
Self-Perceived Stress in Association with Emotional Experiences Following Patient Death and Coping Adequacy among Clinical Nurses in Lithuania: A Cross-Sectional Study

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, and Data Collection
2.2. Measures
2.2.1. Perceived Stress Scale (PSS-10)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Instrument | Content | Scaling |
|---|---|---|
| Demographic and occupational questionnaire (7 items). Questions concerning the emotions and feelings in nurses triggered by the death of a patient (12 items) [24]. | Age, work experience, educational attainment, marital status, workplace, nursing shifts, and experiences with patient loss. Issues about the feelings and emotions after dealing with the death of a patient: guilt, compassion, indifference, disappointment, sadness, depressive mood, despair, calmness, anger, helplessness, grief, and anxiety. | Ratio scales. Ordinal scale: 1 = ‘never’ to 4 = ‘several times a month’. Nominal scale: 0 = ‘No’ to 1 = ‘Yes’. |
| Perceived Stress Scale (PSS-10) (10 items) [4,5,48]. | PSS-10 helps to assess how overloaded, unpredictable, and uncontrolled persons perceive their lives. PSS-10 questions relate to feelings and thoughts that a person has experienced in the last month. | Five-point Likert scale: 0 = ‘never’ to 4 = ‘very often’; high score = stressful situation was experienced more often. The cut-off scores of 13 and 26 are used to arrange the total PSS-10 score into the low, moderate, and high levels of the perceived chronic stress [47]. |
| Coping orientation to problems experienced inventory (Brief-COPE) (28 items) [34]. | The Brief-COPE was constructed to measure the effective and ineffective ways to cope with a stressful life event. This scale is often used in healthcare settings to assess the patients’ emotional response to difficult circumstances. In general, Brief-COPE consists of 3 dimensions with 14 sub-dimensions and assesses 3 styles of coping: (1) problem-focused coping, (2) emotion-focused coping, and (3) avoidant coping [49]. | Four-point Likert scale: 1 = ‘I haven’t been doing this at all’ to 4 = ‘I’ve been doing this a lot’. Scores are presented for three overarching coping styles as average scores, delineating the degree to which the person was engaged in a coping style. There is no cut-off score for the Brief-COPE scale and its subscales. |
2.2.2. Coping Strategies Inventory (Brief-COPE)
2.3. The Statistical Data Analysis
3. Results
3.1. The Descriptive and Frequency Analyses
3.2. Chronic Stress and Emotional States in Relation to Patient Death
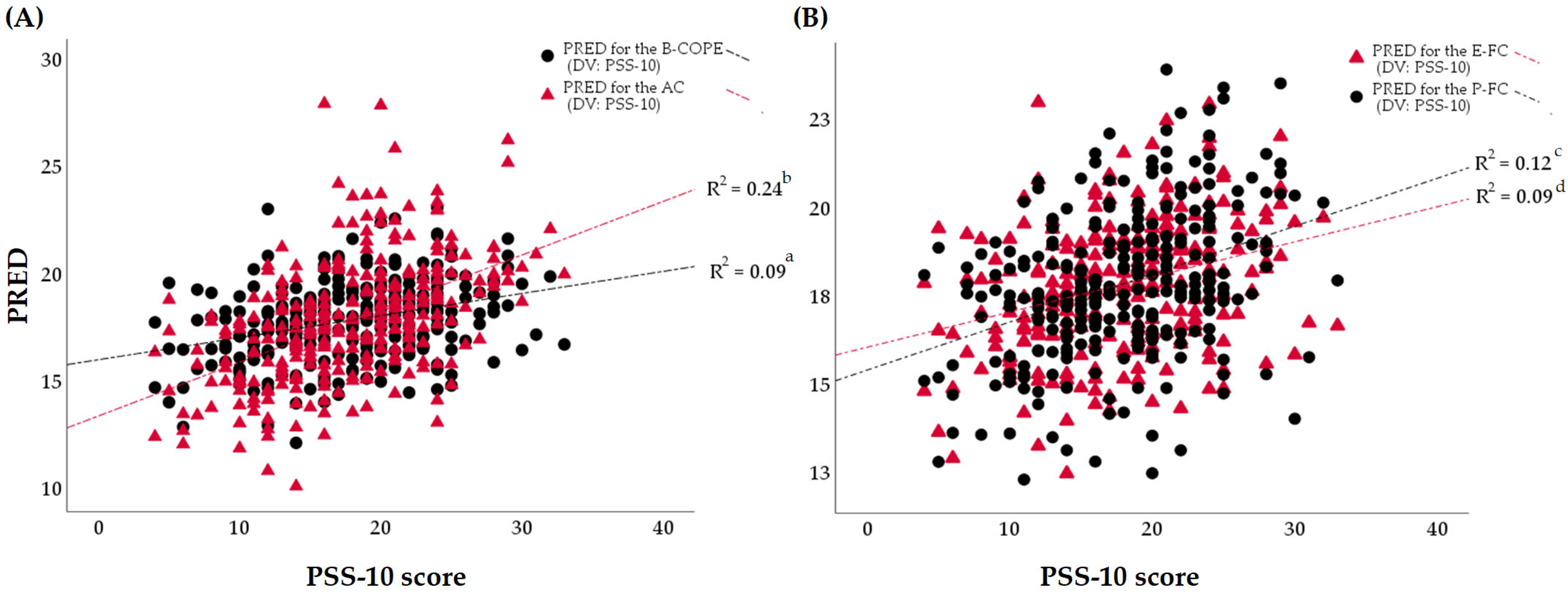
