
Relationship Between Health-Related Quality of Life and Exercise Tolerance Improvement in Remote Cardiac Rehabilitation: Sub-Analysis of RecRCR Study

 , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
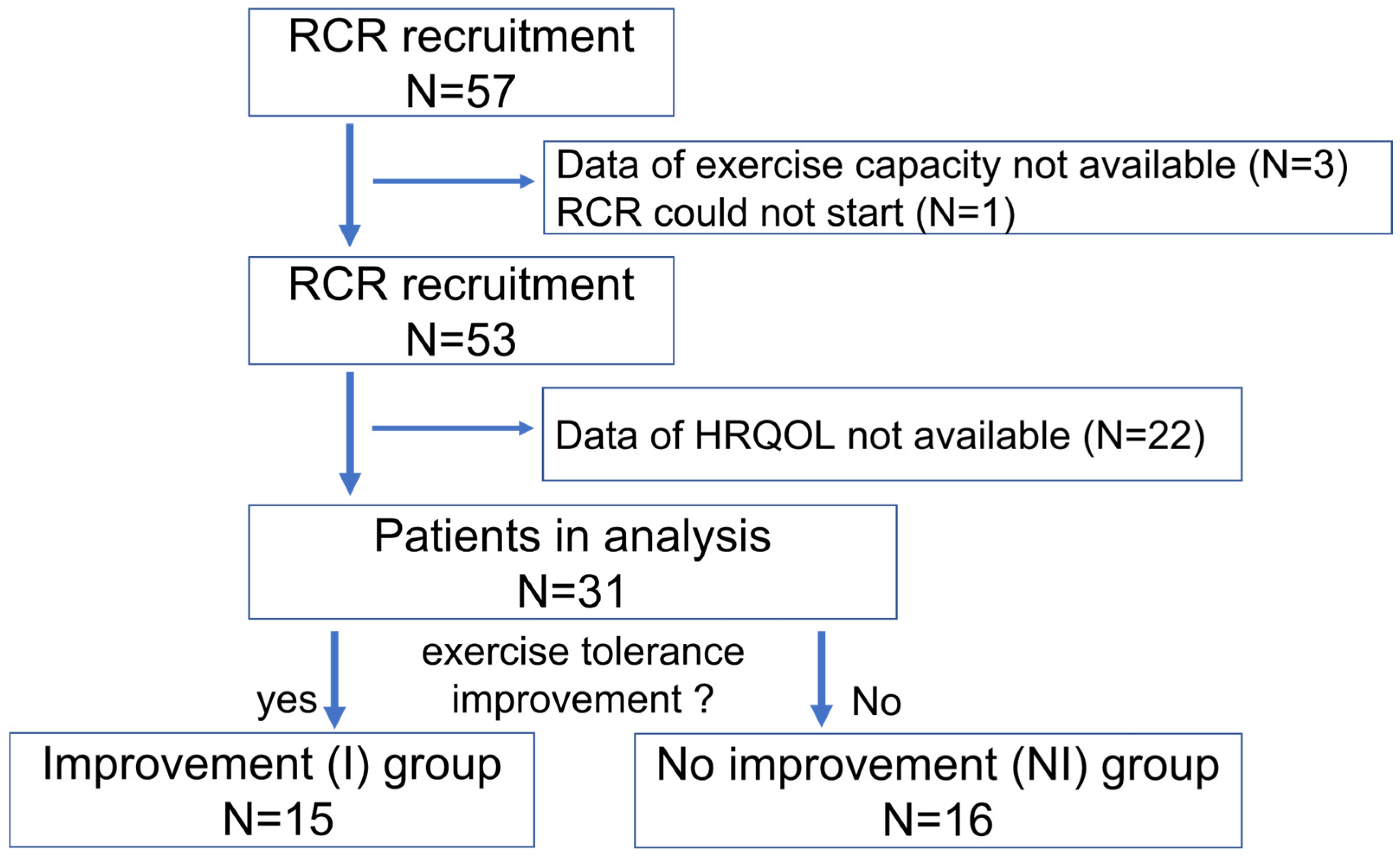
2.1. Study Patients
2.2. Intervention
2.3. Health-Related QOL Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
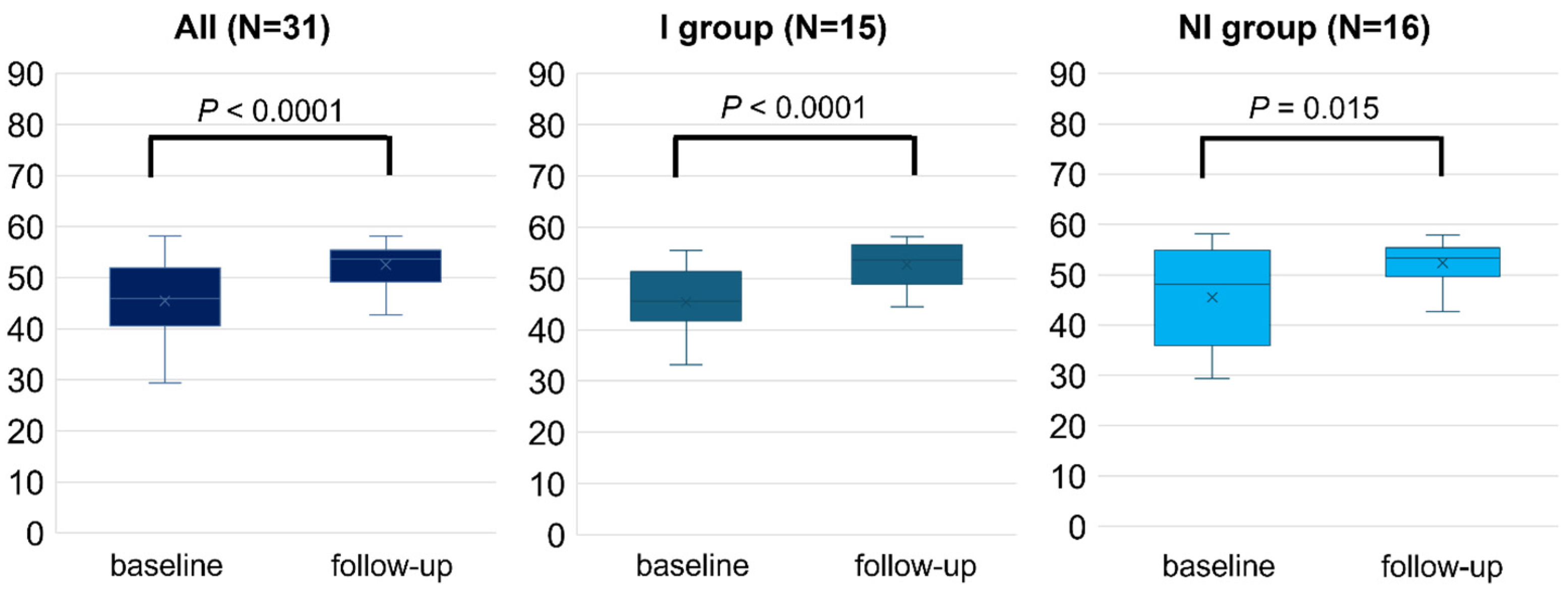
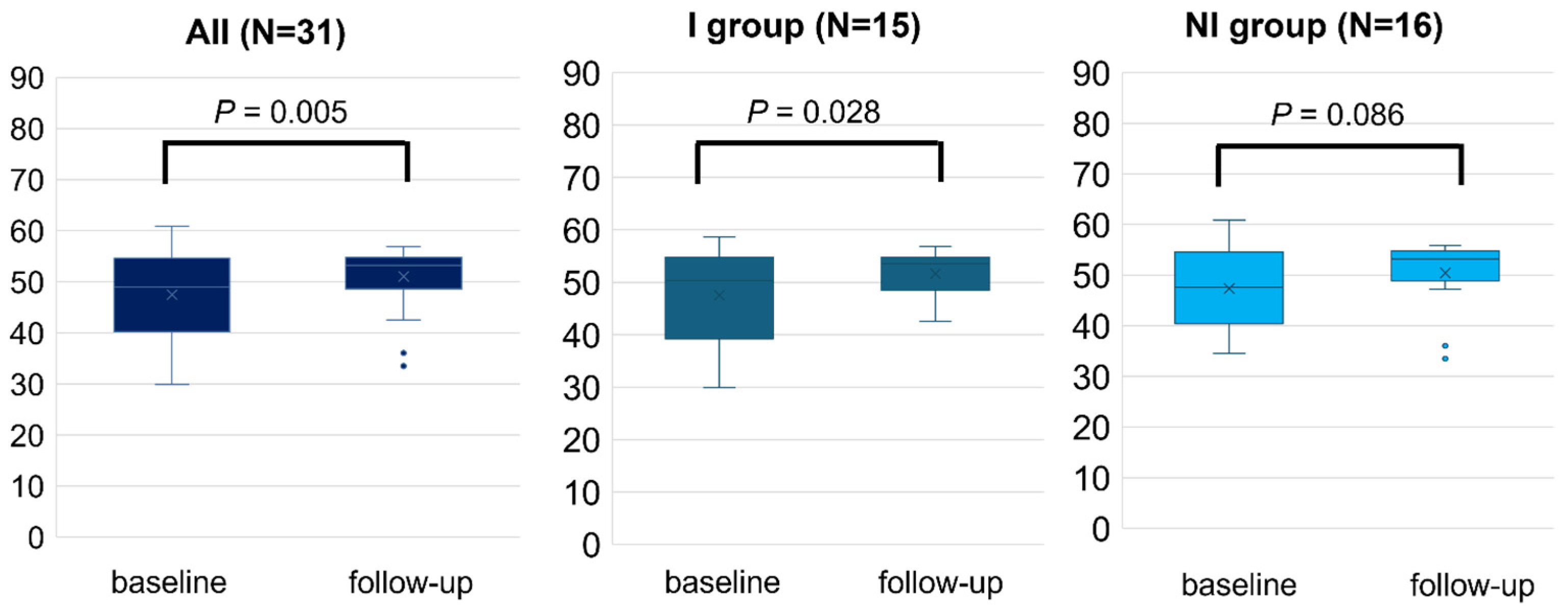
3.2. HRQOL Measured by SF-8
3.3. Correlations Between Changes in PCS, MCS and Various Parameters
4. Discussion
4.1. Change in HRQOL During RCR
4.2. Relationship Between HRQOL Score and Exercise Capacity During RCR
4.3. Limitaions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACEi | angiotensin converting enzyme inhibitor |
| Alb | albumin |
| ARB | angiotensin II receptor blocker |
| ARNI | angiotensin receptor/neprilysin inhibitor |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| BNP | B-type natriuretic peptide |
| CPET | cardiopulmonary exercise testing |
| CR | cardiac rehabilitation |
| CVD | cardiovascular diseases |
| dBP | diastolic blood pressure |
| eGFR | estimated glomerular filtration rate |
| Hb | hemoglobin |
| HRQOL | health related quality of life |
| LDL | low density lipoprotein |
| LVEF | left ventricular ejection fraction |
| MCS | mental health component summary score |
| NT-proBNP | N-terminal pro-brain natriuretic peptide |
| PCS | physical health component summary score |
| QOL | quality of life |
| RCR | remote cardiac rehabilitation |
| sBP | systolic blood pressure |
| SF-8 | Short-Form Health Survey-8 |
| SGLT2i | sodium-glucose cotransporter-2 inhibitor |
| UA | uric acid |
| VO2 | oxygen consumption |
| 6MWT | 6-minute walk test |
References
