

Prostate Artery Embolization as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review
 , , , , ,
, , , , , 
 ,
,  ,
,
Abstract
1. Introduction
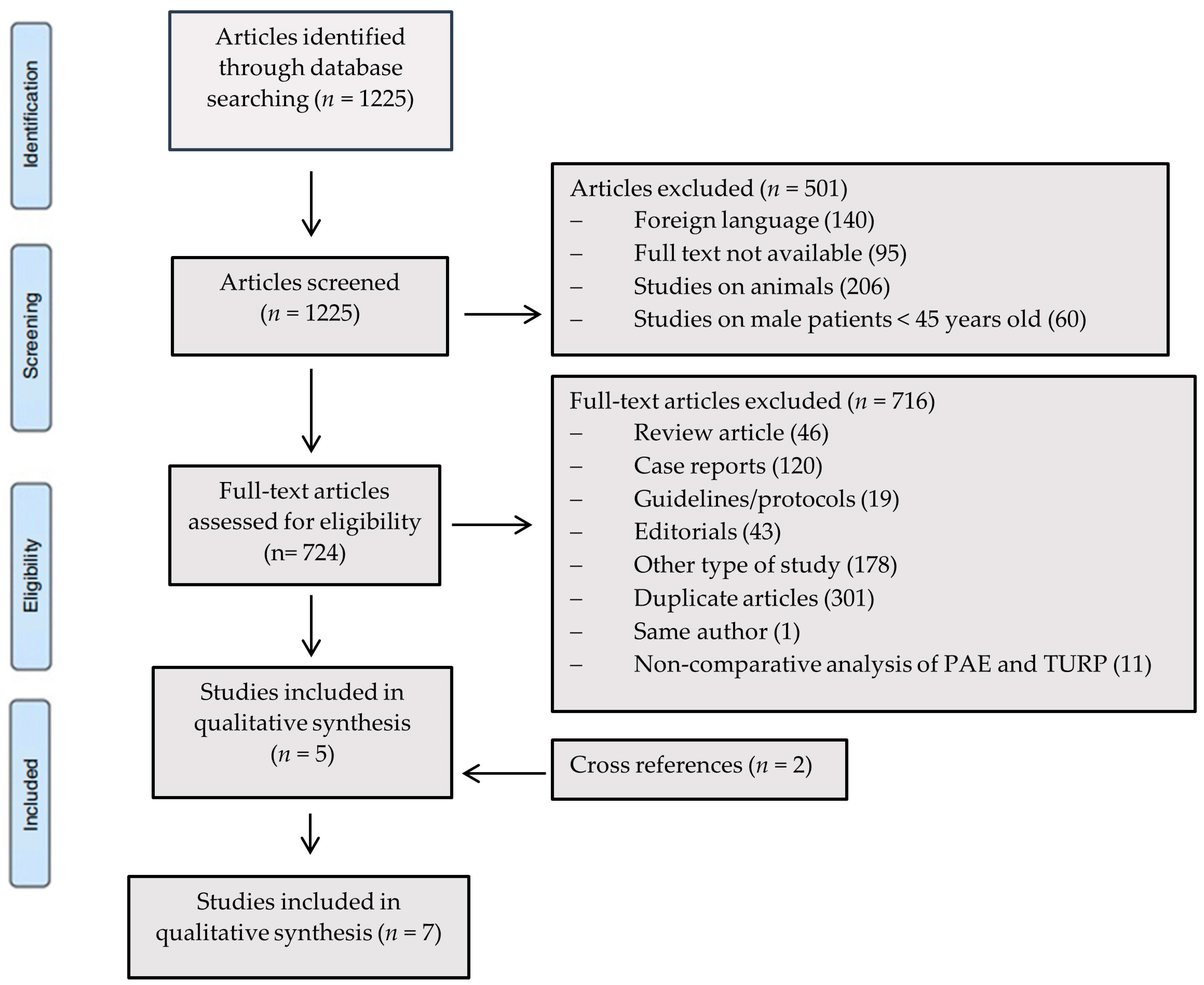
2. Materials and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devlin, C.M.; Simms, M.S.; Maitland, N.J. Benign prostatic hyperplasia—What do we know? BJU Int. 2021, 127, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Vuichoud, C.; Loughlin, K.R. Benign prostatic hyperplasia: Epidemiology, economics and evaluation. Can. J. Urol. 2015, 22, 1–6. [Google Scholar] [PubMed]
- Egan, K.B. The Epidemiology of Benign Prostatic Hyperplasia Associated with Lower Urinary Tract Symptoms: Prevalence and Incident Rates. Urol. Clin. N. Am. 2016, 43, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Oelke, M.; Bachmann, A.; Descazeaud, A.; Emberton, M.; Gravas, S.; Michel, M.C.; N’dow, J.; Nordling, J.; de la Rosette, J.J. European Association of Urology. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur. Urol. 2013, 64, 118–140. [Google Scholar] [CrossRef] [PubMed]
- Csikós, E.; Horváth, A.; Ács, K.; Papp, N.; Balázs, V.L.; Dolenc, M.S.; Kenda, M.; Kočevar Glavač, N.; Nagy, M.; Protti, M.; et al. Treatment of Benign Prostatic Hyperplasia by Natural Drugs. Molecules 2021, 26, 7141. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Allkanjari, O.; Busetto, G.M.; Cai, T.; Larganà, G.; Magri, V.; Perletti, G.; Robustelli Della Cuna, F.S.; Russo, G.I.; Stamatiou, K.; et al. Nutraceutical treatment and prevention of benign prostatic hyperplasia and prostate cancer. Arch. Ital. Urol. Androl. 2019, 91. [Google Scholar] [CrossRef]
- McVary, K.T.; Roehrborn, C.G.; Avins, A.L.; Barry, M.J.; Bruskewitz, R.C.; Donnell, R.F.; Foster, H.E., Jr.; Gonzalez, C.M.; Kaplan, S.A.; Penson, D.F.; et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J. Urol. 2011, 185, 1793–1803. [Google Scholar] [CrossRef] [PubMed]
- Picel, A.C.; Hsieh, T.C.; Shapiro, R.M.; Vezeridis, A.M.; Isaacson, A.J. Prostatic Artery Embolization for Benign Prostatic Hyperplasia: Patient Evaluation, Anatomy, and Technique for Successful Treatment. Radiographics 2019, 39, 1526–1548. [Google Scholar] [CrossRef] [PubMed]
- Foo, K.T. What is a disease? What is the disease clinical benign prostatic hyperplasia (BPH)? World J. Urol. 2019, 37, 1293–1296. [Google Scholar] [CrossRef] [PubMed]
- Sershon, P.D.; Barry, M.J.; Oesterling, J.E. Serum prostate-specific antigen discriminates weakly between men with benign prostatic hyperplasia and patients with organ-confined prostate cancer. Eur. Urol. 1994, 25, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Chapple, C.; Khoury, S.; Roehrborn, C.; de la Rosette, J.; International Scientific Committee. Evaluation and treatment of lower urinary tract symptoms in older men. J. Urol. 2009, 181, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Golzarian, J.; Antunes, A.A.; Bilhim, T.; Carnevale, F.C.; Konety, B.; McVary, K.T.; Parsons, J.K.; Pisco, J.M.; Siegel, D.N.; Spies, J.; et al. Prostatic artery embolization to treat lower urinary tract symptoms related to benign prostatic hyperplasia and bleeding in patients with prostate cancer: Proceedings from a multidisciplinary research consensus panel. J. Vasc. Interv. Radiol. 