
The Real-World Effectiveness, Persistence, Adherence, and Safety of Janus Kinase Inhibitor Baricitinib in Rheumatoid Arthritis: A Long-Term Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
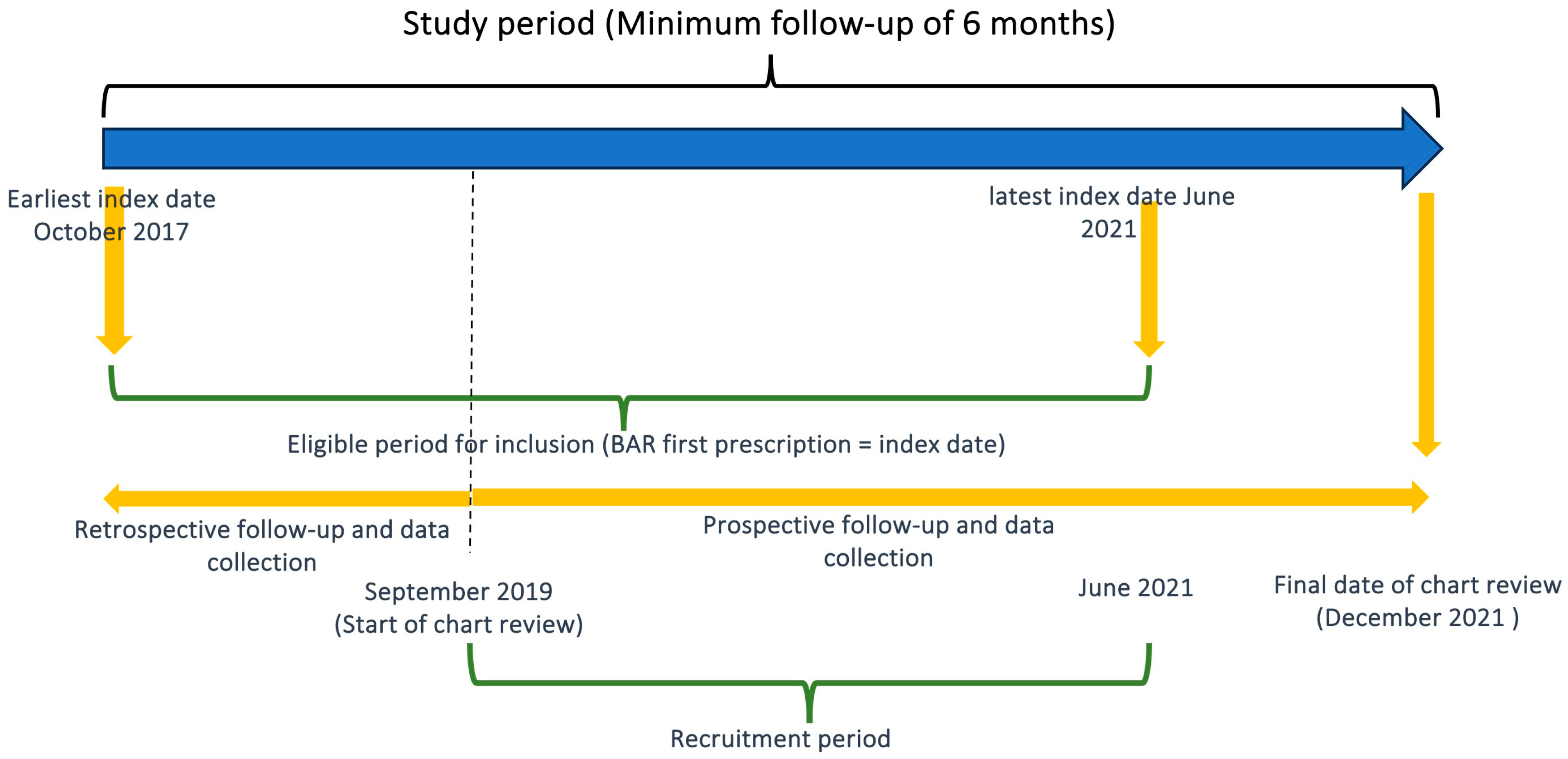
2.1. Study Design and Population
2.2. Outcomes
2.3. Statistical Analysis
3. Results
3.1. Baseline Population Demographics and Treatments Patterns
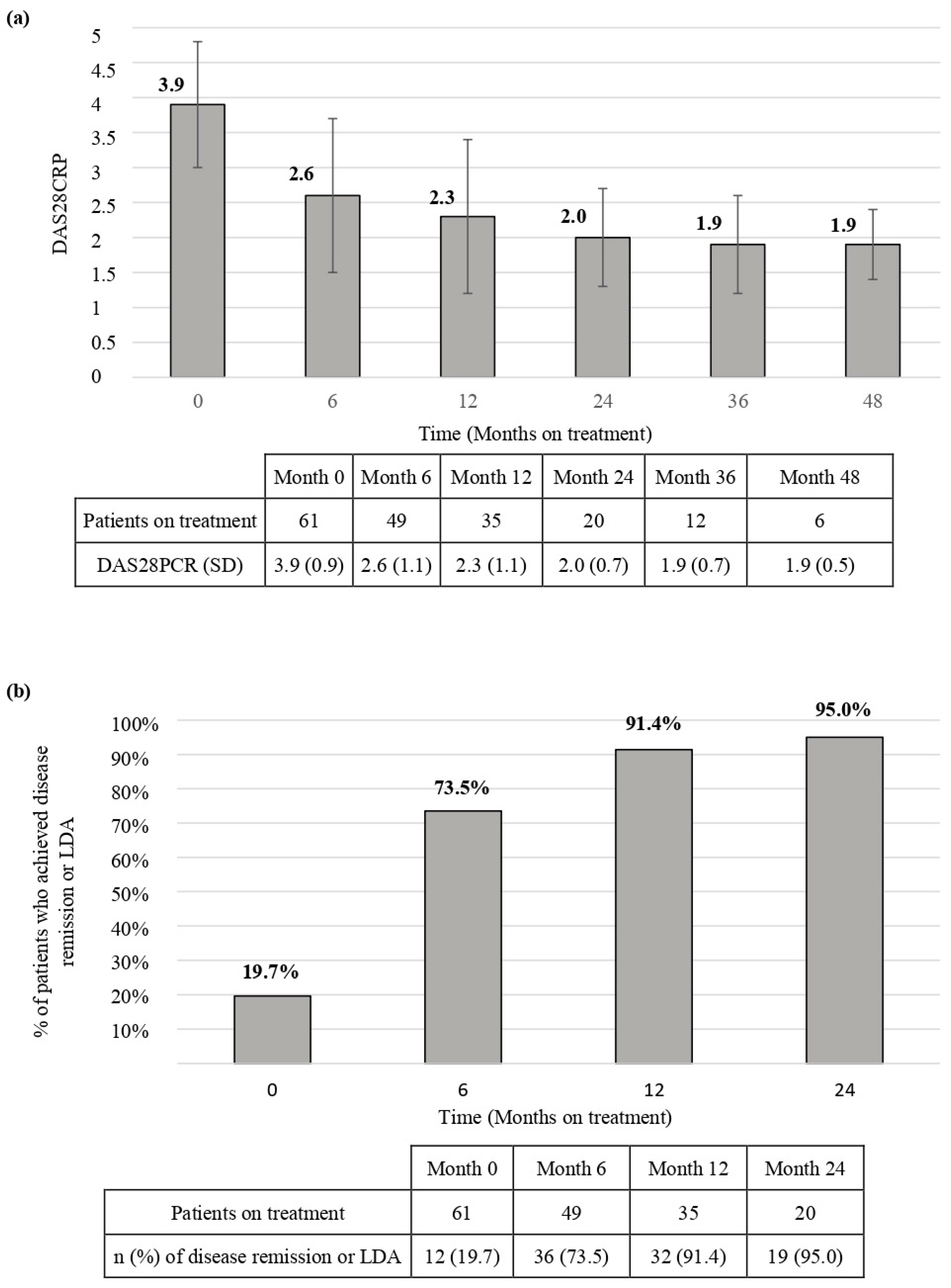
3.2. Effectiveness
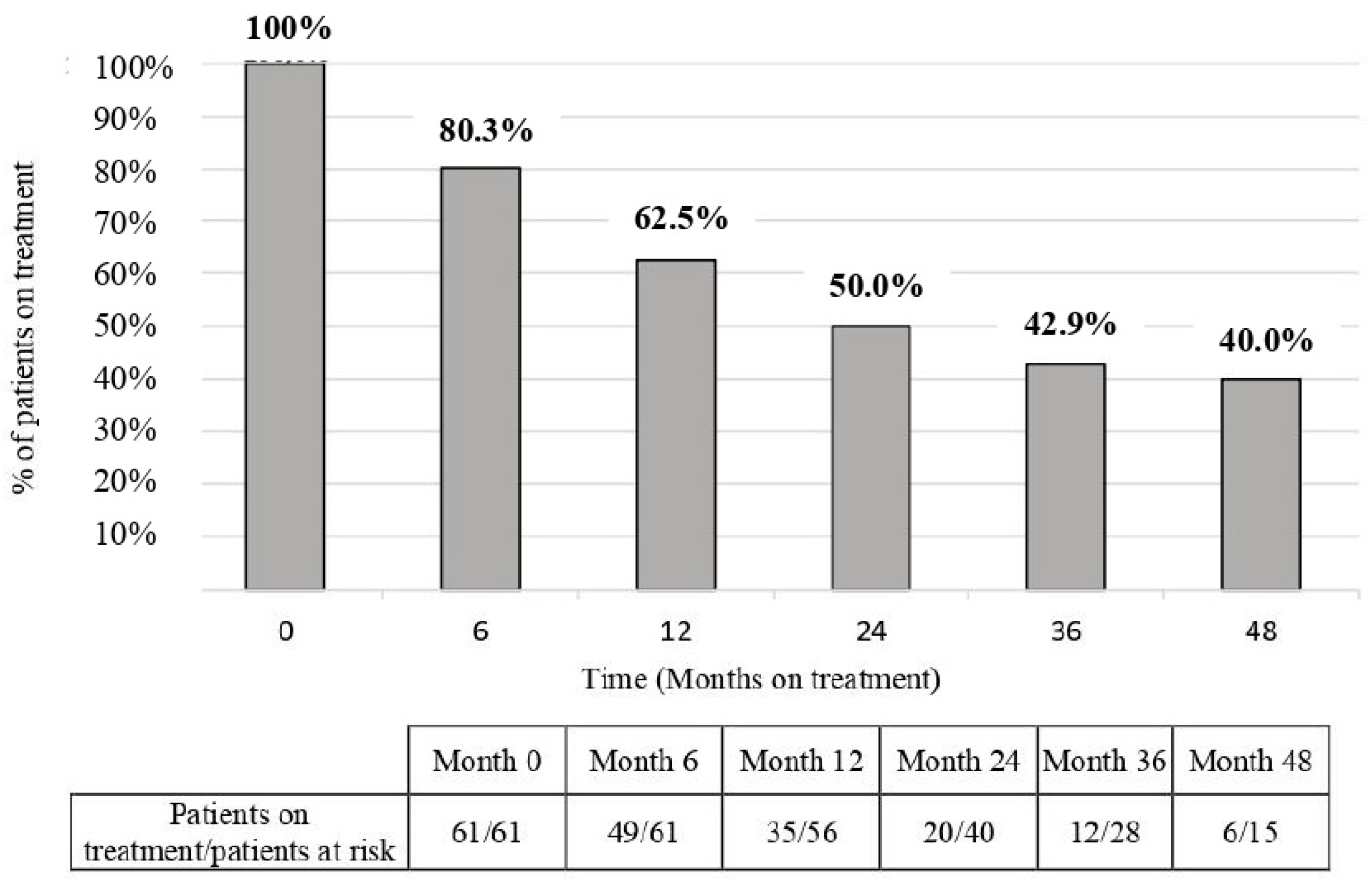
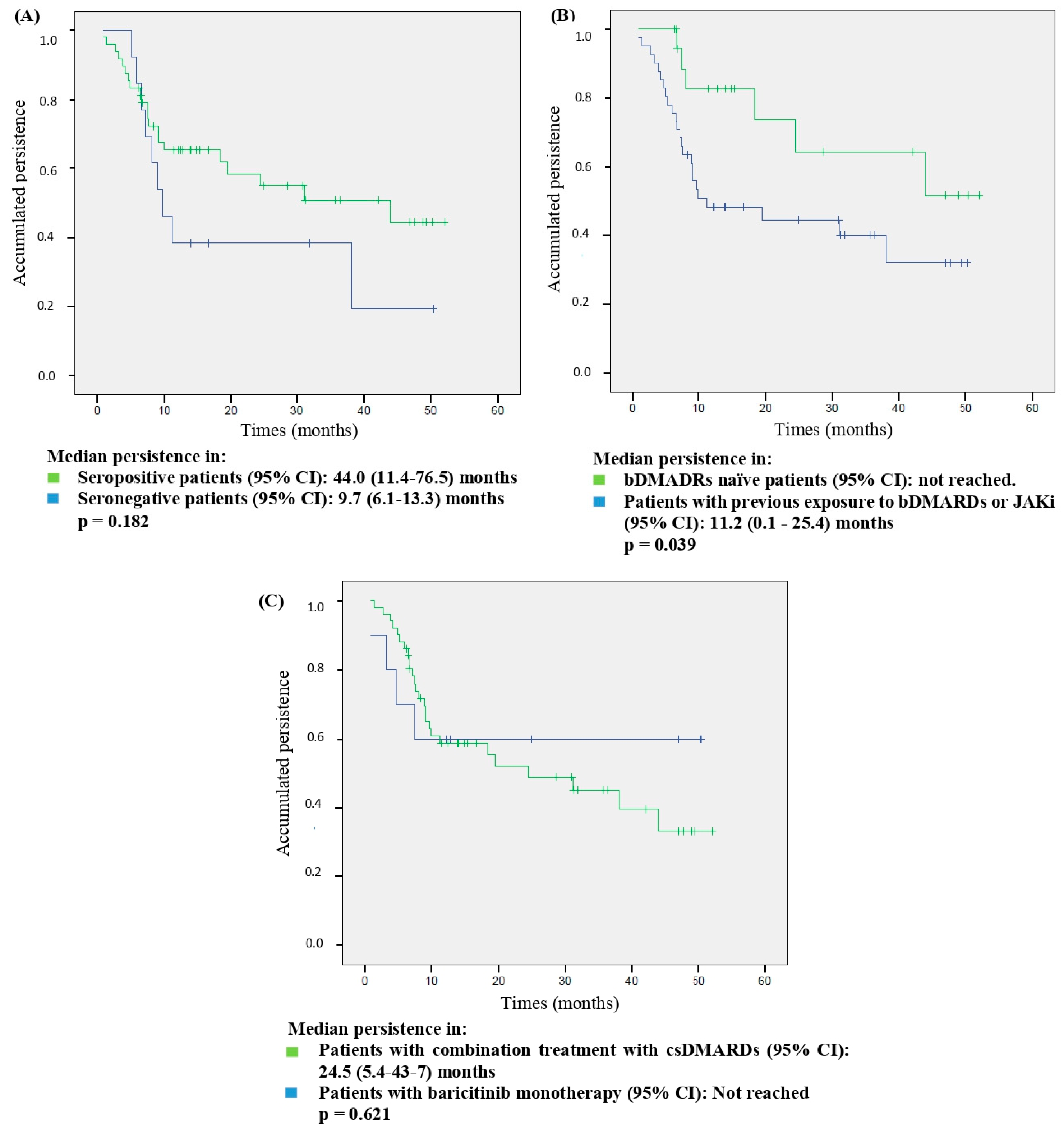
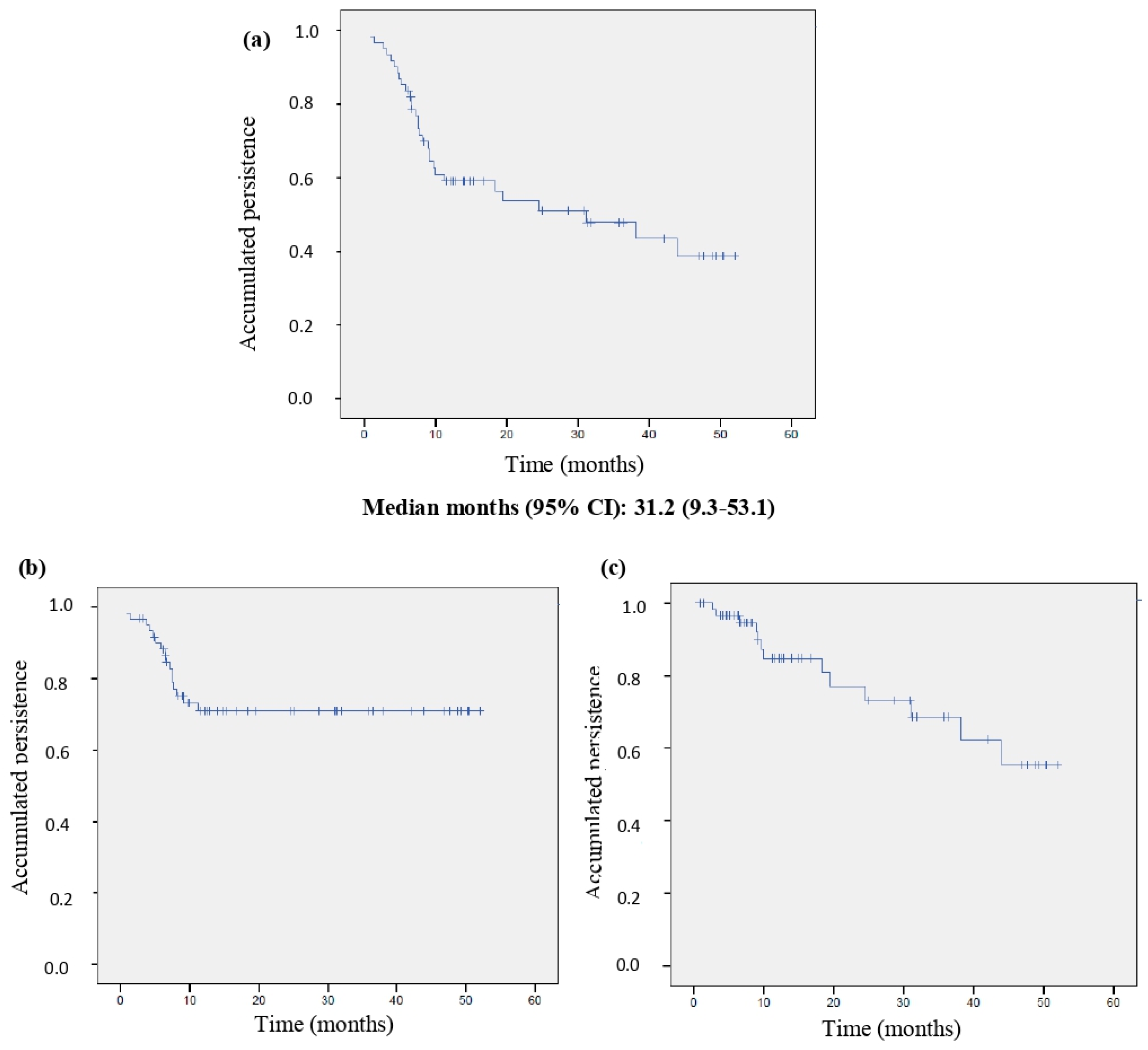
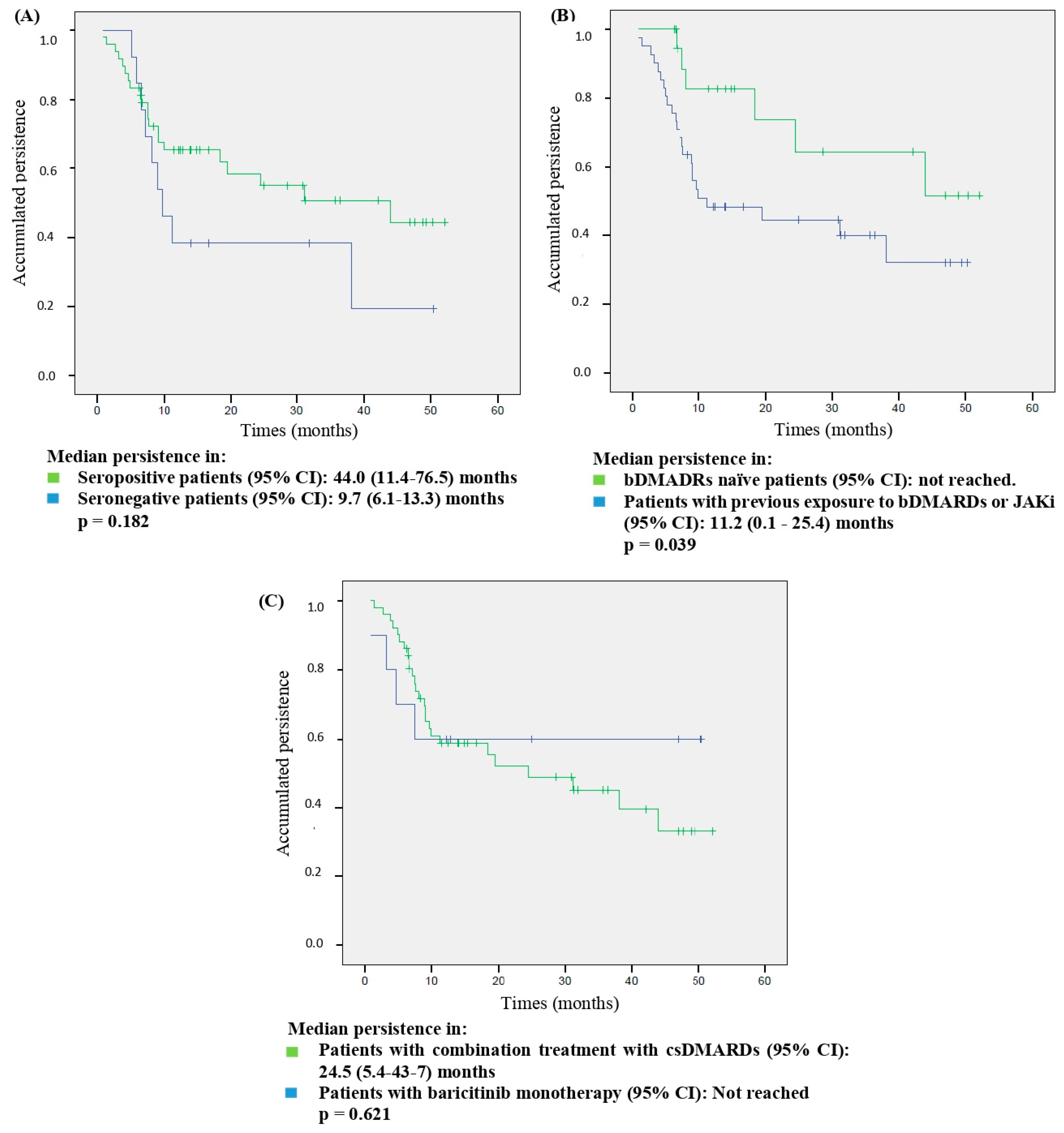
3.3. Persistence
3.4. Adherence
