Network Analysis of Legg–Calve–Perthes Disease and Its Comorbidities



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
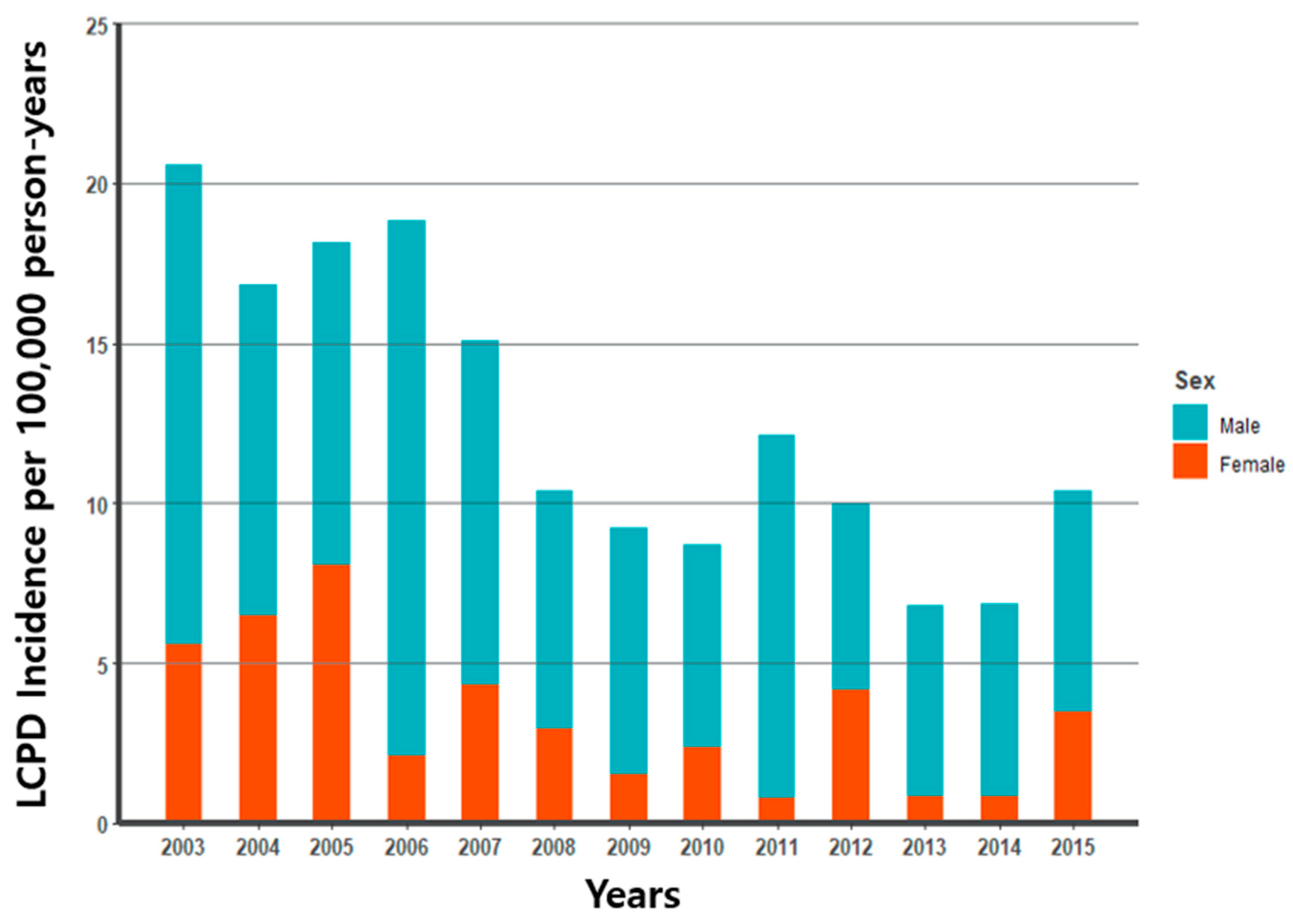
2.2. Incidence
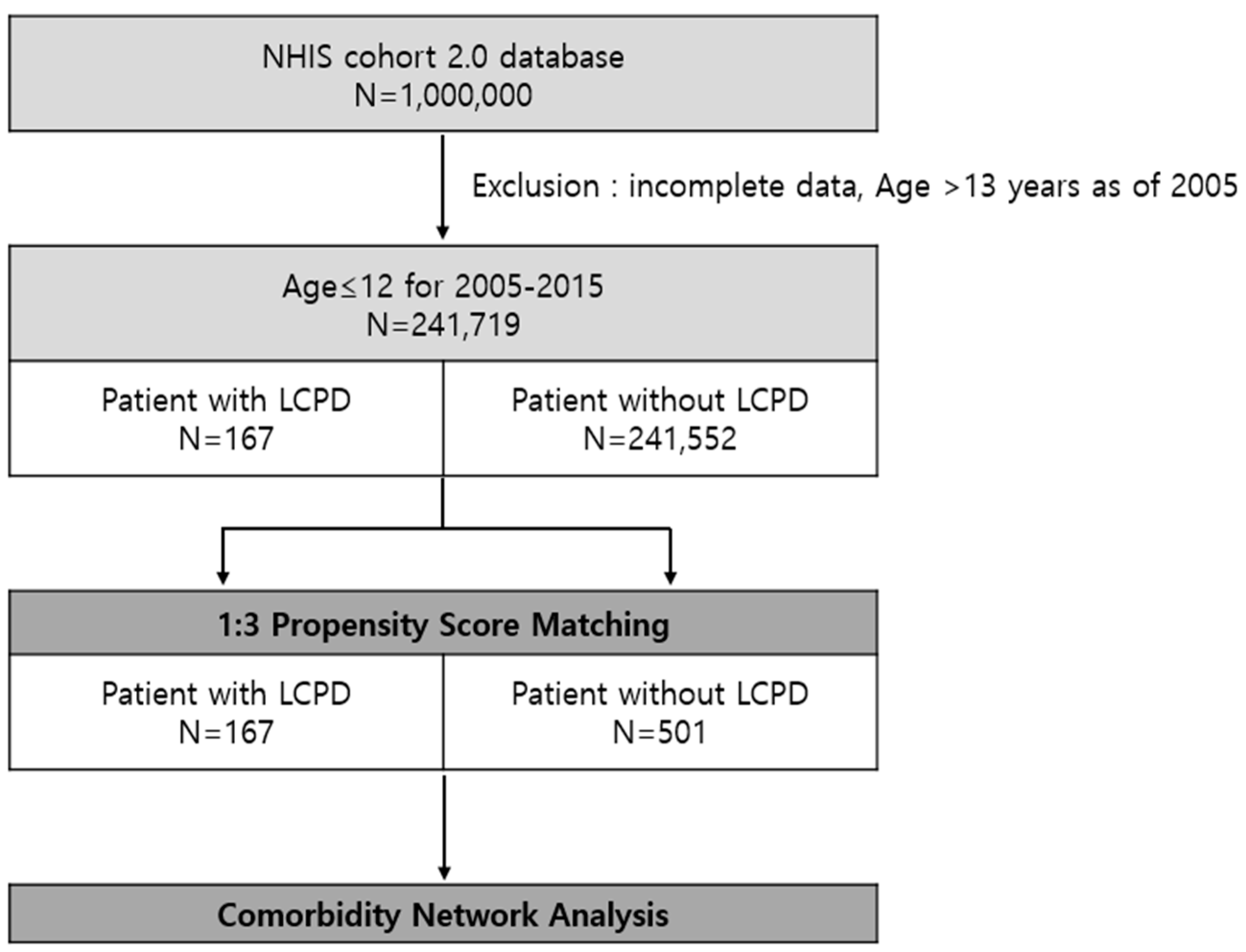
2.3. LCPD Group
2.4. Control Group
2.5. Disease Classification
2.6. Analysis of Association
2.7. Network Map
2.8. Statistical Analysis
3. Results
3.1. Incidence in Korean Population
3.2. Study Population
3.3. Comorbidity Network
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Yoon, S.; Kim, J.; Ahn, W.; Lee, S. Network analysis of osteoporosis provides a global view of associated comorbidities and their temporal relationships. Arch. Osteoporos. 2023, 18, 79. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef]
- Aguado, A.; Moratalla-Navarro, F.; López-Simarro, F.; Moreno, V. MorbiNet: Multimorbidity networks in adult general population. Analysis of type 2 diabetes mellitus comorbidity. Sci. Rep. 2020, 10, 2416. [Google Scholar] [CrossRef]
- Li, X.; Liu, G.; Chen, W.; Bi, Z.; Liang, H. Network analysis of autistic disease comorbidities in Chinese children based on ICD-10 codes. BMC Med. Inform. Decis. Mak. 2020, 20, 268. [Google Scholar] [CrossRef]
- Pavone, V.; Chisari, E.; Vescio, A.; Lizzio, C.; Sessa, G.; Testa, G. Aetiology of Legg–Calvé–Perthes disease: A systematic review. World J. Orthop. 2019, 10, 145–165. [Google Scholar] [CrossRef]
