

Inflammatory Cytokines Associated with Obesity, Type-2 Diabetes, and Hypertension Exacerbate Breast Cancer Risk in Underserved African American and Latin American Women

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
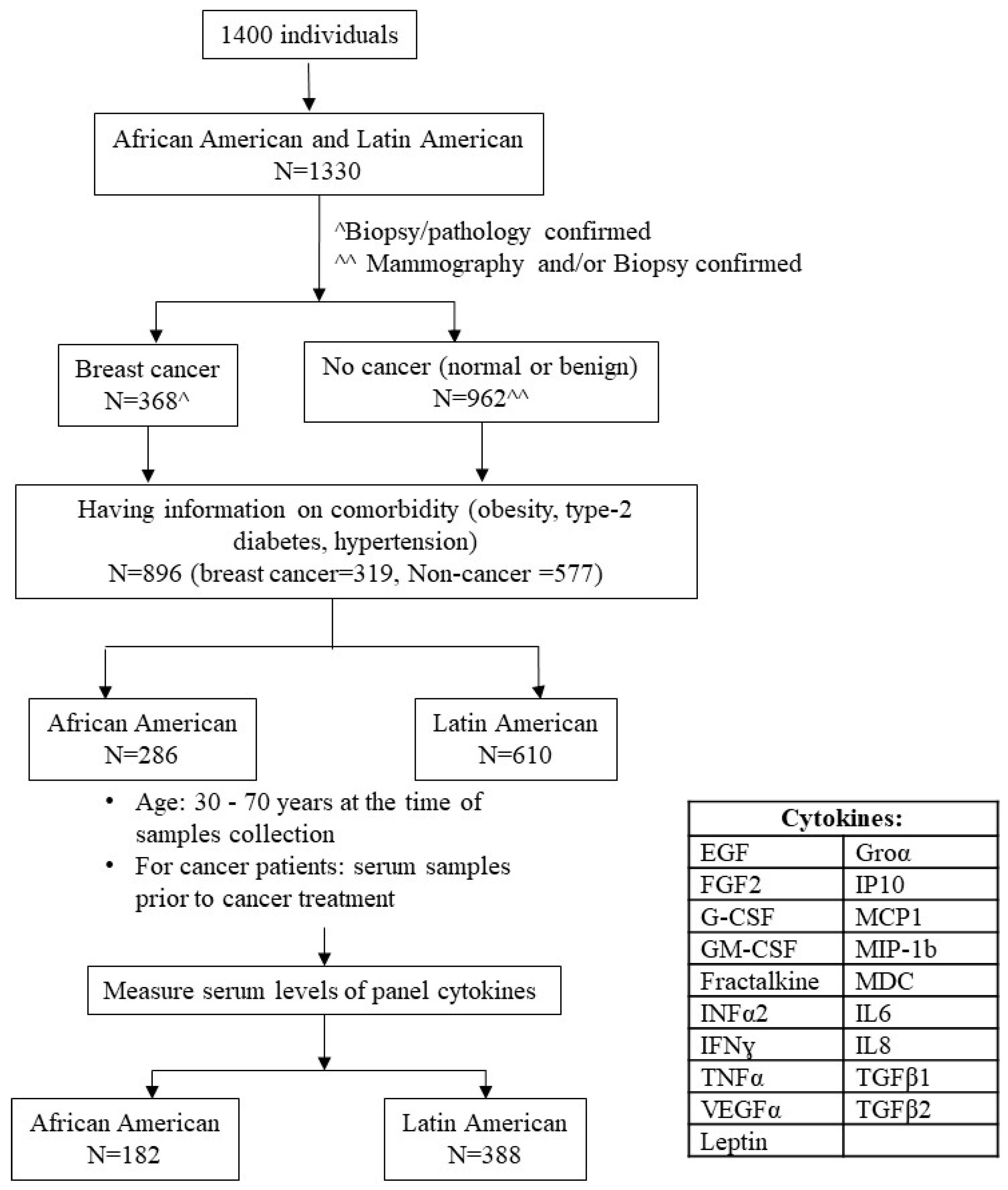
