
Effect of Sex, Age, and Cardiovascular Risk Factors on Aortoiliac Segment Geometry

 and
and
Abstract
1. Introduction
2. Patients and Methods
2.1. Selection of Participants
2.2. Image Processing
2.2.1. Arterial Segmentation
2.2.2. Arterial Geometry
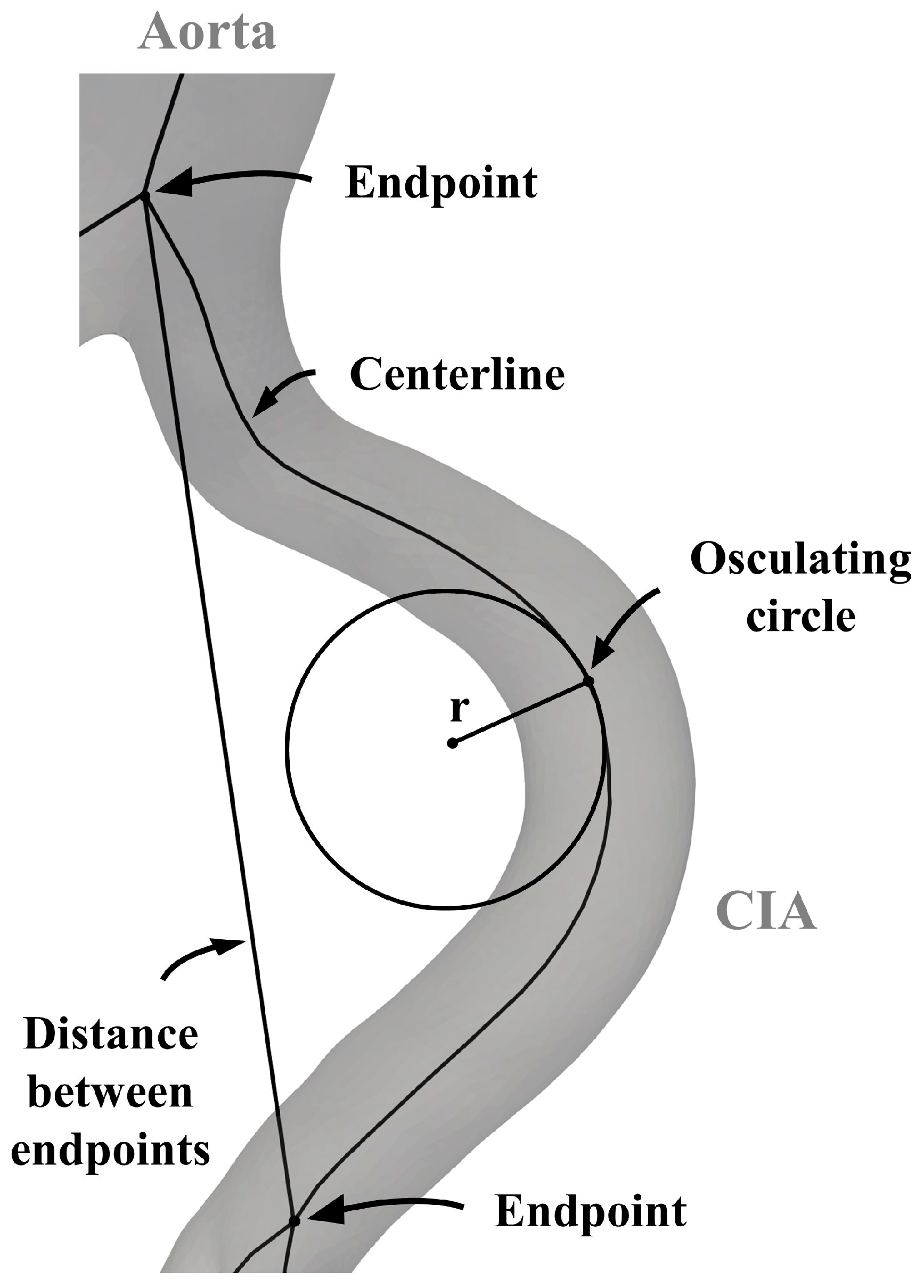
2.2.3. Arterial Elongation
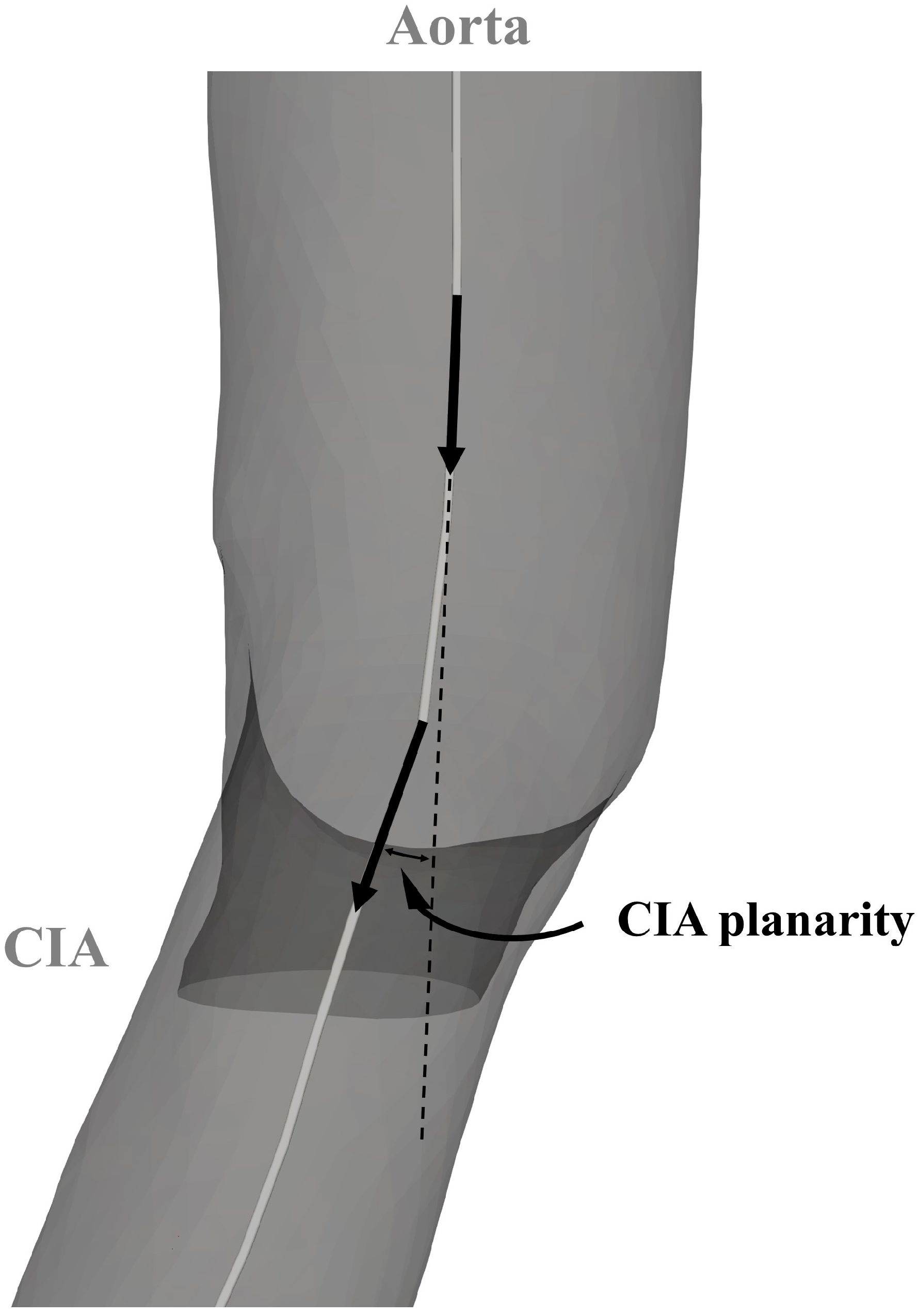
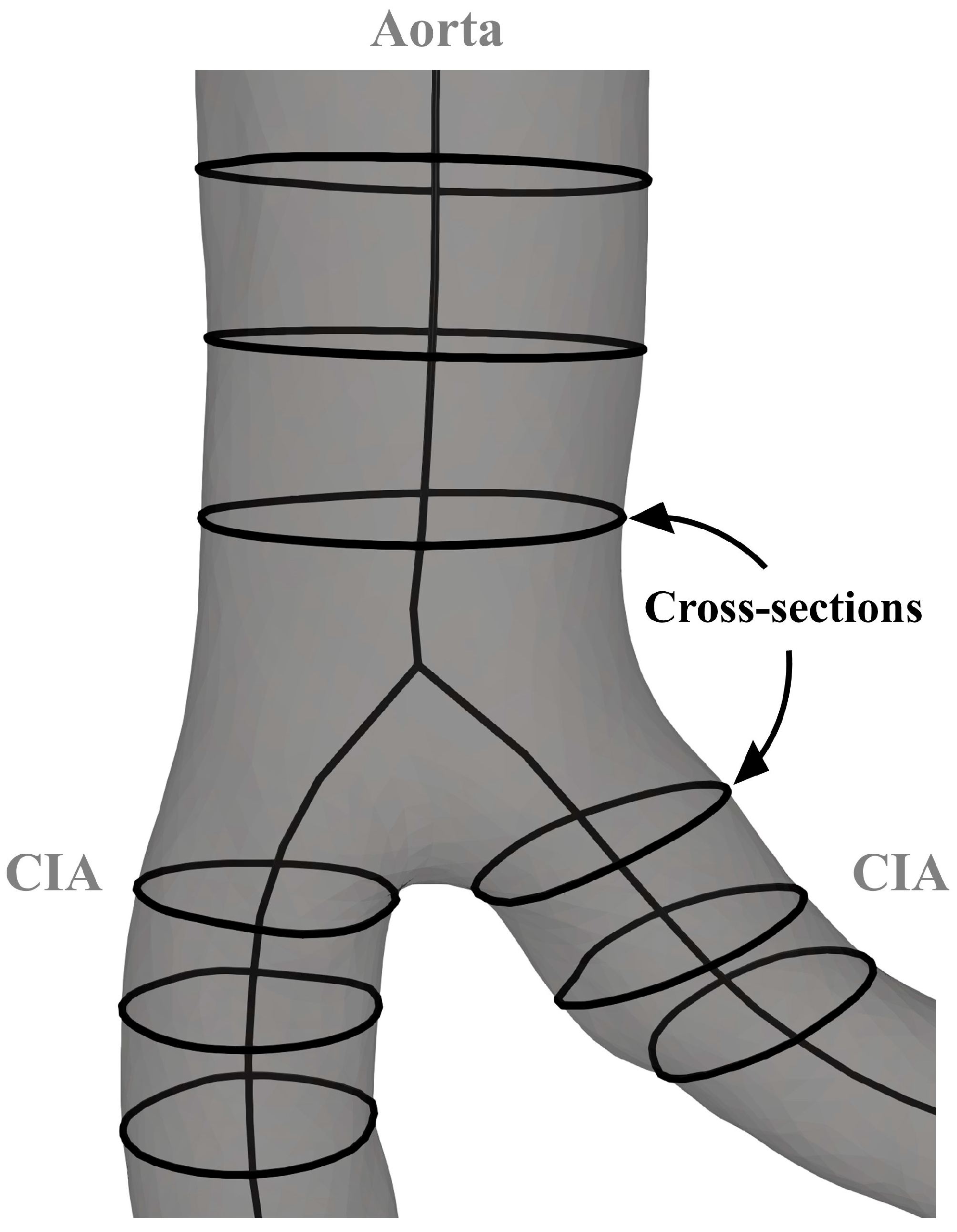
2.2.4. Geometry of Aortic Bifurcation
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics and Cardiovascular Risk Factors
3.2. Arterial Elongation
3.3. Geometry of Aortic Bifurcation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Criqui, M.H.; Matsushita, K.; Aboyans, V.; Hess, C.N.; Hicks, C.W.; Kwan, T.W.; McDermott, M.M.; Misra, S.; Ujueta, F.; American Heart Association Council on Epidemiology and Prevention; et al. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e171–e191, Erratum in Circulation 2021, 144, e193. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526, Erratum in Circ. Res. 2015, 117, e12. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, T.S.; McDermott, M.M. Lower Extremity Peripheral Artery Disease without Chronic Limb-Threatening Ischemia: A Review. JAMA 2021, 325, 2188–2198. [Google Scholar] [CrossRef] [PubMed]
- Mach, M.; Poschner, T.; Hasan, W.; Szalkiewicz, P.; Andreas, M.; Winkler, B.; Geisler, S.; Geisler, D.; Rudziński, P.N.; Watzal, V.; et al. The Iliofemoral tortuosity score predicts access and bleeding complications during transfemoral transcatheter aortic valve replacement: Data from the VIenna Cardio Thoracic aOrtic valve registrY (VICTORY). Eur. J. Clin. Investig. 2021, 51, e13491. [Google Scholar] [CrossRef] [PubMed]
- Fenelli, C.; Gargiulo, M.; Prendes, C.F.; Faggioli, G.; Stavroulakis, K.; Gallitto, E.; Stana, J.; Spath, P.; Rantner, B.; Tsilimparis, N. Effect of iliac tortuosity on outcomes after iliac branch procedures. J. Vasc. Surg. 2022, 76, 714–723.e1. [Google Scholar] [CrossRef] [PubMed]
- Dósa, E.; Hirschberg, K.; Apor, A.; Járányi, Z.; Entz, L.; Acsády, G.; Hüttl, K. Echolucent or predominantly echolucent femoral plaques predict early restenosis after eversion carotid endarterectomy. J. Vasc. Surg. 2010, 51, 345–350. [Google Scholar] [CrossRef] [PubMed]