2014, 25, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Gratzke, C.; Bachmann, A.; Descazeaud, A.; Drake, M.J.; Madersbacher, S.; Mamoulakis, C.; Oelke, M.; Tikkinen, K.A.O.; Gravas, S. EAU Guidelines on the Assessment of Non-neurogenic Male Lower Urinary Tract Symptoms including Benign Prostatic Obstruction. Eur. Urol. 2015, 67, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Foster, H.E.; Barry, M.J.; Dahm, P.; Gandhi, M.C.; Kaplan, S.A.; Kohler, T.S.; Lerner, L.B.; Lightner, D.J.; Parsons, J.K.; Roehrborn, C.G.; et al. Surgical Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA Guideline. J. Urol. 2018, 200, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.M.; de Assis, A.M.; Carnevale, F.C.; Antunes, A.A.; Srougi, M.; Cerri, G.G. A Review of Adverse Events Related to Prostatic Artery Embolization for Treatment of Bladder Outlet Obstruction Due to BPH. Cardiovasc. Interv. Radiol. 2017, 40, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, F.C.; Iscaife, A.; Yoshinaga, E.M.; Moreira, A.M.; Antunes, A.A.; Srougi, M. Transurethral Resection of the Prostate (TURP) Versus Original and PErFecTED Prostate Artery Embolization (PAE) Due to Benign Prostatic Hyperplasia (BPH): Preliminary Results of a Single Center, Prospective, Urodynamic-Controlled Analysis. Cardiovasc. Interv. Radiol. 2016, 39, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Insausti, I.; Sáez de Ocáriz, A.; Galbete, A.; Capdevila, F.; Solchaga, S.; Giral, P.; Bilhim, T.; Isaacson, A.; Urtasun, F.; Napal, S. Randomized Comparison of Prostatic Artery Embolization versus Transurethral Resection of the Prostate for Treatment of Benign Prostatic Hyperplasia. J. Vasc. Interv. Radiol. 2020, 31, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.A.; Huang, Y.; Zhang, R.; Yang, Y.D.; Zhang, Q.; Hou, M.; Wang, Y. Benign prostatic hyperplasia: Prostatic arterial embolization versus transurethral resection of the prostate—A prospective, randomized, and controlled clinical trial. Radiology 2014, 270, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Radwan, A.; Farouk, A.; Higazy, A.; Samir, Y.R.; Tawfeek, A.M.; Gamal, M.A. Prostatic artery embolization versus transurethral resection of the prostate in management of benign prostatic hyperplasia. Prostate Int. 2020, 8, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Abt, D.; Müllhaupt, G.; Hechelhammer, L.; Markart, S.; Güsewell, S.; Schmid, H.P.; Mordasini, L.; Engeler, D.S. Prostatic Artery Embolisation Versus Transurethral Resection of the Prostate for Benign Prostatic Hyperplasia: 2-yr Outcomes of a Randomised, Open-label, Single-centre Trial. Eur. Urol. 2021, 80, 34–42. [Google Scholar] [CrossRef]