- Nieminen, M.S.; Dickstein, K.; Fonseca, C.; Serrano, J.M.; Parissis, J.; Fedele, F.; Wikström, G.; Agostoni, P.; Atar, S.; Baholli, L.; et al. The patient perspective: Quality of life in advanced heart failure with frequent hospitalisations. Int. J. Cardiol. 2015, 191, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.; Brieger, D.B.; Owen, R.; Chen, J.; Cohen, M.G.; Goodman, S.; Granger, C.B.; Nicolau, J.C.; Simon, T.; Westermann, D.; et al. Health-related quality of life 1–3 years post-myocardial infarction: Its impact on prognosis. Open Heart 2021, 8, e001499. [Google Scholar] [CrossRef]
- Thomas, R.J. Cardiac Rehabilitation—Challenges, Advances; and the Road Ahead. N. Engl. J. Med. 2024, 390, 830–841. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.M.; Franklin, B.; Sanderson, B.; Southard, D.; American Heart Association Exercise; et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation; and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing; Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2007, 115, 2675–2682. [Google Scholar] [PubMed]
- Endo, N.; Goto, A.; Suzuki, T.; Matsuda, S.; Yasumura, S. Factors associated with enrollment and adherence in outpatient cardiac rehabilitation in Japan. J. Cardiopulm. Rehabil. Prev. 2015, 35, 186–192. [Google Scholar] [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation; the American Heart Association; and the American College of Cardiology. Circulation 2019, 140, e69–e89. [Google Scholar] [CrossRef]
- McDonagh, S.T.; Dalal, H.; Moore, S.; Clark, C.E.; Dean, S.G.; Jolly, K.; Cowie, A.; Afzal, J.; Taylor, R.S. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst. Rev. 2023, 10, CD007130. [Google Scholar]
- Itoh, H.; Amiya, E.; Jimba, T.; Shimbo, M.; Narita, K.; Taya, M.; Kadokami, T.; Yasu, T.; Oka, H.; Sogawa, M.; et al. Efficacy and safety of remote cardiac rehabilitation in the recovery phase of cardiovascular diseases (RecRCR study): A multicenter; nonrandomized; and interventional trial in Japan. Int. J. Cardiol. Heart Vasc. 2024, 52, 101421. [Google Scholar] [CrossRef]
- Itoh, H.; Amiya, E.; Narita, K.; Shimbo, M.; Taya, M.; Komuro, I.; Hasegawa, T.; Makita, S.; Kimura, Y. Efficacy and Safety of Remote Cardiac Rehabilitation in the Recovery Phase of Cardiovascular Diseases: Protocol for a Multicenter; Nonrandomized; Single-Arm; Interventional Trial. JMIR Res. Protoc. 2021, 10, e30725. [Google Scholar] [CrossRef]
