

Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development
 , , ,
, , ,
Abstract
1. Introduction
2. Reports of Hypernatremia in Hyperglycemia
3. Reports of Hyperglycemic Syndromes with Mean [Na]S in the Hypernatremic Range
4. Studies Assessing Risks Created by Hypernatremia in Hyperglycemic Syndromes
5. Case Reports of Hypernatremia in Hyperglycemic Syndromes
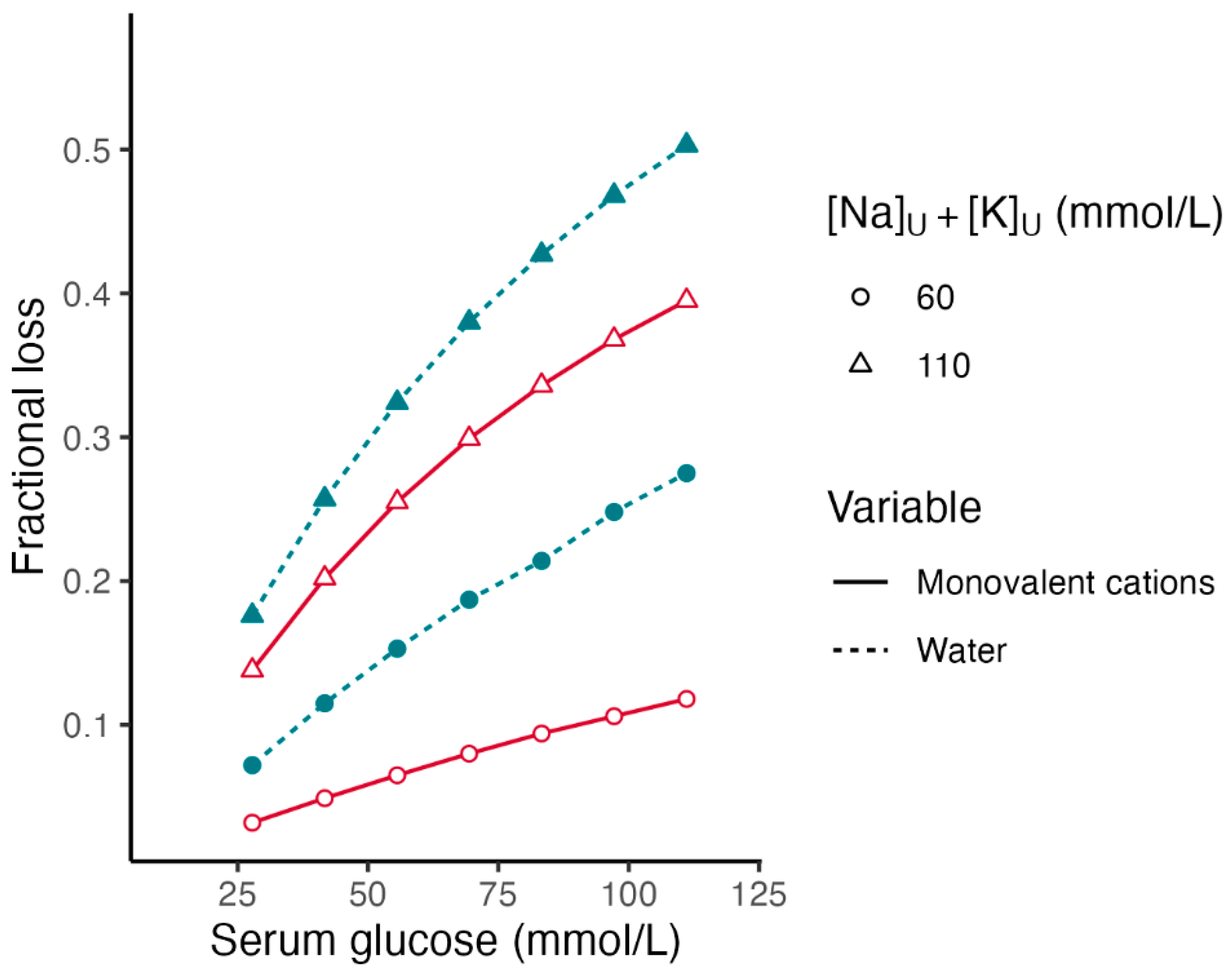
6. Fractional Losses of Body Water and Monovalent Cations in Hyperglycemia
7. Limitations of the Method for Calculating Fractional Losses
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seldin, D.W.; Tarail, R. Effects of hypertonic solutions on metabolism and excretion of electrolytes. Am. J. Physiol. 1949, 159, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, E.; Guidetti, F.; Bergamasco, L. Estimating excess glucose, sodium and water deficits in non-ketotic hyperglycaemia. Nephrol. Dial. Transplant. 2007, 22, 3478–3486. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Khitan, Z.J.; Glew, R.H.; Roumelioti, M.E.; Rondon-Berrios, H.; Elisaf, M.S.; Raj, D.S.; Owen, J.; Sun, Y.; Siamopoulos, K.C.; et al. Serum sodium concentration and tonicity in hyperglycemic crises: Major influences and treatment implications. J. Am. Heart Assoc. 2019, 8, e011786. [Google Scholar] [CrossRef] [PubMed]
- Gennari, F.J.; Kassirer, J.P. Osmotic diuresis. N. Engl. J. Med. 1974, 291, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Roumelioti, M.E.; Ing, T.S.; Rondon-Berrios, H.; Glew, R.H.; Khitan, Z.J.; Sun, Y.; Malhotra, D.; Raj, D.S.; Agaba, E.I.; Murata, G.H.; et al. Principles of quantitative water and electrolyte replacement of losses from osmotic diuresis. Int. Urol. Nephrol. 2018, 50, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Ing, T.S.; Ganda, K.; Bhave, G.; Lew, S.Q.; Agaba, E.I.; Argyropoulos, C.; Tzamaloukas, A.H. The corrected serum sodium concentration in hyperglycemic crises: Computation and clinical applications. Front. Med. 2020, 7, 477. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Levinstone, A.R.; Gardner, K.D., Jr. Hyperglycemia in advanced renal failure: Sodium and water metabolism. Nephron 1982, 31, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Chiasson, J.L.; Aris-Jilwan, N.; Bélanger, R.; Bertrand, S.; Beauregard, H.; Ekoé, J.M.; Fournier, H.; Havrankova, J. Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state. CMAJ 2003, 168, 859–866. [Google Scholar] [PubMed]
- Milionis, H.J.; Elisaf, M.S. Therapeutic management of hyperglycaemic hyperosmolar syndrome. Expert Opin. Pharmacother. 2005, 6, 1841–1849. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Umpierrez, G.E.; Murphy, M.B.; Kreisberg, R.A. Hyperglycemic crises in adult patients with diabetes: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 2739–2748. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Nyenwe, E.A.; Kitabchi, A.E. Evidence-based management of hyperglycemic emergencies in diabetes mellitus. Diabetes Res. Clin. Pract. 2011, 94, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Sherani, K.; Surani, S.; Vakil, A. Guidelines and controversies in the management of diabetic ketoacidosis. World J. Diabetes 2018, 9, 226–229. [Google Scholar] [CrossRef]
- Long, B.; Willis, G.C.; Lentz, S.; Koyfman, A.; Gottlieb, M. Diagnosis and management of the critically ill adult patient with hyperglycemic hyperosmolar state. J. Emerg. Med. 2021, 61, 365–375. [Google Scholar] [CrossRef]
- Glaser, N.; Fritsch, M.; Priyambada, L.; Rewers, A.; Cherubini, V.; Estrada, S.; Wolfsdorf, J.I.; Codner, E. ISPAD clinical practice consensus guidelines 2022: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr. Diabetes 2022, 23, 835–856. [Google Scholar] [CrossRef]
- Hassan, E.M.; Mushtag, H.; Mahmoud, E.E.; Chhibber, S.; Saleem, S.; Issa, A.; Nitesh, J.; Jama, A.B.; Khedr, A.; Boike, S.; et al. Overlap of diabetic ketoacidosis and hyperosmolar hyperglycemic state. World J. Clin. Cases 2022, 10, 11702–11711. [Google Scholar] [CrossRef]
- Mustafa, O.G.; Haq, M.; Dashora, U.; Castro, E.; Dhatariya, K.K.; Joint British Diabetes Societies (JBDS) for Inpatient care Group. Management of hyperosmolar hyperglycaemic state (HHS) in adults: An updated guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care Group. Diabet. Med. 2023, 40, e15005. [Google Scholar] [CrossRef] [PubMed]
- Atchley, D.W.; Loeb, R.F.; Richards, D.W.; Benedict, E.M.; Driscoll, M.E. On diabetic acidosis: A detailed study of electrolyte balances following the withdrawal and reestablishment of insulin therapy. J. Clin. Investig. 1933, 12, 297–326. [Google Scholar] [CrossRef]
- Brodsky, W.A.; Rapoport, S.; West, C.D. The mechanism of glycosuric diuresis in diabetic man. J. Clin. Investig. 1950, 29, 1021–1032. [Google Scholar] [CrossRef] [PubMed]