2.1. Human Subjects
2.2. Demographic and Clinical Information Collection
2.3. Cytokines Penal and Measurement
2.4. Statistical Analysis
3. Results
3.1. Study Population and Serum Cytokines Levels
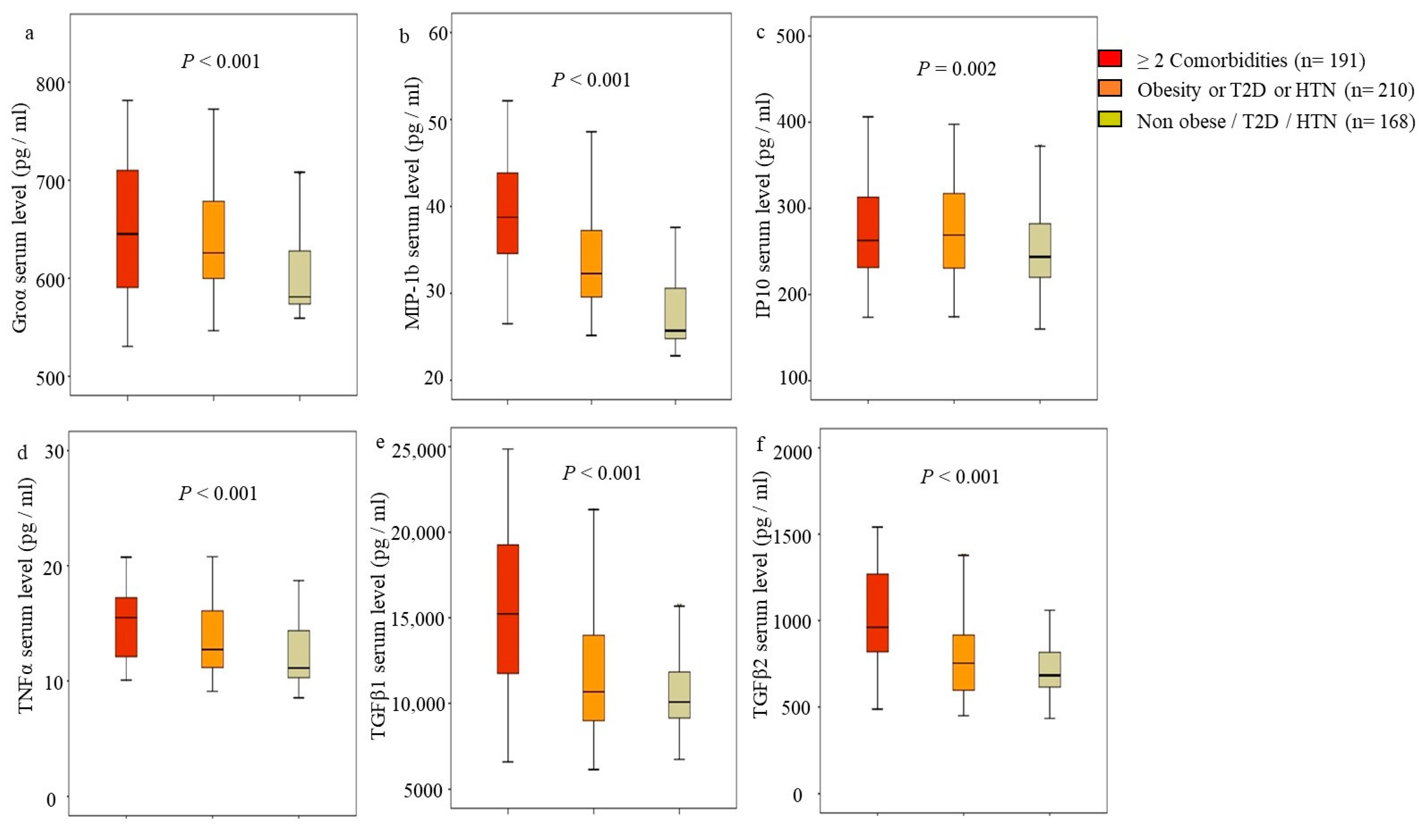