- Hilu, R.; Haskiah, F.; Khaskia, A.; Assali, A.; Baron, I.; Gabarin, M.; Chen, J.; Pereg, D. Effectiveness and Safety of Remote Cardiac Rehabilitation for Patients After Acute Coronary Syndrome. Am. J. Cardiol. 2023, 207, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Suzukamo, Y. Manual of the SF-8 Japanese Version; Qualitest: Kyoto, Japan, 2004; Volume 2021. [Google Scholar]
- Makita, S.; Yasu, T.; Akashi, Y.J.; Adachi, H.; Izawa, H.; Ishihara, S.; Iso, Y.; Ohuchi, H.; Omiya, K.; Ohya, Y.; et al. JCS/JACR2021 Guideline on Rehabilitation in Patients With Cardiovascular Disease. Circ. J. 2022, 87, 155–235. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Su, Y.; Hu, Z.; Sun, X.; Li, X.; Dolansky, M.A.; Qu, M.; Hu, X. Home-based telehealth exercise training program in Chinese patients with heart failure: A randomized controlled trial. Medicine 2018, 97, e12069. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Walker, S.; Smart, N.A.; Piepoli, M.F.; Warren, F.C.; Ciani, O.; Whellan, D.; O’Connor, C.; Keteyian, S.J.; Coats, A.; et al. Impact of Exercise Rehabilitation on Exercise Capacity and Quality-of-Life in Heart Failure: Individual Participant Meta-Analysis. J. Am. Coll. Cardiol. 2019, 73, 1430–1443. [Google Scholar] [CrossRef]
- Mansilla-Chacón, M.; Gómez-Urquiza, J.L.; Martos-Cabrera, M.B.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De La Fuente, G.A.; Suleiman-Martos, N. Effects of Supervised Cardiac Rehabilitation Programmes on Quality of Life among Myocardial Infarction Patients: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 166. [Google Scholar] [CrossRef]
- Chen, Y.W.; Wang, C.Y.; Lai, Y.H.; Liao, Y.C.; Wen, Y.K.; Chang, S.T.; Huang, J.L.; Wu, T.J. Home-based cardiac rehabilitation improves quality of life; aerobic capacity; and readmission rates in patients with chronic heart failure. Medicine 2018, 97, e9629. [Google Scholar] [CrossRef]