- Seldin, D.W.; Tarail, R. The metabolism of glucose and electrolytes in diabetic acidosis. J. Clin. Investig. 1950, 29, 552–565. [Google Scholar] [CrossRef]
- Popli, S.; Tzamaloukas, A.H.; Ing, T.S. Osmotic diuresis-induced hypernatremia: Better explained by solute-free water clearance or electrolyte-free water clearance? Int. Urol. Nephrol. 2014, 46, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Pasquel, F.J.; Tsegka, K.; Wang, H.; Cardona, S.; Galindo, R.J.; Fayfman, M.; Davis, G.; Vellanki, P.; Migdal, A.; Gujral, U.; et al. Clinical outcomes in patients with isolated or combined diabetic ketoacidosis and hyperosmolar hyperglycemic state: A retrospective, hospital-based cohort study. Diabetes Care 2020, 43, 349–357. [Google Scholar] [CrossRef] [PubMed]
- McCurdy, D.K. Hyperosmolar hyperglycemic nonketotic diabetic coma. Med. Clin. N. Am. 1970, 54, 689–699. [Google Scholar] [CrossRef]
- Al-Kudsi, R.R.; Daugirdas, J.T.; Ing, T.S.; Kheirbek, A.O.; Popli, S.; Hano, J.E.; Gandhi, V.C. Extreme hyperglycemia in dialysis patients. Clin. Nephrol. 1982, 17, 228–231. [Google Scholar] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrica 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Danowski, T.S.; Nabarro, J.D. Hyperosmolar and other types of nonketoacidotic coma in diabetes. Diabetes 1965, 14, 162–165. [Google Scholar] [CrossRef]
- Halmos, P.B.; Nelson, J.K.; Lowry, R.C. Hyperosmolar non-ketoacidotic coma in diabetes. Lancet 1966, 1, 675–679. [Google Scholar] [CrossRef]
- Piniés, J.A.; Cairo, G.; Gaztambibe, S.; Vasquez, J.A. Course and prognosis of 132 patients with diabetic non ketotic hyperosmolar state. Diabetes Metab. 1994, 20, 43–48. [Google Scholar]
- Fulop, M.; Rosenblatt, A.; Kreitzer, S.M.; Gerstenhaber, B. Hyperosmolar nature of diabetic coma. Diabetes 1975, 24, 594–599. [Google Scholar] [CrossRef]
- Poser, C.M. Hyperglycemic non-ketotic coma. Role of sodium in the pathogenesis of the neurologic manifestations. Dis. Nerv. Syst. 1972, 33, 725–729. [Google Scholar]
- Daugirdas, J.T.; Kronfol, N.O.; Tzamaloukas, A.H.; Ing, T.S. Hyperosmolar coma; cellular dehydration and the serum sodium concentration. Ann. Intern. Med. 1989, 110, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Nyenwe, E.A.; Razavi, L.N.; Kitabchi, A.E.; Khan, A.N.; Wan, J.Y. Acidosis: The prime determinant of depressed sensorium in diabetic ketoacidosis. Diabetes Care 2010, 33, 1837–1839. [Google Scholar] [CrossRef] [PubMed]
- Popli, S.; Sun, Y.; Tang, H.L.; Kjellstrand, C.M.; Tzamaloukas, A.H.; Ing, T.S. Acidosis and coma in adult diabetic maintenance dialysis patients with extreme hyperglycemia. Int. Urol. Nephrol. 2013, 45, 1687–1692. [Google Scholar] [CrossRef] [PubMed]
- Wachtel, T.J.; Silliman, R.A.; Lamberton, P. Prognostic factors in the diabetic hyperosmolar state. J. Am. Geriatr. Soc. 1987, 35, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Singhal, P.C.; Abramovici, M.; Ayer, S.; Desroches, L. Determinants of rhabdomyolysis in the diabetic state. Am. J. Nephrol. 1991, 11, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Lado-Abeal, J.; Lorenzo-Solar, M.; Lago-Lestón, R.; Palos-Paz, F.; Dominguez-Gerpe, L. Hyperglycaemic hyperosmolar nonketotic state as a cause of low gonadotropin levels in postmenopausal diabetic women; a role for severe hypernatraemia. J. Neuroendocrinol. 2007, 19, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Bermick, J.; Dechert, R.E.; Sarkar, S. Does hyperglycemia in hypernatremic preterm infants increase the risk of intraventricular hemorrhage? J. Perinatol. 2016, 36, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.I.; Butterfield, W.J.H. The stress response in the severely burned: An interim report. Ann. Surg. 1951, 134, 588–613. [Google Scholar] [CrossRef]
- De Graeff, J.; Lips, J.B. Hypernatrimia as a complication of diabetes mellitus. Ned. Tijdschr. Geneeskd. 1956, 100, 3623–3632. [Google Scholar]
- De Graeff, J.; Lips, J.B. Hypernatraemia in diabetes mellitus. Acta Med. Scand. 1957, 157, 71–75. [Google Scholar] [CrossRef]
- Zierler, K.L. Hyperosmolarity in adults: A critical review. J. Chronic Dis. 1958, 7, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Arney, G.K.; Pearson, E.; Sutherland, A.B. Burn stress pseudodiabetes. Ann. Surg. 1960, 152, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Rossier, P.H.; Reutter, F.; Frick, P. Hyper-osmolar non-acidotic coma in diabetes mellitus. Dtsch. Med. Wochenschr. 1961, 86, 2145–2148. [Google Scholar] [CrossRef] [PubMed]
- von Rechenberg, H. Hyperosmotic, anacidotic diabetic coma. Schweiz. Med. Wochenschr. 1962, 92, 1415–1416. [Google Scholar] [PubMed]