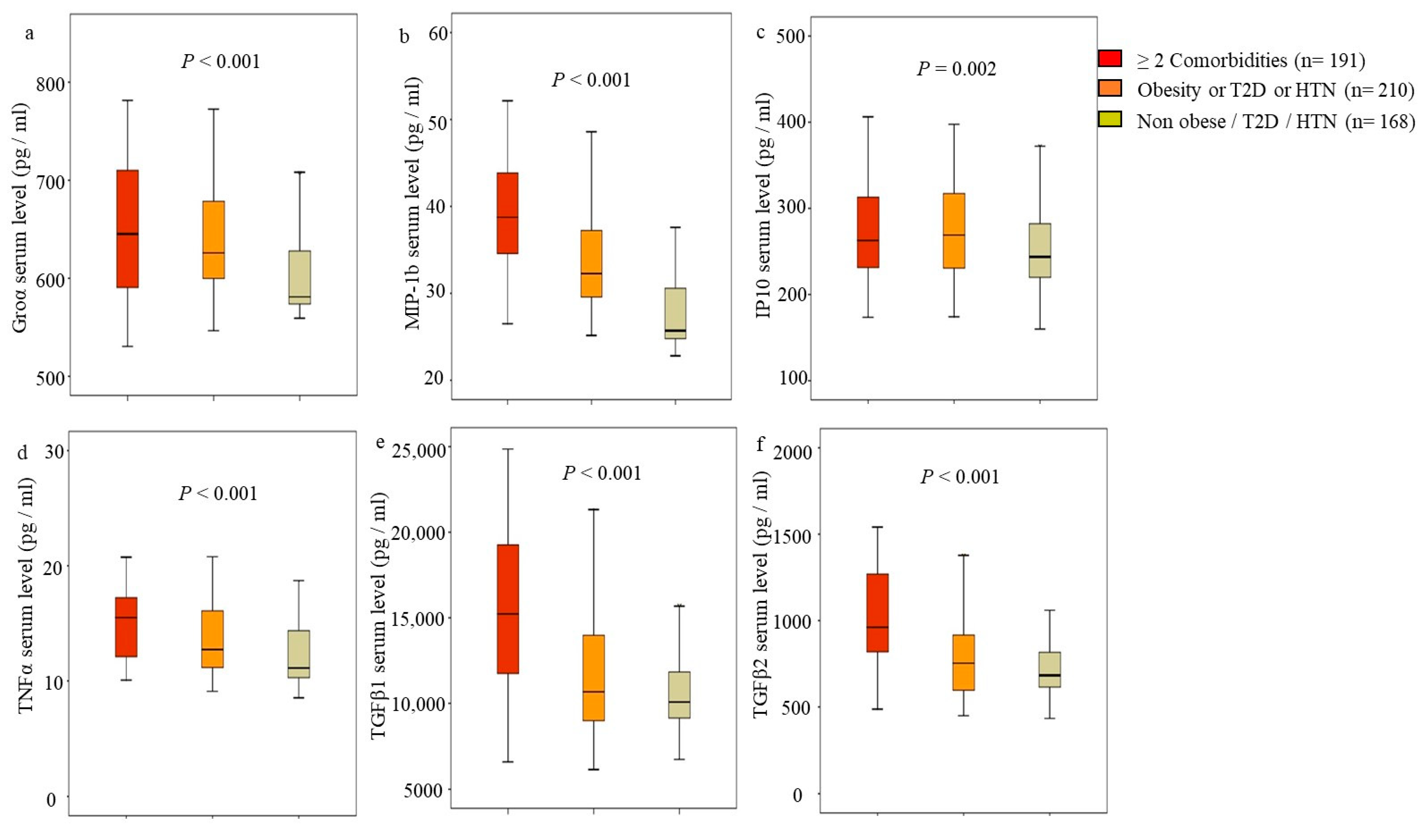
3.2. Identifying Independent Association of Cytokines with Comorbidities in AA and LA Women
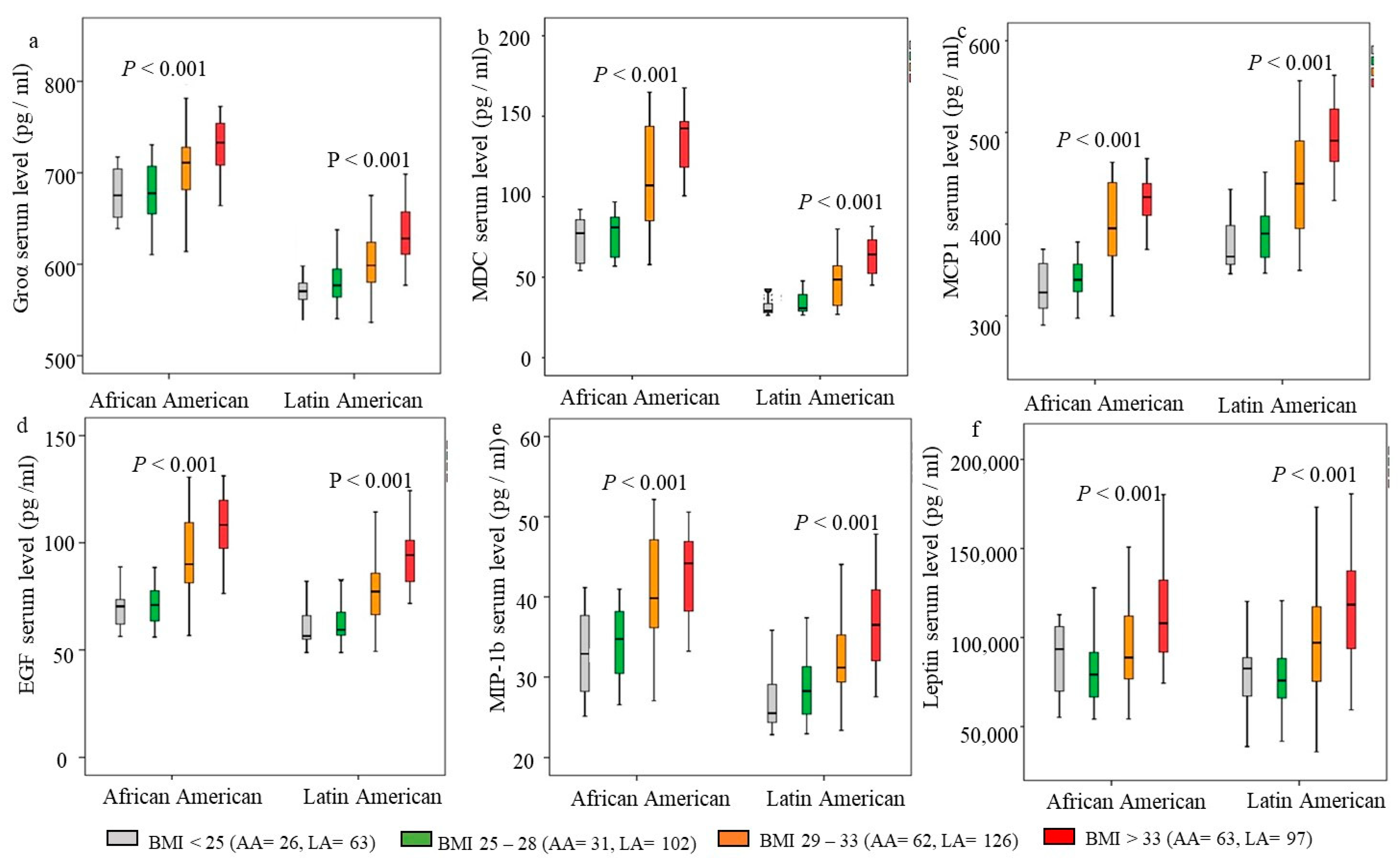
3.3. Association of Increasing Obesity-Associated Cytokines and BMI
3.4. Association of Cytokines and Breast Cancer
3.5. Identifying Cytokines’ Levels for Increasing Breast Cancer Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Centers for Disease Control and Prevention: Adult Obesity Facts. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 18 December 2023).