- Qiu, Z.; Zhang, C.; Wang, X.; Cheng, K.; Liang, X.; Wang, D.; Hou, S.; Wang, X. Clinical evaluation of embolization of the superior vesical prostatic artery for treatment of benign prostatic hyperplasia: A single-center retrospective study. Wideochir. Inne Tech. Maloinwazyjne 2017, 12, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.F.; Powell, J.; Speakman, M.J.; Longford, N.T.; DasGupta, R.; Bryant, T.; Modi, S.; Dyer, J.; Harris, M.; Carolan-Rees, G.; et al. Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: An observational study and propensity-matched comparison with transurethral resection of the prostate (the UK-ROPE study). BJU Int. 2018, 122, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Shin, J.H.; Tsao, T.F.; Ko, H.G.; Yoon, H.K.; Han, K.C.; Thamtorawat, S.; Hong, B. Prostatic Arterial Embolization for Control of Hematuria in Patients with Advanced Prostate Cancer. J. Vasc. Interv. Radiol. 2017, 28, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Sánchez, F.M.; Crisóstomo, V.; Lima, J.R.; Luis, L.; García-Martínez, V.; López-Sánchez, C.; Usón, J.; Maynar, M. Benign prostatic hyperplasia: Transcatheter arterial embolization as potential treatment--preliminary study in pigs. Radiology 2008, 246, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Jeon, G.S.; Won, J.H.; Lee, B.M.; Kim, J.H.; Ahn, H.S.; Lee, E.J.; Park, S.I.; Park, S.W. The effect of transarterial prostate embolization in hormone-induced benign prostatic hyperplasia in dogs: A pilot study. J. Vasc. Interv. Radiol. 2009, 20, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, F.C.; Antunes, A.A.; da Motta Leal Filho, J.M.; de Oliveira Cerri, L.M.; Baroni, R.H.; Marcelino, A.S.; Freire, G.C.; Moreira, A.M.; Srougi, M.; Cerri, G.G. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: Preliminary results in two patients. Cardiovasc. Interv. Radiol. 2010, 33, 355–361. [Google Scholar] [CrossRef] [PubMed]
- McWilliams, J.P.; Bilhim, T.A.; Carnevale, F.C.; Bhatia, S.; Isaacson, A.J.; Bagla, S.; Sapoval, M.R.; Golzarian, J.; Salem, R.; McClure, T.D.; et al. Society of Interventional Radiology Multisociety Consensus Position Statement on Prostatic Artery Embolization for Treatment of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: From the Society of Interventional Radiology, the Cardiovascular and Interventional Radiological Society of Europe, Société Française de Radiologie, and the British Society of Interventional Radiology: Endorsed by the Asia Pacific Society of Cardiovascular and Interventional Radiology, Canadian Association for Interventional Radiology, Chinese College of Interventionalists, Interventional Radiology Society of Australasia, Japanese Society of Interventional Radiology, and Korean Society of Interventional Radiology. J. Vasc. Interv. Radiol. 2019, 30, 627–637. [Google Scholar] [PubMed]
- Sun, F.; Crisóstomo, V.; Báez-Díaz, C.; Sánchez, F.M. Prostatic Artery Embolization (PAE) for Symptomatic Benign Prostatic Hyperplasia (BPH): Part 2, Insights into the Technical Rationale. Cardiovasc. Interv. Radiol. 2016, 39, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, F.H.; Bilhim, T.; Hacking, N.; Sapoval, M.; Tapping, C.R.; Carnevale, F.C. CIRSE Standards of Practice on Prostatic Artery Embolisation. Cardiovasc. Interv. Radiol. 2020, 43, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Monaco, R.; Garategui, L.; Kizilevsky, N.; Peralta, O.; Rodriguez, P.; Palacios-Jaraquemada, J. Human cadaveric specimen study of the prostatic arterial anatomy: Implications for arterial embolization. J. Vasc. Interv. Radiol. 2014, 25, 315–322. [Google Scholar] [CrossRef]