3.3. Chronic Stress and Coping Styles
4. Discussion
4.1. Proportion of Chronic Stress in Clinical Nurses
4.2. Emotional Experiences following Patient Death and Chronic Stress
4.3. Styles and Strategies for Coping with Chronic Stress
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Nomenclature
| Term | Definition |
| AC | Avoidant Coping Subscale |
| APA | American Psychological Association |
| B-COPE | Brief-COPE Scale |
| CI | Confidence Interval |
| COPE | Coping Orientation to Problems Experienced |
| COVID-19 | Coronavirus Disease |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders |
| DV | Dependent Variable |
| ECT | Emotional Freedom Techniques |
| E-FC | Emotion-Focused Coping Subscale |
| yr. | Year |
| F | F-Statistic |
| LB | Lower Bound |
| P | p-value |
| ɸ | Phi Coefficient |
| M | Mean |
| mo. | Month |
| AOR | Adjusted Odds Ratio |
| P-FC | Problem-Focused Coping Subscale |
| PRED | Unstandardized Predicted Value |
| PSS-10 | Perceived Stress Scale |
| R2 | R-Squared |
| SAM | Self-Assessment Manikin |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| UB | Upper bound |
| V | Cramer’s V Correlation Coefficient |
| VIF | Variance Inflation Factor |
| vs. | Versus |
| WHO | World Health Organization |
Appendix A

References
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological stress and disease. J. Am. Med. Assoc. 2007, 298, 1685–1687. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Press: Washington, DC, USA, 2013. [Google Scholar]
- Dhabhar, F.S. The short-term stress response–Mother nature’s mechanism for enhancing protection and performance under conditions of threat, challenge, and opportunity. Front. Neuroendocr. 2018, 49, 175–192. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Williamson, G. Perceived stress in a probability sample of the United States. In The Social Psychology of Health: Claremont Symposium on Applied Social Psychology; Spacapan, S., Oskamp, S., Eds.; Sage: Thousand Oaks, CA, USA, 1988. [Google Scholar]
- Vankar, P. Percentage of Individuals Worldwide Reporting Moderate to Severe Symptoms of Stress, Depression, and Anxiety in 2022, by Age Group. Statistika. 2023. Available online: https://www.statista.com/statistics/1400861/percentage-of-individuals-reporting-symptoms-of-stress-depression-anxiety-by-age-group-worldwide/ (accessed on 15 March 2024).
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Pandemic Triggers 25% Increase in Prevalence of Anxiety and Depression Worldwide. Wake-up call to All Countries to Step up Mental Health Services and Support. Available online: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (accessed on 23 January 2024).