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef]
- Parr, C.L.; Batty, G.D.; Lam, T.H.; Barzi, F.; Fang, X.; Ho, S.C.; Jee, S.H.; Ansary-Moghaddam, A.; Jamrozik, K.; Ueshima, H.; et al. Asia-Pacific Cohort Studies Collaboration. Body-mass index and cancer mortality in the Asia-Pacific Cohort Studies Collaboration: Pooled analyses of 424,519 participants. Lancet Oncol. 2010, 11, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Neuhouser, M.L.; Aragaki, A.K.; Prentice, R.L.; Manson, J.E.; Chlebowski, R.; Carty, C.L.; Ochs-Balcom, H.M.; Thomson, C.A.; Caan, B.J.; Tinker, L.F.; et al. Overweight, Obesity, and Postmenopausal Invasive Breast Cancer Risk: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trials. JAMA Oncol. 2015, 1, 611–621. [Google Scholar] [CrossRef]
- Sarkissyan, M.; Wu, Y.; Vadgama, J.V. Obesity is associated with breast cancer in African American but not Hispanic women in South Los Angeles. Cancer 2011, 117, 3814–3823. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; MacCallum, P.R. The Obesity, Metabolic Syndrome, and Type 2 Diabetes Mellitus Pandemic: Part I. Increased Cardiovascular Disease Risk and the Importance of Atherogenic Dyslipidemia in Persons with the Metabolic Syndrome and Type 2 Diabetes Mellitus. J. Cardiometab. Syndr. 2009, 4, 113–119. [Google Scholar] [CrossRef]
- Jiang, S.Z.; Lu, W.; Zong, X.F.; Ruan, H.Y.; Liu, Y. Obesity and hypertension. Exp. Ther. Med. 2016, 12, 2395–2399. [Google Scholar] [CrossRef]
- Scully, T.; Ettela, A.; LeRoith, D.; Gallagher, E.J. Obesity, Type 2 Diabetes, and Cancer Risk. Front. Oncol. 2021, 10, 615375. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Kar, S.; Carter, P.; Vithayathil, M.; Mason, A.M.; Burgess, S.; Larsson, S.C. Is Type 2 Diabetes Causally Associated with Cancer Risk? Evidence from a Two-Sample Mendelian Randomization Study. Diabetes 2020, 69, 1588–1596. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, K.M.; McTigue, K.M.; Fidler, C.J.; Neaton, J.D.; Chang, Y.; Fried, L.F.; Liu, S.; Kuller, L.H. Hypertension and obesity and the risk of kidney cancer in two large cohorts of US men and women. Hypertension 2014, 63, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Colt, J.S.; Schwartz, K.; Graubard, B.I.; Davis, F.; Ruterbusch, J.; Digaetano, R.; Purdue, M.; Rothman, N.; Wacholder, S.; Chow, W.H. Hypertension and risk of renal cell carcinoma among white and black Americans. Epidemiology 2011, 22, 797–804. [Google Scholar] [CrossRef]
- Bloom, M.W.; Hamo, C.E.; Cardinale, D.; Ky, B.; Nohria, A.; Baer, L.; Skopicki, H.; Lenihan, D.J.; Gheorghiade, M.; Lyon, A.R.; et al. Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging. Circ. Heart Fail. 2016, 9, e002661. [Google Scholar] [CrossRef]
- Han, H.; Guo, W.; Shi, W.; Yu, Y.; Zhang, Y.; Ye, X.; He, J. Hypertension and breast cancer risk: A systematic review and meta-analysis. Sci. Rep. 2017, 20, 44877. [Google Scholar] [CrossRef]
- Harding, J.L.; Sooriyakumaran, M.; Anstey, K.J.; Adams, R.; Balkau, B.; Brennan-Olsen, S.; Briffa, T.; Davis, T.M.E.; Davis, W.A.; Dobson, A.; et al. Hypertension, antihypertensive treatment and cancer incidence and mortality. J. Hypertens. 2016, 34, 149–155. [Google Scholar] [CrossRef]
- Mohammed, T.; Singh, M.; Tiu, J.G.; Kim, A.S. Etiology and management of hypertension in patients with cancer. Cardio Oncol. 2021, 7, 14. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Kanaya, A.M.; Araneta, M.R.G.; Saydah, S.H.; Kahn, H.S.; Gregg, E.W.; Fujimoto, W.Y.; Imperatore, G. Prevalence of Diabetes by Race and Ethnicity in the United States, 2011–2016. JAMA 2019, 322, 2389–2398. [Google Scholar] [CrossRef] [PubMed]
- Lackland, D.T. Racial Differences in Hypertension: Implications for High Blood Pressure Management. Am. J. Med. Sci. 2014, 348, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Daw, J. Contribution of Four Comorbid Conditions to Racial/Ethnic Disparities in Mortality Risk. Am. J. Prev. Med. 2017, 52, S95–S102. [Google Scholar] [CrossRef] [PubMed]