- DeMeritt, J.S.; Wajswol, E.; Wattamwar, A.; Osiason, A.; Chervoni-Knapp, T.; Zamudio, S. Duplicated Prostate Artery Central Gland Blood Supply: A Retrospective Analysis and Classification System. J. Vasc. Interv. Radiol. 2018, 29, 1595–1600. [Google Scholar] [CrossRef] [PubMed]
- Bagla, S.; Smirniotopoulos, J.; Orlando, J.; Piechowiak, R. Cost Analysis of Prostate Artery Embolization (PAE) and Transurethral Resection of the Prostate (TURP) in the Treatment of Benign Prostatic Hyperplasia. Cardiovasc. Interv. Radiol. 2017, 40, 1694–1697. [Google Scholar] [CrossRef] [PubMed]
- Ini’, C.; Distefano, G.; Sanfilippo, F.; Castiglione, D.G.; Falsaperla, D.; Giurazza, F.; Mosconi, C.; Tiralongo, F.; Foti, P.V.; Palmucci, S.; et al. Embolization for acute nonvariceal bleeding of upper and lower gastrointestinal tract: A systematic review. CVIR Endovasc. 2023, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Svarc, P.; Taudorf, M.; Nielsen, M.B.; Stroomberg, H.V.; Røder, M.A.; Lönn, L. Postembolization Syndrome after Prostatic Artery Embolization: A Systematic Review. Diagnostics 2020, 10, 659. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.L.; Qian, L.J. Transurethral resection of the prostate versus prostatic artery embolization in the treatment of benign prostatic hyperplasia: A meta-analysis. BMC Urol. 2019, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; McCutcheon, K.A.; Borofsky, M.; Young, S.; Golzarian, J.; Kim, M.H.; Narayan, V.M.; Dahm, P. Prostatic arterial embolization for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia. Cochrane Database Syst. Rev. 2022, 12, CD012867. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Ferreira, R.; Barragan, C.; Bhojani, N.; Lajkosz, K.; Zorn, K.C.; Chughtai, B.; Annamalai, G.; Elterman, D.S. Comparing prostatic artery embolization to surgical and minimally invasive procedures for the treatment of benign prostatic hyperplasia: A systematic review and meta-analysis. BMC Urol. 2024, 24, 22. [Google Scholar] [CrossRef] [PubMed]
- Sajan, A.; Mehta, T.; Desai, P.; Isaacson, A.; Bagla, S. Minimally Invasive Treatments for Benign Prostatic Hyperplasia: Systematic Review and Network Meta-Analysis. J. Vasc. Interv. Radiol. 2022, 33, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Malling, B.; Røder, M.A.; Brasso, K.; Forman, J.; Taudorf, M.; Lönn, L. Prostate artery embolisation for benign prostatic hyperplasia: A systematic review and meta-analysis. Eur. Radiol. 2019, 29, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Bilhim, T. Prostatic Artery Embolization: An Update. Korean J. Radiol. 2023, 24, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Bilhim, T.; McWilliams, J.P.; Bagla, S. Updated American Urological Association Guidelines for the Management of Benign Prostatic Hyperplasia: Prostatic Artery Embolization Made it into the Guidelines! Cardiovasc. Interv. Radiol. 2024, 47, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Pisco, J.M.; Bilhim, T.; Pinheiro, L.C.; Fernandes, L.; Pereira, J.; Costa, N.V.; Duarte, M.; Oliveira, A.G. Medium- and Long-Term Outcome of Prostate Artery Embolization for Patients with Benign Prostatic Hyperplasia: Results in 630 Patients. J. Vasc. Interv. Radiol. 2016, 27, 1115–1122. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Grade | Definition |
