

Evaluation of Outcome after Total Hip Arthroplasty for Femoral Neck Fracture: Which Factors Are Relevant for Better Results?
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Surgical Technique
2.3. Radiographic Evaluation
2.4. Outcome Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, C.A.; Starr, A.Z.; Nunley, J.A. Analysis of past secular trends of hip fractures and predicted number in the future 2010–2050. J. Orthop. Trauma. 2012, 26, 117–122. [Google Scholar] [CrossRef]
- Swayambunathan, J.; Dasgupta, A.; Rosenberg, P.S.; Hannan, M.T.; Kiel, D.P.; Bhattacharyya, T. Incidence of hip fracture over 4 decades in the Framingham Heart study. JAMA Intern. Med. 2020, 180, 1225–1231. [Google Scholar] [CrossRef]
- Lewiecki, E.M.; Wright, N.C.; Curtis, J.R.; Siris, E.; Gagel, R.F.; Saag, K.G.; Singer, A.J.; Steven, P.M.; Adler, R.A. Hip fracture trends in the United States, 2002 to 2015. Osteoporos. Int. 2018, 29, 717–722. [Google Scholar] [CrossRef]
- Chen, I.J.; Chiang, C.Y.; Li, Y.H.; Chang, C.H.; Hu, C.C.; Chen, D.W.; Chang, Y.; Yang, W.-E.; Shih, H.-N.; Ueng, S.W.-N.; et al. Nationwide cohort study of hip fractures: Time trends in the incidence rates and projections up to 2035. Osteoporos. Int. 2015, 26, 681–688. [Google Scholar] [CrossRef]
- Konnopka, A.; Jerusel, N.; Konig, H.H. The health and economic consequences of osteopenia- and osteoporosis-attributable hip fractures in Germany: Estimation for 2002 and projection until 2050. Osteoporos. Int. 2009, 20, 1117–1129. [Google Scholar] [CrossRef]
- Rosengren, B.E.; Karlsson, M.K. The annual number of hip fractures in Sweden will double from year 2002 to 2050, projections based on local and nationwide data. Acta Orthop. 2014, 85, 234–237. [Google Scholar] [CrossRef]
- Brauer, C.A.; Coca-Perraillon, M.; Cutler, D.M.; Rosen, A.B. Incidence and mortality of hip fractures in the United States. JAMA 2009, 302, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Schairer, W.W.; Lane, J.M.; Halsey, D.A.; Iorio, R.; Padgett, D.E.; McLawhorn, A.S. The Frank Stinchfield Award: Total hip arthroplasty for femoral neck fracture is not a typical DRG 470, a propensity-matched cohort study. Clin. Orthop. Relat. Res. 2017, 475, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F.; Ivanescu, A.D.; Fodor, P.; Moldovan, L.; Bataga, T. Correlation between Inflammatory Systemic Biomarkers and Surgical Trauma in Elderly Patients with Hip Fractures. J. Clin. Med. 2023, 12, 5147. [Google Scholar] [CrossRef] [PubMed]