- Parada, M.E.; Moreno, R.; Mejías, M.Z.; Rivas, F.A.; Rivas, F.F.; Cerrada, S.J.; Rivas, P.F. Job satisfaction and burnout syndrome in the nursing staff of the Instituto Autónomo Hospital Universitario Los Andes, Mérida, Venezuela. Rev. Fac. Nac. 2005, 23, 33–45. [Google Scholar]
- Tavares, J.P.; Cócaro, M.G.; Olino, L.; Vieira, L.S.; Magnago, T.S.B.D.S.; Dantas Filho, F.F.; Pai, D.D. Psychological changes in nursing professionals belonging to the risk group for complications of COVID-19. Texto Contexto-Enferm. 2022, 31, e20220449. [Google Scholar] [CrossRef]
- Rainho, C. Síndroma de Burnout em enfermeiros: Aplicação do questionário breve de Burnout. Nursing 2005, 16, 7–11. [Google Scholar]
- Gómez-Urquiza, J.L.; Monsalve-Reyes, C.S.; San Luis-Costas, C.; Fernández-Castillo, R.; Aguayo-Estremera, R.; Cañadas-de la Fuente, G.A. Factores de riesgo y niveles de burnout en enfermeras de atención primaria: Una revisión sistemática. Aten. Primaria 2017, 49, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Yazdanshenas, M.; Kavian, M.; Ahmadloo, M.; Jarchi, A.; Golchin, S.; Latifi, S.; Hossein, S.A.; Ghajarzadeh, M. The association between life satisfaction and the extent of depression, anxiety and stress among Iranian nurses: A multicenter survey. Iran J. Psychiatry 2016, 11, 120–127. [Google Scholar]
- Karasek, R.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Mao, A.; Tam, H.L.; Cheong, P.L.; Van, I.K. “You need to get over the difficulties and stand up again”—A qualitative inquiry into young nurses’ coping with lateral violence from the feminist perspective. Int. J. Environ. Res. Public Health 2021, 18, 7167. [Google Scholar] [CrossRef]
- Membrive-Jiménez, M.J.; Gómez-Urquiza, J.L.; Suleiman-Martos, N.; Velando-Soriano, A.; Ariza, T.; De la Fuente-Solana, E.I.; Cañadas-De la Fuente, G.A. Relation between burnout and sleep problems in nurses: A systematic review with meta-analysis. Healthcare 2022, 10, 954. [Google Scholar] [CrossRef] [PubMed]
- de Pinho, L.G.; Sampaio, F.; Sequeira, C.; Teixeira, L.; Fonseca, C.; Lopes, M.J. Portuguese nurses’ stress, anxiety, and depression reduction strategies during the COVID-19 outbreak. Int. J. Environ. Res. Public Health 2021, 18, 3490. [Google Scholar] [CrossRef] [PubMed]
- Salvagioni, D.A.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; de Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef] [PubMed]
- American Nurses Association. Combating Stress. Available online: https://www.nursingworld.org/practice-policy/work-environment/health-safety/combating-stress/ (accessed on 1 April 2024).
- Costeira, C.; Ventura, F.; Pais, N.; Santos-Costa, P.; Dixe, M.A.; Querido, A.; Laranjeira, C. Workplace stress in Portuguese oncology nurses delivering palliative care: A pilot study. Nurs. Rep. 2022, 12, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Üstükuş, A.; Eskimez, Z. The effect of death anxiety in nurses on their approach to dying patients: A cross-sectional study. Perspect. Psychiatr. Care 2021, 57, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Shen, M.; Li, Z. When cultural values meets professional values: A qualitative study of Chinese nurses’ attitudes and experiences concerning death. BMC Palliat. Care 2022, 21, 181. [Google Scholar]
- Khosrowabadi, R. Stress and perception of emotional stimuli: Long-term stress rewiring the brain. Basic Clin. Neurosci. 2018, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- Kostka, A.M.; Borodzicz, A.; Krzemińska, S.A. Feelings and emotions of nurses related to dying and death of patients—A pilot study. Psychol. Res. Behav. Manag. 2021, 14, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.C.; Chaves, C.; Campos, S. Coping strategies of nurses in terminal ill. Procedia Soc. Behav. Sci. 2014, 113, 171–180. [Google Scholar] [CrossRef][Green Version]