- Hoang, T.; Lee, J.; Kim, J. Comorbidity Risk Score in Association with Cancer Incidence: Results from a Cancer Screenee Cohort. Cancers 2020, 12, 1834. [Google Scholar] [CrossRef]
- Gallagher, E.J.; LeRoith, D. Obesity and Diabetes: The Increased Risk of Cancer and Cancer-Related Mortality. Physiol. Rev. 2015, 95, 727–748. [Google Scholar] [CrossRef]
- Katsogiannos, P.; Kamble, P.G.; Pereira, M.J.; Sundbom, M.; Carlsson, P.O.; Eriksson, J.W.; Espes, D. Changes in Circulating Cytokines and Adipokines After RYGB in Patients with and without Type 2 Diabetes. Obesity 2021, 29, 535–542. [Google Scholar] [CrossRef]
- Picon-Ruiz, M.; Morata-Tarifa, C.; Valle-Goffin, J.J.; Friedman, E.R.; Slingerland, J.M. Obesity and Adverse Breast Cancer Risk and Outcome: Mechanistic Insights and Strategies for Intervention. CA Cancer J. Clin. 2017, 67, 378–397. [Google Scholar] [CrossRef]
- Li, J.J.; Fang, C.H.; Hui, R.T. Is hypertension an inflammatory disease? Med. Hypotheses 2005, 64, 236–240. [Google Scholar] [CrossRef]
- Balkwill, F.; Charles, K.A.; Mantovani, A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell 2005, 7, 211–217. [Google Scholar] [CrossRef]
- Hamet, P. Cancer and hypertension. An unresolved issue. Hypertension 1996, 28, 321–324. [Google Scholar] [CrossRef]
- Azizian, M.; Mahdipour, E.; Mirhafez, S.R.; Shoeibi, S.; Nematy, M.; Esmaily, H.; Ferns, G.A.A.; Ghayour-Mobarhan, M. Cytokine profiles in overweight and obese subjects and normal weight individuals matched for age and gender. Ann. Clin. Biochem. 2016, 53, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Williamsa, A.; Greenea, N.; Kimbro, K.S. Increased Circulating Cytokine Levels in African American women with Obesity and Elevated HbA1c. Cytokine 2020, 128, 154989. [Google Scholar] [CrossRef]
- Denis, G.V.; Sebastiani, P.; Andrieu, G.; Tran, A.H.; Strissel, K.J.; Lombardi, F.L.; Palmer, J.R. Relationships among obesity, Type 2 diabetes and plasma cytokines in African American women. Obesity 2017, 25, 1916–1920. [Google Scholar] [CrossRef] [PubMed]
- DeLoach, S.; Huan, Y.; Keith, S.W.; Cantarin, M.P.M.; Falkner, B. Relationship of blood pressure and obesity with inflammatory cytokines among African Americans. Ther. Adv. Cardiovasc. Dis. 2011, 5, 149–157. [Google Scholar] [CrossRef]
- Li, L.; Chen, L.; Zhang, W.; Liao, Y.; Chen, J.; Shi, Y.; Luo, S. Serum cytokine profile in patients with breast cancer. Cytokine 2017, 89, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Jabeena, S.; Espinoza, J.A.; Torlandb, L.A.; Zucknick, M.; Kumara, S.; Haakensene, V.D.; Lüders, T.; Engebraaten, O.; Børresen-Daleb, A.L.; Kytef, J.A.; et al. Noninvasive profiling of serum cytokines in breast cancer patients and clinicopathological characteristics. Oncoimmunology 2018, 8, e1537691. [Google Scholar] [CrossRef]
- Park, J.W.; Chang, H.J.; Yeo, H.Y.; Han, N.; Kim, B.C.; Kong, S.Y.; Kim, J.; Oh, J.H. The relationships between systemic cytokine profiles and inflammatory markers in colorectal cancer and the prognostic significance of these parameters. Br. J. Cancer 2020, 123, 610–618. [Google Scholar] [CrossRef]
- Barrera, L.; Montes-Servín, E.; Barrera, A.; Ramírez-Tirado, L.A.; Salinas-Parra, F.; Bañales-Méndez, J.L.; Sandoval-Ríos, M.; Arrieta, Ó. Cytokine profiles determined by data-mining analysis were set into clusters of non-small-cell lung cancer patients according to prognosis. Ann. Oncol. 2015, 26, 428–435. [Google Scholar] [CrossRef]
- Capone, F.; Guerriero, E.; Sorice, A.; Colonna, G.; Ciliberto, G.; Costantini, S. Serum Cytokinome Profile Evaluation: A Tool to Define New Diagnostic and Prognostic Markers of Cancer Using Multiplexed Bead-Based Immunoassays. Mediat. Inflamm. 2016, 2016, 3064643. [Google Scholar] [CrossRef]
- Lan, T.; Chen, L.; Wei, X. Inflammatory Cytokines in Cancer: Comprehensive Understanding and Clinical Progress in Gene Therapy. Cells 2021, 10, 100. [Google Scholar] [CrossRef]
- Los Angeles County Department of Public Health. Key Indicators of Health by Service Plan Area. 2017. Available online: http://publichealth.lacounty.gov/ha/docs/2015lachs/keyindicator/ph-kih_2017-sec%20updated.pdf (accessed on 18 December 2023).