- 3D Slicer Image Computing Platform. 3D Slicer. Available online: https://www.slicer.org (accessed on 6 August 2023).
- Kikinis, R.; Pieper, S.D.; Vosburgh, K. 3D Slicer: A platform for subject-specific image analysis, visualization, and clinical support. In Intraoperative Imaging Image-Guided Therapy; Ferenc, A.J., Ed.; Springer: New York, NY, USA, 2014; pp. 277–289, ISBN: 978-1-4614-7656-6 (Print) 978-1-4614-7657-3 (Online). [Google Scholar]
- Kapur, T.; Pieper, S.; Fedorov, A.; Fillion-Robin, J.C.; Halle, M.; O’Donnell, L.; Lasso, A.; Ungi, T.; Pinter, C.; Finet, J.; et al. Increasing the impact of medical image computing using community-based open-access hackathons: The NA-MIC and 3D Slicer experience. Med. Image Anal. 2016, 33, 176–180. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Pinter, C.; Lasso, A.; Fichtinger, G. Polymorph segmentation representation for medical image computing. Comput. Methods Programs Biomed. 2019, 171, 19–26. [Google Scholar] [CrossRef]
- Antiga, L.; Piccinelli, M.; Botti, L.; Ene-Iordache, B.; Remuzzi, A.; Steinman, D.A. An image-based modeling framework for patient-specific computational hemodynamics. Med. Biol. Eng. Comput. 2008, 46, 1097–1112. [Google Scholar] [CrossRef]
- The Vascular Modelling Toolkit. VMTK. Available online: https://www.vmtk.org (accessed on 10 August 2023).
- Shakeri, A.B.; Tubbs, R.S.; Shoja, M.M.; Nosratinia, H.; Oakes, W.J. Aortic bifurcation angle as an independent risk factor for aortoiliac occlusive disease. Folia Morphol. 2007, 66, 181–184. [Google Scholar] [CrossRef]
- Murray, C.D. The Physiological Principle of Minimum Work: I. The Vascular System and the Cost of Blood Volume. Proc. Natl. Acad. Sci. USA 1926, 12, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.D. The physiological principle of minimum work applied to the angle of branching of arteries. J. Gen. Physiol. 1926, 9, 835–841. [Google Scholar] [CrossRef] [PubMed]
- JASP Team. JASP (Version 0.17.3) [Computer Software]. 2023. Available online: https://jasp-stats.org/ (accessed on 10 August 2023).
