
The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation
 , , ,
, , , 
Abstract
1. Introduction
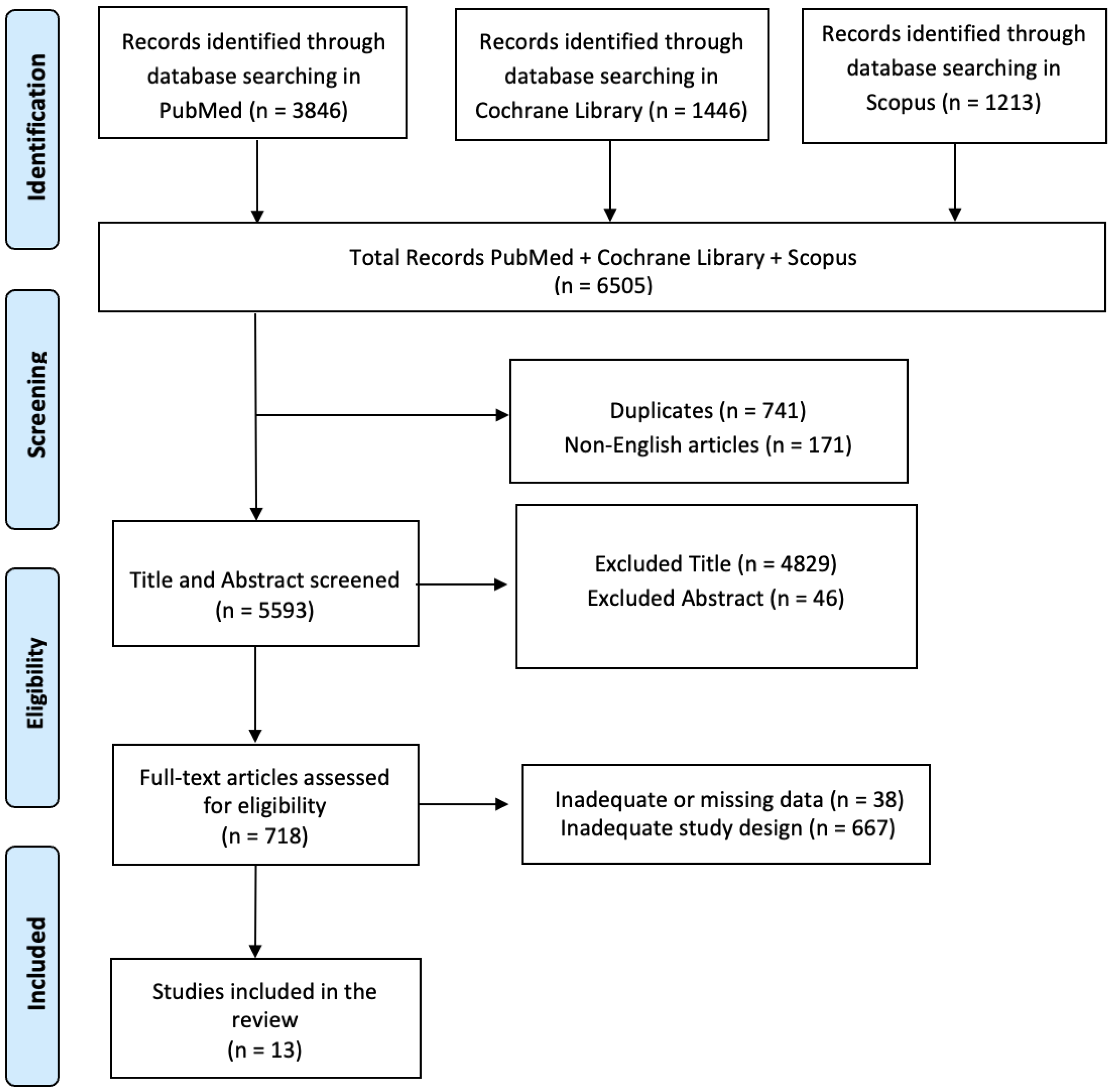
2. Materials and Methods
2.1. Search Strategy
2.2. PICO Evaluation
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Assess Quality of Included Studies—Risk of Bias
3. Results
3.1. QoL and Assessment in Patients with SCI
3.2. Rehabilitation, Comorbidities, and Functional Status in SCI
4. Discussion
Funding
Data Availability Statement
Conflicts of Interest
References
- American Spinal Injury Association. 2015. Available online: http://www.asia-spinalinjury.org (accessed on 9 October 2018).
