1. Introduction
Both inflammatory bowel disease (IBD) and type 2 diabetes mellitus (T2DM) are chronic, multifactorial diseases influenced by environmental factors acting on genetic predisposition.
A diet rich in fats, particularly animal fats, and polyunsaturated fatty acids has been associated with an increased incidence of Crohn’s disease (CD) and ulcerative colitis (UC), as well as type 2 diabetes mellitus (T2DM), due to its influence of increasing the systemic inflammatory status [
1]. Certain dietary components can indeed affect the structure and function of the microbiota, with downstream effects on immune activity [
2]. A factor implicated in both diseases is intestinal dysbiosis; both diseases share an increase in the presence of microbial species with pathogenic potential, such as
Ruminococcus gnavus, which utilizes mucin and dietary glycans and produces bacteriocins and adhesins. These compounds elicit a pro-inflammatory host response and modulate host metabolism of bile acids and tryptophan metabolic pathways [
3,
4]. Conversely, there is a decrease in
Akkermansia muciniphila, a bacterium that plays a beneficial role in maintaining intestinal mucosal integrity and reducing the production of pro-inflammatory substances [
5].
The growing interest in the management of comorbidities, within an increasingly elderly population, has prompted several research groups to investigate the relationship between these diseases.
In a cohort study conducted in Denmark on 6,028,844 people, a higher number of diabetic subjects was observed in the cohort of IBD patients compared to the general population, resulting in a 50% higher risk of IBD patients developing T2DM [
6]. In another cohort study conducted in South Korea, an increased relative risk (RR) of 1.09 was observed in IBD patients for developing T2DM: 1.41 in CD patients and 1.04 in UC patients [
7]. Additionally, in a cohort study conducted in China, involving 454,804 individuals, CD patients showed an increased risk of T2DM compared to the general population, as well as UC patients [
8].
Corticosteroid therapy is one of the main assumptions underlying the link between IBD and T2DM, as steroids are currently a first-line therapy to induce remission in IBD exacerbations [
9,
10]. The effect of systemic corticosteroids (but also, partially, topical corticosteroids) of raising blood glucose has been widely demonstrated [
11].
In mouse models, hyperglycemia has been observed to worsen the clinical outcomes of IBD activity, presumably acting on the integrity of the colonic epithelial barrier [
12]. However, the role of T2DM in the course of IBD in clinical trials is controversial. For example, in Uwagbale et al.’s study, patients with IBD and T2DM were found to have a lower risk of IBD-related complications and a lower risk of undergoing IBD-related surgery, compared to patients with isolated IBD; on the other hand, an increase in septic complications was highlighted [
13]. An increase in septic complications was also described by Kumar et al., together with an increase in hospitalizations, IBD-related complications, and disease flare-ups, despite a non-significant difference in the incidence of IBD-related surgeries [
14]. Fuschillo et al. conducted a meta-analysis, where it emerged that T2DM in patients with IBD did not worsen the course of the disease in terms of IBD-related complications, IBD-related surgery, and mortality, despite representing an independent risk factor for IBD-related hospitalizations and sepsis [
15].
The characterization of the new category of patients with IBD and T2DM has not been well detailed yet: studies on the effects of diabetes on inflammatory disease have yielded conflicting results. Among the possible explanations, the heterogeneity of IBD clinical presentations stands out, along with the variability in the criteria for endpoint attribution and the description of results [
15]. Therefore, to assess how T2DM might influence the course of intestinal disease, we selected the definition of severe IBD as the primary objective of our study, independent of the increased comorbidity risk associated with T2DM.
Furthermore, both IBD and T2DM patients are at an elevated risk for liver disease compared to the general population [
16,
17,
18], yet the extent of these complications in patients with both conditions has been poorly investigated. Consequently, as a secondary endpoint, we examined the prevalence of steatotic liver disease (SLD) and liver damage in patients with IBD and T2DM.
2. Materials and Methods
We conducted a retrospective case–control study to compare patients with both IBD and T2DM to patients who had IBD without T2DM. We reviewed the medical records of patients followed at the IBD Clinical Center of the ‘San Giovanni Antica Sede’ Hospital, AOU Città della Salute e della Scienza in Turin, Italy.
2.1. Inclusion and Exclusion Criteria
Inclusion in cases:
- -
Minimum follow-up period of 1 year;
- -
Confirmed diagnosis of IBD according to the 2019 ECCO-ESGAR guidelines [
19];
- -
History of T2DM at the time of their last visit.
