
Patient-Reported Outcomes After Arthroscopic Single-Row Rotator Cuff Repair: A Monocentric Retrospective Study at Minimum 12 Years Follow-Up

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Clinical Outcomes
2.2. Population
2.3. Statistical Analysis
3. Results
3.1. Overall Results
3.2. Results and Risk Factors (Table 2)
3.2.1. Sex
3.2.2. Age at Surgery
3.2.3. Tendon Repair Pattern
3.2.4. Length of Follow-Up

{kind=link}
| Parameters | QuickDASH | ASES | SST | Satisfaction | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| M | 4.81 ± 12.1 | p < 0.001 | 87.2 ± 21.6 | p < 0.001 | 92.9 ± 18.3 | p = 0.004 | 322 (97.0%) | p = 0.623 |
| F | 9.9 ± 18.5 | 79.9 ± 25.7 | 86.4 ± 25.8 | 284 (96.0%) | ||||
| Age | ||||||||
| <50 years old | 6.9 ± 18.0 | 0.302 | 85.3 ± 24.0 | 0.389 | 91.3 ± 22.4 | 0.287 | 119 (95.2%) | 0.351 |
| 51–59 | 8.3 ± 16.5 | 82.1 ± 25.3 | 88.5 ± 24.4 | 229 (97.9%) | ||||
| 60–69 | 6.1 ± 13.7 | 83.9 ± 23.3 | 91.3 ± 20.0 | 207 (96.3%) | ||||
| ≥70 | 7.3 ± 13.7 | 86.8 ± 19.2 | 86.9 ± 21.8 | 51 (94.4%) | ||||
| N^ Tendons Repaired | ||||||||
| Single tendon | 6.5 ± 14.4 | 0.531 | 84.2 ± 23.6 | 0.309 | 91.2 ± 20.7 | 0.14 | 414 (95.6%) | 0.199 |
| 2 tendons | 9.1 ± 19.3 | 82.1 ± 25.7 | 86.3 ± 26.7 | 132 (98.5%) | ||||
| >2 tendons | 7.9 ± 15.0 | 84.4 ± 22.0 | 88.3 ± 22.5 | 60 (98.4%) | ||||
| Anterior Tear | ||||||||
| Yes | 8.3 ± 17.4 | 0.242 | 83.1 ± 24.3 | 0.352 | 88.9 ± 22.6 | 0.515 | 146 (98.0%) | 0.317 |
| No | 6.9 ± 15.1 | 84.0 ± 23.8 | 90.2 ± 22.3 | 460 (96.0%) | ||||
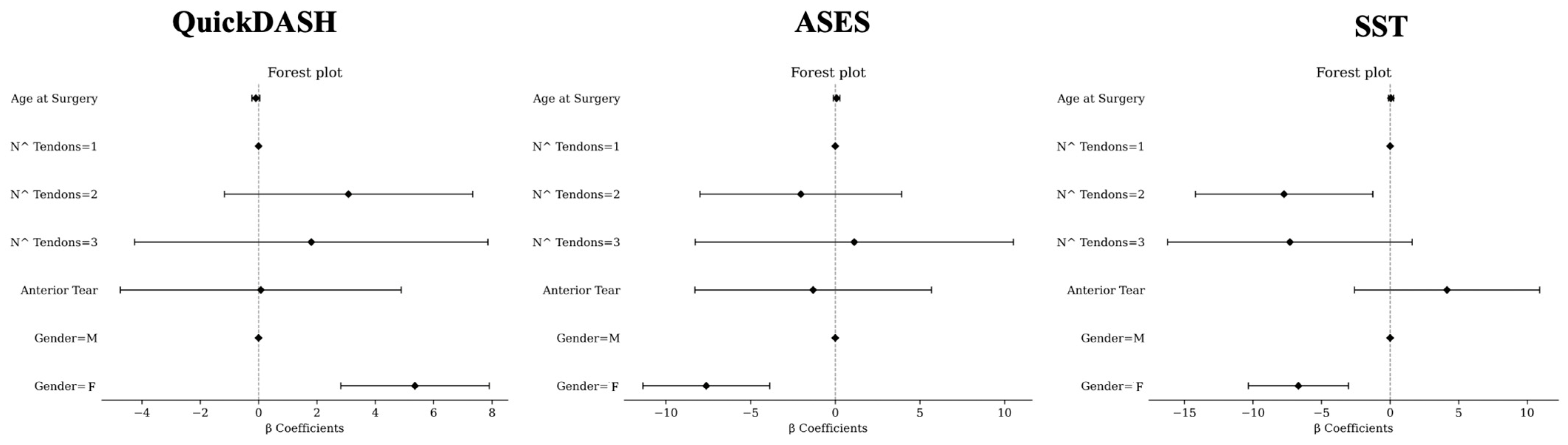
3.2.5. Results According to Multivariate Analysis (Figure 1)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tashjian, R.Z. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin. Sports Med. 2012, 31, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Mighell, M. Massive Irreparable Rotator Cuff Tears; Thieme Medical: New York, NY, USA, 2008. [Google Scholar]
- Longo, U.G.; Salvatore, G.; Rizzello, G.; Berton, A.; Ciuffreda, M.; Candela, V.; Denaro, V. The burden of rotator cuff surgery in Italy: A nationwide registry study. Arch. Orthop. Trauma Surg. 2017, 137, 217–224. [Google Scholar] [CrossRef]
- Black, E.M.; Higgins, L.D.; Warner, J.J.P. Value-based shoulder surgery: Practicingoutcomes-driven, cost-conscious care. J. Shoulder Elb. Surg. 2013, 22, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Makhni, E.C.; Baumhauer, J.F.; Ayers, D.; Bozic, K.J. Patient-Reported Outcome Measures: How and Why They Are Collected. Instr. Course Lect. 2019, 68, 675–680. [Google Scholar] [PubMed]
- MacDermid, J.C.; Khadilkar, L.; Birmingham, T.B.; Athwal, G.S. Validity of the QuickDASH in patients with shoulder-related disorders undergoing surgery. J. Orthop. Sports Phys. Ther. 2015, 45, 25–36. [Google Scholar] [CrossRef]
- DASH. Welcome to Our Website Where You Will Find Up-to-Date Information About the DASH Outcome Measure, the QuickDASH and Related DASH. Available online: https://www.dash.iwh.on.ca/ (accessed on 12 May 2022).