- Khorasanizadeh, M.; Yousefifard, M.; Eskian, M.; Lu, Y.; Chalangari, M.; Harrop, J.S.; Jazayeri, S.B.; Seyedpour, S.; Khodaei, B.; Hosseini, M.; et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J. Neurosurg. Spine 2019, 30, 683–699. [Google Scholar] [CrossRef]
- Williams, R.; Murray, A. Prevalence of depression after spinal cord injury: A meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Lude, P.; Kennedy, P.; Elfström, M.; Ballert, C. Quality of life in and after spinal cord injury rehabilitation: A longitudinal multicenter study. Top. Spinal Cord Inj. Rehabil. 2014, 20, 197–207. [Google Scholar] [CrossRef]
- Middleton, J.; Tran, Y.; Craig, A. Relationship between quality of life and self-efficacy in persons with spinal cord injuries. Arch. Phys. Med. Rehabil. 2007, 88, 1643–1648. [Google Scholar] [CrossRef]
- Lidal, I.B.; Veenstra, M.; Hjeltnes, N.; Biering-Sørensen, F. Health-related quality of life in persons with long-standing spinal cord injury. Spinal Cord 2008, 46, 710–715, Erratum in Spinal Cord 2008, 46, 765. [Google Scholar] [CrossRef]
- Kortte, K.B.; Gilbert, M.; Gorman, P.; Wegener, S.T. Positive psychological variables in the prediction of life satisfaction after spinal cord injury. Rehabil. Psychol. 2010, 55, 40–47. [Google Scholar] [CrossRef]
- Geyh, S.; Ballert, C.; Sinnott, A.; Charlifue, S.; Catz, A.; Greve, J.M.D.; Post, M.W.M. Quality of life after spinal cord injury: A comparison across six countries. Spinal Cord 2013, 51, 322–326. [Google Scholar] [CrossRef]
- Shin, J.C.; Goo, H.R.; Yu, S.J.; Kim, D.H.; Yoon, S.Y. Depression and Quality of Life in Patients within the First 6 Months after the Spinal Cord Injury. Ann. Rehabil. Med. 2012, 36, 119–125. [Google Scholar] [CrossRef] [PubMed]
- van Leeuwen, C.M.; Post, M.W.; van Asbeck, F.W.; Bongers-Janssen, H.M.; van der Woude, L.H.; de Groot, S.; Lindeman, E. Life satisfaction in people with spinal cord injury during the first five years after discharge from inpatient rehabilitation. Disabil. Rehabil. 2012, 34, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.; Tran, Y.; Middleton, J. Psychological morbidity and spinal cord injury: A systematic review. Spinal Cord 2009, 47, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Mortenson, W.B.; Noreau, L.; Miller, W.C. The relationship between and predictors of quality of life after spinal cord injury at 3 and 15 months after discharge. Spinal Cord 2010, 48, 73–79. [Google Scholar] [CrossRef]
- Kennedy, P.; Lude, P.; Elfström, M.L.; Smithson, E. Sense of coherence and psychological outcomes in people with spinal cord injury: Appraisals and behavioural responses. Br. J. Health Psychol. 2010, 15 Pt 3, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P.; Lude, P.; Elfström, M.L.; Smithson, E. Appraisals, coping and adjustment pre and post SCI rehabilitation: A 2-year follow-up study. Spinal Cord 2012, 50, 112–118. [Google Scholar] [CrossRef]
- O’connor, P.J. Survival after spinal cord injury in Australia. Arch. Phys. Med. Rehabil. 2005, 86, 37–47. [Google Scholar] [CrossRef]
- Andresen, E.M.; Fouts, B.S.; Romeis, J.C.; Brownson, C.A. Performance of health-related quality-of-life instruments in a spinal cord injured population. Arch. Phys. Med. Rehabil. 1999, 80, 877–884. [Google Scholar] [CrossRef]
- Chapin, M.H.; Miller, S.M.; Ferrin, J.M.; Chan, F.; Rubin, E.S. Psychometric validation of a subjective well-being measure for people with spinal cord injuries. Disabil. Rehabil. 2004, 26, 1135–1142. [Google Scholar] [CrossRef]
- Dijkers, M.P. Individualization in quality of life measurement: Instruments and approaches. Arch. Phys. Med. Rehabil. 2003, 84 (Suppl. S2), S3–S14. [Google Scholar] [CrossRef] [PubMed]
- Dirzyte, A.; Perminas, A.; Biliuniene, E. Psychometric Properties of Satisfaction with Life Scale (SWLS) and Psychological Capital Questionnaire (PCQ-24) in the Lithuanian Population. Int. J. Environ. Res. Public Health 2021, 18, 2608. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.R.; the SCIRE Research Team; Noonan, V.K.; Sakakibara, B.M.; Miller, W.C. Quality of life instruments and definitions in individuals with spinal cord injury: A systematic review. Spinal Cord 2010, 48, 438–450. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A.; WHOQOL Group. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Can, G.; Durna, Z.; Aydiner, A. The validity and reliability of the Turkish version of the Quality of Life Index [QLI] (Cancer version). Eur. J. Oncol. Nurs. 2010, 14, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Almeida, L.d.O.; de Lima, A.; Sprizon, G.S.; Ilha, J. Measurement properties of assessment instruments of quality of life in people with spinal cord injury: A systematic review. J. Spinal Cord Med. 2023, 47, 15–50. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Wu, J.; Han, Y.; Zhao, F.-L.; Zhou, J.; Chen, Z.; Sun, H. Validation and comparison of EuroQoL-5 dimension (EQ-5D) and Short Form-6 dimension (SF-6D) among stable angina patients. Health Qual. Life Outcomes 2014, 12, 156. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saadat, S.; Javadi, M.; Divshali, B.S.; Tavakoli, A.H.; Ghodsi, S.M.; Montazeri, A.; Rahimi-Movaghar, V. Health-related quality of life among individuals with long-standing spinal cord injury: A comparative study of veterans and non-veterans. BMC Public Health 2010, 10, 6. [Google Scholar] [CrossRef]
- De Bruin, A.; Diederiks, J.; de Witte, L.; Stevens, F.; Philipsen, H. Assessing the responsiveness of a functional status measure: The Sickness Impact Profile versus the SIP68. J. Clin. Epidemiol. 1997, 50, 529–540. [Google Scholar] [CrossRef]