Exclusion in cases:
- -
Inability to determine severe disease according to a composite outcome that considers IBD manifestations and complications described by Yarur et al. (see
Section 2.3) [
20].
Inclusion in controls:
- -
Minimum follow-up period of 1 year;
- -
Confirmed diagnosis of IBD according to the 2019 ECCO-ESGAR guidelines [
19].
Exclusion in controls:
- -
Inability to determine severe disease according to a composite outcome that considers IBD manifestations and complications described by Yarur et al. (see
Section 2.3) [
20];
- -
Medical history of T2DM or iatrogenic diabetes;
- -
Past/current therapy with hypoglycemic drugs.
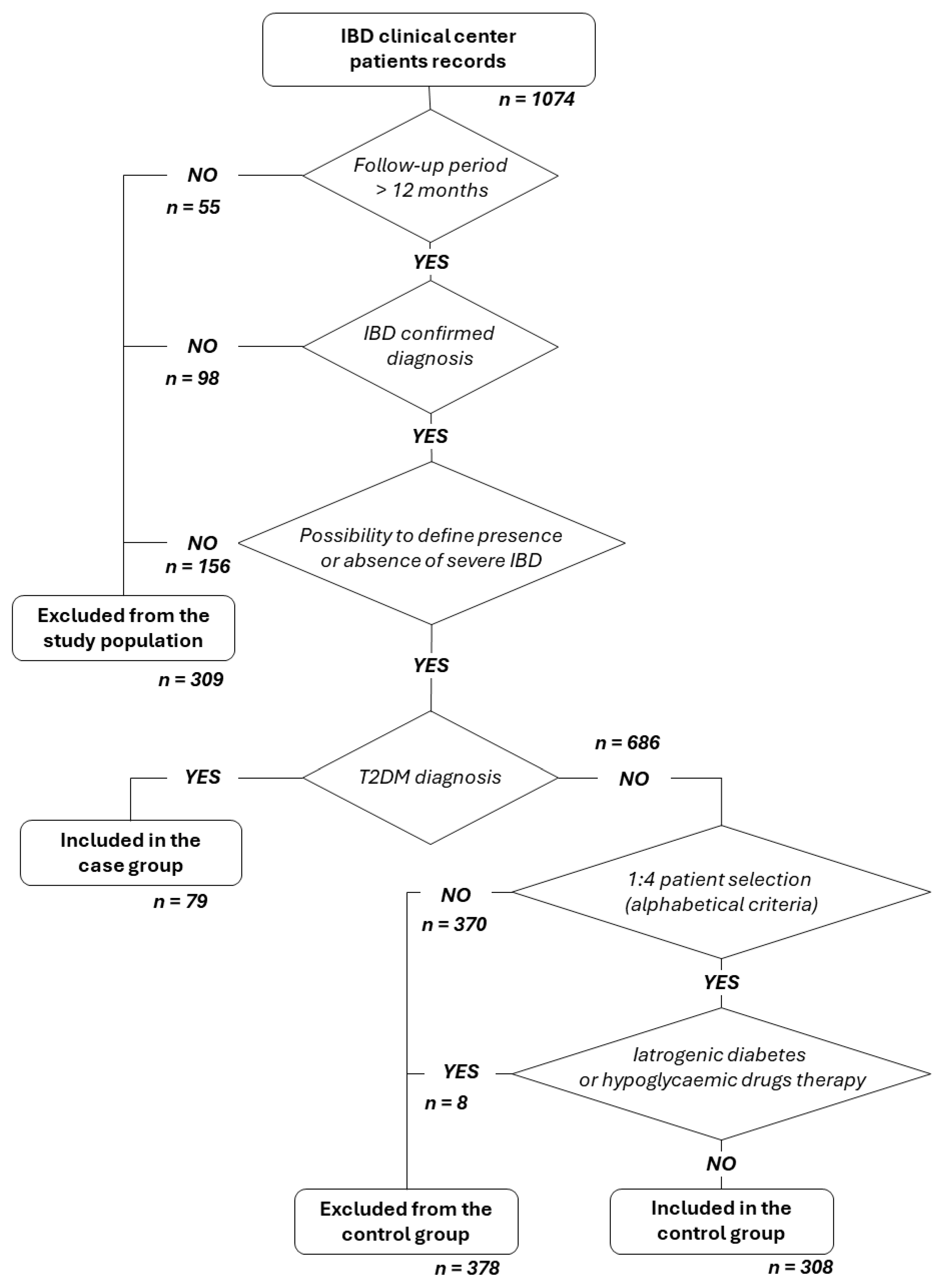
Figure 1 presents the patient qualification flow chart.
