

Oral Findings in Male Prisoners: A Systematic Review

 , , , , and
, , , , and
Abstract
1. Introduction
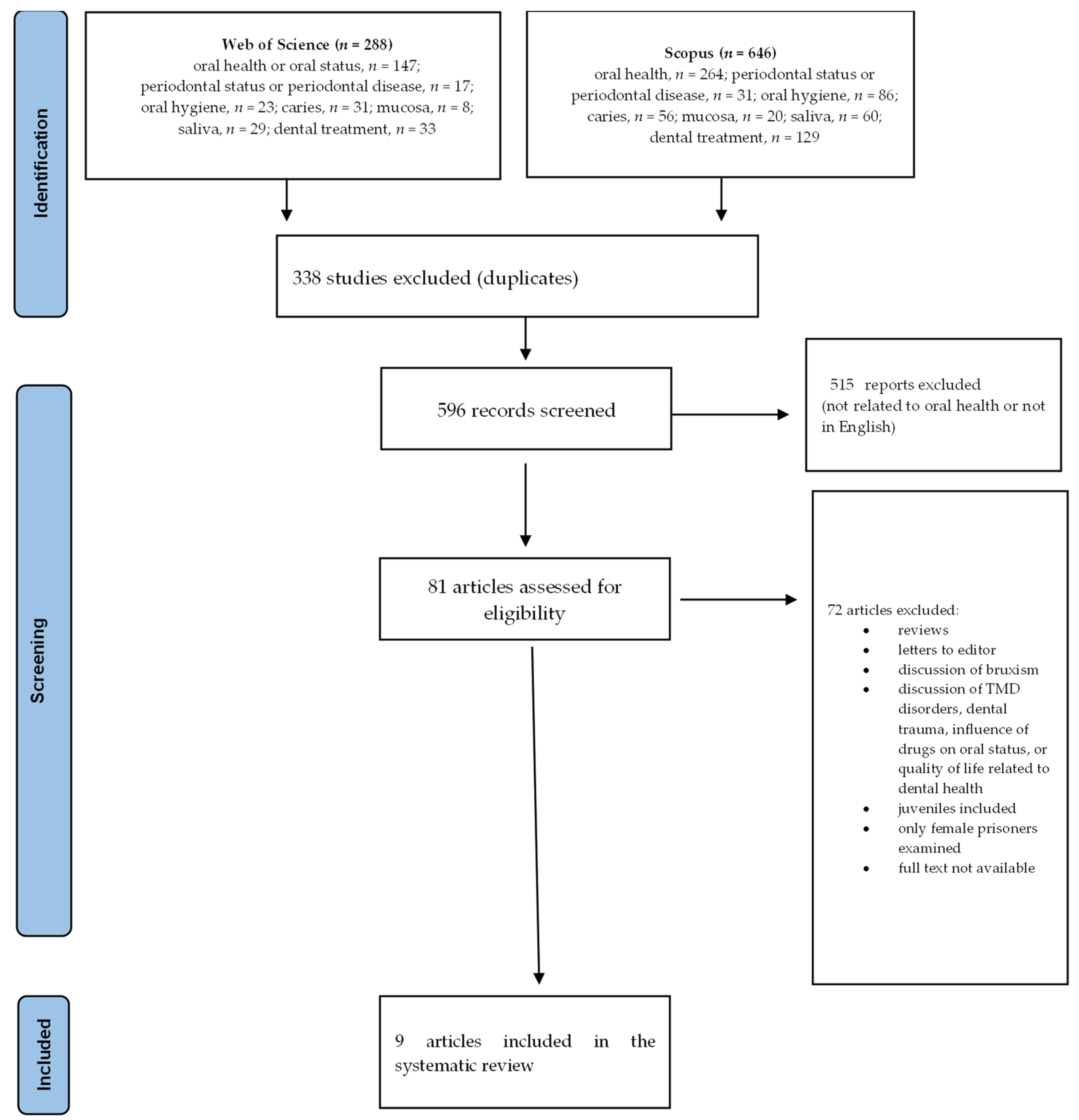
2. Materials and Methods
- <0.00—poor;
- 0.00–0.20—slight;
- 0.21–0.40—fair;
- 0.41–0.60—moderate;
- 0.61–0.80—substantial;
- 0.81–1.00—almost perfect.