- Lucas-Wright, A.; Bazargan, M.; Jones, L.; Vadgama, J.V.; Vargas, R.; Sarkissyan, M.; Smith, J.; Yazdanshenas, H.; Maxwell, A.E. Correlates of the perceived risk of developing cancer among African Americans in South Los Angeles. J. Community Health 2014, 39, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic Adipose Tissue Inflammation Linking Obesity to Insulin Resistance and Type 2 Diabetes. Front. Physiol. 2020, 10, 1607. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Faßhauer, M.; Stumvoll, M.; et al. Inflammatory Cytokines in General and Central Obesity and Modulating Effects of Physical Activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef] [PubMed]
- Alia, M.M.; Naquiallahc, D.; Qureshic, M.; Mirzac, M.I.; Hassand, C.; Masrurd, M.; Biancod, F.M.; Frederick, P.; Cristoforod, G.P.; Gangemid, A.; et al. DNA methylation profile of genes involved in inflammation and autoimmunity correlates with vascular function in morbidly obese adults. Epigenetics 2022, 17, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Cartier, A.; Lemieux, I.; Alméras, N.; Tremblay, A.; Bergeron, J.; Després, J.P. Visceral obesity and plasma glucose-insulin homeostasis: Contributions of interleukin-6 and tumor necrosis factor-alpha in men. J. Clin. Endocrinol. Metab. 2008, 93, 1931–1938. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Park, H.S.; Kawada, T.; Kim, J.H.; Lim, D.; Hubbard, N.E.; Kwon, B.S.; Erickson, K.L.; Yu, R. Circulating levels of MCP-1 and IL-8 are elevated in human obese subjects and associated with obesity-related parameters. Int. J. Obes. 2006, 30, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Breslin, W.L.; Johnston, C.A.; Strohacker, K.; Carpenter, K.C.; Davidson, T.R.; Moreno, J.P.; Foreyt, J.P.; McFarlin, B.K. Obese Mexican American Children Have Elevated MCP-1, TNF-a, Monocyte Concentration, and Dyslipidemia. Pediatrics 2012, 129, e1180–e1186. [Google Scholar] [CrossRef]
- Straczkowski, M.; Dzienis-straczkowska, S.; Stepien, A.; Kowalska, I.; Szelachowska, M.; Kinalska, I. Plasma Interleukin-8 Concentrations Are Increased in Obese Subjects and Related to Fat Mass and Tumor Necrosis Factor-α System. J. Clin. Endocrinol. Metab. 2002, 87, 4602–4606. [Google Scholar] [CrossRef]
- Spranger, J.; Kroke, A.; Mohlig, M.; Hoffmann, K.; Bergmann, M.; Ristow, M.; Boeing, H.; Pfeiffer, A. Inflammatory Cytokines and the risk of developing type 2 diabetes. Diabetes 2003, 52, 812–817. [Google Scholar] [CrossRef]
- Hellmich, B.; Schiller, M.; Schatz, H.; Pfeiffer, A. Activation of transforming growth factor-beta1 in diabetic kidney disease. Metab. Clin. Exp. 2000, 49, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Rashed, L. Estimation of transforming growth factor-beta 1 as a marker of renal injury in type II diabetes mellitus. Saudi Med. J. 2007, 28, 519–523. [Google Scholar] [PubMed]