- Azerad, E.; Lubetzki, J. The comas due to hyperglycemia and hyperosmolarity, without acido-ketosis, in the diabetic. Presse Med. (1893) 1963, 71, 261–264. [Google Scholar] [PubMed]
- Boulet, P.; Barjon, P.; Vallat, G.; Fabre, S.; Jover, A. Hyperglycemia and coma without ketoacidosis in diabetics. Apropos of 4 cases. Diabete 1963, 11, 325–329. [Google Scholar] [PubMed]
- Jarrett, E.; Bacon, G. Hyperosmolarity and diabetic coma. Lancet 1963, 1, 891. [Google Scholar] [CrossRef]
- Lucas, C.P.; Grant, N.; Daily, W.J.; Reaven, G.M. Diabetic coma without ketoacidosis. Lancet 1963, 1, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Mach, R.S.; De Sousa, R.C. Coma with hyperosmolarity and dehydration in hyperglycemic patients without ketoacidosis. Schweiz. Med. Wochenschr. 1963, 93, 1256–1263. [Google Scholar]
- Ward, F.G. Diabetic coma without ketoacidosis. Lancet 1963, 1, 450. [Google Scholar] [CrossRef]
- Behar, A.; Bental, E.; Aviram, A. Central pontine myelinolysis. (A case report). Acta Neuropathol. 1964, 3, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.I. Diabetic coma without ketoacidosis in a patient with acute pancreatitis. Br. Med. J. 1964, 1, 356. [Google Scholar] [CrossRef] [PubMed]
- Dürr, F. A case of hyperosmolar nonacidotic diabetic coma. German Med. Month. 1964, 9, 58–63. [Google Scholar]
- Dibenedetto, R.J.; Crocco, J.A.; Soscia, J.L. Hyperglycemic nonketotic coma. Arch. Intern. Med. 1965, 116, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.A.; Brief, D.K.; Kinney, J.M.; Herrera, M.G.; Wilson, R.E.; Moore, F.D. The syndrome of dehydration, coma, and severe hyperglycemia without ketosis in patients convalescing from burns. N. Engl. J. Med. 1965, 272, 931–938. [Google Scholar] [CrossRef]
- Jackson, W.P.; Forman, R. Hyperosmolar nonketotic diabetic coma. Diabetes 1966, 15, 714–722. [Google Scholar] [CrossRef]
- Boyer, M.H. Hyperosmolar anacidotic coma in association with glucocorticoid therapy. JAMA 1967, 202, 1007–1009. [Google Scholar] [CrossRef]
- Drapkin, A.; Matz, R. Hyperosmolar dehydration and coma in diabetes mellitus. N. Y. State J. Med. 1967, 67, 823–829. [Google Scholar] [PubMed]
- Lestradet, H.; Martineti, J.; Deschamps, I.; Gentil, M.; Coriat, A. Coma with hypernatremia and hyperglycemia without acido-ketosis in children. Ann. Pediatr. 1967, 14, 1420–1426. [Google Scholar]
- Martin, A. Hyperosmolar non-keto-acidotic diabetic coma. A report of three cases and review of the literature. Postgrad. Med. J. 1968, 44, 218–222. [Google Scholar] [CrossRef][Green Version]
- Sherins, R.S.; Vrity, M.A. Central pontine myelinolysis associated with acute hemorrhagic pancreatitis. J. Neurol. Neurosurg. Psychiatry 1968, 31, 583–588. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cabezas-Moya, R.; Patterson, M. Hyperglycemia without ketosis and the hyperosmolality syndrome. South. Med. J. 1969, 62, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.D.; Conn, J.W.; Dykman, C.J.; Pek, S.; Starr, J.I. Mechanisms and management of hyperosmolar coma without ketoacidosis in the diabetic. Diabetes 1969, 18, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.L.; Done, A.K. Extreme hyperosmolality and “transient diabetes” due to inappropriately diluted infant formula. Am. J. Dis. Child. 1969, 118, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, J.A.; Keefe, D.M. Transient hyperglycemia and aketotic hyperosmolar acidosis with heat stroke. Pediatrics 1969, 44, 737–741. [Google Scholar] [CrossRef]
- Oakes, D.D.; Schreibman, P.H.; Hoffman, R.S.; Arky, R.A. Hyperglycemic, nonketotic coma in the patient with burns: Factors in pathogenesis. Metabolism 1969, 18, 103–109. [Google Scholar] [CrossRef]
- Rubin, H.M.; Kramer, R.; Drash, A. Hyperosmolality complicating diabetes mellitus in childhood. J. Pediatr. 1969, 74, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Davidson, A.R. Hyperosmolar non-ketoacidotic coma as a complication of cerebral compression. Postgrad. Med. J. 1970, 46, 720–722. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stevenson, R.E.; Bowyer, F.P. Hyperglycemia with hyperosmolal dehydration in nondiabetic infants. J. Pediatr. 1970, 77, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Gerich, J.E.; Martin, M.M.; Recant, L. Clinical and metabolic characteristics of hyperosmolar nonketotic coma. Diabetes 1971, 20, 228–238. [Google Scholar] [CrossRef]
- Hazard, J.; Perlemuter, L.; Emile, J.; Nochy, D.; Fraysse, B.; Le Bézu, M.; Bernheim, R. Hyperglycemic hyperosmolar coma (apropos of 3 cases). Ann. Med. Interne 1971, 122, 623–632. [Google Scholar]