- Hurdus, B.; Munyombwe, T.; Dondo, T.B.; Aktaa, S.; Oliver, G.; Hall, M.; Doherty, P.; Hall, A.S.; Gale, C.P. Association of cardiac rehabilitation and health-related quality of life following acute myocardial infarction. Heart 2020, 106, 1726–1731. [Google Scholar] [CrossRef]
- Santiago de Araújo Pio, C.; Chaves, G.S.; Davies, P.; Taylor, R.S.; Grace, S.L. Interventions to promote patient utilisation of cardiac rehabilitation. Cochrane Database Syst. Rev. 2019, 2, CD007131. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Pencina, M.J.; Opolski, G.; Zareba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Szalewska, D.; Pluta, S.; Glówczynska, R.; et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients [TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 300–308. [Google Scholar] [CrossRef]
- Rawstorn, J.C.; Gant, N.; Rolleston, A.; Whittaker, R.; Stewart, R.; Benatar, J.; Warren, I.; Meads, A.; Jiang, Y.; Maddison, R. End Users Want Alternative Intervention Delivery Models: Usability and Acceptability of the REMOTE-CR Exercise-Based Cardiac Telerehabilitation Program. Arch. Phys. Med. Rehabil. 2018, 99, 2373–2377. [Google Scholar] [CrossRef]
- Benzer, W.; Philippi, A.; Hoefer, S.; Friedrich, O.; Oldridge, N. Health-related quality of life predicts unplanned rehospitalization following coronary revascularization. Herz 2016, 41, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Rumsfeld, J.S.; Alexander, K.P.; Goff, D.C., Jr.; Graham, M.M.; Ho, P.M.; Masoudi, F.A.; Moser, D.K.; Roger, V.L.; Slaughter, M.S.; Smolderen, K.G.; et al. Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American Heart Association. Circulation 2013, 127, 2233–2249. [Google Scholar] [CrossRef] [PubMed]