- Cook, K.F.; Teal, C.R.; Engebretson, J.C.; Hart, K.A.; Mahoney, J.S.; Robinson-Whelen, S.; Sherwood, A.M. Development and validation of Patient Reported Impact of Spasticity Measure (PRISM). J. Rehabil. Res. Dev. 2007, 44, 363–371. [Google Scholar] [CrossRef]
- Batool-Anwar, S.; Omobomi, O.; Quan, S. The effect of CPAP on HRQOL as measured by the Quality of Well-Being Self -Administered Questionaire (QWB-SA). Southwest J. Pulm. Crit. Care 2020, 20, 29–40. [Google Scholar] [CrossRef]
- Stanford, E.R.; Soden, R.; Bartrop, R.; Mikk, M.; Taylor, T.K.F. Spinal cord and related injuries after attempted suicide: Psychiatric diagnosis and long-term follow-up. Spinal Cord 2007, 45, 437–443. [Google Scholar] [CrossRef]
- Harris, E.C.; Barraclough, B.M.; Grundy, D.J.; Bamford, E.S.; Inskip, H.M. Attempted suicide and completed suicide in traumatic spinal cord injury. Case reports. Spinal Cord 1996, 34, 752–753. [Google Scholar] [CrossRef][Green Version]
- Kennedy, P.; Rogers, B.; Speer, S.; Frankel, H. Spinal cord injuries and attempted suicide: A retrospective review. Spinal Cord 1999, 37, 847–852. [Google Scholar] [CrossRef]
- Iyer, S.N.; Rothmann, T.L.; Vogler, J.E.; Spaulding, W.D. Evaluating outcomes of rehabilitation for severe mental illness. Rehabil. Psychol. 2005, 50, 43–55. [Google Scholar] [CrossRef]
- Dubayova, T.; Krokavcova, M.; Nagyova, I.; Rosenberger, J.; Gdovinova, Z.; Middel, B.; Groothoff, J.W.; van Dijk, J.P. Type D, anxiety and depression in association with quality of life in patients with Parkinson’s disease and patients with multiple sclerosis. Qual. Life Res. 2013, 22, 1353–1360. [Google Scholar] [CrossRef]
- Kasai, Y.; Suzuki, E.; Iwase, T.; Doi, H.; Takao, S. Type D personality is associated with psychological distress and poor self-rated health among the elderly: A population-based study in Japan. PLoS ONE 2013, 8, e77918. [Google Scholar] [CrossRef]
- Kennedy, P.; Lude, P.; Elfström, M.L.; Smithson, E.F. Psychological contributions to functional independence: A longitudinal investigation of spinal cord injury rehabilitation. Arch. Phys. Med. Rehabil. 2011, 92, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Mikula, P.; Nagyova, I.; Krokavcova, M.; Vitkova, M.; Rosenberger, J.; Szilasiova, J.; Gdovinova, Z.; Groothoff, J.W.; van Dijk, J.P. Do coping strategies mediate the association between Type D personality and quality of life among people with multiple sclerosis? J. Health Psychol. 2018, 23, 1557–1565. [Google Scholar] [CrossRef]
- Yamaguchi, D.; Izawa, A.; Matsunaga, Y. The Association of Depression with Type D Personality and Coping Strategies in Patients with Coronary Artery Disease. Intern. Med. 2020, 59, 1589–1595. [Google Scholar] [CrossRef]
- Kawanishi, C.Y.; Greguol, M. Physical activity, quality of life, and functional autonomy of adults with spinal cord injuries. Adapt. Phys. Act. Q. 2013, 30, 317–337. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Devillard, X.; Rimaud, D.; Roche, F.; Calmels, P. Effects of training programs for spinal cord injury. Ann. Réadapt. Méd. Phys. 2007, 50, 490–498, (In English and French). [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.S.; Forchheimer, M.; Heinemann, A.W.; Warren, A.M.; McCullumsmith, C. Assessment of the relationship of spiritual well-being to depression and quality of life for persons with spinal cord injury. Disabil. Rehabil. 2017, 39, 491–496. [Google Scholar] [CrossRef]
- Zwecker, M.; Heled, E.; Bluvstein, V.; Catz, A.; Bloch, A.; Zeilig, G. Assessment of the unmediated relationship between neurological impairment and health-related quality of life following spinal cord injury. J. Spinal Cord Med. 2022, 45, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Cijsouw, A.; Adriaansen, J.J.; Tepper, M.; Dijksta, C.A.; Van Linden, S.; De Groot, S.; Post, M.W.M. Associations between disability-management self-efficacy, participation and life satisfaction in people with long-standing spinal cord injury. Spinal Cord 2017, 55, 47–51. [Google Scholar] [CrossRef]
- Rivers, C.S.; Fallah, N.; Noonan, V.K.; Whitehurst, D.G.; Schwartz, C.E.; Finkelstein, J.A.; Craven, B.C.; Ethans, K.; O’Connell, C.; Truchon, B.C.; et al. Health Conditions: Effect on Function, Health-Related Quality of Life, and Life Satisfaction After Traumatic Spinal Cord Injury. A Prospective Observational Registry Cohort Study. Arch. Phys. Med. Rehabil. 2018, 99, 443–451. [Google Scholar] [CrossRef]
- Kunz, S.; Carrard, V.; Aparicio, M.G.; Scheel-Sailer, A.; Fekete, C.; Lude, P.; Post, M.W.M.; Westphal, M. Longitudinal measurement invariance of the international spinal cord injury quality of life basic data set (SCI-QoL-BDS) during spinal cord injury/disorder inpatient rehabilitation. Qual. Life Res. 2022, 31, 1247–1256. [Google Scholar] [CrossRef]
- Migliorini, C.; Callaway, L.; New, P. Preliminary investigation into subjective well-being, mental health, resilience, and spinal cord injury. J. Spinal Cord Med. 2013, 36, 660–665. [Google Scholar] [CrossRef]
- Eroğlu, S.; Solak, S.; Dündar, Ü. The association of Type D personality with functional outcomes, quality of life and neuropathic pain in persons with spinal cord injury. Spinal Cord 2022, 60, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Siddiqui, S.; Slocum, C.S.; Goldstein, R.; Zafonte, R.D.; Schneider, J.C. Assessing the Ability of Comorbidity Indexes to Capture Comorbid Disease in the Inpatient Rehabilitation Spinal Cord Injury Population. Arch. Phys. Med. Rehabil. 2020, 101, 1731–1738. [Google Scholar] [CrossRef] [PubMed]