- Evans, C.C.; Littler, W.A.; Meade, J.B. Hyperosmolar hyperglycaemic non-ketotic diabetic coma complicating open heart surgery. Br. Heart J. 1972, 34, 1075–1077. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Doromal, N.M.; Canter, J.W. Hyperosmolar hyperglycemic nonketotic coma complicating intravenous hyperalimentation. Surg. Gynecol. Obstet. 1973, 136, 729–732. [Google Scholar] [PubMed]
- Haddad, G.; Hajjar, E.T.; Abu-Faysal, K.; Abu-Haydar, H. Hyperosmolar nonketotic hyperglycemic coma. J. Med. Liban. 1973, 26, 277–286. [Google Scholar] [PubMed]
- Heggarty, H.; Trindade, P.; Bryan, E.M. Hyperglycaemia in hyperosmolar dehydration. Arch. Dis. Child. 1973, 48, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Hobin, F.P.; Maraist, F.B. Diabetic hyperosmolar nonketoacidotic coma complicated by mesenteric thrombosis. Case report. JFMA 1973, 60, 25–26. [Google Scholar] [PubMed]
- Tchertkoff, V.; Nayak, S.V.; Kamath, C.; Salomon, M.I. Hyperosmolar nonketotic diabetic coma: Vascular complications. J. Am. Geriatr. Soc. 1974, 22, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Asplund, K.; Eriksson, S.; Hägg, E.; Lithner, F.; Strand, T.; Wester, P.O. Hyperosmolar non-ketotic coma in diabetic stroke patients. Acta Med. Scand. 1982, 212, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, V.; Phear, D.N. Hyperosmolar non-ketotic diabetic syndrome precipitated by treatment with diuretics. Br. Med. J. (Clin. Res. Ed.) 1982, 284, 36–37. [Google Scholar] [CrossRef][Green Version]
- Noda, S.; Takao, A.; Itoh, H.; Umezaki, H. Opsoclonus in hyperosmolar nonketotic coma. J. Neurol. Neurosurg. Psychiatry 1985, 48, 1186–1187. [Google Scholar] [CrossRef][Green Version]
- Okeda, R.; Kitano, M.; Sawabe, M.; Yamada, I.; Yamada, M. Distribution of demyelinating lesions in pontine and extrapontine myelinolysis: Three autopsy cases including one case devoid of central pontine myelinolysis. Acta Neuropathol. 1986, 69, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Worthley, L.I. Hyperosmolar coma treated with intravenous sterile water. A study of three cases. Arch. Intern. Med. 1986, 146, 945–947. [Google Scholar] [CrossRef] [PubMed]
- Gocht, A.; Colmant, H.J. Central pontine and extrapontine myelinolysis: A report of 58 cases. Clin. Neuropathol. 1987, 6, 262–270. [Google Scholar]
- Singhal, P.C.; Schlondorff, D. Hyperosmolal state associated with rhabdomyolysis. Nephron 1987, 47, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.T.; Lin, C.K.; Tsai, M.D.; Chien, B.I.; Cheng, T.I.; Lin, C.S. Rhabdomyolysis associated with hyperosmolar non-ketotic coma—A case report. Zhonghua Yi Xue Za Zhi Med. J. 1988, 41, 309–310. [Google Scholar]
- McKee, A.C.; Winkelman, M.D.; Banker, B.Q. Central pontine myelinolysis in severely burned patients: Relationship to serum hyperosmolality. Neurology 1988, 38, 1211–1217. [Google Scholar] [CrossRef]
- Wood, M.L.; Griffith, D.N.; Hooper, R.J.; Patterson, D.L.; Yudkin, J.S. Fatal rhabdomyolysis associated with hyperosmolar diabetic decompensation. Diabetes Res. 1988, 8, 97–99. [Google Scholar] [PubMed]
- McComb, R.D.; Pfeiffer, R.F.; Casey, J.H.; Wolcott, G.; Till, D.J. Lateral pontine and extrapontine myelinolysis associated with hypernatremia and hyperglycemia. Clin. Neuropathol. 1989, 8, 284–288. [Google Scholar]
- Lustman, C.C.; Guérin, J.M.; Barbotin-Larrieu, F.E. Hyperosmolar nonketotic syndrome associated with rhabdomyolysis and acute kidney failure. Diabetes Care 1991, 14, 146–147. [Google Scholar] [CrossRef]
- Leung, C.B.; Li, P.K.; Lui, S.F.; Lai, K.N. Acute renal failure (ARF) caused by rhabdomyolysis due to diabetic hyperosmolar nonketotic coma: A case report and literature review. Ren. Fail. 1992, 14, 81–85. [Google Scholar] [CrossRef]
- Lord, G.M.; Scott, J.; Pusey, C.D.; Rees, A.J.; Walport, M.J.; Davies, K.A.; Bulpitt, C.; Bloom, S.R.; Muntoni, F.M. Diabetes and rhabdomyolysis. A rare complication of a common disease. Case Rep. BMJ 1993, 307, 1126–1128. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Trump, D.; O’Hanlon, S.; Rinsler, M.; Sharp, P. Hyperosmolar non-ketotic diabetic coma and rhabdomyolysis. Postgrad. Med. J. 1994, 70, 44–46. [Google Scholar] [CrossRef][Green Version]
- Rosa, E.C.; Lopes, A.C.; Liberatori Filho, A.W.; Schor, N. Rhabdomyolysis due to hyperosmolarity leading to acute renal failure. Ren. Fail. 1997, 19, 295–301. [Google Scholar] [CrossRef]
- Tanaka, S.; Kobayashi, T.; Kawanami, D.; Hori, A.; Okubo, M.; Nakanishi, K.; Katori, H.; Murase, T. Paradoxical glucose infusion for hypernatraemia in diabetic hyperglycaemic hyperosmolar syndrome. J. Intern. Med. 2000, 248, 166–168. [Google Scholar] [CrossRef]
- Ka, T.; Takahashi, S.; Tsutsumi, Z.; Moriwaki, Y.; Yamamoto, T.; Fukuchi, M. Hyperosmolar non-ketotic diabetic syndrome associated with rhabdomyolysis and acute renal failure: A case report and review of literature. Diabetes Nutr. Metab. 2003, 16, 317–322. [Google Scholar]