- German, C.A.; Brubaker, P.H.; Nelson, M.B.; Fanning, J.; Ye, F.; Kitzman, D.W. Relationships Between Objectively Measured Physical Activity; Exercise Capacity; and Quality of Life in Older Patients With Obese Heart Failure and Preserved Ejection Fraction. J. Card. Fail. 2021, 27, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.S.; Laustsen, S.; Petersen, A.K. Correlation Between Exercise Capacity and Quality of Life in Patients With Cardiac Disease. J. Cardiopulm. Rehabil. Prev. 2018, 38, 297–303. [Google Scholar] [CrossRef]
- Xiong, G.L.; Fiuzat, M.; Kuchibhatla, M.; Krishnan, R.; O’Connor, C.M.; Jiang, W.; SADHART-CHF Investigators. Health status and depression remission in patients with chronic heart failure: Patient-reported outcomes from the SADHART-CHF Trial. Circ. Heart Fail. 2012, 5, 688–692. [Google Scholar] [CrossRef]
- Fillies, B.; Stapel, B.; Lemke, L.H.; Löffler, F.; Bauersachs, J.; Kahl, K.G.; Westhoff-Bleck, M. Remission from depression is associated with improved quality of life and preserved exercise capacity in adults with congenital heart disease. Front. Cardiovasc. Med. 2024, 11, 1418342. [Google Scholar] [CrossRef]
- Guazzi, M.; Dickstein, K.; Vicenzi, M.; Arena, R. Six-minute walk test and cardiopulmonary exercise testing in patients with chronic heart failure: A comparative analysis on clinical and prognostic insights. Circ. Heart Fail. 2009, 2, 549–555. [Google Scholar] [CrossRef]
- Mariani, M.V.; Pierucci, N.; Forleo, G.B.; Schiavone, M.; Bernardini, A.; Gasperetti, A.; Mitacchione, G.; Mei, M.; Giunta, G.; Piro, A.; et al. The Feasibility, Effectiveness and Acceptance of Virtual Visits as Compared to In-Person Visits among Clinical Electrophysiology Patients during the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 620. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| I Group N = 15 | NI Group N = 16 | p-Value | |
|---|---|---|---|
| Age (years) | 61.8 ± 13.6 | 64.6 ± 14.7 | 0.582 |
| Gender male (%) | 12 (80.0%) | 14 (87.5%) | 0.654 |
| BMI (kg/m2) | 24.5 ± 5.2 | 23.8 ± 3.3 | 0.673 |
| Indication for CR (%) | 0.300 | ||
| Ischemic heart disease, n (%) | 9 (60.0%) | 6 (37.5%) | |
| Heart failure, n (%) | 5 (33.3%) | 6 (37.5%) | |
| Post cardiac surgery, n (%) | 1 (6.7%) | 1 (6.3%) | |