- Tawfik, A.M.; Sobh, D.M.; Gadelhak, B.; Sobh, H.M.; Batouty, N.M. The effect of age and gender on tortuosity of the descending thoracic Aorta. Eur. J. Radiol. 2019, 110, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Togay-Işikay, C.; Kim, J.; Betterman, K.; Andrews, C.; Meads, D.; Tesh, P.; Tegeler, C.; Oztuna, D. Carotid artery tortuosity, kinking, coiling: Stroke risk factor, marker, or curiosity? Acta Neurol. Belg. 2005, 105, 68–72. [Google Scholar]
- Chiha, J.; Mitchell, P.; Gopinath, B.; Burlutsky, G.; Kovoor, P.; Thiagalingam, A. Gender differences in the prevalence of coronary artery tortuosity and its association with coronary artery disease. Int. J. Cardiol. Heart Vasc. 2016, 14, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Wood, N.B.; Zhao, S.Z.; Zambanini, A.; Jackson, M.; Gedroyc, W.; Thom, S.A.; Hughes, A.D.; Xu, X.Y. Curvature and tortuosity of the superficial femoral artery: A possible risk factor for peripheral arterial disease. J. Appl. Physiol. 2006, 101, 1412–1418. [Google Scholar] [CrossRef]
- Song, X.; Zhang, X.; Cui, L.; Liu, X.; Chen, Y.; Zheng, Y. Iliac Artery Tortuosity Index in Chinese Patients with or without Aortic Artery Aneurysms and Related Influencing Factors. Ann. Vasc. Surg. 2023, 94, 323–330. [Google Scholar] [CrossRef]
- Belvroy, V.M.; de Beaufort, H.W.L.; van Herwaarden, J.A.; Bismuth, J.; Moll, F.L.; Trimarchi, S. Tortuosity of the descending thoracic aorta: Normal values by age. PLoS ONE 2019, 14, e0215549. [Google Scholar] [CrossRef]
- Thomas, J.B.; Antiga, L.; Che, S.L.; Milner, J.S.; Steinman, D.A.; Spence, J.D.; Rutt, B.K.; Steinman, D.A. Variation in the carotid bifurcation geometry of young versus older adults: Implications for geometric risk of atherosclerosis. Stroke 2005, 36, 2450–2456. [Google Scholar] [CrossRef]
- Sun, Z.; Jiang, D.; Liu, P.; Muccio, M.; Li, C.; Cao, Y.; Wisniewski, T.M.; Lu, H.; Ge, Y. Age-Related Tortuosity of Carotid and Vertebral Arteries: Quantitative Evaluation with MR Angiography. Front. Neurol. 2022, 13, 858805. [Google Scholar] [CrossRef] [PubMed]
- Khosravani-Rudpishi, M.; Joharimoghadam, A.; Rayzan, E. The significant coronary tortuosity and atherosclerotic coronary artery disease; What is the relation? J. Cardiovasc. Thorac. Res. 2018, 10, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Roach, M.R.; Burton, A.C. The effect of age on the elasticity of human iliac arteries. Can. J. Biochem. Physiol. 1959, 37, 557–570. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, Z.W.; Fang, L.J.; Cheng, S.Q.; Wang, X.; Liu, N.F. Correlation analysis of coronary artery tortuosity and calcification score. BMC Surg. 2022, 22, 66. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.F.; Wang, D.M.; Wang, J.J.; Wang, L.J.; Lu, J.; Qi, P.; Hu, S.; Yang, X.M.; Chen, K.P. Extracranial Internal Carotid Artery Tortuosity and Body Mass Index. Front. Neurol. 2017, 8, 508. [Google Scholar] [CrossRef] [PubMed]