- Batista, P. Stress e Coping nos Enfermeiros dos Cuidados Paliativos em Oncologia. In Manual for the Ways of Coping Questionnaire (Research Edition); Folkman, S., Lazarus, R.S., Eds.; Consulting Psychologists Press: Palo Alto, CA, USA, 2008. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Ghanem, I.; Castelo, B.; Jimenez-Fonseca, P.; Carmona-Bayonas, A.; Higuera, O.; Beato, C.; García, T.; Hernández, R.; Calderon, C. Coping strategies and depressive symptoms in cancer patients. Clin. Transl. Oncol. 2020, 22, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Xu, F.; Liu, H. Emotional responses and coping strategies in nurses and nursing students during COVID-19 outbreak: A comparative study. PLoS ONE 2020, 15, e0237303. [Google Scholar] [CrossRef] [PubMed]
- Portero de la Cruz, S.; Cebrino, J.; Herruzo, J.; Vaquero-Abellán, M. A multicenter study into burnout, perceived stress, job satisfaction, coping strategies, and general health among emergency department nursing staff. J. Clin. Med. 2020, 9, 1007. [Google Scholar] [CrossRef] [PubMed]
- Büyükaşik-Çolak, C.; Gündoğdu-Aktürk, E.; Bozo, Ö. Mediating role of coping in the dispositional optimism–posttraumatic growth relation in breast cancer patients. J. Psychol. 2012, 146, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Sehularo, L.A.; Molato, B.J.; Mokgaola, I.O.; Gause, G. Coping strategies used by nurses during the COVID-19 pandemic: A narrative literature review. Health SA 2021, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You want to measure coping but your protocol is too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Wood, S.K.; Bhatnagar, S. Resilience to the effects of social stress: Evidence from clinical and preclinical studies on the role of coping strategies. Neurobiol. Stress 2015, 1, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Kalaitzaki, A.; Theodoratou, M.; Tsouvelas, G.; Tamiolaki, A.; Konstantakopoulos, G. Coping profiles and their association with vicarious post-traumatic growth among nurses during the three waves of the COVID-19 pandemic. J. Clin. Nurs. 2024. early view. [Google Scholar] [CrossRef] [PubMed]
- Dougall, A.L.; Wroble Biglan, M.C.; Swanson, J.N.; Baum, A. Stress, coping, and immune function. In Handbook of Psychology, 2nd ed.; Weiner, I.B., Nelson, R.J., Mizumori, S.J.Y., Eds.; John Wiley and Sons: New York, NY, USA, 2012; Volume 3, pp. 440–460. [Google Scholar]
- Tripathy, C.S.; Tripathy, S.; Gupta, B.; Kar, S.K. Stress, coping, and immunologic relevance: An empirical literature review. J. Med. Sci. 2019, 39, 107–113. [Google Scholar]
- Hedlund, M.; Ronne-Engström, E.; Carlsson, M.; Ekselius, L. Coping strategies, health-related quality of life and psychiatric history in patients with aneurysmal subarachnoid haemorrhage. Acta Neurochir. 2010, 152, 1375–1382. [Google Scholar] [CrossRef]
- Passier, P.E.C.A.; Visser-Meily, J.M.A.; van Zandvoort, M.J.E.; Rinkel, G.J.E.; Lindeman, E.; Post, M.W.M. Predictors of long-term Health-Related Quality of Life in patients with aneurysmal subarachnoid hemorrhage. Neuro. Rehabil. 2012, 30, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, J.; Jakobsson, H.; Rentzos, A.; Jakola, A.S.; Nilsson, D. Neurological outcome, mental fatigue, and occurrence of aneurysms > 15 years after aneurysmal subarachnoid hemorrhage. World Neurosurg. 2021, 151, e122–e127. [Google Scholar] [CrossRef] [PubMed]
- World Heath Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 26 March 2024).
- Lithuanian Parliament. On the Adoption of the Action Plan on Safety and Health at Work 2022–2027. Available online: https://e-seimas.lrs.lt/portal/legalact/lt/tad/81574c22b51711ec9f0095b4d96fd400?jfwid=- (accessed on 16 February 2024).