| Others, n (%) | 0 (0.0%) | 0 (0.0%) | |
| Risk factors | |||
| Hypertension, n (%) | 8 (53.3%) | 9 (56.3%) | 0.870 |
| Diabetes, n (%) | 4 (26.7%) | 3 (18.8%) | 0.598 |
| Lipid disorders, n (%) | 9 (60.0%) | 11 (68.8%) | 0.611 |
| Smoking never/past/current, n (%) | 6 (40.0%)/6 (40.0%)/3 (20.0%) | 8 (50.0%)/6 (37.5%)/2 (12.5%) | 0.797 |
| sBP (mmHg) | 113.1 ± 17.3 | 116.4 ± 15.8 | 0.584 |
| dBP (mmHg) | 68.7 ± 9.5 | 62.2 ± 9.7 | 0.068 |
| Heart rate (bpm) | 71.1 ± 7.4 | 67.1 ± 10.2 | 0.219 |
| LVEF (%) | 57.1 ± 17.6 | 56.8 ± 21.7 | 0.960 |
| Laboratory data | |||
| Hb (g/dL) | 13.3 ± 2.2 | 12.5 ± 1.4 | 0.237 |
| Alb (mg/dL) | 3.8 ± 0.4 | 3.7 ± 0.4 | 0.474 |
| eGFR (mL/min/1.73 m2) | 70.3 ± 17.8 | 68.9 ± 20.2 | 0.851 |
| AST (mg/dL) | 20.6 ± 6.9 | 24.3 ± 9.0 | 0.218 |
| ALT (mg/dL) | 22.0 ± 8.6 | 29.9 ± 17.9 | 0.143 |
| UA (mg/dL) | 6.5 ± 2.2 | 6.4 ± 1.5 | 0.954 |
| LDL (mg/dL) | 87.9 ± 33.1 | 86.6 ± 25.4 | 0.907 |
| HbA1c (%) | 6.2 ± 1.4 | 6.1 ± 0.6 | 0.769 |
| BNP (pg/dL) | 65.7 [11.4–227.0] (n = 10) | 54.9 [8.1–323.2] (n = 11) | 0.526 |
| NT-proBNP (pg/dL) | 560.0 [56.7–850.0] (n = 3) | 258.0 [8.4–3889.0] (n = 9) | 0.340 |
| Medications, n (%) | |||
| Beta blockers | 10 (66.7%) | 10 (62.5%) | 0.809 |
| ACE-i/ARB | 7 (46.7%) | 8 (50.0%) | 0.853 |
| ARNI | 1 (6.7%) | 2 (12.5%) | 0.583 |
| Ca blocker | 6 (40.0%) | 8 (50.0%) | 0.576 |
| Loop diuretics | 5 (33.3%) | 7 (43.8%) | 0.552 |
| SGLT2i | 2 (13.3%) | 3 (18.8%) | 0.682 |
| Exercise tolerance | |||
| Peak VO2 (mL/min/kg) | 14.8 ± 4.7 (n = 10) | 17.2 ± 5.1 (n = 11) | 0.269 |
| 6MWT distance (m) | 376.3 ± 102.7 (n = 6) | 372.0 ± 68.5 (n = 5) | 0.935 |
| SF-8 | |||
| PCS | 45.3 ± 6.4 | 45.5 ± 9.5 | 0.965 |
| MCS | 47.5 ± 8.5 | 47.3 ± 7.5 | 0.954 |
| Physical Functioning | 44.7 [44.7,54.3] | 44.7 [44.7,54.3] | 0.252 |
| Role Physical | 43.6 [43.6,54.9] | 47.8 [43.6,54.9] | 0.829 |
| Bodily Pain | 51.3 [45.0,59.1] | 52.1 [37.1,59.1] | 0.792 |
| General Health | 43.0 [43.0,52.7] | 43.0 [36.4,60.0] | 0.754 |