- Substantive analysis
- Quality assessment
- 9–10 points: very good quality;
- 7–8 points: good quality;
- 5–6 points: satisfactory quality;
3. Results
3.1. Quality Assessment of Studies Included in the Systematic Review
3.2. Characteristics of the Included Studies
3.3. Oral Findings in Male Inmates on the Basis of the Studies Included in the Review

{kind=link}
| Reference Number | Hard Tissue Conditions |
|---|---|
| [15] | Prevalence of caries—97.5%; Mean decayed, missing, or filled teeth (DMFT)—5.26; One or more decayed (D) teeth—92.5%; One or more missing (M) teeth—57.1%; One or more filled (F) teeth—24.6%. |
| [7] | Percentages of prisoners with decayed (D) (90.2%) or missing (M) (80.5%) teeth were higher than those of the control group (D = 57%, M = 60.8%); Percentage of prisoners with filled (F) teeth was 31.7%, while for the controls, it was 50.6%; Median DMF was higher in prisoners than in controls (M = 8 vs. M = 5, p = 0.001). |
| [8] | Mean DMFT index value was 19.72; Mean values of each component were as follows: D (11.06 ± 5.37), M (7.20 ± 7.23), and F (1.46 ± 2.45). |
| [9] | 58.2% of males and 54.2% of females had decayed teeth; About 4.1% of males and 2.9% of females had filled teeth; Mean decayed, missing, and filled teeth index was 5.1 and 3.9 for female and male prisoners, respectively. |
| [10] | Mean DMFT and the values of its components in the entire group were as follows: DMFT = 16.8 (±8.9), D = 5.0 (±5.11), F = 6.9 (±5.15), and M = 4.7 (±6.01); In prisoners younger than 30 y., D = 4.8 (±5.76) and DMFT = 12.4 (±7.5); In prisoners older than 30 y., D = 5.1 (±4.80) and DMFT = 19.0 (±8.80). |
| [14] | Mean DMFT was 14.86 (±0.26), D = 6.48 (±2.18), M = 2.92 (±1.24), and F = 4.24 (±1.29). |
| [16] | Total DMFT score was 180 and average DMFT was 1.37 for the total prison population; Percentages of prisoners with decayed, missing, or filled teeth were as follows: 64.9%, 61.1%, and 7.7%, respectively. |
| [17] | 67% of the prisoners had decayed teeth or teeth missing as a result of caries. |
| [18] | Mean DMFT scores were as follows: overall, 5.92 (+4.65); 18 to 29 years, 4.14 (+3.49); 30 to 39 years, 6.17 (+4.19); 40 to 49 years, 9.08 (+5.38); and older than 50 years, 11.31 (+6.30). A statistically significant relationship was found between DMFT and age (p-value: 0.000). Decayed teeth were found in 64.34% of the participants, 71.85% recorded missing teeth, and filled teeth (FT) were noted in only 8.04% of the study sample. |
| Reference Number | Periodontal Status |
|---|---|
| [15] | CPI (community periodontal index) score of 2 in 39.3% of prisoners and 3 or 4 in 48.6% of prisoners; LOA score of 1 or 2 in 30.1% of prisoners and 4 in 1.7% of prisoners. |
| [10] | Percentages of CPI in entire group were as follows: CPI1—7%, CPI2—52%, CPI3—34%, and CPI4—7%; In those under 30, the scores were as follows: CPI1—2.9%, CPI2—67.7%, CPI3—26.5%, and CPI4—2.9%; In those 30 and over, the scores were as follows: CPI1—9.1, CPI2—49.9%, CPI3—25.3%, and CPI4—9.1%; The percentage of prisoners with BOP (bleeding on probing) was as follows: 0–1 sextans (A)—6%, 2–3 sextans (B)—6%, and 4–6 sextans (C)—88%; in those under 30, the percentages were as follows: A—3%, B—3%, and C—93.9%; in those 30 and over, the percentages were as follows: A—7.5%, B—7.5%, and C—85.1%. |