- Capossela, S.; Landmann, G.; Ernst, M.; Stockinger, L.; Stoyanov, J. Assessing the Feasibility of a Multimodal Approach to Pain Evaluation in Early Stages after Spinal Cord Injury. Int. J. Mol. Sci. 2023, 24, 11122. [Google Scholar] [CrossRef]
- Harkema, S.J.; Shogren, C.; Ardolino, E.; Lorenz, D.J. Assessment of Functional Improvement without Compensation for Human Spinal Cord Injury: Extending the Neuromuscular Recovery Scale to the Upper Extremities. J. Neurotrauma 2016, 33, 2181–2190. [Google Scholar] [CrossRef]
- Hodel, J.; Ehrmann, C.; Stucki, G.; Bickenbach, J.E.; Prodinger, B.; the SwiSCI Study Group. Examining the complexity of functioning in persons with spinal cord injury attending first rehabilitation in Switzerland using structural equation modelling. Spinal Cord 2020, 58, 570–580, Erratum in Spinal Cord 2020, 58, 630. [Google Scholar] [CrossRef]
- Hodel, J.; Ehrmann, C.; Scheel-Sailer, A.; Stucki, G.; Bickenbach, J.E.; Prodinger, B. Identification of Classes of Functioning Trajectories and Their Predictors in Individuals with Spinal Cord Injury Attending Initial Rehabilitation in Switzerland. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100121. [Google Scholar] [CrossRef]
- Scivoletto, G.; Marcella, M.; Floriana, P.; Federica, T.; Marco, M. Impact of complications at admission to rehabilitation on the functional status of patients with spinal cord lesion. Spinal Cord 2020, 58, 1282–1290. [Google Scholar] [CrossRef]
- Post, M.W.; Van Dijk, A.J.; Van Asbeck, F.W.; Schrijvers, A.J. Life satisfaction of persons with spinal cord injury compared to a population group. Scand. J. Rehabil. Med. 1998, 30, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.P. Reporting of “quality of life”: A systematic review and quantitative analysis of research publications in palliative care journals. Indian J. Palliat. Care 2012, 18, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.; Nissim, E.N.; Wood, K.; Hwang, K.; Tulsky, D. Objective and subjective handicap following spinal cord injury: Interrelationships and predictors. J. Spinal Cord Med. 2002, 25, 11–22. [Google Scholar] [CrossRef]
- Gill, T.M.; Feinstein, A.R. A critical appraisal of the quality of quality-of-life measurements. JAMA 1994, 272, 619–626. [Google Scholar] [CrossRef]
- Dijkers, M. Measuring quality of life: Methodological issues. Am. J. Phys. Med. Rehabil. 1999, 78, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, B.; Manigandan, C.; Macaden, A.; Tharion, G.; Bhattacharji, S. Re-examining the psychology of spinal cord injury: A meaning centered approach from a cultural perspective. Spinal Cord 2001, 39, 323–326. [Google Scholar] [CrossRef]
- Najman, J.M.; Levine, S. Evaluating the impact of medical care and technologies on the quality of life: A review and critique. Soc. Sci. Med. Part F Med. Soc. Ethics 1981, 15, 107–115. [Google Scholar] [CrossRef]
- Walsh, P. Tetraplegics and the justice of resource allocation. Paraplegia 1993, 31, 143–146. [Google Scholar] [CrossRef][Green Version]
- Kennedy, P.; Rogers, B. Reported quality of life of people with spinal cord injuries: A longitudinal analysis of the first 6 months post-discharge. Spinal Cord 2000, 38, 498–503. [Google Scholar] [CrossRef]
- Nakamura, Y. Working ability of the paraplegics. Spinal Cord 1973, 11, 182–193. [Google Scholar] [CrossRef]
- Goldberg, G.; Shephard, R.J. Personality profiles of disabled individuals in relation to physical activity patterns. J. Sports Med. Phys. Fit. 1982, 22, 477–484. [Google Scholar]
- Jackson, R.W. Sport for the spinal paralysed person. Paraplegia 1987, 25, 301–304. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rohe, D.E.; Athelstan, G.T. Vocational interests of persons with spinal cord injury. J. Couns. Psychol. 1982, 29, 283–291. [Google Scholar] [CrossRef]
- Lollar, D.J.; Ericson, G.D. Factors Affecting Learning among Spinal Cord Injured Patients. In Proceedings of the 96th Annual Meeting, American Psychological Association, Atlanta, GA, USA, 14 August 1988. [Google Scholar]
- Berry, J.W.; Elliott, T.R.; Rivera, P. Resilient, undercontrolled, and overcontrolled personality prototypes among persons with spinal cord injury. J. Pers. Assess. 2007, 89, 292–302. [Google Scholar] [CrossRef]
- Rohe, D.E.; Krause, J. Stability of interests after severe physical disability: An 11-year longitudinal study. J. Vocat. Behav. 1998, 52, 45–58. [Google Scholar] [CrossRef]
- Thorn, B.E.; Pence, L.B.; Ward, L.C.; Kilgo, G.; Clements, K.L.; Cross, T.H.; Davis, A.M.; Tsui, P.W. A randomized clinical trial of targeted cognitive behavioral treatment to reduce catastrophizing in chronic headache sufferers. J. Pain 2007, 8, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Arkowitz, H.; Burke, B.L. Motivational interviewing as an integrative framework for the treatment of depression. In Motivational Interviewing in the Treatment of Psychological Problems; Arkowitz, H., Westra, H.A., Miller, W.R., Rollnick, S., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 145–272. [Google Scholar]
- Rollnick, S.; Miller, W.R.; Butler, C.C. Motivational Interviewing in Health Care: Helping Patients Change Behavior; Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Schoo, A. Motivational interviewing in the prevention and management of chronic disease: Improving physical activity and exercise in line with choice theory. Int. J. Real. Ther. 2008, 27, 26–29. [Google Scholar]


{kind=link}
| Study | Selection | Comparability | Outcome Assessment | Total Score |
|---|---|---|---|---|
| Wilson et al., 2017 [43] | 2 | 2 | 1 | 5 |
| Zwecker et al., 2022 [44] | 2 | 1 | 2 | 5 |
| Cijsouw et al., 2017 [45] | 2 | 1 | 1 | 4 |
| Rivers et al., 2018 [46] | 2 | 2 | 2 | 6 |