- Sullivan, K.M. Open Source Statistics for Public Health. Available online: http://www.openepi.com/SampleSize/SSCohort.htm (accessed on 15 August 2021).
- Ekman, P. Basic emotions. In Handbook of Cognition and Emotion; Dagleish, T., Power, M., Eds.; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 1999; pp. 45–60. [Google Scholar]
- Taylor, J.M. Psychometric analysis of the Ten-Item Perceived Stress Scale. Psychol. Assess. 2015, 27, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Janicki-Deverts, D. Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 20091. J. Appl. Soc. Psychol. 2012, 42, 1320–1334. [Google Scholar] [CrossRef]
- Geceviciene, S. Students, Studying Stress and Coping Strategies Correlation with Satisfaction at Studies. Master’s Thesis, Vytautas Magnus University, Faculty of Social Sciences, Kaunas, Lithuania, 2017; pp. 1–69. [Google Scholar]
- Dias, C.; Cruz, J.F.; Fonseca, A.M. The relationship between multidimensional competitive anxiety, cognitive threat appraisal, and coping strategies: A multi-sport study. Int. J. Sport Exerc. Psychol. 2012, 10, 52–65. [Google Scholar] [CrossRef]
- Perminas, A.; Galvydienė, E. Association between healthy diet and stress coping strategies among students. Int. J. Psychol. Biopsychosoc. Approach 2008, 1, 71–85. [Google Scholar]
- Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). Available online: https://www.strobe-statement.org/ (accessed on 15 February 2024).
- Antczak-Komoterska, A.; Haor, B.; Malinowska, M.; Grzelak, L.; Biercewicz, M.; Kochman, D.; Krajewska, K.; Filipska-Blejder, K.; Wiśniewski, A.; Ślusarz, R. Analysis of the level of stress and methods of coping with stress among the nursing staff. Nurs. Rep. 2023, 13, 1318–1330. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.; Mahapatra, S.S.; Sarkar, A.P.; Biswas, A. Stress and coping mechanism among nursing students of a selected tertiary care centre of West Bengal. Natl. J. Community Med. 2023, 14, 512–518. [Google Scholar] [CrossRef]
- Marciniak, A.; Ślusarska, B.; Nowicki, G. Empathetic skills and coping with cancer patients care difficulties among nurses. Palliat. Med. 2015, 7, 161–167. [Google Scholar]
- Muraczyńska, B. Nurses’ professional problems in palliative care-selected issues. Ann. UMCS Sect. I 2001, 15, 201–206. [Google Scholar]
- Gułag, B. Difficult situations in the work environment of nurses and the ability to deal with them. Nurs. Public Health 2004, 114, 367–370. [Google Scholar]
- Sleziona, M.; Krzyżanowski, D. Attitudes of the nurses in the face of patient’ dying and death. Nurs. Public Health 2011, 1, 217–223. [Google Scholar]
- Makowicz, D.; Dziubaszewska, R.; Makowicz, N.; Barna, P.; Piękoś, M. The attitude of nursing staff towards the death and dying of the patient. Nurs. 21st Century 2019, 18, 151–161. [Google Scholar] [CrossRef]
- Givon, E.; Itzhak-Raz, A.; Karmon-Presser, A.; Danieli, G.; Meiran, N. How does the emotional experience evolve? Feeling generation as evidence accumulation. Emotion 2020, 20, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.D. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, U. Stress and (public) health. In International Encyclopedia of Public Health; Heggenhougen, K., Ed.; Academic Press: Oxford, UK, 2008; pp. 241–250. [Google Scholar]
- Kowalczuk, K.; Shpakou, A.; Hermanowicz, J.M.; Krajewska-Kułak, E.; Sobolewski, M. Strategies for coping with stress used by nurses in Poland and Belarus during the COVID-19 pandemic. Front. Psychiatry 2022, 13, 867148. [Google Scholar] [CrossRef] [PubMed]
- Siemianowska, T.; Podsiadły, D.; Slusarz, R. Occupational stress reactions among nurses working in behavioral wards. Innov. Nurs. Health Sci. 2018, 4, 9–23. [Google Scholar]
- Chang, E.M.; Bidewell, J.W.; Huntington, A.D.; Daly, J.; Johnson, A.; Wilson, H.; Lambert, V.A.; Lambert, C.E. A survey of role stress, coping and health in Australian and New Zealand hospital nurses. Int. J. Nurs. Stud. 2007, 44, 1354–1362. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, T.D. Coping strategies among nurses in South-West Ethiopia: Descriptive, institution-based cross-sectional study. BMC Res. Notes 2018, 11, 421. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, C.; Pan, W.; Zheng, J.; Gao, J.; Huang, X.; Cai, S.; Zhai, Y.; Latour, J.M.; Zhu, C. Stress, burnout, and coping strategies of frontline nurses during the COVID-19 epidemic in wuhan and Shanghai, China. Front. Psychiatry 2020, 11, 565520. [Google Scholar] [CrossRef] [PubMed]
- Catapano, P.; Cipolla, S.; Sampogna, G.; Perris, F.; Luciano, M.; Catapano, F.; Fiorillo, A. Organizational and individual interventions for managing work-related stress in healthcare professionals: A systematic review. Medicina 2023, 59, 1866. [Google Scholar] [CrossRef] [PubMed]
- APA Dictionary of Psychology. Available online: https://dictionary.apa.org/disengagement (accessed on 3 April 2024).