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aletaha, D.; Smolen, J. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Firestein, G.; McInnes, I.B. Immunopathogenesis of rheumatoid arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewé, R.B.M.; Bergstra, S.A.; Kerschbaumer, A.; Sepriano, A.; Aletaha, D.; Caporali, R.; Edwards, C.J.; Hyrich, K.L.; Pope, J.E.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann. Rheum. Dis. 2023, 82, 3–18. [Google Scholar] [CrossRef]
- Taylor, P.C.; Laedermann, C.; Alten, R.; Feist, E.; Choy, E.; Haladyj, E.; De La Torre, I.; Richette, P.; Finckh, A.; Tanaka, Y. A JAK Inhibitor for Treatment of Rheumatoid Arthritis: The Baricitinib Experience. J. Clin. Med. 2023, 12, 4527. [Google Scholar] [CrossRef]
- Fleischmann, R.; Schiff, M.; van der Heijde, D.; Ramos-Remus, C.; Spindler, A.; Stanislav, M.; Zerbini, C.A.; Gurbuz, S.; Dickson, C.; de Bono, S.; et al. Baricitinib, Methotrexate, or Combination in Patients with RA and No or Limited Prior DMARDs Treatment. Arthritis Rheumatol. 2017, 69, 506–517. [Google Scholar] [CrossRef]
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich, C.; et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2017, 76, 88–95. [Google Scholar] [CrossRef]
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in Patients with Refractory Rheumatoid Arthritis. N. Engl. J. Med. 2016, 374, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Ytterberg, S.R.; Bhatt, D.L.; Mikuls, T.R.; Koch, G.G.; Fleischmann, R.; Rivas, J.L.; Germino, R.; Menon, S.; Sun, Y.; Wang, C.; et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N. Engl. J. Med. 2022, 386, 316–326. [Google Scholar] [CrossRef]
- Taylor, P.C.; Bieber, T.; Alten, R.; Witte, T.; Galloway, J.; Deberdt, W.; Issa, M.; Haladyj, E.; De La Torre, I.; Grond, S.; et al. Baricitinib Safety for Events of Special Interest in Populations at Risk: Analysis from Randomised Trial Data Across Rheumatologic and Dermatologic Indications. Adv. Ther. 2023, 40, 1867–1883. [Google Scholar] [CrossRef]
- Sabaté, E. Adherence to Long-Term Therapies: Evidence for Action. 2003. Available online: http://www.who.int/chronic_conditions/adherencereport/en/ (accessed on 15 July 2023).