| Kunz et al., 2022 [47] | 2 | 1 | 1 | 4 |
| Migliorini et al., 2013 [48] | 0 | 1 | 2 | 3 |
| Eroglu et al., 2022 [49] | 1 | 1 | 2 | 4 |
| Huang et al., 2020 [50] | 3 | 2 | 1 | 6 |
| Capossela et al., 2023 [51] | 0 | 1 | 2 | 3 |
| Harkema et al., 2016 [52] | 1 | 2 | 2 | 4 |
| Hodel et al., 2020 [53] | 2 | 2 | 1 | 5 |
| Hodel et al., 2021 [54] | 3 | 1 | 1 | 4 |
| Scivoletto et al., 2020 [55] | 1 | 1 | 1 | 3 |
| Author | Aim | Study Design/Intervention | Treatment Period | Sample Size | Outcomes Measures | Main Findings | Study Limitations | Statistical Analyses |
|---|---|---|---|---|---|---|---|---|
| Wilson et al., 2017 [43] | To determine the relationship between mental well-being, demographic characteristics, QoL, and depressive symptoms after SCI. | Randomized controlled trial. | Not specified. | 210 individuals with SCI. | PHQ-9, FACIt-Sp, Neuro-QOL, PAWB, PANAS. | Spirituality, as measured by FACIT-Sp, is strongly associated with QoL and the likelihood of MDD. Spirituality assessments should be carried out using more traditional psychological measures for better treatment. | This study is limited by its sample. It is unclear whether the dynamics of QOL and depression in this sample reflect the dynamics of the SCI population as a whole. In addition, this study does not address the causal nature of the observed relationships. | Descriptive statistics and tests of association (Pearson correlation, t-test, analysis of variance, chi-square test, etc.) were used to examine the relationship between sample attributes and survey results, and ultimately assess which attributes should be included in the multivariate analysis as adjustment factors. |
| Zwecker et al., 2022 [44] | To evaluate the unmediated relationship between neurologic impairment and QoL in patients with SCI in early post-acute and long-term rehabilitation settings. | An observational, prospective, cross-sectional study. | Not specified. | 156 adults with SCI. | WHOQOL-BREF, ASIA, AIS, SWLS, LISAT-9, PWI. | WHOQOL-BREF differentiated between tetraplegic and paraplegic groups, but not between complete and incomplete injury groups; QoL in the early post-acute rehabilitation period was significantly higher in paraplegics than in tetraplegics. | The generalizability of the results of this study is limited by the sampling technique. This is because only SCI participants who voluntarily attended outpatient follow-up were included in the chronic group. These patients are more likely to have medical comorbidities that may unidirectionally affect HRQoL. | Binomial Logistic Regression Analysis was performed to determine which questionnaire score most effectively differentiates between groups based on injury level (paraplegic vs. quadriplegic), setting (inpatient vs. outpatient), and injury type (complete vs. incomplete). The dependent variable in this analysis was the scale used for classification, and the independent variable was the QoL questionnaire. |
| Cijsouw et al., 2017 [45] | To examine DMSE and its correlates across different life domains in a large sample of Dutch people with long-term SCI. | Cross-sectional study. | Between November 2011 and February 2014. | 261 individuals. | UW-SES-6. | DMSE is a psychological resource associated with higher engagement and life satisfaction after SCI. The UWSES-6 is a simple and easy-to-use measure of this psychological resource. | The limitations of this study stem from the inclusion criteria. The study sample predominantly consists of patients with traumatic complete SCI, and these patients acquired an SCI at a relatively young age. This affects the extent to which the results of this study can be generalized to all patients with SCI. | The relationships between UW-SES-6 scores and other variables were analyzed using t-tests or analysis of variance for categorical variables and Pearson correlation coefficient for continuous variables. A correlation coefficient of 0.30 was interpreted as weak, 0.30–0.50 as moderate, and up to 0.50 as strong. |
| Rivers et al., 2018 [46] | To analyze the relationship between injury, demographic and environmental factors, and function, HRQoL and life satisfaction in persons with traumatic SCI. | Prospective observational registry cohort study. | From 2004 to 2014. | 340 participants. | FIM, HRQoL, PCS, MCS, LISAT-11. | Higher age, higher severity of injury, cervical spine injury, and worse health status had a negative effect on FIM motor scores, while employment had a positive effect. Higher age, lower level of education, more serious injury and worse health status were negatively correlated with PCS. More health conditions were negatively correlated with lower MCS but positively correlated with poorer functioning. Being married and having higher functioning had a positive impact on Lisat-11, while worse health status had a negative impact. | Model results only apply to the 340 of the 580 individuals who met the study inclusion criteria and for whom all outcome data were available; outcome data were not imputed because there was a sufficient sample size to use only real-world data. | Path analysis was performed using Mplus version. Starting from a saturated model, a backward selection process was used to remove associations of non-significant variables. The goodness of fit of the model was assessed with five fit indices: the chi-square test (p > 0.05 is considered a good fit), root mean square error of approximation (<0.05 was considered a close fit, and an upper value of 0.080 was considered a reasonable fit), the 39 comparative fit index and the Tucker–Lewis Index (value > 0.95 × 1.0 indicates a good fit of 40, where the model is close to the study data), and standardized root mean square residual difference (<0.08 recommended). |