- Mundi, S.; Pindiprolu, B.; Simunovic, N.; Bhandari, M. Similar mortality rates in hip fracture patients over the past 31 years. Acta Orthop. 2014, 85, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.J.; Callaghan, J.J.; Cram, P.; Karam, M.; Marsh, J.L.; Noiseux, N.O. Changing trends in the treatment of femoral neck fractures: A review of the American Board of Orthopaedic Surgery Database. J. Bone Jt. Surg. Am. 2014, 96, e149. [Google Scholar] [CrossRef]
- Schiavi, P.; Pogliacomi, F.; Colombo, M.; Amarossi, A.; Ceccarelli, F.; Vaienti, E. Acetabular erosion following bipolar hemiarthroplasty: A Role for the size of femoral head? Injury 2019, 50 (Suppl. S4), S21–S25. [Google Scholar] [CrossRef]
- Stronach, B.M.; Bergin, P.F.; Perez, J.L.; Watson, S.; Jones, L.C.; McGwin, G.; Ponce, B.A. The rising use of total hip arthroplasty for femoral neck fractures in the United States. Hip Int. 2020, 30, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Goh, S.-K.; Samuel, M.; Su, D.H.C.; Chan, E.S.-Y.; Yeo, S.-J. Meta-analysis comparing total hip arthroplasty with hemiarthroplasty in the treatment of displaced neck of femur fracture. J. Arthroplast. 2009, 24, 400–406. [Google Scholar] [CrossRef]
- Yu, L.; Wang, Y.; Chen, J. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fractures: Meta-analysis of randomized trials. Clin. Orthop. Relat. Res. 2012, 470, 2235–2243. [Google Scholar] [CrossRef] [PubMed]
- Awad, M.E.; Farley, B.J.; Mostafa, G.; Saleh, K.J. Direct anterior approach has short term functional benefit and higher resource requirements compared with the posterior approach in primary total hip arthroplasty: A meta-analysis of functional outcomes and cost. Bone Jt. J. 2021, 103-B, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Bergin, P.F.; Doppelt, J.D.; Kephart, C.J.; Benke, M.T.; Graeter, J.H.; Holmes, A.S.; Haleem-Smith, H.; Tuan, R.S.; Unger, A.S. Comparison of minimally invasive direct anterior versus posterior total hip arthroplasty based on inflammation and muscle damage markers. J. Bone Jt. Surg. Am. 2011, 93, 1392–1398. [Google Scholar] [CrossRef]