The control group was randomly selected from selected IBD patients (in alphabetical order) at an approximate ratio of 1:4 between cases and controls.
2.2. Type and Source of Data
In
Table 1 type and source of data are listed.
2.3. Endpoint Definition
The primary endpoint of this study was to determine the prevalence of severe IBD in IBD-T2DM patients compared to a control group of IBD patients without T2DM. For this purpose, we used a composite outcome that considers IBD manifestations and complications described by Yarur et al. in a systematic review aimed at establishing predictors of aggressive IBD [
20]. Thus, patients were considered to have severe IBD if at least one of the following conditions occurred during the entire follow-up period:
Need for IBD-related surgery; need for immunosuppressive drugs/biologics/small molecules as maintenance therapy; more than two courses of systemic corticosteroids during the entire duration of follow-up; need for hospitalization for flare-ups or complications after initial diagnosis; at least one of the following: presence of persistent diarrhea for more than 12 months with nocturnal awakenings or urgency, intestinal stricture with symptoms.
Moreover, we chose the presence of liver damage and the presence of hepatic steatosis as secondary endpoints.
We defined liver damage through the use of the FIB4 score, calculated as age in years × AST in U/L/platelets in ×10⁹/L × √ALT in U/L [
21]; in this study, a result higher than 1.3 determined the presence of liver damage. This endpoint was evaluated only in patients whose records reported AST, ALT, and platelet count values at least once. Where multiple measurements were reported, the most recent ones were taken into consideration.
We took into consideration the presence of SLD if steatosis was described in medical history, and if examinations by abdominal ultrasound or FibroScan® were suggestive of it. Patients who had never undergone ultrasound/Fibroscan were not evaluated. The absence of steatosis was defined for those patients who underwent at least one of the previous imaging investigations and in whom hepatic steatosis was not described in their medical history, the liver was normal, or the CAP values were normal.
2.4. Statistical Analysis
Continuous variables were reported as mean (standard deviation (SD)) or median (interquartile range (IQR)) based on the distribution of values. Normality was verified using the D’Agostino–Pearson test. Categorical variables were reported as numbers and percentages.
Comparison between independent categorical variables was performed using the Chi-square test. Comparison between continuous variables was performed using the independent samples t-test or the Mann–Whitney test based on the distribution of values.
The association between variables was tested using the proportional hazard model or Cox regression; therefore, the strength of the association was reported as a hazard ratio (HR) with a 95% confidence interval (95% CI).
All statistical analyses were performed using MedCalc® v. 20.104 (MedCalc Software Ltd., Ostend, Belgium), and a p value ≤ 0.05 was considered statistically significant.
4. Discussion
Median age at IBD diagnosis was significantly higher in cases (48.0), while in controls (32.0;
p < 0.0001), the median age fell within the range reported in epidemiology for this pathology (25–35 years) [
22]. This result has not been described in the literature to date.
In the sub-analysis in patients with CD, there was a notable difference in the disease location of activity between cases and controls: 24.3% of the CD-DMT2 group had a disease localized exclusively at the colonic level (L2), compared to 5% in the group without T2DM (
p = 0.003). Furthermore, no upper-intestinal localization (L4) was found in any case, whereas it was present in 10 patients in the control group (6.2%). This distribution does not reflect the percentages described in the literature [
22,
23], and could suggest another distinct characteristic of this special subpopulation.