- Çokar, O.; Aydin, B.; Ozer, F. Non-ketotic hyperglycaemia presenting as epilepsia partialis continua. Seizure 2004, 13, 264–269. [Google Scholar] [CrossRef]
- Morales, A.E.; Rosenbloom, A.L. Death caused by hyperglycemic hyperosmolar state at the onset of type 2 diabetes. J. Pediatr. 2004, 144, 270–273. [Google Scholar] [CrossRef]
- Tarcan, A.; Güracan, B.; Tiker, F. Breastfeeding malnutrition and hypernatraemia: Three severe cases that featured hyperglycaemia. Ann. Trop. Paediatr. 2004, 24, 187–188. [Google Scholar] [CrossRef]
- Bhowmick, S.K.; Levens, K.L.; Rettig, K.R. Hyperosmolar hyperglycemic crisis: An acute life-threatening event in children and adolescents with type 2 diabetes mellitus. Endocr. Pract. 2005, 11, 23–29. [Google Scholar] [CrossRef]
- McDonnell, C.M.; Pedreira, C.C.; Vadamalayan, B.; Cameron, F.J.; Werther, G.A. Diabetic ketoacidosis, hyperosmolarity and hypernatremia: Are high-carbohydrate drinks worsening initial presentation? Pediatr. Diabetes 2005, 6, 90–94. [Google Scholar] [CrossRef]
- Bhowmick, S.K.; Hundley, O.T.; Rettig, K.R. Severe hypernatremia and hyperosmolality exacerbated by an herbal preparation in a patient with diabetic ketoacidosis. Clin. Pediatr. 2007, 46, 831–834. [Google Scholar] [CrossRef]
- Blas-Macedo, J.; Blas-Soto, V. Hypernatremia in hyperosmolar hyperglycemic syndrome. Rev. Med. Inst. Seguro Soc. 2011, 49, 335–337. [Google Scholar]
- Nwosu, B.U.; Adhami, S.; Rogol, A.D. Stroke in a child with Adams-Oliver syndrome and mixed diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. J. Pediatr. Endocrinol. Metab. 2012, 25, 357–361. [Google Scholar] [CrossRef]
- Hegazi, M.O.; Mashankar, A. Central pontine myelinolysis in the hyperosmolar hyperglycaemic state. Med. Princ. Pract. 2013, 22, 96–99. [Google Scholar] [CrossRef]
- Masood, M.; Kumar, S.; Asghar, A.; Jabbar, A. An unusual case of central diabetes insipidus & hyperglycemic hyperosmolar state following cardiorespiratory arrest. BMC Res. Notes 2013, 6, 325. [Google Scholar]
- Kim, H.J.; Kim, D.H.; Jun, Y.H.; Lee, J.E. A rare diabetes ketoacidosis in combined severe hypernatremic hyperosmolarity in a new-onset in an adolescent with type I diabetes. BMJ Case Rep. 2014, 2014, bcr2014208016. [Google Scholar] [CrossRef]
- Vigil, D.; Ganta, K.; Sun, Y.; Dorin, R.I.; Tzamaloukas, A.H.; Servilla, K.S. Prolonged hypernatremia triggered by hyperglycemic hyperosmolar state with coma: A case report. World J. Nephrol. 2015, 4, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Arya, M.K.; Ahmed, S.M.; Shah, K.N.; Ali, U.S. Diabetic ketoacidosis with extreme hypernatremia in a 4-year-old girl. Ind. J. Crit. Care Med. 2017, 21, 610–612. [Google Scholar] [CrossRef]
- Brzezniak, C.E.; Vietor, N.; Hogan, P.E.; Oronsky, B.; Thilagar, B.; Ray, C.M.; Caroen, S.; Lybeck, M.; Oronsky, N.; Cater, C.A. A case of paraneoplastic Cushing syndrome presenting as hyperglycemic hyperosmolar nonketotic syndrome. Case Rep. Oncol. 2017, 10, 321–324. [Google Scholar] [CrossRef]
- Amin, A.; Gandhi, B.; Torre, S.; Amirpour, A.; Cheng, G.; Patel, M.; Hossain, M.A. Rhabdomyolysis-induced acute kidney injury in diabetic emergency: Underdiagnosed and an important association to be aware of. Case Rep. Med. 2018, 2018, 4132738. [Google Scholar] [CrossRef]
- Burmazovic, S.; Henzen, C.; Brander, L.; Cioccari, L. One too many diabetes; the combination of hyperglycaemic hyperosmolar state and central diabetes insipidus. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018, 18–0029. [Google Scholar] [CrossRef]
- Estifan, E.; Nanavati, S.M.; Kumar, V.; Gibiezaite, S.; Michael, P. Salty diabetes: A case series of hypernatremia presenting with diabetic ketoacidosis. AME. Case Rep. 2019, 3, 27. [Google Scholar] [CrossRef] [PubMed]
- Galili, Y.; Gonzalez, C.; Lytle, M.; Carlan, S.J.; Madruga, M. Full recovery from extreme hypernatremia in an elderly woman with hyperosmolar hyperglycemic syndrome and abnormal electroencephalogram. SAGE Open Med. Case Rep. 2019, 7, 2050313X19848887. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Barmanray, R.; Qian, S.; De Alwis, D.; Fennessy, G. Survival following extreme hypernatraemia associated with severe dehydration and undiagnosed diabetes mellitus. Case Rep. Endocrinol. 2019, 2019, 4174259. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, G.; Majmundar, M.M.; Pacheco, E.; Zala, H.; Chaudhari, S. Hypernatremia in diabetic ketoacidosis: Rare presentation and a cautionary tale. Cureus 2020, 12, e11841. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Q.; Khalid, L.; Usman, N.; Neupane, N.; Mahmoud, A. Rhabdomyolysis induced acute kidney injury in hyperglycemic hyperosmolar state patient with new-onset diabetes: A case report. Cureus 2020, 12, e9188. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, K.; Koriyama, N.; Kojima, N.; Ikeda, M.; Nishio, Y. Central pontine myelolysis during treatment of hyperglycemic hyperosmolar syndrome: A case report. Clin. Diabetes Endocrinol. 2020, 1, 23. [Google Scholar] [CrossRef] [PubMed]