- Loder, R.T.; Skopelja, E.N. The epidemiology and demographics of Legg–Calvé–Perthes’ disease. ISRN Orthop. 2011, 2011, 504393. [Google Scholar] [CrossRef]
- Leroux, J.; Abu Amara, S.A.; Lechevallier, J. Legg-Calvé-Perthes disease. Orthop. Traumatol. Surg. Res. 2018, 104, S107–S112. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.E.; Schoenecker, P.L.; Osland, J.D.; Dobbs, M.B.; Szymanski, D.A.; Luhmann, S.J. Smoking and socioeconomic status in the etiology and severity of Legg-Calvé-Perthes’ disease. J. Pediatr. Orthop. B 2004, 13, 367–370. [Google Scholar] [CrossRef]
- Neal, D.C.; Alford, T.H.; Moualeu, A.; Jo, C.H.; Herring, J.A.; Kim, H.K. Prevalence of Obesity in Patients With Legg-Calvé-Perthes Disease. J. Am. Acad. Orthop. Surg. 2016, 24, 660–665. [Google Scholar] [CrossRef]
- Rodríguez-Olivas, A.O.; Hernández-Zamora, E.; Reyes-Maldonado, E. Legg–Calvé–Perthes disease overview. Orphanet J. Rare Dis. 2022, 17, 125. [Google Scholar] [CrossRef]
- Hresko, M.T.; McDougall, P.A.; Gorlin, J.B.; Vamvakas, E.C.; Kasser, J.R.; Neufeld, E.J. Prospective reevaluation of the association between thrombotic diathesis and Legg-Perthes disease. J. Bone Jt. Surg. Am. 2002, 84, 1613–1618. [Google Scholar] [CrossRef]
- Sirvent, N.; Fisher, F.; Hayek, T.E.; Appert, A.; Giudicelli, H.; Griffet, J. Absence of congenital prethrombotic disorders in children with Legg-Perthes disease. J. Pediatr. Orthop. B 2000, 9, 24–27. [Google Scholar] [CrossRef]