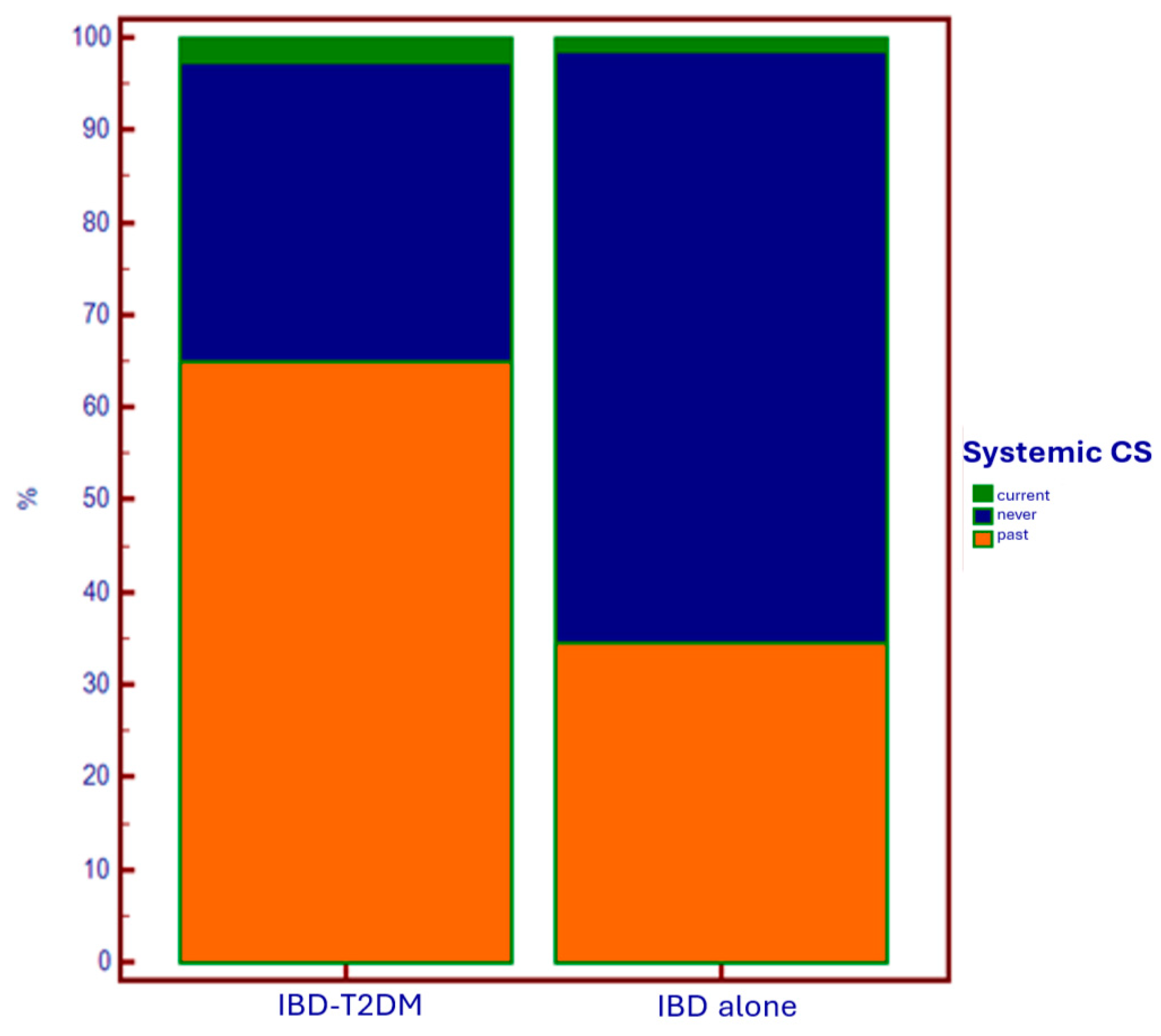
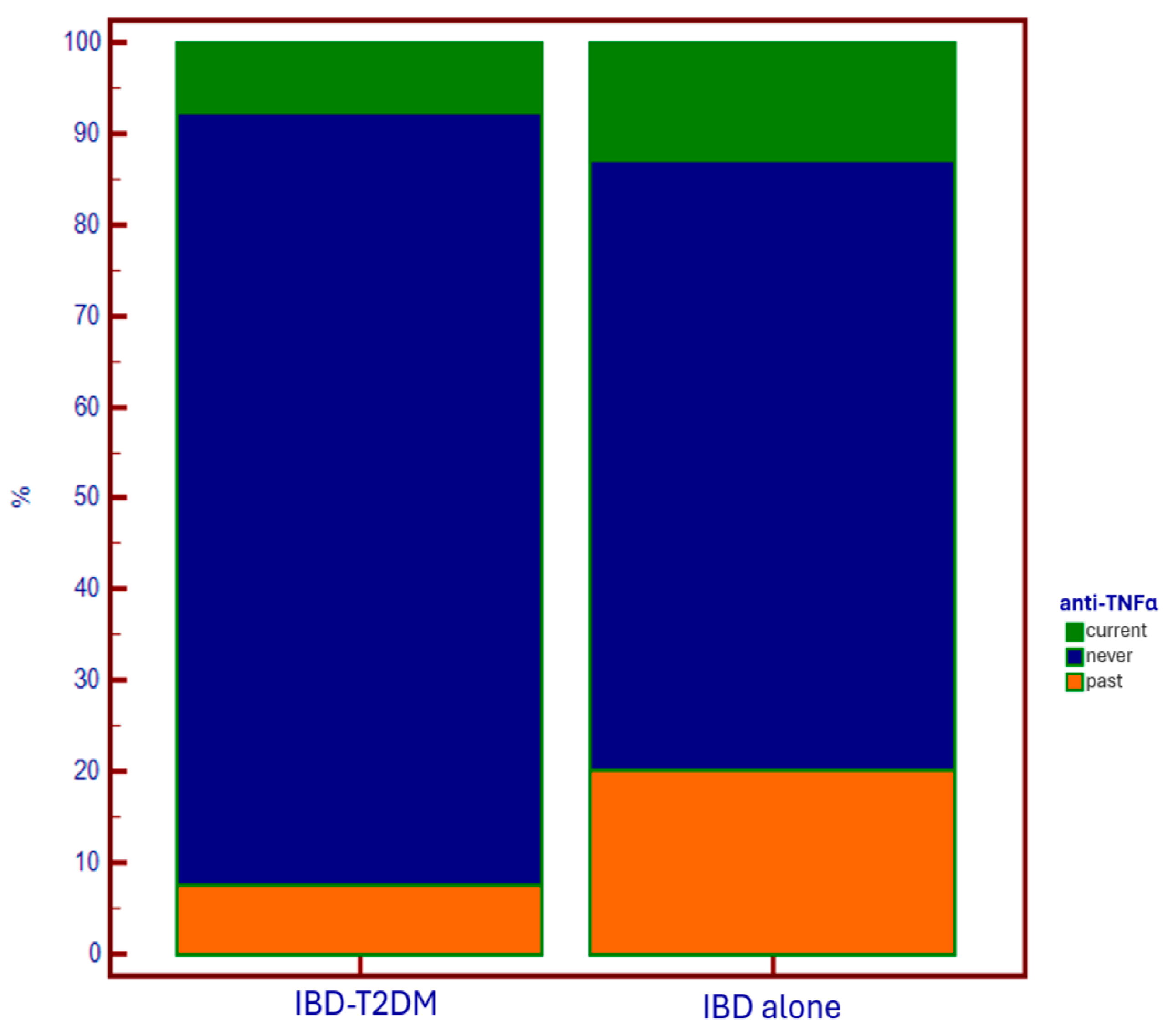
Regarding specific therapy for IBD, in diabetic patients, we observed a wider (current and especially past) administration of systemic corticosteroids, and a lower administration of anti-TNF-alpha drugs. The first data could support an iatrogenic explanation of the epidemiological relationship between IBD and T2DM. On the other hand, in patients using anti-TNF-alpha as maintenance therapy for disease control, there is a lower need for steroids. This results in a reduced need to undergo steroid courses due to disease flare-ups, which has a favorable impact on reducing the risk of developing diabetes associated with steroid administration.
The reason why anti-TNF-alpha agents are underutilized in patients with diabetes is likely due to the increased fragility of these patients, both because of the immune system deficiency that makes them more susceptible to infections (to which anti-TNF-alpha agents could further expose them), and due to the older age of this population, which is associated with the presence of multiple comorbidities, including those in which anti-TNF-alpha agents are contraindicated (e.g., heart failure). In this context, the use of anti-integrin and anti-IL12/23 agents would certainly be appropriate options, thanks to the lower immunosuppressive effect and the better safety profile [
24,
25]. Conversely, the use of anti-JAK molecules would not be a good choice for these patients, considering the EMA alert on their administration in populations with increased metabolic/thrombotic risk, and suggesting that they be considered only in the absence of other alternatives [
26]. Anyway, it is clear how in IBD-T2DM patients, it is fundamental to identify the best therapeutic strategy that allows for a reduction in steroid administration, through optimal disease control. In fact, the usage of steroids in patients who already have a diagnosis of diabetes is implicated in the occurrence of diabetes decompensation and, consequently, the development of multiple complications [
27].