- Shima, S.; Umino, S.; Kitamura, M.; Ushijima, K.; Yatsuga, S. Severe hypernatremia in combined diabetic ketoacidosis and hyperglycemic hyperosmolar state: A case report of two Japanese children. Cureus 2020, 12, e9672. [Google Scholar] [CrossRef] [PubMed]
- Sohal, R.J.; Joshi, S. Salty, sweet and difficult to treat; a case of profound hypernatremia in the setting of hyperosmotic hyperglycemic state. Cureus 2020, 12, 37278. [Google Scholar] [CrossRef]
- Maduemem, K.E.; Adesanya, O.; Anuruegbe, O.O.; Rafiq, A. Hyperglycaemic hyperosmolar state: First presentation of type 1 diabetes mellitus in an adolescent with complex medical needs. BMJ Case Rep. 2021, 14, e237793. [Google Scholar] [CrossRef]
- Choo, S.J.; Lee, H.G.; Kim, C.J.; Yang, E.M. Severe hypernatremia in soft drink ketoacidosis and hyperglycemic hyperosmolar state at the onset of type 2 diabetes mellitus: A case series of three adolescents. Clin. Pediatr. Endocrinol. 2022, 31, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Lathiya, M.K.; Errabelli, P.; Cullinan, S.M.; Amadi, E.J. Severe hypernatremia in hyperglycemic conditions; managing it effectively: A case report. World J. Crit. Care Med. 2023, 9, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, A.L. Hyperglycemic hyperosmolar state: An emerging pediatric problem. J. Pediatr. 2010, 156, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.Y.; She, D.M.; Wang, F.; Guo, G.; Li, R.; Fang, P.; Li, L.; Zhou, Y.; Zhang, K.Q.; Xue, Y. Clinical profiles, outcomes and risk factors among type 2 diabetic inpatients with diabetic ketoacidosis and hyperglycemic hyperosmolar state: A hospital-based analysis over a 6-year period. BMC. Endocr. Disord. 2020, 20, 182. [Google Scholar] [CrossRef] [PubMed]
- Rondon-Berrios, H.; Argyropoulos, C.; Ing, T.S.; Raj, D.S.; Malhotra, D.; Agaba, E.I.; Rohrscheib, M.; Khitan, Z.J.; Murata, G.; Shapiro, J.I.; et al. Hypertonicity: Clinical entities, manifestations and treatment. World J. Nephrol. 2017, 6, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mange, K.; Matsuura, D.; Cizman, B.; Soto, H.; Ziyadeh, F.N.; Goldfarb, S.; Neilson, E.G. Language guiding therapy: The case of dehydration versus volume depletion. Ann. Intern. Med. 1997, 127, 848–853. [Google Scholar] [CrossRef]
- Spital, A. Dehydration versus volume depletion—And the importance of getting it right. Am. J. Kidney Dis. 2007, 49, 721–722. [Google Scholar] [CrossRef] [PubMed]
- Roumelioti, M.E.; Glew, R.H.; Khitan, Z.J.; Rondon-Berrios, H.; Argyropoulos, C.P.; Malhotra, D.; Raj, D.S.; Agaba, E.I.; Rohrscheib, M.; Murata, G.H.; et al. Fluid balance concepts in medicine: Principles and practice. World J. Nephrol. 2018, 7, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Bhave, G.; Neilson, E.G. Volume depletion versus dehydration: How understanding the difference can guide therapy. Am. J. Kidney Dis. 2011, 58, 302–309. [Google Scholar] [CrossRef]
- Rohrscheib, M.; Rondon-Berrios, H.; Argyropoulos, C.; Glew, R.H.; Murata, G.H.; Tzamaloukas, A.H. Indices of serum tonicity in clinical practice. Am. J. Med. Sci. 2015, 349, 537–544. [Google Scholar] [CrossRef]
- Popli, S.; Leehey, D.J.; Daugirdas, J.T.; Bansal, V.K.; Ho, D.S.; Hano, J.E.; Ing, T.S. Asymptomatic, nonketotic, severe hyperglycemia with hyponatremia. Arch. Intern. Med. 1990, 150, 1962–1964. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Yi, J.H.; Han, S.W.; Kim, H.J. Recurrent symptomatic hyperglycemia on maintenance hemodialysis is not necessarily related to hypertonicity: A case report. Electrolyte Blood Press 2008, 6, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Ing, T.S.; Siamopoulos, K.C.; Raj, D.S.C.; Elisaf, M.S.; Rohrscheib, M.; Murata, G.H. Pathophysiology and management of fluid and electrolyte disturbances in patients on chronic dialysis with severe hyperglycemia. Semin. Dial. 2008, 21, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Roumelioti, M.E.; Ganta, K.; Glew, R.H.; Gibb, J.; Vigil, D.; Do, C.; Servilla, K.S.; Wagner, B.; Owen, J.; et al. Dialysis-associated hyperglycemia: Manifestations and treatment. Int. Urol. Nephrol. 2020, 52, 505–517. [Google Scholar] [CrossRef] [PubMed]
- Koves, I.H.; Neutze, J.; Donath, S.; Lee, W.; Werther, G.A.; Barnett, P.; Cameron, F.J. The accuracy of clinical assessment of dehydration during diabetic ketoacidosis in childhood. Diabetes Care 2004, 27, 2485–2487. [Google Scholar] [CrossRef] [PubMed]