| Kunz et al., 2022 [47] | Validation of the internal consistency and longitudinal measurement invariance of the SCI-QoL-BDS in SCI and disability patients undergoing initial inpatient rehabilitation. | Prospective observational cohort Study. | Between May 2013 and January 2021. | 218 participants. | SCI-QoL-BDS. | The SCI-QoL-BDS is a consistent and valid measure that is used to assess QoL in people undergoing inpatient rehabilitation for the first time due to SCI/disability. However, to account for potential variations in response, it is recommended to use a latent variable framework rather than a mean score when examining longitudinal changes in the measures. | The longitudinal measurement invariance of the SCI-QoL-BDS has been examined in the inpatient rehabilitation of SCI patients. Therefore, it is unclear whether similar results would have emerged if measurement time points in community settings had been included. The post-hoc study of partial invariance at the intercept level is a data-driven approach. When comparing participant and non-participant characteristics with the existing data, the current study showed a slight selection bias. | Frequency statistics were used to describe the characteristics of the study sample and the SCI-QoL-BDS items and total scores. To test the internal consistency of the SCI-QoL-BDS, McDonald’s omega, Cronbach’s alpha, and corrected item–total correlations were calculated for each time point. Item–total correlations were calculated for each time point (T1, T2, T3). The longitudinal measurement invariance of the SCI-QoL-BDS was examined using cross-factor analysis. |
| Migliorini et al., 2013 [48] | To test whether people whose subjective well-being returns to a normal homeostatic range after SCI are more resilient and therefore less at risk of emotional distress in the long term. | Longitudinal study. | Not specified. | Not specified. | COMQoL-A5), PWI, DASS-21. | Patients with chronic SCI may be vulnerable to mental health problems even if they have previously demonstrated good resilience and subjective well-being. Subjective well-being may not be stable after SCI. | The small sample size is a serious limitation of the study and restricts the ability to draw firm conclusions from the study results. In addition, the sampling method used for the purpose of this study may also have influenced the study results. | Cronbach’s alpha coefficient is 0.84. Subjective well-being was calculated as the average of the seven subjective QoL domains and converted into a percentage of the highest score of the scale. |
| Eroglu et al., 2022 [49] | The aim of this study was to examine the relationship between TDP and functional outcomes, HRQoL and neuropathic pain in people with SCI using binary and continuous analysis methods. | Cross-sectional study. | 12 months. | 105 persons with SCI. | FIM, HRQoL, DS-14, LANSS. | The mental component of HRQoL is associated with Type D in SCI patients in both analyses. Identifying potential differences is useful for the development and implementation of individual-specific goals in SCI rehabilitation. | The cross-sectional design of the study does not provide information on the course of type D patients over time. The small number of participants treated at a single center may limit the generalizability of the results to the entire population of SCI patients. The collection of limited demographic variables is also a limitation. | Categorical variables are expressed as the number and percentage of cases. Continuous data for normal distributions are presented as mean (standard deviation) unless otherwise stated. Chi-square tests were used to compare data on gender, injury severity, and the level and presence of neuropathic pain between D and non-D groups. |
| Huang et al., 2020 [50] | Examine whether commonly used comorbidity indicators and CMS comorbidities capture the comorbidities of acute trauma and non-traumatic SCI inpatient rehabilitation patients. | Retrospective cross-sectional study. | From 10 October 2015 to 31 December 2017. | 833 inpatients. | ICD-10-CM. | Commonly used comorbidity indices do not reflect the extent of comorbidity in SCI rehabilitation populations. This study suggests that alternative indicators are needed to capture the complexity of this population. | UDSMR records represent discharges from rehabilitation, not individual persons. This implies that an individual who was discharged more than once from an IRF would be represented more than once. | Descriptive statistics of demographic and medical data were calculated using Stata version 15.1 (StataCorp LLC, College Station, TX, USA). The study population was divided into traumatic and non-traumatic etiologies. For the total population, traumatic, and non-traumatic groups, comorbidity frequencies for each ICD-10-CM code were calculated as a percentage of the total number of discharges in each group. Comorbidity frequencies of above 1% were reported. |
| Capossela et al., 2023 [51] | This study will evaluate the feasibility of a multimodal pain assessment protocol in rehabilitation after SCI. | Cohort study. | From September 2017 to December 2018. | 53 patients | CW/QST, SCIPI. | The SCIPI has been shown to be effective in differentiating between nociceptive and neuropathic pain, with a progressive increase in severity over time. Descriptive statistical analysis showed no difference in QoL, but stress and depression decreased and anxiety increased after initial rehabilitation. | Successful SCI-related pain research requires the coordination of recruitment settings, time resources, and assessment protocols. Questionnaires were not always completed by patients. | In gene expression and immunoassay analyses, the nonparametric Wilcoxon signed-rank test was used as the variable of interest to compare T1 and T4. |