- Vosmaer, A.; Pereira, R.R.; Koenderman, J.S.; Rosendaal, F.R.; Cannegieter, S.C. Coagulation abnormalities in Legg-Calvé-Perthes disease. J. Bone Jt. Surg. Am. 2010, 92, 121–128. [Google Scholar] [CrossRef]
- Perry, D.C.; Bruce, C.E.; Pope, D.; Dangerfield, P.; Platt, M.J.; Hall, A.J. Comorbidities in Perthes’ disease: A case control study using the General Practice Research database. J. Bone Jt. Surg. Br. 2012, 94, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Hailer, Y.D.; Hailer, N.P. Is Legg-Calvé-Perthes disease a local manifestation of a systemic condition? Clin. Orthop. Relat. Res. 2018, 476, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Haldane, J.B.S. The estimation and significance of the logarithm of a ratio of frequencies. Ann. Hum. Genet. 1956, 20, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Anscombe, F.J. On estimating binomial response relations. Biometrika 1656, 43, 461–464. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Edition 2010. 2016. Available online: https://icd.who.int/browse10/Content/statichtml/ICD10Volume2_en_2010.pdf (accessed on 8 March 2021).
- Bastian, M.; Heymann, S. Gephi SM: An Open Source Software for Exploring and Manipulating Networks. In Proceedings of the International AAAI Conference on Weblogs and Social Media, San Jose, CA, USA, 17–20 May 2009; Available online: http://www.aaai.org/ocs/index.php/ICWSM/09/paper/view/154 (accessed on 27 January 2015).