| Vitality | 47.4 [41.1,55.5] | 47.4 [42.7,53.5] | 0.967 |
| Social Functioning | 47.3 [33.1,55.2] | 55.2 [41.4,55.2] | 0.522 |
| Role Emotional | 49.0 [43.7,55.2] | 55.2 [36.5,55.2] | 0.9.9 |
| Mental Health | 51.2 [38.3,56.7] | 45.1 [40.0,56.7] | 0.586 |
| Number of RCR times | 26.9 ± 8.8 | 21.9 ± 8.3 | 0.133 |
| Days of RCR | 80.0 ± 20.5 | 77.9 ± 18.9 | 0.801 |
| Days from admission to RCR | 40.5 ± 22.7 | 33.1 ± 17.6 | 0.363 |
| All | I Group N = 15 | NI Group N = 16 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | |
| Physical Functioning | 44.7 [44.7,54.2] | 54.3 [48.7,54.3] | <0.001 * | 44.7 [44.7,54.3] | 54.3 [48.7,54.3] | 0.002 * | 44.7 [44.7,54.3] | 54.3 [50.1,54.3] | 0.002 * |
| Role Physical | 47.8 [43.6,54.9] | 54.9 [54.9,54.9] | 0.001 * | 43.6 [43.6,54.9] | 54.9 [54.9,54.9] | 0.003 * | 47.8 [43.6,54.9] | 54.9 [49.6,54.9] | 0.078 |
| Bodily Pain | 51.3 [37.1,59.1] | 59.1 [51.3,59.1] | 0.027 * | 51.3 [45.0,59.1] | 59.1 [51.3,59.1] | 0.168 | 52.1 [37.1,59.1] | 59.1 [46.6,59.1] | 0.094 |
| General Health | 43.0 [43.0,52.7] | 52.7 [52.7,60.0] | <0.001 * | 43.0 [41.1,55.5] | 52.7 [52.7,60.0] | <0.001 * | 43.0 [43.0,52.7] | 52.7 [52.7,60.0] | 0.003 * |
| Vitality | 47.4 [41.1,55.4] | 55.5 [47.4,55.5] | <0.001 * | 47.4 [41.1,55.2] | 55.2 [47.3,55.2] | 0.001 * | 47.4 [42.7,53.5] | 55.5 [47.4,55.5] | 0.025 * |
| Social Functioning | 47.3 [41.4,55.2] | 55.2 [47.3,55.2] | 0.004 * | 47.3 [33.1,55.2] | 55.2 [49.0,55.2] | 0.016 * | 55.2 [41.4,55.2] | 55.2 [49.2,55.2] | 0.096 |
| Role Emotional | 55.2 [43.7,55.2] | 55.2 [49.0,55.2] | 0.015 * | 49.0 [43.7,55.2] | 56.7 [51.2,56.7] | 0.015 * | 55.2 [36.5,55.2] | 55.2 [49.0,55.2] | 0.102 |
| Mental Health | 45.1 [38.3,56.7] | 56.7 [51.2,56.7] | 0.003 * | 51.2 [38.3,55.5] | 55.5 [55.5,58.1] | 0.029 * | 45.1 [40.0,56.7] | 56.7 [46.7,56.7] | 0.047 * |
| Changes in PCS (N = 31) | Changes in MCS (N = 31) | |||
|---|---|---|---|---|
| rs | p-Value | rs | p-Value | |
| Age (years) | 0.19 | 0.301 | 0.17 | 0.359 |
| BMI (kg/m2) | 0.01 | 0.997 | −0.06 | 0.757 |