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Europen Medicine Agency. EMA Confirms Measures to Minimise Risk of Serious Side Effects with Janus Kinase Inhibitors for Chronic Inflammatory Disorders. Available online: https://www.ema.europa.eu/en/medicines/human/referrals/janus-kinase-inhibitors-jaki (accessed on 6 March 2023).
- Fransen, J.; van Riel, P.L. The Disease Activity Score and the EULAR response criteria. Rheum. Dis. Clin. N. Am. 2009, 35, 745–757. [Google Scholar] [CrossRef]
- Aletaha, D.; Landewe, R.; Karonitsch, T.; Bathon, J.; Boers, M.; Bombardier, C.; Bombardieri, S.; Choi, H.; Combe, B.; Dougados, M.; et al. Reporting disease activity in clinical trials of patients with rheumatoid arthritis: EULAR/ACR collaborative recommendations. Ann. Rheum. Dis. 2008, 67, 1360–1364. [Google Scholar] [CrossRef]
- Raebel, M.A.; Schmittdiel, J.; Karter, A.J.; Konieczny, J.L.; Steiner, J.F. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med. Care 2013, 51, S11–S21. [Google Scholar] [CrossRef]
- Martínez-López de Castro, N.; Álvarez-Payero, M.; Samartín-Ucha, M.; Martín-Vila, A.; Piñeiro-Corrales, G.; Pego Reigosa, J.M.; Rodríguez-Rodríguez, M.; Melero-González, R.B.; Maceiras-Pan, F.J. Adherence to biological therapies in patients with chronic inflammatory arthropathies. Farm. Hosp. 2019, 43, 134–139. [Google Scholar] [CrossRef]
- de Klerk, E.; van der Heijde, D.; Landewé, R.; van der Tempel, H.; van der Linden, S. The compliance-questionnaire-rheumatology compared with electronic medication event monitoring: A validation study. J. Rheumatol. 2003, 30, 2469–2475. [Google Scholar]
- Hughes, L.D.; Done, J.; Young, A. A 5 item version of the Compliance Questionnaire for Rheumatology (CQR5) successfully identifies low adherence to DMARDs. BMC Musculoskelet Disord. 2013, 14, 286. [Google Scholar] [CrossRef]
- Fernández-Avila, D.G.; Accini, M.; Tobón, M.; Moreno, S.; Rodriguez, V.; Matín Gutierrez, J. Validación y calibración al español del cuestionario CQR para la medición de adherencia a la terapia antirreumática en un grupo de pacientes colombianos con artritis reumatoide. Clin. Exp. Rheumatol. 2019, 26, 105–110. [Google Scholar] [CrossRef]
- Agencia Española de Medicamentos y Productos Sanitarios. Ficha Técnica Olumiant (Baricitinib). Available online: https://cima.aemps.es/cima/pdfs/ft/1161170010/FT_1161170010.pdf (accessed on 15 July 2022).
- United Stated Deparment of Health and Human Service. Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 15 July 2022).
- US Food and Drug Administration. FDA Requires Warnings about Increased Risk of Serious Heart-Related Events, Cancer, Blood Clots, and Death for JAK Inhibitors That Treat Certain Chronic Inflammatory Conditions. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requires-warnings-about-increased-risk-serious-heart-related-events-cancer-blood-clots-and-death (accessed on 6 March 2023).
- Kearsley-Fleet, L.; Davies, R.; De Cock, D.; Watson, K.D.; Lunt, M.; Buch, M.H.; Isaacs, J.D.; Hyrich, K.L. Biologic refractory disease in rheumatoid arthritis: Results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann. Rheum. Dis. 2018, 77, 1405–1412. [Google Scholar] [CrossRef]
- Hernández-Cruz, B.; Kiltz, U.; Avouac, J.; Treuer, T.; Haladyj, E.; Gerwien, J.; Gupta, C.D.; Conti, F. Evidence on Baricitinib for the Treatment of Rheumatoid Arthritis. Rheumatol. Ther. 2023, 10, 1417–1457. [Google Scholar] [CrossRef]
- Smolen, J.S.; Xie, L.; Jia, B.; Taylor, P.C.; Burmester, G.; Tanaka, Y.; Elias, A.; Cardoso, A.; Ortmann, R.; Walls, C.; et al. Efficacy of baricitinib in patients with moderate-to-severe rheumatoid arthritis with 3 years of treatment: Results from a long-term study. Rheumatology 2021, 60, 2256–2266. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Asai, S.; Kobayakawa, T.; Kaneko, A.; Watanabe, T.; Kato, T.; Nishiume, T.; Ishikawa, H.; Yoshioka, Y.; Kanayama, Y.; et al. Predictors for clinical effectiveness of baricitinib in rheumatoid arthritis patients in routine clinical practice: Data from a Japanese multicenter registry. Sci. Rep. 2020, 10, 21907. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, N.; Sato, S.; Kurushima, S.; Michitsuji, T.; Nishihata, S.; Okamoto, M.; Tsuji, Y.; Endo, Y.; Shimizu, T.; Sumiyoshi, R.; et al. Real-world comparative effectiveness and safety of tofacitinib and baricitinib in patients with rheumatoid arthritis. Arthritis Res. Ther. 2021, 23, 197. [Google Scholar] [CrossRef] [PubMed]
- Fitton, J.; Melville, A.R.; Emery, P.; Nam, J.L.; Buch, M.H. Real-world single centre use of JAK inhibitors across the rheumatoid arthritis pathway. Rheumatology 2021, 60, 4048–4054. [Google Scholar] [CrossRef] [PubMed]
- Barbulescu, A.; Askling, J.; Chatzidionysiou, K.; Forsblad-d’Elia, H.; Kastbom, A.; Lindström, U.; Turesson, C.; Frisell, T. Effectiveness of baricitinib and tofacitinib compared with bDMARDs in RA: Results from a cohort study using nationwide Swedish register data. Rheumatology 2022, 61, 3952–3962. [Google Scholar] [CrossRef]