- Miller, L.E.; Gondusky, J.S.; Kamath, A.F.; Boettner, F.; Wright, J.; Bhattacharyya, S. Influence of surgical approach on complication risk in primary total hip arthroplasty. Acta Orthop. 2018, 89, 289–294. [Google Scholar] [CrossRef]
- Taunton, M.J.; Mason, J.B.; Odum, S.M.; Springer, B.D. Direct anterior total hip arthroplasty yields more rapid voluntary cessation of all walking aids: A prospective, randomized clinical trial. J. Arthroplast. 2014, 29 (Suppl. S9), 169–172. [Google Scholar] [CrossRef]
- Taunton, M.J.; Trousdale, R.T.; Sierra, R.J.; Kaufman, K.; Pagnano, M.W. John Charnley Award: Randomized clinical trial of direct anterior and miniposterior approach THA: Which provides better functional recovery? Clin. Orthop. Relat. Res. 2018, 476, 216–229. [Google Scholar] [CrossRef]
- Peters, R.M.; van Beers, L.; van Steenbergen, L.N.; Wolkenfelt, J.; Ettema, H.B.; Ten Have, B.; Rijk, P.C.; Stevens, M.; Bulstra, S.K.; Poolman, R.W.; et al. Similar superior patient-reported outcome measures for anterior and posterolateral approaches after total hip arthroplasty: Postoperative patient- reported outcome measure improvement after 3 months in 12,774 primary total hip arthroplasties using the anterior, anterolateral, straight lateral, or posterolateral approach. J. Arthroplast. 2018, 33, 1786–1793. [Google Scholar]
- Sibia, U.S.; Turner, T.R.; MacDonald, J.H.; King, P.J. The impact of surgical technique on patient reported outcome measures and early complications after total hip arthroplasty. J. Arthroplast. 2017, 32, 1171–1175. [Google Scholar] [CrossRef]
- Le Manach, Y.; Collins, G.; Bhandari, M.; Bessissow, A.; Boddaert, J.; Khiami, F.; Chaudhry, H.; De Beer, J.; Riou, B.; Landais, P.; et al. Outcomes after hip fracture surgery compared with elective total hip replacement. JAMA 2015, 314, 1159–1166. [Google Scholar] [CrossRef]
- Heinonen, M.; Karppi, P.; Huusko, T.; Kautiainen, H.; Sulkava, R. Post-operative degree of mobilization at two weeks predicts one-year mortality after hip fracture. Aging Clin. Exp. Res. 2004, 16, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Imura, K.; Ishii, Y.; Yagisawa, K.; Matsueda, M. Postoperative ambulatory level after hip fracture in the elderly predicts survival rate. Arch. Orthop. Trauma. Surg. 2000, 120, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Iosifidis, M.; Iliopoulos, E.; Panagiotou, A.; Apostolidis, K.; Traios, S.; Giantsis, G. Walking