Among patients with IBD and T2DM, 67.1% were hypertensive, while 59.7% were dyslipidemic (vs. 18.6% and 21.2% in controls). However, these percentages were comparable to those found in diabetics without intestinal comorbidity [
28].
Regarding the presence of severe IBD, as the primary endpoint, no significant difference emerged from the comparison between the IBD + T2DM group and the controls, with a prevalence of 59.5 and 59.7%, respectively. These data partly differ from the literature, where an increase in IBD-related hospitalizations (included in the composite endpoint) in IBD-T2DM patients is reported [
14,
15], despite very discordant data among studies [
13,
15]. Then, our study confirmed a lack of increased need for IBD surgery in IBD-T2DM patients [
13,
14,
15].
In our cohort, 69.3% of patients with severe IBD were diagnosed with CD, whereas only 41.7% of patients who did not have severe IBD were diagnosed with CD (p < 0.0001). However, in the univariate analysis, which accounts for the different follow-up lengths for each patient, the presence of CD was not associated with an increased risk of a severe IBD course (HR 1.25; 95% CI 0.94–1.65).
In our study, being naïve to SGLT2 inhibitors, although significant in the χ
2 test (27.7% vs. 12.5%;
p = 0.0383), was not protective against severe disease in the univariate analysis. Instead, being naïve to GLP-1 ra was significantly protective for severe IBD in the univariate analysis, but this significance was not confirmed in the multivariate analysis. Currently, in the literature, there are no clinical studies on the prescription of SGLT2i in the specific population of IBD-DMT2. As regards GLP-1 ra, one study assumed that these drugs could improve the course of IBD [
29], but a similar result was not observed in our study.
The only significant predictor for severe disease in uni- and multivariable analysis was the age at last follow-up: increasing age decreases the risk of severe IBD (HR: 0.98; 95% CI: 0.97 to 0.99;
p < 0.0001). This finding may be explained by the fact that IBD in elderly patients has a more indolent presentation [
30], with symptoms and complications that do not fit our definition of serious disease.
Regarding secondary endpoints, the comparison between the IBD-T2DM group and controls revealed a more than doubled prevalence of hepatic steatosis in cases (62.9% vs. 27.2%;
p < 0.0001). However, the prevalence of steatosis in IBD-T2DM patients did not differ from the prevalence reported in the general diabetic population [
31]; thus, we presume that the association of the two pathologies does not provide a multiplicative risk factor for steatosis.
The assessment of liver damage, using the Fib-4 score, differs significantly between cases and controls (55.4% vs. 26.6%;
p < 0.0001). However, it is likely that the difference in average age (higher in diabetic patients of 19.2y) has negatively influenced score parameters (ALT, AST, and no. of platelets) [
32,
33]. Evaluating the predictors of Fib-4 score > 1.3, DMT2 increased the risk for liver damage (HR: 1.57) with a trend toward statistical significance in the univariate analysis (95% CI 0.99 to 2.51;
p = 0.06).
In the sub-analysis evaluating the characteristics of the population regarding the presence of liver damage, the association of hypertension (HR: 1.61;
p = 0.047) and dyslipidemia (HR: 1.68;
p = 0.03) was statistically significant in the univariate analysis. This aligns with the numerous studies describing metabolic syndrome and its effects on the liver [
16,
31,
34]. Moreover, in the univariate analysis, we observed that being naïve to thiopurine constituted another risk factor for liver damage (HR: 1.81;
p = 0.02), even though the contribution of the covariates hypertension, dyslipidemia, and being naïve to thiopurines was not significant in the multivariate analysis. The contribution of being naïve to anti-TNF-alpha drugs was not significant.
In the multivariable analysis on predictors of liver damage, age was the only covariate resulting in a significant increase in risk (HR 1.03; 95% CI 1.01–1.05;
p = 0.01). This result, although relevant from a statistical point of view, raises doubts about the clinical usefulness of a non-specific predictor such as Fib-4 in the older population due to the presence of age in the numerator of the score, as already highlighted by van Kleef et al. [
33].
No association between liver damage and alcohol consumption was observed, although alcohol is one of the most important causes of liver fibrosis and an increase in hepatic cytolysis indices. However, it is possible that this result was conditioned by the data collection method, since the definition of alcohol consumption included the occasional drink, so it was not possible to define the alcohol units consumed.


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}