- Hernández-Cruz, B.; Rosas, J.; Díaz-Torné, C.; Belzunegui, J.; García-Vicuña, R.; Inciarte-Mundo, J.; Pons, A.; Millán, A.M.; Jeria-Navarro, S.; Valero, J.A.; et al. Real-World Treatment Patterns and Clinical Outcomes of Baricitinib in Rheumatoid Arthritis Patients in Spain: Results of a Multicenter, Observational Study iRoutine Clinical Practice (The ORBIT-RA Study). Rheumatol. Ther. 2022, 9, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, F.R.; Ceccarelli, F.; Garufi, C.; Duca, I.; Mancuso, S.; Cipriano, E.; Dell’Unto, E.; Alessandri, C.; Di Franco, M.; Perricone, C.; et al. Effectiveness and safety of baricitinib in rheumatoid arthritis: A monocentric, longitudinal, real-life experience. Clin. Exp. Rheumatol. 2021, 39, 525–531. [Google Scholar] [CrossRef]
- González-Freire, L.; Giménez-Candela, R.M.; Castro-Luaces, S.; Veiga-Villaverde, A.B.; Crespo-Diz, C. Baricitinib and tofacitinib in patients with rheumatoid arthritis: Results of regular clinical practice. Farm. Hosp. 2021, 45, 165–169. [Google Scholar]
- González Mazarío, R.; Fragío Gil, J.J.; Ivorra Cortés, J.; Grau García, E.; Cañada Martínez, A.J.; González Puig, L.; Negueroles Albuixech, R.M.; Román Ivorra, J.A. Efectividad y seguridad en el mundo real de los inhibidores de JAK en la artritis reumatoide: Estudio unicéntrico. Reumatol. Clin. 2022, 18, 523–530. [Google Scholar] [CrossRef]
- Takagi, M.; Atsumi, T.; Matsuno, H.; Tamura, N.; Fujii, T.; Okamoto, N.; Takahashi, N.; Nakajima, A.; Nakajima, A.; Tsujimoto, N.; et al. Safety and Effectiveness of Baricitinib for Rheumatoid Arthritis in Japanese Clinical Practice: 24-Week Results of All-Case Post-Marketing Surveillance. Mod. Rheumatol. 2023, 4, 647–656. [Google Scholar] [CrossRef]
- Alten, R.; Burmester, G.R.; Matucci-Cerinic, M.; Salmon, J.H.; Lopez-Romero, P.; Fakhouri, W.; de la Torre, I.; Zaremba-Pechmann, L.; Holzkämper, T.; Fautrel, B. The RA-BE-REAL Multinational, Prospective, Observational Study in Patients with Rheumatoid Arthritis Receiving Baricitinib, Targeted Synthetic, or Biologic Disease-Modifying Therapies: A 6-Month Interim Analysis. Rheumatol. Ther. 2023, 10, 73–93. [Google Scholar] [CrossRef]
- Guidelli, G.M.; Viapiana, O.; Luciano, N.; De Santis, M.; Boffini, N.; Quartuccio, L.; Birra, D.; Conticini, E.; Chimenti, M.S.; Bazzani, C.; et al. Efficacy and safety of baricitinib in 446 patients with rheumatoid arthritis: A real-life multicentre study. Clin. Exp. Rheumatol. 2021, 39, 868–873. [Google Scholar] [CrossRef]
- Deprez, V.; Le Monnier, L.; Sobhy-Danial, J.M.; Grados, F.; Henry-Desailly, I.; Salomon-Goëb, S.; Rabin, T.; Ristic, S.; Fumery, M.; Fardellone, P.; et al. Therapeutic Maintenance of Baricitinib and Tofacitinib in Real Life. J. Clin. Med. 2020, 9, 3319. [Google Scholar] [CrossRef]
- Scheepers, L.; Yang, Y.; Chen, Y.L.; Jones, G. Persistence of Janus-kinase (JAK) inhibitors in rheumatoid arthritis: Australia wide study. Semin. Arthritis Rheum. 2024, 64, 152314. [Google Scholar] [CrossRef]
- Rosas, J.; Senabre-Gallego, J.M.; Santos-Soler, G.; Antonio Bernal, J.; Pons Bas, A. Efficacy and Safety of Baricitinib in Patients with Rheumatoid Arthritis and Inadequate Response to Conventional Synthetic DMARDs and/or Biological DMARDs: Data from a Local Registry. Reumatol. Clin. 2022, 18, 188–189. [Google Scholar] [CrossRef]
- Retuerto, M.; Trujillo, E.; Valero, C.; Fernandez-Espartero, C.; Soleto, C.Y.; Garcia-Valle, A.; Aurrecoechea, E.; Garijo, M.; Lopez, A.; Loricera, J.; et al. Efficacy and safety of switching Jak inhibitors in rheumatoid arthritis: An observational study. Clin. Exp. Rheumatol. 2021, 39, 453–455. [Google Scholar] [CrossRef]
- Ebina, K.; Hirano, T.; Maeda, Y.; Yamamoto, W.; Hashimoto, M.; Murata, K.; Onishi, A.; Jinno, S.; Hara, R.; Son, Y.; et al. Drug retention of sarilumab, baricitinib, and tofacitinib in patients with rheumatoid arthritis: The ANSWER cohort study. Clin. Rheumatol. 2021, 40, 2673–2680. [Google Scholar] [CrossRef]
- Baldi, C.; Berlengiero, V.; Falsetti, P.; Cartocci, A.; Conticini, E.; D’Alessandro, R.; D’Ignazio, E.; Bardelli, M.; Fabbroni, M.; Cantarini, L.; et al. Baricitinib retention rate: ‘real-life’ data from a mono-centric cohort of patients affected by rheumatoid arthritis. Front. Med. 2023, 10, 1176613. [Google Scholar] [CrossRef]
- Parisi, S.; Andrea, B.; Chiara, D.M.; Alberto, L.G.; Maddalena, L.; Palma, S.; Olga, A.; Massimo, R.; Marino, P.; Rosalba, C.; et al. Analysis of survival rate and persistence predictors of baricitinib in real-world data from a large cohort of rheumatoid arthritis patients. Curr. Res. Pharmacol. Drug Discov. 2024, 6, 100178. [Google Scholar] [CrossRef]
- Martinez-Molina, C.; Gich, I.; Diaz-Torné, C.; Park, H.S.; Feliu, A.; Vidal, S.; Corominas, H. Patient-related factors influencing the effectiveness and safety of Janus Kinase inhibitors in rheumatoid arthritis: A real-world study. Sci. Rep. 2024, 14, 172. [Google Scholar] [CrossRef]