ability before and after a hip fracture in elderly predict greater longterm survivorship. J. Orthop. Sci. 2016, 21, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Cichos, K.H.; Mabry, S.E.; Spitler, C.A.; McGwin, J.r.G.; Quade, J.H.; Ghanem, E.S. Comparison between the direct anterior and posterior approaches for total hip arthroplasty performed for femoral neck fracture. J. Orthop. Trauma. 2021, 35, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Heiden, J.J.; Goodin, S.R.; Mormino, M.A.; Siebler, J.C.; Putnam, S.M.; Lyden, E.R.; Tao, M.A. Early ambulation after hip fracture surgery is associated with decreased 30-day mortality. J. Am. Acad. Orthop. Surg. 2021, 29, e238–e242. [Google Scholar] [CrossRef] [PubMed]
- Pogliacomi, F.; Schiavi, P.; Grappiolo, G.; Ceccarelli, F.; Vaienti, E. Outcome of short versus conventional stem for total hip arthroplasty in the femur with a high cortical index: A five year follow-up prospective multicentre comparative study. Int. Orthop. 2020, 44, 61–68. [Google Scholar] [CrossRef]
- Loppini, M.; Schiavi, P.; Rocca, A.D.; Traverso, F.; Rocca, F.D.; Mazziotta, G.; Astore, F.; Grappiolo, G. Double-trabecular metal cup technique for the management of Paprosky type III defects without pelvic discontinuity. Hip Int. 2018, 28 (Suppl. S2), 66–72. [Google Scholar] [CrossRef]
- Hossain, F.; Konan, S.; Volpin, A.; Haddad, F.S. Early performance-based and patient-reported outcomes of a contemporary taper fit bone-conserving short stem femoral component in total hip arthroplasty. Bone Jt. J. 2017, 99-B, 49–55. [Google Scholar] [CrossRef]
- Khalily, C.; Lester, D.K. Results of a tapered cementless femoral stem implanted in varus. J. Arthroplast. 2002, 17, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F.; Moldovan, L.; Bataga, T. A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania. Healthcare 2023, 11, 1866. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, C.; Geissler, A. Utilization rates of hip arthroplasty in OECD countries. Osteoarthr. Cartil. 2014, 22, 734–741. [Google Scholar] [CrossRef]
- Yoon, R.S.; Iorio, R.; Bosco, J.A.; Hutzler, L.H.; Mahure, S.A. Hip arthroplasty for fracture vs elective care. J. Arthroplast. 2017, 32, 2353–2358. [Google Scholar] [CrossRef] [PubMed]