- Janoff-Bulman, R. Characterological versus behavioral self-blame: Inquiries into depression and rape. J. Pers. Soc. Psychol. 1979, 37, 1798–1809. [Google Scholar] [CrossRef] [PubMed]
- Balzarotti, S.; Biassoni, F.; Villani, D.; Prunas, A.; Velotti, P. Individual differences in cognitive emotion regulation: Implications for subjective and psychological well-being. J. Happiness Stud. 2016, 17, 125–143. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, F.; Zhang, S.; Liu, C.; Feng, Y.; Chen, J. Effects of a mindfulness-based interventions on stress, burnout in nurses: A systematic review and meta-analysis. Front. Psychiatry 2023, 14, 1218340. [Google Scholar] [CrossRef] [PubMed]
- Lang, P.J. Behavioral treatment and bio-behavioral assessment: Computer applications. In Technology in Mental Health Care Delivery Systems; Sidowski, J., Johnson, J., Williams, T., Eds.; Ablex Pub.: Norwood, NJ, USA, 1980; pp. 119–137. [Google Scholar]



| PSS-10 Points | Sten | Perceived Stress Level | n | % |
|---|---|---|---|---|
| Below 7 | 1 | Low | 11 | 3.9 |
| 8–10 | 2 | 19 | 6.7 | |
| 11–13 | 3 | 37 | 13.1 | |
| 14–17 | 4 | Moderate | 66 | 23.3 |
| 18–20 | 5 | 57 | 20.1 | |
| 21–23 | 6 | 43 | 15.2 | |
| 24–25 | 7 | 28 | 9.9 | |
| 26–27 | 8 | High | 7 | 2.5 |
| 28–30 | 9 | 12 | 4.2 | |
| Over 31 | 10 | 3 | 1.1 |
| Variables | Self-Perceived Chronic Stress Levels | φ a/V b | p | |||
|---|---|---|---|---|---|---|
| Low (Score: 0–13) | Moderate–High (Score: 14–40) | |||||
| n | % | n | % | |||
| Age (yr.) (M (SD)) | 40.9 (11.9) | 36.1 (11.4) | ||||
| Age category | ||||||
| 20 to 37 years old | 29 | 19.6 | 119 | 80.4 | –0.1 a | 0.091 |
| 38 to 70 years old | 38 | 28.1 | 97 | 71.9 | ||
| Educational attainment | ||||||
| University | 31 | 20.7 | 119 | 79.3 | –0.1 a | 0.206 |
| College | 36 | 27.1 | 97 | 72.9 | ||
| Marital status | ||||||
| In a relationship | 15 | 22.4 | 52 | 77.6 | 0.1 b | 0.494 |
| Divorced | 4 | 22.2 | 14 | 77.8 | ||
| Married | 31 | 21.1 | 116 | 78.9 | ||
| Widowed | 2 | 40.0 | 3 | 60.0 | ||
| Single | 15 | 32.6 | 31 | 67.4 | ||
| Workplace | ||||||
| Intensive care unit | 19 | 28.8 | 47 | 71.2 | –0.1 b | 0.464 |
| Surgical profile unit | 7 | 28.0 | 18 | 72.0 | ||
| Therapeutic profile unit | 17 | 25.0 | 51 | 75.8 | ||
| Emergency profile unit | 24 | 19.4 | 100 | 80.6 | ||
| Nursing shifts | ||||||