| Harkema et al., 2016 [52] | Explore the features of the expanded NRS, introduce and evaluate new scoring methods, and examine its relationship to other SCI outcome measures. | Prospective observational study. | 5 training sessions per week. | 152 participants. | ISNCSCI, NRS, 6MWT, 10MWT, MFR, BBS. | The new NRS score responded most to changes related to motor training. The expanded NRS appears to be a valuable tool for measuring functional recovery from SCI. | The analysis does not represent a formal psychometric evaluation of the properties of the updated NRS. In particular, the added arm and shoulder items require reliability testing and a formal NRS validity assessment rather than principal component analysis. | Baseline demographic and clinical characteristics were summarized as numbers and percentages for categorical data, means and standard deviations for continuous data. Associations between NRS scores, NRS stages, NRS empirical subscale scores, and other continuous functional and clinical measures were assessed by calculating marginal Pearson correlation coefficients for clustered data. |
| Hodel et al., 2020 [53] | To examine the relationship between activity, physical structure, and function, as well as their association with etiology, age, and gender during initial rehabilitation discharge in patients with SCI. | Cross-sectional study. | Not specified. | 390 participants with SCI. | ICF, ADL. | The structural model for optimism showed a good fit across all indicators, whereas the models for anxiety, depression, and self-esteem showed conflicting fit indicators for each. | Invariance in the measurement model and group differences in the structural model could not be detected. Small sample size. | SEM was used to examine the indirect effects of physical structure and function on independence in ADL performance through the mental functions of anxiety, depression, optimism, and self-esteem, separately for each mental function. |
| Hodel et al., 2021 [54] | To identify functional trajectory classes in SCI patients undergoing initial rehabilitation after injury and to examine the potential determinants of class membership to inform clinical planning of the rehabilitation process. | Longitudinal cohort study. | Between May 2013 and September 2019. | 748 individuals. | SCIM III. | The mean predicted functional trajectories by class were stable high functioning (n = 307; 41.04%), early functional recovery (n = 39; 5.21%), moderate functional recovery (n = 287; 38.37%), and slow functional recovery (n = 115; 15.37%). Multinomial logistic regression results showed that age, level of injury, severity of injury, and ventilator assistance were strong predictors that differentiated the functional trajectory classes defined in this sample. | Selection bias may have occurred. This was due to the exclusion of individuals with fewer than two observations. Country-specific differences in clinical rehabilitation practices (e.g., availability, appropriateness, comprehensiveness, and duration of inpatient rehabilitation) may further limit the generalizability of the results. | LPMMs were used to determine the number of different functional trajectory classes within the current sample of individual interval-based SCIM III total score trajectories. |
| Scivoletto et al., 2020 [55] | The aim of the study was to evaluate the impact of complications at admission on the functional status of patients with SCI. | Retrospective cohort study. | Between 1996 and 2020. | 207 patients. | SCIM, RMI, WISCI. | Patients with complications on admission are more likely to have traumatic lesions. Patients without complications had significantly better functional status at admission and discharge compared to patients with complications. | The study was initiated in 1996 and only the associated lesions and complications were included. Both associated lesions and complications were simply classified as present/absent, without any assessment of severity that could make a clear difference. | Descriptive data analysis: descriptive values expressed as mean + SD were provided for all continuous clinical data. Paired data were analyzed by paired t-test; McNemar’s chi-square test was applied to assess split differences. |
| QoL Measures in SCI Patients | Description/Structure |
|---|---|
| Subjective Tools | |
| Satisfaction With Life Scale (SWLS) [19] | Assess life satisfaction comprehensively, encapsulating a global perspective of an individual’s values. Due to the open-ended nature of the questions, the scale proves suitable for adults from diverse backgrounds, acknowledging the potential for varied interpretations. It is best suited for use in non-clinical populations. Subjective well-being is conceptualized as consisting of two main components: an affective/emotional component and a judgmental/cognitive component; the SWLS is designed to measure the judgmental component. It is structured into five items: a 7-point Likert Scale from “1” (strongly disagree) to “7” (strongly agree). |
| Sense of Well-Being Index (SWBI) [20] | Addresses a subjective index of QoL for people with disabilities during work rehabilitation, addresses successful rehabilitation beyond objective employment outcomes. It assesses QoL in people with SCI using four factors (financial, family and social, psychological, and physical well-being). It is structured into 26 items: a 4-point Likert scale from “1” (strongly disagree) to “4” (strongly agree). |