- Adrogué, H.J.; Madias, N.E. Hypernatremia. N. Engl. J. Med. 2000, 342, 1493–1499. [Google Scholar] [CrossRef]
- Feig, P.U. Hypernatremia and hypertonic syndromes. Med. Clin. N. Am. 1981, 65, 271–290. [Google Scholar] [CrossRef] [PubMed]
- Edelman, I.S.; Leibman, J.; O’Meara, M.P.; Birkenfeld, L.W. Interrelations between serum sodium concentration, serum osmolarity and total exchangeable sodium, total exchangeable potassium and total body water. J. Clin. Investig. 1958, 37, 1236–1256. [Google Scholar] [CrossRef] [PubMed]
- Rose, B.D. New approach to disturbances in the plasma sodium concentration. Am. J. Med. 1986, 81, 1033–1040. [Google Scholar] [CrossRef]
- Wagner, B.; Malhotra, D.; Schmidt, D.; Raj, D.S.; Khitan, Z.J.; Shapiro, J.I.; Tzamaloukas, A.H. Hypertonic saline infusion for hyponatremia: Limitations of the Adrogué-Madias and other formulas. Kidney360 2023, 4, e555–e561. [Google Scholar] [CrossRef]
- Liamis, G.; Gianoutsos, C.; Elisaf, M.S. Hyperosmolar nonketotic syndrome with hypernatremia: How can we monitor treatment? Diabetes Metab. 2000, 26, 403–405. [Google Scholar] [PubMed]
- Palmer, B.F.; Clegg, D.J. Electrolyte and acid-base disturbances in patients with diabetes mellitus. N. Engl. J. Med. 2015, 373, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Konstantinov, N.K.; Sun, Y.; Dorin, R.I.; Ing, T.S.; Malhotra, D.; Murata, G.H.; Shapiro, J.I. Principles of quantitative fluid and cation replacement in extreme hyperglycemia. Cureus 2013, 5, e110. [Google Scholar] [CrossRef]
- Fayfman, M.; Pasquel, F.J.; Umpierrez, G.E. Management of hyperglycemic crises: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Med. Clin. N. Am. 2017, 101, 587–606. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.; Guo, Y.W.; Chen, H.S. Corrected sodium levels for hyperglycemia is a better predictor than measured sodium levels or clinical outcomes among patients with extreme hyperglycemia. J. Chin. Med. Assoc. 2020, 83, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Soni, A.; Rao, S.V.; Bajaj, R.; Treser, G. Extreme hyperglycemia and hyperosmolarity. Diabetes Care 1990, 13, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.A. Hyperglycemia-induced hypernatremia—Calculation of the expected serum sodium depression. N. Engl. J. Med. 1973, 289, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Robin, A.P.; Ing, T.S.; Lancaster, G.A.; Soung, L.S.; Sparagana, M.; Geis, W.P.; Hano, J.E. Hyperglycemia-induced hyponatremia: A fresh look. Clin. Chem. 1979, 25, 496–497. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Kyner, W.T.; Galey, W.R., Jr. Determinants of osmotic phenomena created by an isolated change in extracellular solute in anuria. Miner. Electrolyte Metab. 1987, 13, 117–125. [Google Scholar]
- Tzamaloukas, A.H.; Ing, T.S.; Siamopoulos, K.C.; Rohrscheib, M.; Elisaf, M.S.; Raj, D.S.C.; Murata, G.H. Body fluid abnormalities in severe hyperglycemia in patients on chronic dialysis: Theoretical analysis. J. Diabetes Complicat. 2007, 21, 374–380. [Google Scholar] [CrossRef]
- Arieff, A.I.; Carroll, H.J. Nonketotic hyperosmolar coma with hyperglycemia: Clinical features, pathophysiology, renal function, acid-base balance, plasma-cerebrovascular fluid equilibria and the effects of therapy in 37 cases. Medicine 1972, 51, 73–94. [Google Scholar] [CrossRef] [PubMed]
- Flythe, J.E.; Chang, T.I.; Gallagher, M.P.; Lindley, E.; Madero, M.; Sarafidis, P.A.; Unruh, M.L.; Wang, A.Y.M.; Weiner, D.E.; Cheung, M.; et al. Blood pressure and volume management in dialysis: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2020, 97, 861–876. [Google Scholar] [CrossRef] [PubMed]
- Lorber, D. Nonketotic hypertonicity in diabetes mellitus. Med. Clin. N. Am. 1995, 79, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Ing, T.S.; Elisaf, M.S.; Raj, D.S.C.; Siamopoulos, K.C.; Rohrscheib, M.; Murata, G.H. Abnormalities of serum potassium concentration in dialysis-associated hyperglycemia and their correction with insulin: A unique clinical/physiologic exercise in internal potassium balance. Int. Urol. Nephrol. 2010, 42, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Ing, T.S.; Elisaf, M.S.; Raj, D.S.C.; Siamopoulos, K.C.; Rohrscheib, M.; Murata, G.H. Abnormalities of serum potassium concentration in dialysis-associated hyperglycemia and their correction with insulin: Review of published reports. Int. Urol. Nephrol. 2011, 43, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Moran, S.M.; Jamison, R.L. The variable hyponatremic response to hyperglycemia. West. J. Med. 1985, 142, 49–53. [Google Scholar] [PubMed]