- Lauric, A.; Safain, M.G.; Hippelheuser, J.; Malek, A.M. High curvature of the internal carotid artery is associated with the presence of intracranial aneurysms. J. NeuroInterv. Surg. 2014, 6, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Faarvang, A.S.; Rørdam Preil, S.A.; Nielsen, P.S.; Beck, H.C.; Kristensen, L.P.; Rasmussen, L.M. Smoking is associated with lower amounts of arterial type I collagen and decorin. Atherosclerosis 2016, 247, 201–206. [Google Scholar] [CrossRef]
- Li, Y.; Shen, C.; Ji, Y.; Feng, Y.; Ma, G.; Liu, N. Clinical implication of coronary tortuosity in patients with coronary artery disease. PLoS ONE 2011, 6, e24232. [Google Scholar] [CrossRef]
- Han, H.C. Twisted blood vessels: Symptoms, etiology and biomechanical mechanisms. J. Vasc. Res. 2012, 49, 185–197. [Google Scholar] [CrossRef]
- Arribas, S.M.; Hinek, A.; González, M.C. Elastic fibres and vascular structure in hypertension. Pharmacol. Ther. 2006, 111, 771–791. [Google Scholar] [CrossRef]
- Groves, S.S.; Jain, A.C.; Warden, B.E.; Gharib, W.; Beto, R.J. Severe coronary tortuosity and the relationship to significant coronary artery disease. West Va. Med. J. 2009, 105, 14–17. [Google Scholar]
- Smith, E.R.; Tomlinson, L.A.; Ford, M.L.; McMahon, L.P.; Rajkumar, C.; Holt, S.G. Elastin degradation is associated with progressive aortic stiffening and all-cause mortality in predialysis chronic kidney disease. Hypertension 2012, 59, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.Y.; Han, B.; Lamm, S.D.; Fierro, C.A.; Han, H.C. Effects of elastin degradation and surrounding matrix support on artery stability. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H873–H884. [Google Scholar] [CrossRef] [PubMed]
- Lakchayapakorn, K.; Siriprakarn, Y. Anatomical variations of the position of the aortic bifurcation, iliocava junction and iliac veins in relation to the lumbar vertebra. J. Med. Assoc. Thai. 2008, 91, 1564–1570. [Google Scholar] [PubMed]
- Sun, H.; Kuban, B.D.; Schmalbrock, P.; Friedman, M.H. Measurement of the geometric parameters of the aortic bifurcation from magnetic resonance images. Ann. Biomed. Eng. 1994, 22, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.J.; Kwak, H.S.; Chung, G.H. Widening and Rotation of Carotid Artery with Age: Geometric Approach. J. Stroke Cerebrovasc. Dis. 2018, 27, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Schoenenberger, A.W.; Urbanek, N.; Toggweiler, S.; Seelos, R.; Jamshidi, P.; Resink, T.J.; Erne, P. Deviation from Murray's law is associated with a higher degree of calcification in coronary bifurcations. Atherosclerosis 2012, 221, 124–130. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cardiovascular Risk Factors/ Comorbidities, n (%) | All Participants (n = 204) | Female Participants (n = 84) | Male Participants (n = 120) |
|---|---|---|---|
| Obesity | 32 (15.7) | 10 (11.9) | 22 (18.3) |
| Smoking | 25 (12.3) | 9 (10.7) | 16 (13.3) |
| Hypertension | 104 (51.0) | 35 (41.7) | 69 (57.5) |
| Diabetes mellitus | 40 (19.6) | 14 (16.7) | 26 (21.7) |
| Hyperlipidemia | 71 (34.8) | 25 (29.8) | 46 (38.3) |