| [14] | Data were presented with regard to sex and time of incarceration: Males <5 years: CPI0—0, CPI1—5%, CPI2—36.3%, CPI3—33.7%, and CPI4—20%; Males >5 years: CPI0—0, CPI1—0, CPI2—22.1%, CPI3—33.7%, and CPI4—7%; Females <5 years: CPI0—0, CPI1—8%, CPI2—46.7%, CPI3—29.3%, and CPI4—12%; Females >5 years: CPI0—o, CPI1—1.8%, CPI2—29.1%, CPI3—32.7%, and CPI4—23.7%. |
| [17] | CPI0 was observed in 5.2% of participants, and CPI1–4 was observed in 94.8% of them. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rogalska, A.; Baranski, K.; Rachwaniec-Szczecinska, Z.; Holecki, T.; Bąk-Sosnowska, M. Assessment of Satisfaction with Health Service samong Prisoners—Descriptive Study. Healthcare 2022, 10, 548. [Google Scholar] [CrossRef]
- Rogala, D.; Banach, A.; Jachimowicz-Gaweł, D.; Skinder, Ż.; Leźnicka, M. Health care system for persons detained in prisons in Poland. Hygeia Public Health 2013, 48, 441–448. [Google Scholar]
- Clare, J.H. Dental health status, unmet needs and utilization of services in a cohort of adult felons at admission and after 3 years’ incarceration. J. Correct. Health Care 2002, 9, 65–76. [Google Scholar] [CrossRef]
- Sharma, A.; Parkar, S.; Gaur, A.; Bagri, B. Impact of incarceration on nutritional status and oral health among male inmates of central jail of Jaipur city, India. Rev. Esp. Sanid. Penit. 2020, 22, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.; Gonçalves, M.; Rompante, P.; Salazar, F.; Monteiro, L.; Pacheco, J.J.; Relvas, M. Assessment of Oral Health Status in a Prison Population in Northern Portugal. J. Clin. Exp. Dent. 2023, 15, e912–e919. [Google Scholar] [CrossRef] [PubMed]
- Skowroński, B.; Talik, E. Quality of Life and Its Correlates in People Serving Prison Sentences in Penitentiary Institutions. Int. J. Environ. Res. Public Health 2021, 18, 1655. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, R.M.F.; Al-Sulaimi, A.M.H.; Fadaak, A.H.; Balhaddad, A.A.; AlKhalfan, A.M.A.; El Tantawi, M.M.A.; Al-Ansari, A.A. Oral health amongst male inmates in Saudi prisons compared with that of a sample of general male population. S. Afr. Dent. J. 2017, 72, 402–407. [Google Scholar] [CrossRef]
- Cavalcanti, A.L.; Rodrigues, I.S.; Silveira, I.T.; de Oliveira, T.B.; Pinto, M.S.; Xavier, A.F.; de Castro, R.D.; Padilha, W.W.N. Dental Caries Experience and Use of dental Services among Brazilian Prisoners. Int. J. Environ. Res. Public Health 2014, 11, 12118–12128. [Google Scholar] [CrossRef] [PubMed]
- George, B.; John, J.; Saravanan, S.; Arumugham, I.M.; Johny, M.K. Dental caries status of inmates in central prison, Chennai, Tamil Nadu, India. J. Nat. Sci. Biol. Med. 2015, 6, s110–s112. [Google Scholar] [CrossRef]
- Vainionpää, R.; Peltokangas, A.; Leinonen, J.; Pesonen, P.; Laitala, M.L.; Antonnen, V. Oral health and oral health-related habits of Finnish prisoners. BDJ Open 2017, 3, 17006. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Herzog, R.; Alvaez-Pasquin, M.J.; Diaz, C.; Del Barrio, J.l.; Estrada, J.M.; Gil, A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Kondratyev, S.A.; Turkina, A.Y.; Franco, A.; Budina, T.V.; Ovsienko, A.G. Prevalence of oral diseases and the assessment of the simplified oral hygiene, Decayed-Missing-Filling and Community Periodontal Indices among inmates of the Russian Federation. Biosci. J. 2019, 35, 666–673. [Google Scholar] [CrossRef]