| Day shifts | 14 | 21.9 | 50 | 78.1 | –0.1 b | 0.683 |
| Night shifts | 8 | 19.5 | 33 | 80.5 | ||
| Mixture of day and night shifts | 45 | 25.3 | 133 | 74.7 | ||
| Experiences with patient loss | ||||||
| One time or several times a year | 35 | 31.0 | 78 | 69.0 | 0.2 a | 0.019 |
| Several times a month | 32 | 18.8 | 138 | 81.2 | ||
| Nursing experience | ||||||
| 9.1–50 years | 25 | 37.3 | 117 | 54.2 | 0.2 a | 0.016 |
| 0.5–9.0 years | 42 | 29.8 | 99 | 70.2 | ||
| Model | Independent Variable | β (SE) | Wald | p | AOR 95% CI (LB; UB) |
|---|---|---|---|---|---|
| 1. PSS-10 (score: 14–40) a × 1 | Guilt (+) 1 | 1.6 (0.6) | 6.3 | 0.012 | 4.7 [1.4; 5.7] |
| 2. PSS-10 (score: 14–40) a × 2 | Compassion (+) 2 | –0.2 (0.3) | 0.4 | 0.530 | 0.8 [0.4; 1.5] |
| 3. PSS-10 (score: 14–40) a × 3 | Disappointment (+) 3 | 0.6 (0.3) | 5.2 | 0.039 | 1.9 [1.1; 3.5] |
| 4. PSS-10 (score: 14–40) a × 4 | Sadness (+) 4 | 0.3 (0.3) | 1.4 | 0.236 | 1.4 [0.8; 2.5] |
| 5. PSS-10 (score: 14–40) a × 5 | Depressed mood (+) 5 | 1.7 (1.0) | 2.6 | 0.110 | 5.3 [0.7; 8.6] |
| 6. PSS-10 (score: 14–40) a × 6 | Despair (+) 6 | 0.8 (0.6) | 2.1 | 0.144 | 2.3 [0.8; 6.7] |
| 7. PSS-10 (score: 14–40) a × 7 | Calmness (+) 7 | –0.5 (0.2) | 5.9 | 0.045 | 0.6 [0.3; 0.9] |
| 8. PSS-10 (score: 14–40) a × 8 | Anger (+) 8 | 0.8 (0.6) | 2.1 | 0.144 | 2.3 [0.8; 2.7] |
| 9. PSS-10 (score: 14–40) a × 9 | Helplessness (+) 9 | 0.6 (0.2) | 5.1 | 0.041 | 1.7 [1.1; 2.9] |
| 10. PSS-10 (score: 14–40) a × 10 | Grief (+) 10 | 0.02 (0.3) | 0.1 | 0.944 | 1.0 [0.6; 1.8] |
| 11. PSS-10 (score: 14–40) a × 11 | Anxiety (+) 11 | 0.7 (0.3) | 5.8 | 0.049 | 1.9 [1.2; 4.2] |
| Model | Independent Variable | β | 95% CI [LB; UB] | p | F4,278 | VIF | R2 |
|---|---|---|---|---|---|---|---|
| 1. PSS-10 a | Brief-COPE scale | 0.04 | [−0.02; 0.1] | 0.170 | 7.9 | 1.1 | 0.09 |
| 1.1. PSS-10 b | Avoidant coping | 0.5 | [0.4; 0.7] | <0.001 | 23.2 | 1.1 | 0.24 |
| 1.1.1 PSS-10 b × 1 | Denial 1 | 1.6 | [0.7; 2.4] | <0.001 | 11.0 | 1.0 | 0.14 |
| 1.1.2. PSS-10 b × 2 | Behavioral disengagement 2 | 3.0 | [2.3; 3.8] | <0.001 | 24.3 | 1.0 | 0.26 |
| 1.1.3. PSS-10 b × 3 | Self-distraction 3 | 1.4 | [0.7; 2.2] | <0.001 | 11.3 | 1.1 | 0.14 |
| 1.1.4. PSS-10 b × 4 | Substance use 4 | 1.9 | [1.1; 2.7] | <0.001 | 13.7 | 1.1 | 0.17 |
| 1.2. PSS-10 c | Emotion-focused coping | 0.1 | [−0.1; 0.2] | 0.360 | 10.9 | 1.1 | 0.12 |