- Grace, T.R.; Patterson, J.T.; Tangtiphaiboontana, J.; Krogue, J.D.; Vail, T.P.; Ward, D.T. Hip fractures and the bundle: A cost analysis of patients undergoing hip arthroplasty for femoral neck fracture vs degenerative joint disease. J. Arthroplast. 2018, 33, 1681–1685. [Google Scholar] [CrossRef]
- Kester, B.S.; Williams, J.; Bosco, J.A.; Slover, J.D.; Iorio, R.; Schwarzkopf, R. The association between hospital length of stay and 90-day readmission risk for femoral neck fracture patients: Within a total joint arthroplasty bundled payment initiative. J. Arthroplast. 2016, 31, 2741–2745. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E.; Gondusky, J.S.; Bhattacharyya, S.; Kamath, A.F.; Boettner, F.; Wright, J. Does surgical approach affect outcomes in total hip arthroplasty through 90 days of follow-up? A systematic review with meta-analysis. J. Arthroplast. 2018, 33, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Malek, I.A.; Royce, G.; Bhatti, S.U.; Whittaker, J.P.; Phillips, S.P.; Wilson, I.R.; Wootton, J.R.; Starks, I. A comparison between the direct anterior and posterior approaches for total hip arthroplasty: The role of an ‘enhanced recovery’ pathway. Bone Jt. J. 2016, 98-B, 754–760. [Google Scholar] [CrossRef]
- Haller, J.M.; Working, Z.M.; Ross, H.L.; Gililland, J.M.; Kubiak, E.N. Fewer hip dislocations with anterior total hip arthroplasty for displaced femoral neck fracture. Orthopedics 2021, 44, E248–E252. [Google Scholar] [CrossRef]
- Cichos, K.H.; McGwin, G., Jr.; Boyd, B.; Arthroplasty for Hip Fracture Consortium; Ghanem, E.S. Direct Anterior Approach Total Hip Arthroplasty Is Associated with Reduced 1-Year Mortality and Surgical Complications After Femoral Neck Fracture. J. Arthroplast. 2023, 38, 2347–2354.e2. [Google Scholar] [CrossRef]
- Kunkel, S.T.; Sabatino, M.J.; Kang, R.; Jevsevar, D.S.; Moschetti, W.E. A systematic review and meta-analysis of the direct anterior approach for hemiarthroplasty for femoral neck fracture. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 217e2. [Google Scholar] [CrossRef] [PubMed]