- Reddy, V.; Kondareddy, C.V.; Siddanna, S.; Manjunath, M. A survey on oral health status and treatment needs of life-imprisoned in central jails of Karnataka, India. Int. Dent. J. 2012, 62, 27–32. [Google Scholar] [CrossRef]
- Rinki, H.; Thomas, S.; Dagli, R.J.; Solanki, J.; Geetika, A. Prevalence of Dental Caries among Prisoners of Central Jail, Jodhpur City, Rajastan, India. World J. Dent. 2014, 5, 92–97. [Google Scholar]
- Akaji, E.A.; Ashiwaju, M.O. Oral Health Status of Sample of Prisoners in Enguru: A Disadvantaged Population. Ann. Med. Health Sci. Res. 2014, 4, 650–653. [Google Scholar] [CrossRef] [PubMed]
- Rabede, M.; Singh, S. Investigating dental caries rates amongst sentenced prisoners in KwaZulu-Natal South Africa. S. Afr. Dent. J. 2020, 75, 137–141. [Google Scholar]
- Favril, L.; Yu, R.; Hawton, K.; Fazel, S. Risk factors for self-harm in prison: A systematic review and meta-analysis. Lancet Psychiatry 2020, 7, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, R.W.; Story, A.; Hwang, S.W.; Nordentoft, M.; Luchenski, S.A.; Hartwell, G.; Tweed, E.J.; Lewer, D.; Vittal Katikireddi, S.; Hayward, A.C. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: A systematic review and meta-analysis. Lancet 2018, 391, 241–250. [Google Scholar] [CrossRef]
- Korkosz, R.; Trzcionka, A.; Mączkowiak, D.; Kiełbratowski, M.; Kuśka-Kiełbratowska, A.; Rahnama, M.; Tanasiewicz, M. Dental Treatment Needs of Male Inmates in Relation to the Analysis of Medical Databases. J. Clin. Med. 2024, 13, 858. [Google Scholar] [CrossRef] [PubMed]
- Trzcionka, A.; Twardawa, H.; Mocny-Pachońska, K.; Tanasiewicz, M. Periodontal Treatment Needs of Hemodialized Patients. Healthcare 2021, 9, 139. [Google Scholar] [CrossRef] [PubMed]

| Reference Number | Selection | Comparability | Outcome | Quality |
|---|---|---|---|---|
| 15 | 3 | 2 | 3 | GOOD |
| 7 | 3 | 1 | 2 | SATISFACTORY |
| 8 | 2 | 0 | 3 | SATISFACTORY |
| 18 | 3 | 1 | 3 | GOOD |
| 9 | 4 | 1 | 3 | GOOD |
| 10 | 2 | 1 | 3 | SATISFACTORY |
| 14 | 2 | 2 | 3 | GOOD |
| 16 | 4 | 2 | 3 | VERY GOOD |
| 17 | 4 | 1 | 0 | SATISFACTORY |
| Author, Title, and Year of Publication | Country | Participants/Materials | Statistical Analysis |
|---|---|---|---|
| Reddy et al., “A survey on oral health status and treatment needs of life-imprisoned inmates in central jails of Karnataka, India”, 2012 [15] | India | 800 prisoners; 722 males and 78 females | Arithmetic mean, standard deviation, chi-squared test, analysis of variance (ANOVA), and contingency coefficient. The Statistical Package for Social Sciences (SPSS) ver. 16 was used. |
| Bukhari et al., “Oral health amongst male inmates in Sudi prisons compared with that of a sample of the general male population”, 2017 [7] | Saudi Arabia | Study group: 82 male prisoners Control group: 79 males | Chi-squared test, Mann–Whitney U test, Spearman’s rho, binary logistic regression, odds ratio, and confidence intervals. Analyses were performed using SPSS ver. 17. |