| CKD | 14 (6.9) | 7 (8.3) | 7 (5.8) |
| Elongation Parameters | All Participants (n = 204) | Female Participants (n = 84) | Male Participants (n = 120) |
|---|---|---|---|
| Tortuosity index (%), median (IQR) | |||
| Aorta | 0.862 (0.403–2.187) | 0.785 (0.323–1.757) | 0.967 (0.427–2.500) |
| Left CIA | 1.731 (0.753–4.306) | 1.191 (0.635–3.081) | 2.178 (0.918–6.295) |
| Left EIA | 2.856 (0.946–8.020) | 2.049 (0.680–4.567) | 4.132 (1.325–11.058) |
| Right CIA | 0.823 (0.257–2.611) | 0.478 (0.198–2.123) | 0.956 (0.387–3.803) |
| Right EIA | 3.048 (1.289–12.139) | 2.122 (0.929–6.180) | 3.970 (1.664–16.335) |
| Average absolute curvature (×1000), median (IQR) | |||
| Aorta | 6.665 (4.740–10.067) | 6.305 (4.865–9.383) | 7.095 (4.672–10.238) |
| Left CIA | 10.275 (6.395–16.207) | 9.660 (5.610–15.470) | 10.700 (6.888–17.040) |
| Left EIA | 12.640 (7.510–22.225) | 10.375 (6.872–17.948) | 16.190 (8.477–25.733) |
| Right CIA | 11.555 (8.638–18.580) | 10.520 (8.595–16.082) | 12.860 (8.775–19.712) |
| Right EIA | 11.900 (7.672–24.992) | 9.830 (6.750–19.267) | 15.420 (8.430–26.843) |
| Elongation Parameters | r-Value | Beta ± SD | p-Value |
|---|---|---|---|
| Tortuosity index | |||
| Aorta | 0.723 | 0.031 ± 0.002 | <0.001 |
| Left CIA | 0.664 | 0.032 ± 0.003 | <0.001 |
| Left EIA | 0.700 | 0.035 ± 0.003 | <0.001 |
| Right CIA | 0.688 | 0.040 ± 0.003 | <0.001 |
| Right EIA | 0.696 | 0.034 ± 0.002 | <0.001 |
| Average absolute curvature | |||
| Aorta | 0.570 | 0.010 ± 0.001 | <0.001 |
| Left CIA | 0.580 | 0.013 ± 0.001 | <0.001 |
| Left EIA | 0.623 | 0.014 ± 0.001 | <0.001 |
| Right CIA | 0.552 | 0.010 ± 0.001 | <0.001 |
| Right EIA | 0.629 | 0.015 ± 0.001 | <0.001 |
| Elongation Parameters, r-Value | Obesity | Smoking | Hypertension | Diabetes Mellitus | Hyperlipidemia | CKD |
|---|---|---|---|---|---|---|
| Tortuosity index | ||||||
| Aorta | −0.039 | 0.031 | 0.006 | −0.092 | −0.008 | 0.157 * |
| Left CIA | 0.051 | 0.032 | 0.070 | 0.038 | −0.136 | −0.005 |
| Left EIA | −0.077 | −0.123 | 0.058 | 0.080 | −0.051 | 0.067 |
| Right CIA | 0.089 | 0.021 | 0.120 | −0.036 | −0.113 | 0.081 |
| Right EIA | −0.145 * | −0.065 | 0.074 | 0.090 | −0.071 | 0.021 |
| Average absolute curvature | ||||||
| Aorta | −0.091 | −0.006 | 0.030 | −0.034 | 0.074 | 0.173 * |
| Left CIA | 0.058 | −0.057 | 0.157 * | −0.099 | −0.104 | 0.075 |
| Left EIA | −0.125 | −0.162 * | 0.147 | 0.075 | −0.070 | 0.033 |
| Right CIA | −0.036 | −0.064 | 0.179 * | 0.031 | −0.149 * | 0.049 |
| Right EIA | −0.170 * | −0.112 | 0.122 | 0.111 | −0.130 | 0.048 |
| Aortic Bifurcation Metrics | All Participants (n = 204) | Female Participants (n = 84) | Male Participants (n = 120) |
|---|---|---|---|
| Angles (°), median (IQR) | |||
| Left CIA take-off angle | 25.39 (20.48–32.03) | 25.27 (19.01–31.32) | 25.39 (21.43–32.22) |
| Right CIA take-off angle | 26.20 (21.50–31.71) | 25.77 (20.96–30.09) | 26.26 (22.13–32.45) |
| Aortic bifurcation angle | 52.32 (46.06–59.30) | 51.20 (45.04–58.75) | 52.49 (47.90–60.56) |