- Tzamaloukas, A.H.; Rohrscheib, M.; Ing, T.S.; Siamopoulos, K.C.; Elisaf, M.S.; Spalding, C.T. Serum tonicity, extracellular volume and clinical manifestations in symptomatic dialysis-associated hyperglycemia treated with insulin. Int. J. Artif. Organs 2004, 27, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Tzamaloukas, A.H.; Ing, T.S.; Siamopoulos, K.C.; Rohrscheib, M.; Elisaf, M.S.; Raj, D.S.C.; Murata, G.H. Body fluid abnormalities in severe hyperglycemia in patients on chronic dialysis: Review of published reports. J. Diabetes Complicat. 2008, 22, 29–37. [Google Scholar] [CrossRef]
- Rohrscheib, M.; Sam, R.; Raj, D.S.; Argyropoulos, C.P.; Unruh, M.L.; Lew, S.Q.; Ing, T.S.; Levin, N.W.; Tzamaloukas, A.H. Edelman revisited: Concepts, achievements, and challenges. Front. Med. 2022, 8, 808765. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Biochemical Parameter | Reference [26] | Reference [27] | Reference [28] |
|---|---|---|---|
| [Glu]S, mmol/L | 56.1 | 52.2 | 40.7 |
| [Glu]S, mg/dL | 1009.7 | 940.3 | 732.6 |
| [Na]S, mmol/L | 153.4 | 153.6 | 153.0 |
| Tonicity, mOsm/L | 362.9 | 359.4 | 346.7 |
| [Na]Cor, mmol/L | 168.0 | 167.0 | 163.1 |
| Biochemical Parameter | Range | Median | 25th Percentile | 75th Percentile |
|---|---|---|---|---|
| [Glu]S, mmol/L | 20.3–173.3 | 49.7 | 36.1 | 60.9 |
| [Glu]S, mg/dL | 365.0–3120.0 | 894.6 | 649.8 | 1096.2 |
| [Na]S, mmol/L | 145.0–228.0 | 160.0 | 152.0 | 169.5 |
| Tonicity, mOsm/L | 314.0–545.3 | 373.2 | 354.9 | 393.0 |
| [Na]Cor, mmol/L | 151.2–238.6 | 173.6 | 166.8 | 182.2 |
| Abbreviation | Variable Expressed by the Abbreviation |
|---|---|
| TBW | Total body water, TBW1 in baseline euglycemia, TBW2 in hyperglycemia. |
| [Na]S | Serum sodium concentration, [Na]S1 in baseline euglycemia, [Na]S2 in hyperglycemia |
| [Na]Cor | Serum sodium concentration adjusted for the degree of hyperglycemia |
| [Na]Lost | Average sodium concentration in fluids, mainly urine, lost during development of hyperglycemia |
| [Glu]S | Serum glucose concentration, [Glu]S1 in baseline euglycemia, [Glu]S2 in hyperglycemia |
| VLost | Volume of water lost during development of hyperglycemia |
| [K]Lost | Average potassium concentration in fluids, mainly urine, lost during development of hyperglycemia |
| TBNa | Total body sodium, TBNa1 in baseline euglycemia, TBNa2 in hyperglycemia |
| TBK | Total body potassium, TBK1 in baseline euglycemia, TBK2 in hyperglycemia |
| Formula | Reference | |
|---|---|---|
| (1) | [138] | |
| (2) | [139] | |
| (3) | ||
| (4) | [24] | |
| (5) | ||
| (6) | ||
| (7) | ||
| (8) | ||
| (9) | ||
| (10) |
| Biochemical Parameter | DKA 1 | HHS 2 |
|---|---|---|
| [Glu]S2, mmol/L mg/dL | 31.4 566 | 57.4 1034 |
| [Na]S2, mmol/L | 133.7 | 145.8 |
| [Na]Cor, mmol/L | 141.1 | 160.8 |
| [Na]Lost + [K]Lost = 0 VLost/TBW1 | 0.008 | 0.129 |
| [Na]Lost + [K]Lost = 60 mmol/L VLost/TBW1 VLost × ([Na]Lost + [K]Lost)/([Na]S1 × TBW1) | 0.014 0.008 | 0.206 0.088 |
| [Na]Lost + [K]Lost = 110 mmol/L VLost/TBW1 VLost × ([Na]Lost + [K]Lost)/([Na]1 × TBW1) | 0.035 0.028 | 0.409 0.322 |
| Biochemical Parameter | 25th Percentile | Median | 75th Percentile |
|---|---|---|---|
| [Na]Cor, mmol/L | 166.8 | 173.6 | 188.2 |
| [Na]Lost + [K]Lost = 0 VLost/TBW1 | 0.161 | 0.194 | 0.232 |
| [Na]Lost + [K]Lost = 60 mmol/L VLost/TBW1 VLost × ([Na]Lost + [K]Lost)/([Na]S1 × TBW1) | 0.251 0.108 | 0.296 0.128 | 0.345 0.148 |
| [Na]Lost + [K]Lost = 110 mmol/L VLost/TBW1 VLost × ([Na]Lost + [K]Lost)/([Na]1 × TBW1) | 0.472 0.371 | 0.528 0.415 | 0.584 0.459 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, B.; Ing, T.S.; Roumelioti, M.-E.; Sam, R.; Argyropoulos, C.P.; Lew, S.Q.; Unruh, M.L.; Dorin, R.I.; Degnan, J.H.; Tzamaloukas, A.H. Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development. J. Clin. Med. 2024, 13, 1957. https://doi.org/10.3390/jcm13071957
Wagner B, Ing TS, Roumelioti M-E, Sam R, Argyropoulos CP, Lew SQ, Unruh ML, Dorin RI, Degnan JH, Tzamaloukas AH. Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development. Journal of Clinical Medicine. 2024; 13(7):1957. https://doi.org/10.3390/jcm13071957
Chicago/Turabian StyleWagner, Brent, Todd S. Ing, Maria-Eleni Roumelioti, Ramin Sam, Christos P. Argyropoulos, Susie Q. Lew, Mark L. Unruh, Richard I. Dorin, James H. Degnan, and Antonios H. Tzamaloukas. 2024. "Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development" Journal of Clinical Medicine 13, no. 7: 1957. https://doi.org/10.3390/jcm13071957
APA StyleWagner, B., Ing, T. S., Roumelioti, M.-E., Sam, R., Argyropoulos, C. P., Lew, S. Q., Unruh, M. L., Dorin, R. I., Degnan, J. H., & Tzamaloukas, A. H. (2024). Hypernatremia in Hyperglycemia: Clinical Features and Relationship to Fractional Changes in Body Water and Monovalent Cations during Its Development. Journal of Clinical Medicine, 13(7), 1957. https://doi.org/10.3390/jcm13071957