- Bucs, G.; Dande, A.; Patczai, B.; Sebestyen, A.; Almasi, R.; Not, L.G.; Wiegand, N. Bipolar hemiarthroplasty for the treatment of femoral neck fractures with minimally invasive anterior approach in elderly. Injury 2021, 52 (Suppl. S1), S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Nogler, M.; Randelli, F.; Macheras, G.A.; Thaler, M. Hemiarthroplasty of the hip using the direct anterior approach. Operat Orthop. Traumatol. 2021, 33, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Padilla, J.A.; Gabor, J.A.; Ryan, S.P.; Long, W.J.; Seyler, T.M. Schwarzkopf RM Total Hip Arthroplasty for Femoral Neck Fracture: The Economic Implications of Orthopedic Subspecialty Training. J. Arthroplast. 2020, 35, S101–S106. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.C.; Haidukewych , G.J. Total Hip Arthroplasty for Acute Femoral Neck Fractures: Who Should Perform the Operation-Adult Reconstructive or Trauma Surgeons? J. Orthop. Trauma. 2021, 35, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Barrett, J.; Mahomed, N.N.; Baron, J.A.; Wright, R.J.; Losina, E. Association between hospital and surgeon procedure volume and the outcomes of total knee replacement. J. Bone Jt. Surg. Ser. A 2004, 86, 1909–1916. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Losina, E.; Barrett, J.; Phillips, C.; Mahomed, N.N.; Lew, R.A.; Guadagnoli, E.; Harris, W.H.; Poss, R.; Baron, J.A. Association between hospital and surgeon procedure volume with outcome of total hip replacement. J. Bone Jt. Surg. 2001, 83, 1622–1629. [Google Scholar] [CrossRef]
- Shervin, N.; Rubash, H.E.; Katz, J.N. Orthopaedic procedure volume and patient outcomes. Clin. Orthop. Relat. Res. 2007, 457, 35–41. [Google Scholar] [CrossRef]
- Maceroli, M.; Nikkel, L.E.; Mahmood, B.; Ketz, J.P.; Qiu, X.; Ciminelli, J.; Messing, S.M.; Elfar, J.C. Total hip arthroplasty for femoral neck fractures: Improved outcomes with higher hospital volumes. J. Orthop. Trauma. 2016, 30, 597–604. [Google Scholar] [CrossRef]
- Sahni, N.R.; Dalton, M.; Cutler, D.M.; Birkmeyer, J.D.; Chandra, A. Surgeon specialization and operative mortality in United States: Retrospective analysis. BMJ 2016, 354, i3571. [Google Scholar] [CrossRef] [PubMed]
- Hagen, T.P.; Vaughan-Sarrazin, M.S.; Cram, P. Relation between hospital orthopaedic specialisation and outcomes in patients aged 65 and older: Retrospective analysis of US Medicare data. BMJ 2010, 340, c165. [Google Scholar] [CrossRef] [PubMed]
- Browne, J.A.; Pietrobon, R.; Olson, S.A. Hip fracture outcomes: Does surgeon or hospital volume really matter? J. Trauma. Inj. Infect Crit. Care 2009, 66, 809–814. [Google Scholar] [CrossRef] [PubMed]