- Bergman, M.; Chen, N.; Thielen, R.; Zueger, P. One-Year Medication Adherence and Persistence in Rheumatoid Arthritis in Clinical Practice: A Retrospective Analysis of Upadacitinib, Adalimumab, Baricitinib, and Tofacitinib. Adv. Ther. 2023, 40, 4493–4503. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Monteagudo, I.; Salvador, G.; de Toro, F.J.; Escudero, A.; Alegre-Sancho, J.J.; Raya, E.; Ortiz, A.; Carmona, L.; Mestre, Y.; et al. Identification of patients at risk of non-adherence to oral antirheumatic drugs in rheumatoid arthritis using the Compliance Questionnaire in Rheumatology: An ARCO sub-study. Rheumatol. Int. 2017, 37, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Codes-Mendez, H.; Martinez-Molina, C.; Masip, M.; Riera, P.; Pagès Puigdemont, N.; Riera Magallón, A.; Lobo Prat, D.; Sainz Comas, L.; Corominas, H.; Díaz-Torné, C. Therapeutic adherence and persistence of tofacitinib and baricitinib in rheumatoid arthritis patients in daily clinical practice. Ann. Rheum. Dis. 2022, 81, 1330. [Google Scholar] [CrossRef]
- Peng, L.; Xiao, K.; Ottaviani, S.; Stebbing, J.; Wang, Y.J. A real-world disproportionality analysis of FDA Adverse Event Reporting System (FAERS) events for baricitinib. Expert. Opin. Drug Saf. 2020, 19, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Takeuchi, T.; Burmester, G.R.; Durez, P.; Smolen, J.S.; Deberdt, W.; Issa, M.; Terres, J.R.; Bello, N.; Winthrop, K.L. Safety of baricitinib for the treatment of rheumatoid arthritis over a median of 4.6 and up to 9.3 years of treatment: Final results from long-term extension study and integrated database. Ann. Rheum. Dis. 2022, 81, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Ahn, S.M.; Kim, Y.G.; Lee, C.K.; Yoo, B.; Hong, S. Safety of JAK inhibitor use in patients with rheumatoid arthritis who developed herpes zoster after receiving JAK inhibitors. Clin. Rheumatol. 2022, 41, 1659–1663. [Google Scholar] [CrossRef] [PubMed]
- Frisell, T.; Bower, H.; Morin, M.; Baecklund, E.; Di Giuseppe, D.; Delcoigne, B.; Feltelius, N.; Forsblad-d’Elia, H.; Lindqvist, E.; Lindström, U.; et al. Safety of biological and targeted synthetic disease-modifying antirheumatic drugs for rheumatoid arthritis as used in clinical practice: Results from the ARTIS programme. Ann. Rheum. Dis. 2023, 82, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Uchida, T.; Iwamoto, N.; Fukui, S.; Morimoto, S.; Aramaki, T.; Shomura, F.; Aratake, K.; Eguchi, K.; Ueki, Y.; Kawakami, A. Comparison of risks of cancer, infection, and MACEs associated with JAK inhibitor and TNF inhibitor treatment: A multicenter cohort study. Rheumatology 2023, 62, 3358–3365. [Google Scholar] [CrossRef] [PubMed]
- Waldman, R.A.; Sharp, K.L.; Adalsteinsson, J.A.; Grant-Kels, J.M. Herpes zoster subunit vaccine for patients initiating a Janus kinase inhibitor. J. Am. Acad. Dermatol. 2022, 88, 697–698. [Google Scholar] [CrossRef]
- Salinas, C.A.; Louder, A.; Polinski, J.; Zhang, T.C.; Bower, H.; Phillips, S.; Song, Y.; Rashidi, E.; Bosan, R.; Chang, H.C.; et al. Evaluation of VTE, MACE, and Serious Infections among Patients with RA Treated with Baricitinib Compared to TNFi: A Multi-Database Study of Patients in Routine Care Using Disease Registries and Claims Databases. Rheumatol. Ther. 2023, 10, 201–223. [Google Scholar] [CrossRef]
- Gouverneur, A.; Avouac, J.; Prati, C.; Cracowski, J.L.; Schaeverbeke, T.; Pariente, A.; Truchetet, M.E. JAK inhibitors and risk of major cardiovascular events or venous thromboembolism: A self-controlled case series study. Eur. J. Clin. Pharmacol. 2022, 78, 1981–1990. [Google Scholar] [CrossRef] [PubMed]
- Hoisnard, L.; Pina Vegas, L.; Dray-Spira, R.; Weill, A.; Zureik, M.; Sbidian, E. Risk of major adverse cardiovascular and venous thromboembolism events in patients with rheumatoid arthritis exposed to JAK inhibitors versus adalimumab: A nationwide cohort study. Ann. Rheum. Dis. 2023, 82, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Xue, X.; Shannon, J. Characteristics of adverse event reporting of Xeljanz/Xeljanz XR, Olumiant, and Rinvoq to the US Food and Drug Administration. J. Manag. Care Spec. Pharm. 2022, 28, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Kiely, P.D. Biologic efficacy optimization—A step towards personalized medicine. Rheumatology 2016, 55, 780–788. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender (n, % female) | 51 (83.6) |
| Age at initiation of BAR (years, mean, SD) | 58.1 (15.4) |
| Disease duration (years, mean, SD) | 13.9 (8.3) |
| RF positive (n, %) | 47 (77.0) |
| ACPAs positive (n, %) | 43 (70.5) |
| Erosive disease (n, %) | 34 (55.7) |
| Extra-articular disease (n, %) | 26 (42.6) |
| Rheumatic nodules | 10 (16.4) |
| Sjögren syndrome | 7 (11.5) |
| Interstitial pneumonitis | 4 (6.6) |
| Neuropathies | 2 (3.3) |
| Peripheral ulcerative keratitis | 1 (1.6) |
| Raynaud syndrome | 1 (1.6) |