| Left CIA planarity | 5.91 (2.54–10.27) | 6.15 (2.54–9.25) | 5.79 (2.53–10.79) |
| Right CIA planarity | 5.94 (2.34–9.49) | 4.97 (2.12–9.33) | 6.48 (2.63–9.54) |
| Aortic bifurcation angle asymmetry | 0.01 (−0.16–0.19) | 0.01 (−0.16–0.19) | 0.01 (−0.16–0.19) |
| Cross-sectional area (cm2), median (IQR) | |||
| Distal infrarenal aorta | 159.46 (108.42–194.92) | 115.90 (89.28–145.55) | 189.95 (143.85–223.37) |
| Proximal left CIA | 69.05 (40.56–88.68) | 49.90 (32.85–59.00) | 82.46 (52.45–103.65) |
| Proximal right CIA | 74.66 (39.78–88.61) | 50.66 (32.79–64.70) | 91.46 (51.52–100.01) |
| Radius discrepancy (cm), median (IQR) | 1.12 (0.73–1.48) | 0.99 (0.63–1.32) | 1.26 (0.91–1.60) |
| Aortic Bifurcation Metrics | r-Value | Beta ± SD | p-Value |
|---|---|---|---|
| Angles | |||
| Left CIA take-off angle | 0.064 | 0.001 ± 0.001 | 0.365 |
| Right CIA take-off angle | 0.093 | 0.001 ± 0.001 | 0.186 |
| Aortic bifurcation angle | 0.242 | 0.002 ± 0.001 | <0.001 |
| Left CIA planarity | 0.262 | 0.009 ± 0.002 | <0.001 |
| Right CIA planarity | 0.214 | 0.008 ± 0.002 | 0.002 |
| Aortic bifurcation angle asymmetry | 0.225 | 0.001 ± 0.001 | 0.001 |
| Radius discrepancy | 0.394 | 0.009 ± 0.002 | <0.001 |
| Aortic Bifurcation Metrics, r-Value | Obesity | Smoking | Hypertension | Diabetes Mellitus | Hyperlipidemia | CKD |
|---|---|---|---|---|---|---|
| Angles | ||||||
| Left CIA take-off angle | 0.010 | −0.029 | −0.019 | −0.046 | 0.119 | −0.111 |
| Right CIA take-off angle | −0.039 | 0.047 | 0.054 | −0.019 | −0.094 | 0.153 * |
| Aortic bifurcation angle | −0.019 | 0.024 | 0.001 | −0.063 | 0.027 | 0.041 |
| Left CIA planarity | 0.078 | −0.010 | −0.030 | 0.061 | 0.195 ** | 0.041 |
| Right CIA planarity | 0.052 | −0.045 | −0.086 | −0.018 | 0.095 | 0.098 |
| Aortic bifurcation angle asymmetry | 0.055 | −0.014 | −0.107 | 0.056 | 0.119 | 0.062 |
| Radius discrepancy | −0.016 | 0.116 | 0.026 | 0.002 | 0.052 | −0.080 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szőnyi, Á.; Balázs, G.; Nyárády, B.B.; Philippovich, M.; Horváth, T.; Dósa, E. Effect of Sex, Age, and Cardiovascular Risk Factors on Aortoiliac Segment Geometry. J. Clin. Med. 2024, 13, 1705. https://doi.org/10.3390/jcm13061705
Szőnyi Á, Balázs G, Nyárády BB, Philippovich M, Horváth T, Dósa E. Effect of Sex, Age, and Cardiovascular Risk Factors on Aortoiliac Segment Geometry. Journal of Clinical Medicine. 2024; 13(6):1705. https://doi.org/10.3390/jcm13061705
Chicago/Turabian StyleSzőnyi, Ádám, György Balázs, Balázs Bence Nyárády, Márton Philippovich, Tamás Horváth, and Edit Dósa. 2024. "Effect of Sex, Age, and Cardiovascular Risk Factors on Aortoiliac Segment Geometry" Journal of Clinical Medicine 13, no. 6: 1705. https://doi.org/10.3390/jcm13061705
APA StyleSzőnyi, Á., Balázs, G., Nyárády, B. B., Philippovich, M., Horváth, T., & Dósa, E. (2024). Effect of Sex, Age, and Cardiovascular Risk Factors on Aortoiliac Segment Geometry. Journal of Clinical Medicine, 13(6), 1705. https://doi.org/10.3390/jcm13061705