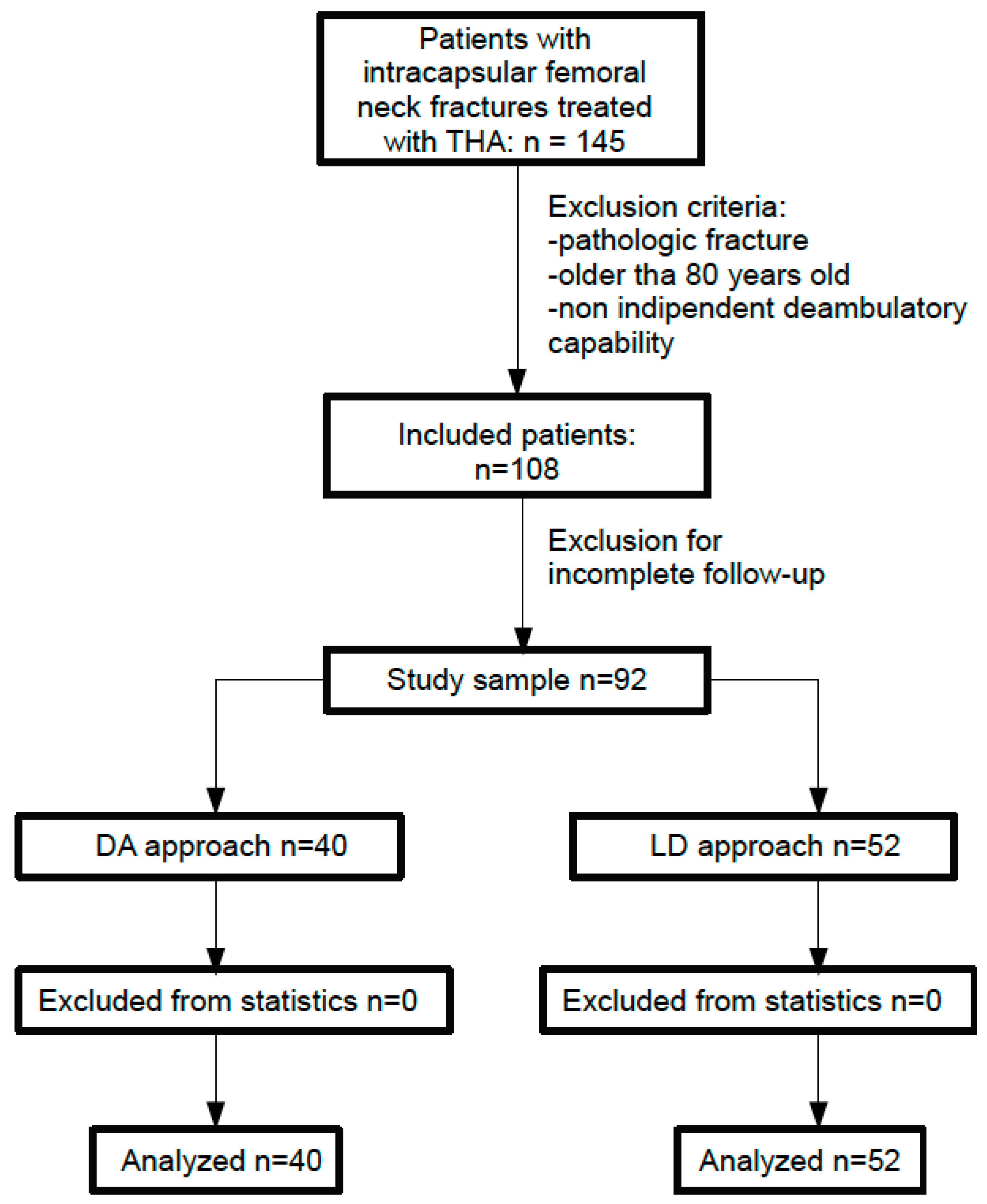

{kind=link}
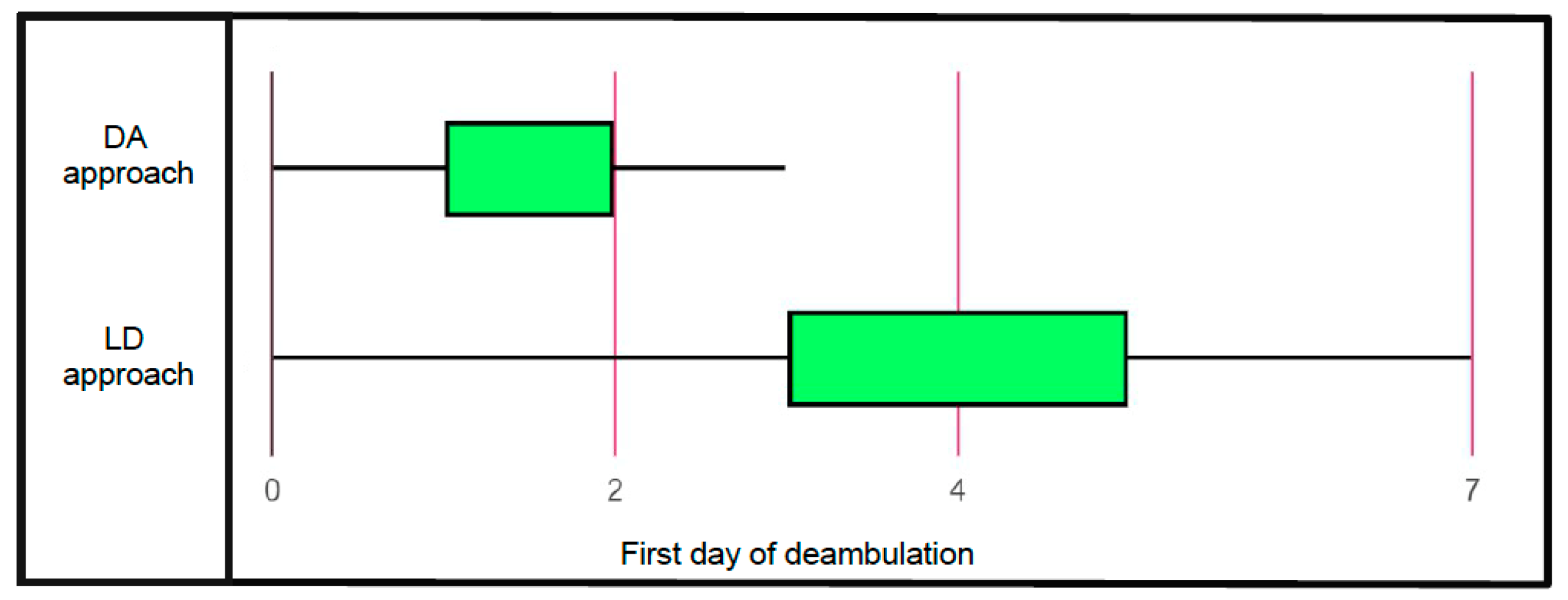
{kind=link}
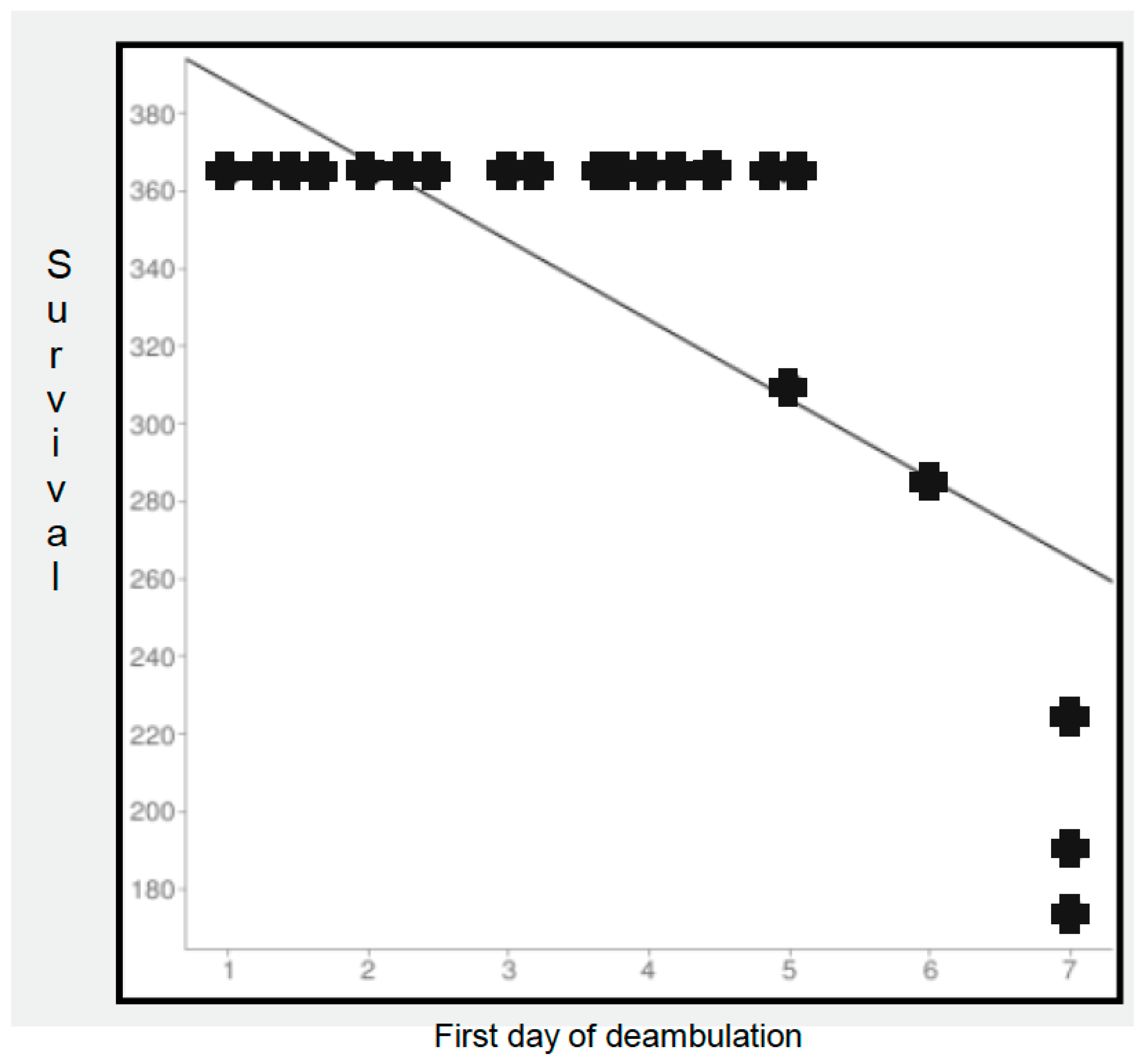
{kind=link}
| N = 92 | |
|---|---|
| Age (mean ± std dev) | 72.6 ± 7.3 |
| Gender | |
| Male | 38 |
| Female | 54 |
| BMI | 25.8 ± 3.1 |
| ASA | |
| 1 | 8 |
| 2 | 29 |
| 3 | 51 |
| 4 | 4 |
| Garden fracture | |
| 2 | 5 |
| 3 | 56 |
| 4 | 31 |
| Time trauma/surgery (hours) | 57.1 ± 13.5 |
| Operative time (min) | 118 ± 14.9 |
| Intraoperative complications | |
| Surg acetabular protrusion | 4 |
| Femoral fracture | 2 |
| Surgical approach | |
| DA | 40 |
| LD | 52 |
| Surgical training | |
| AR | 43 |
| non-AR | 49 |
| Anesthesia type | |
| General | 34 |
| Spinal | 58 |
| Component positioning | |
| Correct | 75 |
| Incorrect | |
| Stem | |
| Varus | 3 |
| Acetabular | |
| Inclination | 7 |
| Anteversion | 5 |
| OR | 95% Confidence Interval | p | |
|---|---|---|---|
| Age | 0.781 | 0.314–0.827 | 0.083 |
| Female | 1.026 | 0.526–1.331 | 0.645 |
| BMI | 0.890 | 0.673–0.995 | 0.286 |
| ASA < 3 | 0.762 | 0.540–0.913 | 0.109 |
| Time trauma/surgery | 1.153 | 0.732–1.385 | 0.622 |
| Operative time | 0.807 | 0.691–1.469 | 0.581 |
| No intraoperative complications | 0.996 | 0.503–1.542 | 0.875 |
| DA surgical approach | 0.291 | 0.106–0.374 | 0.026 |
| AR-trained surgeon | 0.467 | 0.238–0.782 | 0.171 |
| Spinal anesthesia | 0.957 | 0.580–1.463 | 0.602 |
| Correct component positioning | 0.554 | 0.296–0.831 | 0.185 |
| OR | 95% Confidence Interval | p | |
|---|---|---|---|
| Age | 0.862 | 0.764–1.351 | 0.098 |
| Female | 0.615 | 0.391–1.227 | 0.189 |
| BMI | 0.928 | 0.732–1.416 | 0.352 |
| ASA < 3 | 0.349 | 0.206–0.518 | 0.034 |
| Time trauma/surgery | 0.786 | 0.365–1.191 | 0.432 |
| Operative time | 0.883 | 0.475–1.364 | 0.502 |
| No intraoperative complications | 0.512 | 0.256–0.729 | 0.091 |
| DA surgical approach | 0.447 | 0.315–0.580 | 0.026 |
| AR-trained surgeon | 0.546 | 0.129–0.866 | 0.312 |
| Spinal anesthesia | 0.904 | 0.563–1.672 | 0.633 |
| Correct component positioning | 0.735 | 0.306–1.147 | 0.567 |
| OR | 95% Confidence Interval | p | |
|---|---|---|---|
| Age | 0.741 | 0.489–1.266 | 0.659 |
| Female | 0.562 | 0.273–0.984 | 0.416 |
| BMI | 0.397 | 0.137–0.558 | 0.083 |
| ASA < 3 | 0.604 | 0.218–1.165 | 0.687 |