| Cavalcanti et al., “Dental caries experience and use of dental services among Brazilian prisoners”, 2014 [8] | Brazil | 127 male prisoners | Pearson’s chi-squared test, Fischer’s exact test, and Kruskal–Wallis test. SPSS ver. 17 was used. |
| Radebe et al., “Investigating dental caries rates amongst sentenced prisoners in KwaZulu-Natal, South Africa”, 2020 [18] | South Africa | 373 prisoners; 333 males and 40 females | Standard deviation, frequency distribution, measures of central tendency, and Pearson’s chi-squared test. SPSS ver. 24 was used. |
| George et al., “Dental caries status of inmates in central prison, Chennai, Tamil Nadu, India”, 2015 [9] | India | 1060 inmates; 1025 males and 35 females | Independent t-test. Analysis was performed using IBM SPSS ver. 16. |
| Valnionpää et al.,” Oral health and oral health-related habits of Finnish prisoners”, 2017 [10] | Finland | 100 prisoners; 89 males and 11 females | Kappa value, means, minimum and maximum values, frequencies and distributions, Pearson’s chi-squared test, and Fischer’s exact test. Analyses were performed using SPSS ver. 22 (Chicago, IL, USA). |
| Kondratyev et al., “Prevalence of oral diseases and the assessment of the simplified oral hygiene, decayed-missing-filling and community periodontal indices among inmates of the Russian Federation”, 2019 [14] | Russia | 305 inmates; 175 males and 130 females | Pearson’s correlation coefficient and t-tests. SPSS ver. 16 was used. |
| Rinki et al., “Prevalence of dental caries among prisoners of central jail, Jodhpur city, Rajasthan, India”, 2014 [16] | India | 131 male prisoners | Descriptive statistics and chi-squared test. |
| Akaji et al., “Oral health status of a sample of prisoners in Enugu: a disadvantaged population”, 2014 [17] | Nigeria | 230 inmates; 224 males and 6 females | Percentages, standard deviation, and Spearman’s correlation rho. Data were analyzed using SPSS ver. 15 (Chicago, IL) and Graph Pad Prism for Windows, ver. 5 (San Diego, California). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korkosz, R.; Trzcionka, A.; Hildebrandt, T.; Kiełbratowski, M.; Kuśka-Kiełbratowska, A.; Rahnama, M.; Tanasiewicz, M. Oral Findings in Male Prisoners: A Systematic Review. J. Clin. Med. 2024, 13, 1736. https://doi.org/10.3390/jcm13061736
Korkosz R, Trzcionka A, Hildebrandt T, Kiełbratowski M, Kuśka-Kiełbratowska A, Rahnama M, Tanasiewicz M. Oral Findings in Male Prisoners: A Systematic Review. Journal of Clinical Medicine. 2024; 13(6):1736. https://doi.org/10.3390/jcm13061736
Chicago/Turabian StyleKorkosz, Rafał, Agata Trzcionka, Tomasz Hildebrandt, Maksymilian Kiełbratowski, Anna Kuśka-Kiełbratowska, Mansur Rahnama, and Marta Tanasiewicz. 2024. "Oral Findings in Male Prisoners: A Systematic Review" Journal of Clinical Medicine 13, no. 6: 1736. https://doi.org/10.3390/jcm13061736
APA StyleKorkosz, R., Trzcionka, A., Hildebrandt, T., Kiełbratowski, M., Kuśka-Kiełbratowska, A., Rahnama, M., & Tanasiewicz, M. (2024). Oral Findings in Male Prisoners: A Systematic Review. Journal of Clinical Medicine, 13(6), 1736. https://doi.org/10.3390/jcm13061736