| 1.2.1. PSS-10 c × 1 | Use of emotional support 1 | −1.1 | [−1.8; −0.3] | 0.006 | 9.6 | 1.0 | 0.12 |
| 1.2.2. PSS-10 c × 2 | Humor 2 | 0.7 | [−0.04; −1.4] | 0.063 | 8.4 | 1.0 | 0.11 |
| 1.2.3. PSS-10 c × 3 | Religion 3 | −0.2 | [−0.8; 0.5] | 0.646 | 7.5 | 1.0 | 0.09 |
| 1.2.4. PSS-10 c × 4 | Venting 4 | −0.2 | [−0.9; 0.6] | 0.669 | 7.5 | 1.0 | 0.09 |
| 1.2.5. PSS-10 c × 5 | Acceptance 5 | −1.2 | [−2.1; −0.4] | 0.006 | 9.5 | 1.0 | 0.12 |
| 1.2.6. PSS-10 c × 6 | Self-blame 6 | 3.0 | [2.3; 3.7] | <0.001 | 26.8 | 1.2 | 0.27 |
| 1.3. PSS-10 d | Problem-focused coping | −0.2 | [−0.3; −0.1] | <0.001 | 7.7 | 1.0 | 0.09 |
| 1.3.1. PSS-10 d × 1 | Active coping 1 | −1.1 | [−2.1; −0.1] | 0.027 | 6.7 | 1.0 | 0.08 |
| 1.3.2. PSS-10 d × 2 | Positive reframing 2 | −1.4 | [−2.2; −0.6] | 0.001 | 10.8 | 1.0 | 0.14 |
| 1.3.3. PSS-10 d × 3 | Use of instrumental support 3 | −0.5 | [−1.2; −0.3] | 0.198 | 7.9 | 1.0 | 0.10 |
| 1.3.4. PSS-10 d × 4 | Planning 4 | −0.2 | [−0.9; 0.6] | 0.645 | 7.5 | 1.0 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baranauskas, M.; Kalpokas, M.; Kupčiūnaitė, I.; Lieponienė, J.; Stukas, R. Self-Perceived Stress in Association with Emotional Experiences Following Patient Death and Coping Adequacy among Clinical Nurses in Lithuania: A Cross-Sectional Study. J. Clin. Med. 2024, 13, 2533. https://doi.org/10.3390/jcm13092533
Baranauskas M, Kalpokas M, Kupčiūnaitė I, Lieponienė J, Stukas R. Self-Perceived Stress in Association with Emotional Experiences Following Patient Death and Coping Adequacy among Clinical Nurses in Lithuania: A Cross-Sectional Study. Journal of Clinical Medicine. 2024; 13(9):2533. https://doi.org/10.3390/jcm13092533
Chicago/Turabian StyleBaranauskas, Marius, Marius Kalpokas, Ingrida Kupčiūnaitė, Jurgita Lieponienė, and Rimantas Stukas. 2024. "Self-Perceived Stress in Association with Emotional Experiences Following Patient Death and Coping Adequacy among Clinical Nurses in Lithuania: A Cross-Sectional Study" Journal of Clinical Medicine 13, no. 9: 2533. https://doi.org/10.3390/jcm13092533
APA StyleBaranauskas, M., Kalpokas, M., Kupčiūnaitė, I., Lieponienė, J., & Stukas, R. (2024). Self-Perceived Stress in Association with Emotional Experiences Following Patient Death and Coping Adequacy among Clinical Nurses in Lithuania: A Cross-Sectional Study. Journal of Clinical Medicine, 13(9), 2533. https://doi.org/10.3390/jcm13092533