|---|---|
| I | Any unexpected deviation from the normal post-embolization course without the need for additional pharmacological, urologic surgical/endoscopic, or radiological procedures. |
| II | The need for pharmacological treatment with drugs other than those allowed for grade I, as therapeutic use of antibiotics due to infection. Indwelling catheters are used in case of early acute urinary retention. Additional non-invasive tests. |
| III | The need for pharmacological treatment with drugs used in grade II, as well as surgical/endoscopic or radiological procedures, under or without general anesthesia. |
| IV | Any deviation from the normal post-embolization course with a life-threatening complication requiring ICU-management due to single or multi-organ dysfunction. |
| V | Death |
| Suffix ‘d’ | The suffix “d” (for disability) is added to the complication grade if the patient has a complication at the time of discharge, indicating the need for a follow-up to fully evaluate the complication |
| First Author, Year | Type of Study Design | Number of Patients | Embolic Material (PAE) | Mean Procedure Time (min) | Mean Fluoroscopy Time (min) | Age Mean (SD) | Follow-up (Months) | Mean Hospital Stay (Days) |
|---|---|---|---|---|---|---|---|---|
| Insausti, 2020 [17] | Randomized controlled trial | PAE (23) B-TURP (22) | 300–500 µm of polyvinyl alcohol microspheres | PAE 138.7 TURP 70.2 | PAE 58.0 TURP N/A | PAE 72.4 (6.2) TURP 71.8 (5.5) | 12 | PAE 1 TURP 1 |
| Abt, 2021 [20] | Randomized controlled trial | PAE (48) M-TURP (51) | 250–400 µm embozene microspheres (Boston Scientific, Boston, MA, USA) | Not collected | Not collected | PAE 65.7 (9.3) TURP 66.1 (9.8) | 24 | PAE 2.2 TURP 4.2 |
| Carnevale, 2016 [16] | Randomized controlled trial | PAE (15) PERFECTED (15) M-TURP (15) | 300–500 µm tris-acryl gelatin microspheres (embosphere microspheres; Merit Medical, South Jordan, UT, USA) | PAE 144.8 PERFECTED 147.5 TURP 61.7 | PAE 49.2 PERFECTED 45.8 TURP N/A | PAE 63.5 (8.7) PERFECTED 60.4 (5.2) TURP 66.4 (5.6) | 12 | PAE not mentioned PERFECTED 6 hours TURP 2.1 |
| Gao, 2014 [18] | Randomized controlled trial | PAE (54) B-TURP (53) | Polyvinyl alcohol microspheres (355–500 µm, Ivalon; Cook, IL, USA) | PAE 89.7 TURP 83.5 | PAE 33.2 TURP N/A | PAE 67.7 (8.7) TURP 66.4 (7.8) | 1–3–6–12–24 | PAE 2.9 TURP 4.8 |
| Radwan, 2020 [19] | Randomized controlled trial | PERFECTED(20) M-TURP(20) B-TURP (20) | Microspheres | PAE 89 M-TURP 59 B-TURP 68 | PAE (Not collected) TURP N/A | PERFECTED 63 TURP 63 | 1–6 | Not mentioned |
| Ray, 2018 [22] | Observational study | PAE (216) M-TURP(45) B-TURP (44) | - | PAE 144 TURP (Not collected) | PAE 38 TURP N/A | PAE 66 (7.4) TURP 70 (7.5) | 1–3–6–12 | Not mentioned |
| Qiu, 2017 [21] | Observational study | PAE (17) B-TURP (40) | Embosphere microspheres (90–180 µm; Merit Medical, Rockland, MA, USA) | PAE 90 TURP (Not collected) | PAE (Not collected) TURP N/A | PAE 75.35 (4.74) TURP 73.35 (4.75) | 3–6–12 | Not mentioned |
| Fist Author, Year | Number of Patients | PAE Complications (Mean Rate) | TURP Complications (Mean Rate) |