- Rowe, S.M.; Jung, S.T.; Lee, K.B.; Bae, B.H.; Cheon, S.Y.; Kang, K.D. The incidence of Perthes’ disease in Korea: A focus on differences among races. J. Bone Jt. Surg. Br. 2005, 87, 1666–1668. [Google Scholar] [CrossRef]
- Chung, S.M. The arterial supply of the developing proximal end of the human femur. J. Bone Jt. Surg. Am. 1976, 58, 961–970. [Google Scholar] [CrossRef]
- Wynne-Davies, R.; Gormley, J. The aetiology of Perthes’ disease. Genetic, epidemiological and growth factors in 310 Edinburgh and Glasgow patients. J. Bone Jt. Surg. Br. 1978, 60, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Hall, A.J. The epidemiology of Perthes’ disease. Clin. Orthop. Relat. Res. 1986, 209, 89–94. [Google Scholar] [CrossRef]
- Ebong, W.W. Legg-Calvé-Perthes disease in Nigerians. Int. Surg. 1977, 62, 217–218. [Google Scholar]
- Koczewski, P.; Napiontek, M. Perthes’ disease or late avascular necrosis after developmental dislocation of the hip? 10 children followed for 6–35 years. Acta Orthop. Scand. 2001, 72, 331–334. [Google Scholar] [CrossRef]
- Mishima, K.; Fujita, A.; Mizuno, S.; Matsushita, M.; Nagata, T.; Kamiya, Y.; Miyake, N.; Matsumoto, N.; Imagama, S.; Kitoh, H. Legg-Calvé-Perthes disease in a patient with Bardet-Biedl syndrome: A case report of a novel MKKS/BBS6 mutation. Clin. Case Rep. 2020, 8, 3110–3115. [Google Scholar] [CrossRef] [PubMed]
- Mishima, K.; Kamiya, Y.; Matsushita, M.; Imagama, S.; Kitoh, H. Predictive ability of inflammatory markers and laboratory parameters in Legg-Calvé-Perthes disease. Medicine 2022, 101, e29061. [Google Scholar] [CrossRef] [PubMed]
- Spasovski, V.; Srzentić Dražilov, S.S.; Nikčević, G.; Baščarević, Z.; Stojiljković, M.; Pavlović, S.; Spasovski, D. Molecular biomarkers in Perthes disease: A review. Diagnostics 2023, 13, 471. [Google Scholar] [CrossRef] [PubMed]
- Hailer, Y.D.; Montgomery, S.M.; Ekbom, A.; Nilsson, O.S.; Bahmanyar, S. Legg-Calve-Perthes disease and risks for cardiovascular diseases and blood diseases. Pediatrics 2010, 125, e1308–e1315. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | Propensity Score Matched (1:3) | p-Value | |
|---|---|---|---|
| LCPD (N = 167) | Non-LCPD (N = 501) | ||
| Sex | 1 * | ||
| Male | 125 (74.9%) | 375 (74.9%) | |
| Female | 42 (25.1%) | 126 (25.1%) | |
| Age (years) | 7.8 ± 2.7 | 7.8 ± 2.7 | 1 † |
| Period before diagnosis (years) | 5.1 ± 2.3 | 5.1 ± 2.3 | 1 † |
| ICD-10 Code | English Name | LCPD N (%) | Non-LCPD N (%) | p-Value | OR | Degree |
|---|---|---|---|---|---|---|
| D64 | Other anaemias | 8 (4.8) | 7 (1.4) | 0.016 | 3.51 | 3 |
| H16 | Keratitis | 30 (18) | 59 (11.8) | 0.048 | 1.65 | 4 |
| H60 | Otitis externa | 43 (25.7) | 85 (17) | 0.017 | 1.7 | 4 |
| J41 | Simple and mucopurulent chronic bronchitis | 17 (10.2) | 22 (4.4) | 0.012 | 2.48 | 4 |
| J45 | Asthma | 124 (74.3) | 330 (65.9) | 0.045 | 1.49 | 4 |
| L01 | Impetigo | 62 (37.1) | 139 (27.7) | 0.025 | 1.54 | 8 |
| L24 | Irritant contact dermatitis | 40 (24) | 76 (15.2) | 0.013 | 1.77 | 5 |
| M00 | Pyogenic arthritis | 3 (1.8) | 0 (0) | 0.015 | 21.34 | 4 |
| M41 | Scoliosis | 4 (2.4) | 1 (0.2) | 0.015 | 9.18 | 5 |
| M54 | Dorsalgia | 7 (4.2) | 4 (0.8) | 0.007 | 5.17 | 7 |
| M62 | Other disorders of muscle | 7 (4.2) | 4 (0.8) | 0.007 | 5.17 | 6 |
| M65 | Synovitis and tenosynovitis | 15 (9) | 8 (1.6) | <0.001 | 5.9 | 5 |
| M67 | Other disorders of synovium and tendon | 40 (24) | 12 (2.4) | <0.001 | 12.44 | 9 |