| LVEF (Teichholz) (%) (N = 29) | −0.51 | 0.792 | 0.39 | 0.036 |
| Peak VO2 (mL/min/kg) (N = 21) | −0.11 | 0.626 | −0.11 | 0.626 |
| Number of RCR times | 0.35 | 0.071 | 0.09 | 0.637 |
| Days of RCR | 0.04 | 0.861 | −0.04 | 0.857 |
| Days from admission to RCR | −0.17 | 0.388 | −0.51 | 0.007 |
| Changes in peak VO2 (N = 20) | −0.19 | 0.416 | −0.04 | 0.870 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimbo, M.; Amiya, E.; Jimba, T.; Itoh, H.; Narita, K.; Taya, M.; Kadokami, T.; Yasu, T.; Oka, H.; Sogawa, M.; et al. Relationship Between Health-Related Quality of Life and Exercise Tolerance Improvement in Remote Cardiac Rehabilitation: Sub-Analysis of RecRCR Study. J. Clin. Med. 2025, 14, 3265. https://doi.org/10.3390/jcm14103265
Shimbo M, Amiya E, Jimba T, Itoh H, Narita K, Taya M, Kadokami T, Yasu T, Oka H, Sogawa M, et al. Relationship Between Health-Related Quality of Life and Exercise Tolerance Improvement in Remote Cardiac Rehabilitation: Sub-Analysis of RecRCR Study. Journal of Clinical Medicine. 2025; 14(10):3265. https://doi.org/10.3390/jcm14103265
Chicago/Turabian StyleShimbo, Mai, Eisuke Amiya, Takahiro Jimba, Hidetaka Itoh, Koichi Narita, Masanobu Taya, Toshiaki Kadokami, Takanori Yasu, Hideki Oka, Masakazu Sogawa, and et al. 2025. "Relationship Between Health-Related Quality of Life and Exercise Tolerance Improvement in Remote Cardiac Rehabilitation: Sub-Analysis of RecRCR Study" Journal of Clinical Medicine 14, no. 10: 3265. https://doi.org/10.3390/jcm14103265
APA StyleShimbo, M., Amiya, E., Jimba, T., Itoh, H., Narita, K., Taya, M., Kadokami, T., Yasu, T., Oka, H., Sogawa, M., Yokoi, H., Mizutani, K., Miura, S.-i., Tokeshi, T., Date, A., Noma, T., Kutsuzawa, D., Usui, S., Sugawara, S., ... RecRCR Registry Investigators. (2025). Relationship Between Health-Related Quality of Life and Exercise Tolerance Improvement in Remote Cardiac Rehabilitation: Sub-Analysis of RecRCR Study. Journal of Clinical Medicine, 14(10), 3265. https://doi.org/10.3390/jcm14103265