| World Health Organization Quality of Life (WHOQOL-BREF) [21] | An instrument that aligns conceptually with the World Health Organization (WHO) definition of Quality of Life (QoL), encompassing domains such as physical health/capacity, psychological health/well-being, social relationships, environment, overall QoL, and general health. It assesses QoL in the context of personal culture, values, personal goals, standards, and concerns. It is structured into 26 items: a 5-point Likert scale from “1” to “5”. |
| Quality of Life Index (QLI) [22] | The QLI is a self-report scale meticulously crafted to assess subjective QoL by gauging satisfaction across various life domains. This instrument takes into account both satisfaction and perceived importance within four distinct domains: health and functioning, psychological and spiritual well-being, social and economic aspects, and family dynamics. It is structured into 32–37 items: a 6-point Likert scale for importance and for satisfaction, from “1” (very dissatisfied) to “6” (very satisfied). |
| Quality of Life Profile for Adults with Physical Disabilities (QOLP-PD) [23] | A holistic approach to QoL empowers individuals, recognizing that certain QoL elements are shared by both individuals with and without disabilities, yet acknowledging that each may address these issues in unique ways. It is structured into 102 items: a 5-point Likert scale from “1” (not all satisfied) to “5” (extremely satisfied) and from “1” (not important) to “5” (very important). |
| Short Form 36 (SF-36) [24] | A self-administered questionnaire, filled in by the patient, which aims to quantify the state of health and measure QoL related to health. It encompasses fundamental human values pertinent to QoL and well-being by considering individual domains and incorporating two overarching global components. It is structured into 36 items and divided into two summary scores: physical and mental component. |
| Short Form 12 (SF-12) [25] | The SF-12 stands as a self-report outcome measure designed to evaluate the influence of health on an individual’s daily life, commonly employed as an indicator of QoL. Deriving from its predecessor, the SF-36, which originated from the Medical Outcomes Study, the SF-12 was specifically developed to alleviate response burden by offering a more concise version. It is structured into 12 items. |
| Short Form 6-Disability (SF-6D) [26] | A six-dimensional health state classification derived from the SF-36 includes domains such as physical functioning, role limitation, social functioning, pain, mental health, and vitality. It is structured into 11 items with a range from “the worst health state” to “perfect or full health”. |
| Short Form 36 Veterans/SCI (SF-36V) [27] | Version of SF-36 designed for use in the disabled population. It is structured into 36 items, with physical and mental summary scores. |
| Sickness Impact Profile (SIP68) [28] | A generic health status measure that incorporates specific assessments of health-related changes in behavior associated with the execution of daily activities. It is structured into 68 items that assess somatic autonomy, mobility control, mobility range, social behavior, emotional stability, psychological autonomy and communication. |
| Patient-Reported Impact of Spasticity Measure (PRISM) [29] | A health-related subjective well-being scale featuring seven subscales aiming to evaluate the impact of spasticity linked to Spinal Cord Injury (SCI) on Quality of Life (QoL) from the patient’s perspective. These subscales encompass ‘social avoidance/anxiety’, ‘psychological agitation’, ‘daily activities’, ‘need for help/positioning’ and ‘need for intervention’, ‘social embarrassment’, and seven additional dimensions. This scale takes into account both negative and positive aspects related to spasticity. It is structured into 41 items: a 5-point Likert Scale from “0” (never true for me) to “4” (very often true for me). |
| Quality of Well-Being Questionnaire-SA (QWB-SA) [30] | A questionnaire to measure HRQOL with the following specifications: symptoms and problems; mobility; physical activity; social activity. It includes an assessment of symptoms in addition to various areas of functioning. It detects changes in samples of migraineurs, cataract surgery patients, mental health populations, and arthritis patients. It is structured into 71 items. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardile, D.; Calderone, A.; De Luca, R.; Corallo, F.; Quartarone, A.; Calabrò, R.S. The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation. J. Clin. Med. 2024, 13, 1820. https://doi.org/10.3390/jcm13061820
Cardile D, Calderone A, De Luca R, Corallo F, Quartarone A, Calabrò RS. The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation. Journal of Clinical Medicine. 2024; 13(6):1820. https://doi.org/10.3390/jcm13061820
Chicago/Turabian StyleCardile, Davide, Andrea Calderone, Rosaria De Luca, Francesco Corallo, Angelo Quartarone, and Rocco Salvatore Calabrò. 2024. "The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation" Journal of Clinical Medicine 13, no. 6: 1820. https://doi.org/10.3390/jcm13061820
APA StyleCardile, D., Calderone, A., De Luca, R., Corallo, F., Quartarone, A., & Calabrò, R. S. (2024). The Quality of Life in Patients with Spinal Cord Injury: Assessment and Rehabilitation. Journal of Clinical Medicine, 13(6), 1820. https://doi.org/10.3390/jcm13061820