- Tashjian, R.Z.; Deloach, J.; Green, A.; Porucznik, C.A.; Powell, A.P. Minimal clinically important differences in ASES and simple shoulder test scores after nonoperative treatment of rotator cuff disease. J. Bone Jt. Surg. 2010, 92, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; McClure, P.W.; Sennett, B.J. American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, patient self-report section: Reliability, validity, and responsiveness. J. Shoulder Elb. Surg. 2002, 11, 587–594. [Google Scholar] [CrossRef]
- Zeng, G.J.; Hao, Y.; Lie, D.T.T. Gender-based differences in mid-term clinical outcomes and patient acceptable symptomatic state attainment after arthroscopic rotator cuff repair: Minimum 2-year follow up. J. ISAKOS 2024, 9, 100283. [Google Scholar] [CrossRef]
- Jones, I.A.; Togashi, R.; Heckmann, N.; Vangsness, C.T., Jr. Minimal clinically important difference (MCID) for patient-reported shoulder outcomes. J. Shoulder Elb. Surg. 2020, 29, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Dabija, D.I.; Jain, N.B. Minimal Clinically Important Difference of Shoulder Outcome Measures and Diagnoses: A Systematic Review. Am. J. Phys. Med. Rehabil. 2019, 98, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Fossati, C.; Stoppani, C.; Menon, A.; Pierannunzii, L.; Compagnoni, R.; Randelli, P.S. Arthroscopic rotator cuff repair in patients over 70 years of age: A systematic review. J. Orthop. Traumatol. 2021, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Carnevale, A.; Piergentili, I.; Berton, A.; Candela, V.; Schena, E.; Denaro, V. Retear rates after rotator cuff surgery: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2021, 22, 749. [Google Scholar] [CrossRef] [PubMed]
- Genuario, J.W.; Donegan, R.P.; Hamman, D.; Bell, J.E.; Boublik, M.; Schlegel, T.; Tosteson, A.N. The cost-effectiveness of single-row compared with double-row arthroscopic rotator cuff repair. J. Bone Jt. Surg. Am. 2012, 94, 1369–1377. [Google Scholar] [CrossRef]
- Gustavson, K.; Røysamb, E.; Borren, I. Preventing bias from selective non-response in population-based survey studies: Findings from a Monte Carlo simulation study. BMC Med. Res. Methodol. 2019, 19, 120. [Google Scholar] [CrossRef]
| Parameters | n |
|---|---|
| Total Number of Patients | 628 |
Age: mean ± SD (range) [years]
| 57.6 ± 9.6 (16.1 to 78.4) |
| 125 | |
| 234 | |
| 215 | |
| 54 | |
| Sex: Males (%) | 332 (53%) |
| Lesion pattern * N^ tendons
| 433 (69%) 419 12 2 134 (21%) 61 (10%) |
| Presence of anterior tear (Subscapularis involvement) | 149 (24%) |
| Follow-up: mean ± SD (range) [years] | 12.9 ± 1.3 (12–15) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castagna, A.; Campeggi, T.; Minelli, M.M.; Borroni, M.; Conti, M.; Delle Rose, G.; Garofalo, R.; Ranieri, R. Patient-Reported Outcomes After Arthroscopic Single-Row Rotator Cuff Repair: A Monocentric Retrospective Study at Minimum 12 Years Follow-Up. J. Clin. Med. 2025, 14, 235. https://doi.org/10.3390/jcm14010235
Castagna A, Campeggi T, Minelli MM, Borroni M, Conti M, Delle Rose G, Garofalo R, Ranieri R. Patient-Reported Outcomes After Arthroscopic Single-Row Rotator Cuff Repair: A Monocentric Retrospective Study at Minimum 12 Years Follow-Up. Journal of Clinical Medicine. 2025; 14(1):235. https://doi.org/10.3390/jcm14010235
Chicago/Turabian StyleCastagna, Alessandro, Tommaso Campeggi, Marco Maria Minelli, Mario Borroni, Marco Conti, Giacomo Delle Rose, Raffaele Garofalo, and Riccardo Ranieri. 2025. "Patient-Reported Outcomes After Arthroscopic Single-Row Rotator Cuff Repair: A Monocentric Retrospective Study at Minimum 12 Years Follow-Up" Journal of Clinical Medicine 14, no. 1: 235. https://doi.org/10.3390/jcm14010235
APA StyleCastagna, A., Campeggi, T., Minelli, M. M., Borroni, M., Conti, M., Delle Rose, G., Garofalo, R., & Ranieri, R. (2025). Patient-Reported Outcomes After Arthroscopic Single-Row Rotator Cuff Repair: A Monocentric Retrospective Study at Minimum 12 Years Follow-Up. Journal of Clinical Medicine, 14(1), 235. https://doi.org/10.3390/jcm14010235