| Time trauma/surgery | 0.856 | 0.649–1.453 | 0.705 |
| Operative time | 0.915 | 0.807–1.511 | 0.842 |
| No intraoperative complications | 0.789 | 0.625–1.139 | 0.821 |
| DA surgical approach | 0.423 | 0.156–0.727 | 0.234 |
| AR-trained surgeon | 0.258 | 0.114–0.392 | 0.003 |
| Spinal anesthesia | 0.891 | 0.565–1.376 | 0.908 |
| Correct component positioning | 0.672 | 0.496–0.978 | 0.536 |
| Early deambulation completed | 0.218 | 0.129–0.564 | 0.095 |
| OR | 95% Confidence Interval | p | |
|---|---|---|---|
| Age | 0.471 | 0.206–0.872 | 0.247 |
| Female | 0.692 | 0.491–0.958 | 0.535 |
| BMI | 0.543 | 0.387–0.824 | 0.394 |
| ASA < 3 | 0.367 | 0.194–0.525 | 0.021 |
| Time trauma/surgery | 0.825 | 0.657–1.237 | 0.780 |
| Operative time | 0.904 | 0.722–1.369 | 0.829 |
| No intraoperative complications | 0.786 | 0.315–1.196 | 0.452 |
| DA surgical approach | 0.217 | 0.108–0.313 | 0.096 |
| AR-trained surgeon | 0.338 | 0.239–0.482 | 0.081 |
| Spinal anesthesia | 1.026 | 0.524–1.361 | 0.755 |
| Correct component positioning | 0.487 | 0.280–0.712 | 0.274 |
| Early deambulation completed | 0.259 | 0.148–0.306 | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiavi, P.; Pogliacomi, F.; Bergamaschi, M.; Ceccarelli, F.; Vaienti, E. Evaluation of Outcome after Total Hip Arthroplasty for Femoral Neck Fracture: Which Factors Are Relevant for Better Results? J. Clin. Med. 2024, 13, 1849. https://doi.org/10.3390/jcm13071849
Schiavi P, Pogliacomi F, Bergamaschi M, Ceccarelli F, Vaienti E. Evaluation of Outcome after Total Hip Arthroplasty for Femoral Neck Fracture: Which Factors Are Relevant for Better Results? Journal of Clinical Medicine. 2024; 13(7):1849. https://doi.org/10.3390/jcm13071849
Chicago/Turabian StyleSchiavi, Paolo, Francesco Pogliacomi, Matteo Bergamaschi, Francesco Ceccarelli, and Enrico Vaienti. 2024. "Evaluation of Outcome after Total Hip Arthroplasty for Femoral Neck Fracture: Which Factors Are Relevant for Better Results?" Journal of Clinical Medicine 13, no. 7: 1849. https://doi.org/10.3390/jcm13071849
APA StyleSchiavi, P., Pogliacomi, F., Bergamaschi, M., Ceccarelli, F., & Vaienti, E. (2024). Evaluation of Outcome after Total Hip Arthroplasty for Femoral Neck Fracture: Which Factors Are Relevant for Better Results? Journal of Clinical Medicine, 13(7), 1849. https://doi.org/10.3390/jcm13071849