April 2025).
- Brown, F.; Wasag, N.; Bhatt, S.; Gallagher, K. QI short report: Virtual clinics are a safe and efficient method of expanding the hospital diabetic retinopathy service. Future Healthc. J. 2024, 11, 100019. [Google Scholar] [CrossRef]
- Chen, A.; Dang, S.; Chung, M.M.; Ramchandran, R.S.; Bessette, A.P.; DiLoreto, D.A.; Kleinman, D.M.; Sridhar, J.; Wykoff, C.C.; Kuriyan, A.E. Quantitative Comparison of Fundus Images by 2 Ultra-Widefield Fundus Cameras. Ophthalmol. Retin. 2021, 5, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Optos. Product Specifications: Optos California. Available online: https://www.optos.com/products/california/ (accessed on 13 February 2025).
- Carl Zeiss Meditec. Product Specifications: ZEISS CLARUS 500; Imaging Ultra-Wide Without Compromise. Available online: https://www.zeiss.com/meditec/en/products/retinal-cameras/clarus-500.html (accessed on 13 February 2025).
- Matsui, Y.; Ichio, A.; Sugawara, A.; Uchiyama, E.; Suimon, H.; Matsubara, H.; Sugimoto, M.; Ikesugi, K.; Kondo, M. Comparisons of Effective Fields of Two Ultra-Widefield Ophthalmoscopes, Optos 200Tx and Clarus 500. BioMed Res. Int. 2019, 2019, 7436293. [Google Scholar] [CrossRef]
- Fantaguzzi, F.; Servillo, A.; Sacconi, R.; Tombolini, B.; Bandello, F.; Querques, G. Comparison of peripheral extension, acquisition time, and image chromaticity of Optos, Clarus, and EIDON systems. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 1289–1297. [Google Scholar] [CrossRef]
- National Academy of Engineering (US) and Institute of Medicine (US) Committee on Engineering and the Health Care System. The National Academies Collection: Reports Funded by National Institutes of Health. In Building a Better Delivery System: A New Engineering/Health Care Partnership; Reid, P.P., Compton, W.D., Grossman, J.H., Fanjiang, G., Eds.; National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Kossiakoff, A.S.; William, N. Systems Engineering: Principles and Practice (Wiley Series in Systems Engineering and Management); Wiley–Blackwell: Hoboken, NJ, USA, 2002; p. 488. [Google Scholar]
- Nagiel, A.; Lalane, R.A.; Sadda, S.R.; Schwartz, S.D. ULTRA-WIDEFIELD FUNDUS IMAGING: A Review of Clinical Applications and Future Trends. Retina 2016, 36, 660–678. [Google Scholar] [CrossRef]
- Stino, H.; Riessland, S.; Sedova, A.; Datlinger, F.; Sacu, S.; Schmidt-Erfurth, U.; Pollreisz, A. Comparison of two ultra-widefield color-fundus imaging devices for visualization of retinal periphery and microvascular lesions in patients with early diabetic retinopathy. Sci. Rep. 2022, 12, 17449. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Raman, S.; Karamcheti, S.K.M.; Srinivasan, S.; Sharma, A.; Surya, J.; Bhende, M.; Ramasamy, K.; Verma, A.; Raman, R. Comparison of Two Ultra-Widefield Cameras with High Image Resolution and Wider View for Identifying Diabetic Retinopathy Lesions. Transl. Vis. Sci. Technol. 2021, 10, 9. [Google Scholar] [CrossRef]
- Duncan, N.; Barrett, N.; Schildroth, K.; Chang, J.S.; Channa, R.; Rickels, K.; Domalpally, A.; Blodi, B. Comparison of Standard 7-Field, Clarus, and Optos Ultrawidefield Imaging Systems for Diabetic Retinopathy (COCO Study). Ophthalmol. Sci. 2024, 4, 100427. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Chopra, R.; Spitz, T.; Winkens, J.; Obika, A.; Kelly, C.; Askham, H.; Lukic, M.; Huemer, J.; Fasler, K.; et al. Predicting conversion to wet age-related macular degeneration using deep learning. Nat. Med. 2020, 26, 892–899. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Quality Index | Definition |
|---|---|
| Good image quality | Clear and wide field of view that enables confident clinical decision-making |
| Poor image quality | Generalised unclear view of the fundus, which precludes confident clinical decision-making |
| Insufficient field of view (FoV) | Area captured in the images does not incorporate a full view up to the vortex veins |
| Artefact | Focal anomalies due to the imaging process are not thought to be naturally present and are not due to obvious or known clinical pathology |
| Parameter [Valid Cohort; Missing Data] | Total Population [n (%)] | Optos Imaging Subgroup [n (%)] | Clarus Imaging Subgroup [n (%)] | p-Value (Optos vs. Clarus) |
|---|---|---|---|---|
| Age (years) [n = 268] | p = 0.28 | |||
| Average ± SD (range) | 63 ± 17 (16–98) | 65 ± 16 (16–96) | 63 ± 18 (19–98) | |
| Ethnicity [n = 267; missing = 1] | p = 0.38 | |||