| Q65 | Congenital deformities of hip | 4 (2.4) | 0 (0) | 0.004 | 27.61 | 2 |
| Q66 | Congenital deformities of feet | 3 (1.8) | 0 (0) | 0.015 | 21.34 | 1 |
| S30 | Superficial injury of abdomen, lower back and pelvis | 5 (3) | 4 (0.8) | 0.048 | 3.74 | 6 |
| S33 | Dislocation, sprain and strain of joints and ligaments of lumbar spine and pelvis | 15 (9) | 11 (2.2) | <0.001 | 4.34 | 11 |
| S50 | Superficial injury of forearm | 10 (6) | 12 (2.4) | 0.041 | 2.61 | 2 |
| S70 | Superficial injury of hip and thigh | 10 (6) | 7 (1.4) | 0.003 | 4.4 | 8 |
| S73 | Dislocation, sprain and strain of joint and ligaments of hip | 16 (9.6) | 10 (2) | <0.001 | 5.1 | 6 |
| S80 | Superficial injury of lower leg | 16 (9.6) | 19 (3.8) | 0.008 | 2.7 | 10 |
| S83 | Dislocation, sprain and strain of joints and ligaments of knee | 16 (9.6) | 15 (3) | 0.001 | 3.42 | 10 |
| T00 | Superficial injuries involving multiple body regions | 8 (4.8) | 7 (1.4) | 0.016 | 3.51 | 1 |
| ICD-10 Code | English Name | LCPD N (%) | Non-LCPD N (%) | p-Value | OR | Degree |
|---|---|---|---|---|---|---|
| D64 | Other anaemias | 8 (4.8) | 7 (1.4) | 0.016 | 3.51 | 1 |
| H16 | Keratitis | 60 (35.9%) | 130 (25.9%) | 0.017 | 1.6 | 5 |
| H60 | Otitis externa | |||||
| J41 | Simple and mucopurulent chronic bronchitis | 129 (77.2%) | 336(67.1%) | 0.017 | 1.65 | 5 |
| J45 | Asthma | |||||
| L01 | Impetigo | 79 (47.3%) | 185 (36.9%) | 0.022 | 1.53 | 5 |
| L24 | Irritant contact dermatitis | |||||
| M00 | Pyogenic arthritis | 3 (1.8) | 0 (0) | 0.015 | 21.34 | 3 |
| M41 | Scoliosis | 11 (6.6%) | 5 (1.0%) | <0.001 | 6.63 | 4 |
| M54 | Dorsalgia | |||||
| M62 | Other disorders of muscle | 54 (32.3%) | 22 (4.4%) | <0.001 | 10.23 | 7 |
| M65 | Synovitis and tenosynovitis | |||||
| M67 | Other disorders of synovium and tendon | |||||
| Q65 | Congenital deformities of hip | 4 (2.4) | 0 (0) | 0.004 | 27.61 | 3 |
| Q66 | Congenital deformities of feet | 3 (1.8) | 0 (0) | 0.015 | 21.34 | 1 |
| S30 | Superficial injury of abdomen, lower back and pelvis | 32 (19.2%) | 25 (5.0%) | <0.001 | 4.48 | 6 |
| S33 | Dislocation, sprain and strain of joints and ligaments of lumbar spine and pelvis | |||||
| S70 | Superficial injury of hip and thigh | |||||
| S73 | Dislocation, sprain and strain of joint and ligaments of hip | |||||
| S50 | Superficial injury of forearm | 42 (25.1%) | 48 (9.6%) | <0.001 | 3.17 | 7 |
| S80 | Superficial injury of lower leg | |||||
| S83 | Dislocation, sprain and strain of joints and ligaments of knee | |||||
| T00 | Superficial injuries involving multiple body regions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Ko, K.R.; Yoon, S.; Chung, J.; Lee, S. Network Analysis of Legg–Calve–Perthes Disease and Its Comorbidities. J. Clin. Med. 2025, 14, 259. https://doi.org/10.3390/jcm14010259
Kim K, Ko KR, Yoon S, Chung J, Lee S. Network Analysis of Legg–Calve–Perthes Disease and Its Comorbidities. Journal of Clinical Medicine. 2025; 14(1):259. https://doi.org/10.3390/jcm14010259
Chicago/Turabian StyleKim, KyeongMi, Kyung Rae Ko, Siyoung Yoon, Jaiwoo Chung, and Soonchul Lee. 2025. "Network Analysis of Legg–Calve–Perthes Disease and Its Comorbidities" Journal of Clinical Medicine 14, no. 1: 259. https://doi.org/10.3390/jcm14010259
APA StyleKim, K., Ko, K. R., Yoon, S., Chung, J., & Lee, S. (2025). Network Analysis of Legg–Calve–Perthes Disease and Its Comorbidities. Journal of Clinical Medicine, 14(1), 259. https://doi.org/10.3390/jcm14010259