|---|---|---|---|
| Insausti, 2020 [17] | PAE (23) B-TURP (22) | Grade I * 26.7% Grade II * 73.3% Grade III * 0.0% | Grade I * 53.2% Grade II * 44.7% Grade III * 2.1% |
| Abt, 2021 [20] | PAE (48) M-TURP (51) | Grade I * 66% Grade II * 24% Grade III * 11% | Grade I * 64% Grade II * 22% Grade III * 15% |
| Carnevale, 2016 [16] | PAE (15) PERFECTED (15) M-TURP (15) | •Transient minimal rectal bleeding (6.7% in each group) ** •Hematospermia (6.7% in each group) ** •Reduction in ejaculate volume (13.3% in PAE group, 6.7% in PERFECTED group) ** •Transient pubic bone ischemia (6.7% in PAE group) ** •Hematuria (13.3% in PAE group) ** | •Pollakuria, dysuria, and hematuria (100%) ** •Intra-operative damage to the left venous sinus and rupture of the prostatic capsule (6.7%) ** •Hematuria (6.7%) ** •Early urinary incontinence (26.7%) ** •Retrograde ejaculation (100%) ** •Prostate cancer identified incidentally (6.7%) ** |
| Gao, 2014 [18] | PAE (54) B-TURP (53) | Minor advent * 40.7% Major advent * 14.8% | Minor advent * 24.5% Major advent * 7.54% |
| Radwan, 2020 [19] | PERFECTED (20) M-TURP (20) B-TURP (20) | •Acute urinary retention following catheter removal (10%) •Postembolization syndrome (20%) •Severe perianal pain (20%) | Not mentioned |
| Ray, 2018 [22] | PAE (216) M-TURP (45) B-TURP (44) | •Hematuria 18.6% •Hematospermia 12.6% •Incontinence 1.0% •Urinary infection 5.0% •Retrograde ejaculation 24.1% | •Hematuria 63.9% •Hematospermia 1.6% •Incontinence 3.3% •Urinary infection 1.6% •Retrograde ejaculation 47.5% |
| Qiu, 2017 [21] | PAE (17) B-TURP (40) | •Hypogastralgia (pain in the perineum, retropubic space, and/or urethra) 17.6% •Fever 29.4% | Not mentioned |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ini’, C.; Vasile, T.; Foti, P.V.; Timpanaro, C.; Castiglione, D.G.; Libra, F.; Falsaperla, D.; Tiralongo, F.; Giurazza, F.; Mosconi, C.; et al. Prostate Artery Embolization as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review. J. Clin. Med. 2024, 13, 2530. https://doi.org/10.3390/jcm13092530
Ini’ C, Vasile T, Foti PV, Timpanaro C, Castiglione DG, Libra F, Falsaperla D, Tiralongo F, Giurazza F, Mosconi C, et al. Prostate Artery Embolization as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review. Journal of Clinical Medicine. 2024; 13(9):2530. https://doi.org/10.3390/jcm13092530
Chicago/Turabian StyleIni’, Corrado, Tiziana Vasile, Pietro Valerio Foti, Concetta Timpanaro, Davide Giuseppe Castiglione, Federica Libra, Daniele Falsaperla, Francesco Tiralongo, Francesco Giurazza, Cristina Mosconi, and et al. 2024. "Prostate Artery Embolization as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review" Journal of Clinical Medicine 13, no. 9: 2530. https://doi.org/10.3390/jcm13092530
APA StyleIni’, C., Vasile, T., Foti, P. V., Timpanaro, C., Castiglione, D. G., Libra, F., Falsaperla, D., Tiralongo, F., Giurazza, F., Mosconi, C., David, E., Palmucci, S., Lavalle, S., Venturini, M., & Basile, A. (2024). Prostate Artery Embolization as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review. Journal of Clinical Medicine, 13(9), 2530. https://doi.org/10.3390/jcm13092530