| Felty syndrome | 1 (1.6) |
| Glucocorticoid treatment (n, %) | 30 (49.1) |
| Naïve to bDMARDs or JAKi treatment (n, %) | 20 (32.8) |
| Previous exposure to bDMARDs or JAKi (n, %) | 41 (67.2) |
| Number or previous bDMARDs | |
| One previous bDMARD | 6 (9.8) |
| Two previous bDMARDs | 14 (23.0) |
| Three previous bDMARDs | 8 (13.1) |
| Four previous bDMARDs | 7 (11.5) |
| Five previous bDMARDs | 2 (3.3) |
| Six previous bDMARDs | 2 (3.3) |
| Seven previous bDMARDs | 1 (1.6) |
| Eight previous bDMARD | 1 (1.6) |
| Type of previous bDMARDs | |
| TNFi | 41 (67.2) |
| IL-6Ri | 18 (29.1) |
| CTLA4-Ig | 19 (31.1) |
| Anti-CD20 B cell depletion | 21 (34.4) |
| Previous exposure to one JAKi (tofacitinib) (n, %) | 7 (11.5) |
| BAR monotherapy (n, %) | 10 (16.4) |
| BAR in combination with csDMARDs | 51 (83.6) |
| Methotrexate | 31 (50.8) |
| Leflunomide | 14 (23.0) |
| Hydroxychloroquine | 3 (4.9) |
| Sulfasalazine | 2 (3.3) |
| Methotrexate plus leflunomide | 1 (1.6) |
| Baseline DAS28CRP (mean, SD) | 3.9 (0.9) |
| Baseline ESR (mml/h, mean, SD) | 27.8 (23.2) |
| Baseline CRP (mg/dL, mean, SD) | 2.0 (4.8) |
| Baseline | Final | p | |
|---|---|---|---|
| DAS28CRP (average, SD) | 3.9 (0.9) | 2.7 (1.3) | 0.000 |
| CRP (mg/dL, average, SD) | 2.0 (4.8) | 1.1 (1.7) | 0.105 |
| ESR (mml/h, average, SD) | 29.0 (23,2) | 25.7 (22.9) | 0.604 |
| Lymphocyte count (cells/mm3, mean, SD) | 2641 (1501) | 2482.6 (1505) | 0.154 |
| Neutrophil count (cells/mm3, mean, SD) | 4198 (2126) | 4157 (2132) | 0.865 |
| Hemoglobin (g/dL, mean, SD) | 13.5 (1.5) | 12.9 (1.4) | 0.000 |
| IP (n, %) | IR per 100 PY (95% CI) | |
|---|---|---|
| Patients with any AE (Total AEs = 104) | 40/61 (65.6) | 15.2 (15.1–15.3) |
| Anemia | 24/61 (39.3) | 9.1 (9.0–9.2) |
| Any infection | 22/61 (36.1) | 8.4 (8.2–8.6) |
| Herpes Zoster | 7/61 (11.5) | 2.7 (2.4–3.0) |
| URTI | 7/61 (11.5) | 2.7 (2.4–3.0) |
| Skin and soft tissue infection | 5/61 (8.2) | 1.9 (1.7–2.1) |
| Bacterial pneumonia | 3/61 (4.9) | 1.1 (0.8–1.4) |
| Influenza A | 2/61 (3.3) | 0.8 (0.6–1.0) |
| Oral herpes simple | 2/61 (3.3) | 0.8 (0.6–1.0) |
| Hypercholesterolemia | 20/61 (32.8) | 7.6 (7.4–7.8) |
| Abnormal liver enzymes (ALT or AST) | 19/61 (31.1) | 7.2 (6.9–7.5) |
| Nausea and vomiting | 4/61 (6.6) | 1.5 (1.3–1.7) |
| Cancer | 3/61 (4.9) | 1.1 (0.8–1.4) |
| Alopecia | 2/61 (3.3) | 0.8 (0.6–1.0) |
| Skin disorders | 2/61 (3.3) | 0.8 (0.6–1.0) |
| Asthenia | 2/61 (3.3) | 0.8 (0.6–1.0) |
| Weight gain | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Venous thrombotic event | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Hypertriglyceridemia | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Rhabdomyolysis | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Platelet increase | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Patients with SAEs (Grade 3–4) (Total SAEs = 11) | 9/61 (14.8) | 3.5 (3.3–3.7) |
| Bacterial pneumonia with intravenous treatment | 3/61 (4.9) | 1.1 (0.8–1.4) |
| Cancer | 3/61 (4.9) | 1.1 (0.8–1.4) |
| Abnormal liver enzymes (ALT or AST) | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Venous thrombotic event | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Hypertriglyceridemia | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Skin disorders (Urticaria) | 1/61 (1.6) | 0.4 (0.2–0.6) |
| Platelet increase | 1/61 (1.6) | 0.4 (0.2–0.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo-Garcia, A.; Ramírez Herráiz, E.; Llorente Cubas, I.M.; Varas De Dios, B.; Benedí González, J.; Morell Baladrón, A.; García-Vicuña, R. The Real-World Effectiveness, Persistence, Adherence, and Safety of Janus Kinase Inhibitor Baricitinib in Rheumatoid Arthritis: A Long-Term Study. J. Clin. Med. 2024, 13, 2517. https://doi.org/10.3390/jcm13092517
Calvo-Garcia A, Ramírez Herráiz E, Llorente Cubas IM, Varas De Dios B, Benedí González J, Morell Baladrón A, García-Vicuña R. The Real-World Effectiveness, Persistence, Adherence, and Safety of Janus Kinase Inhibitor Baricitinib in Rheumatoid Arthritis: A Long-Term Study. Journal of Clinical Medicine. 2024; 13(9):2517. https://doi.org/10.3390/jcm13092517
Chicago/Turabian StyleCalvo-Garcia, Alberto, Esther Ramírez Herráiz, Irene María Llorente Cubas, Blanca Varas De Dios, Juana Benedí González, Alberto Morell Baladrón, and Rosario García-Vicuña. 2024. "The Real-World Effectiveness, Persistence, Adherence, and Safety of Janus Kinase Inhibitor Baricitinib in Rheumatoid Arthritis: A Long-Term Study" Journal of Clinical Medicine 13, no. 9: 2517. https://doi.org/10.3390/jcm13092517
APA StyleCalvo-Garcia, A., Ramírez Herráiz, E., Llorente Cubas, I. M., Varas De Dios, B., Benedí González, J., Morell Baladrón, A., & García-Vicuña, R. (2024). The Real-World Effectiveness, Persistence, Adherence, and Safety of Janus Kinase Inhibitor Baricitinib in Rheumatoid Arthritis: A Long-Term Study. Journal of Clinical Medicine, 13(9), 2517. https://doi.org/10.3390/jcm13092517