| White | 73 (27.3%) | 45 (29.8%) | 28 (24.1%) | |
| Black | 30 (11.2%) | 13 (8.6%) | 17 (14.7%) | |
| Asian | 73 (27.3%) | 43 (28.5%) | 30 (25.9%) | |
| Other | 91 (34.1%) | 50 (33.1%) | 41 (35.3%) | |
| Virtual clinic site [n = 268] | p = 0.001 | |||
| Moorfields City Road | 137 (51.1%) | 114 (75.0%) | 23 (19.8%) | |
| Moorfields Brent Cross | 18 (6.7%) | 18 (11.8%) | 0 (0.0%) | |
| Moorfields Hoxton | 74 (27.6%) | 6 (3.9%) | 68 (58.6%) | |
| Moorfields Stratford | 22 (8.2%) | 1 (0.7%) | 21 (18.1%) | |
| Moorfields Ealing | 13 (4.9%) | 13 (8.6%) | 0 (0.0%) | |
| Moorfields Northwick Park | 4 (1.5%) | 0 (0.0%) | 4 (3.4%) | |
| New versus follow-up patients [n = 268] | p = 0.005 | |||
| New patient | 56 (20.9%) | 41 (27.0%) | 15 (12.9%) | |
| Follow-up patient | 212 (79.1%) | 111 (73.0%) | 101 (87.1%) |
| Indication [n = 268] | Number (%) | Optos Imaging Subgroup Number (%) | Clarus Imaging Subgroup Number (%) |
|---|---|---|---|
| Diabetic Retinopathy/Maculopathy | 85 (31.7%) | 42 (27.6%) | 43 (37.1%) |
| Age-related macular degeneration | 40 (14.9%) | 20 (13.2%) | 20 (17.2%) |
| Central serous chorioretinopathy | 37 (13.8%) | 19 (12.5%) | 18 (15.5%) |
| Retinal vein occlusion | 29 (10.8%) | 19 (12.5%) | 10 (8.6%) |
| Myopia | 15 (5.6%) | 9 (5.9%) | 6 (5.2%) |
| Retinal lesions | 10 (3.7%) | 7 (4.6%) | 3 (2.6%) |
| Vitreoretinal | 6 (2.2%) | 5 (3.3%) | 1 (0.9%) |
| Hydroxychloroquine screening | 6 (2.2%) | 5 (3.3%) | 1 (0.9%) |
| Other | 40 (14.9%) | 26 (17.1%) | 14 (12.1%) |
| Parameter | Optos California (Optos®, Dunfermline, Scotland, UK) | Zeiss Clarus 500 (Carl Zeiss Meditec AG, Oberkochen, Germany) |
|---|---|---|
| Retinal area captured | Larger (765.6 mm2) [20] | Smaller (566.5 mm2) [20] |
| Field of view (FoV) | 200° single-capture; capacity to create a multiple-image montage in order to create a 220° FoV [21] | 133° single-capture; can produce a UWF photo (200°) through a 2-image-montage, with the ability to increase this to a 267° image (six-image montage) [22] |
| True colour vs. pseudo-colour | Pseudo-colour images are produced due to the use of a red-green or red-green-blue laser as a light source [21,22] | Captures true-colour images due to its white light-emitting diode (LED) light source [21,22] |
| Optical resolution | 14 microns [21] | 7.3 microns [22] |
| Image centre | Fovea [23] | Slightly nasal to the fovea on a 200° montage [23] |
| Acquisition technique | Patient’s face is pressed against a stationary machine, and photos are captured with one click after focusing the lens [21] | 25 mm working distance between the front of the lens and the patient’s eye; the technician has to swing the body of the camera right and left to be able to record at least two images for a 200° montage [22] |
| Acquisition time | Shorter acquisition time (median 32 s) [24] | Longer acquisition time (median 42 s) [24] |
| Other functions |
|
|
| Other models | Silverstone, MonacoPro, Daytona | Zeiss Clarus 700 (added fluorescein angiography function) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzopardi, M.; Gridhar, S.; Tsika, C.; Koutsocheras, G.; Katzakis, M.; Demir, B.; Rahman, W.; Heng, L.Z.; Chong, Y.J.; Logeswaran, A. A Comparison of Ultra-Widefield Imaging Quality Obtained with Zeiss Clarus and Optos for Virtual Medical Retina Services. J. Clin. Med. 2025, 14, 3270. https://doi.org/10.3390/jcm14103270
Azzopardi M, Gridhar S, Tsika C, Koutsocheras G, Katzakis M, Demir B, Rahman W, Heng LZ, Chong YJ, Logeswaran A. A Comparison of Ultra-Widefield Imaging Quality Obtained with Zeiss Clarus and Optos for Virtual Medical Retina Services. Journal of Clinical Medicine. 2025; 14(10):3270. https://doi.org/10.3390/jcm14103270
Chicago/Turabian StyleAzzopardi, Matthew, Sneha Gridhar, Chrysanthi Tsika, Georgios Koutsocheras, Michail Katzakis, Bahar Demir, Waheeda Rahman, Ling Zhi Heng, Yu Jeat Chong, and Abison Logeswaran. 2025. "A Comparison of Ultra-Widefield Imaging Quality Obtained with Zeiss Clarus and Optos for Virtual Medical Retina Services" Journal of Clinical Medicine 14, no. 10: 3270. https://doi.org/10.3390/jcm14103270
APA StyleAzzopardi, M., Gridhar, S., Tsika, C., Koutsocheras, G., Katzakis, M., Demir, B., Rahman, W., Heng, L. Z., Chong, Y. J., & Logeswaran, A. (2025). A Comparison of Ultra-Widefield Imaging Quality Obtained with Zeiss Clarus and Optos for Virtual Medical Retina Services. Journal of Clinical Medicine, 14(10), 3270. https://doi.org/10.3390/jcm14103270