- Zhang, Y.; Proenca, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional Cloning of the Mouse Obese Gene and its Human Homologue. Nature 1994, 372, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Obradovic, M.; Sudar-Milovanovic, E.; Soskic, S.; Essack, M.; Arya, S.; Stewart, A.J.; Gojobori, T.; Isenovic, E.R. Leptin and Obesity: Role and Clinical Implication. Front. Endocrinol. 2021, 12, 585887. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.F.; Tuero, C.; Valenti, V.; Bilbao, I. Relevance of Leptin and Other Adipokines in Obesity-Associated Cardiovascular Risk. Nutrients 2019, 11, 2664. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.H.; Wei, S.G.; Francis, J.; Felder, R.B. Cardiovascular and renal sympathetic activation by blood-borne TNF in the rat: The role of central prostaglandins. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R916–R927. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.U.; Lee, R.T.; Rifai, N.; Ridker, P.M. Blood pressure and inflammation in apparently healthy men. Hypertension 2001, 38, 399–403. [Google Scholar] [CrossRef]
- Stowe, R.P.; Peek, M.K.; Cutchin, M.P.; Goodwin, J.S. Plasma Cytokine Levels in a Population-Based Study: Relation to Age and Ethnicity. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 4, 429–433. [Google Scholar] [CrossRef]
- Quail, D.F.; Dannenberg, A.J. The obese adipose tissue microenvironment in cancer development and progression. Nat. Rev. Endocrinol. 2019, 3, 139–154. [Google Scholar] [CrossRef]
- Cruceriu, D.; Baldasici, O.; Balacescu, O.; Berindan-Neagoe, I. The dual role of tumor necrosis factor-alpha (TNF-α) in breast cancer: Molecular insights and therapeutic approaches. Cell Oncol. 2020, 43, 1–18. [Google Scholar] [CrossRef]
- Soria, G.; Ofri-Shahak, M.; Haas, I.; Yaal-Hahoshen, N.; Leider-Trejo, L.; Leibovich-Rivkin, T.; Weitzenfeld, P.; Meshel, T.; Shabtai, E.; Gutman, M.; et al. Inflammatory mediators in breast cancer: Coordinated expression of TNFα & IL-1β with CCL2 & CCL5 and effects on epithelial-to-mesenchymal transition. BMC Cancer 2011, 11, 130–149. [Google Scholar] [PubMed]
- Katanov, C.; Lerrer, S.; Liubomirski, Y.; Leider-Trejo, L.; Meshel, T.; Bar, J.; Feniger-Barish, R.; Kamer, I.; Soria-Artzi, G.; Kahani, H.; et al. Regulation of the inflammatory profile of stromal cells in human breast cancer: Prominent roles for TNF-α and the NF-κB pathway. Stem Cell Res. Ther. 2015, 6, 87. [Google Scholar] [CrossRef]
- Zhang, T.; Tseng, C.; Zhang, Y.; Sirin, O.; Corn, P.G.; Li-Ning-Tapia, E.M.; Troncoso, P.; Davis, J.; Pettaway, C.; Ward, J.; et al. CXCL1 mediates obesity-associated adipose stromal cell trafficking and function in the tumour microenvironment. Nat. Commun. 2016, 7, 11674. [Google Scholar] [CrossRef] [PubMed]
- Bhat, K.; Sarkissyan, M.; Wu, Y.; Vadgama, J.V. GROα overexpression drives cell migration and invasion in triple-negative breast cancer cells. Oncol. Rep. 2017, 38, 21–30. [Google Scholar] [CrossRef]
- Kawai, M.; Malone, K.E.; Tang, M.T.; Li, C.I. Height, body mass index (BMI), BMI change, and the risk of estrogen receptor-positive, HER2-positive, and triple-negative breast cancer among women ages 20 to 44 years. Cancer 2014, 120, 1548–1556. [Google Scholar] [CrossRef]
- John, E.M.; Sangaramoorthy, M.; Hines, L.M.; Stern, M.C.; Baumgartner, K.B.; Giuliano, A.R.; Wolff, R.K.; Slattery, M.L. Overall and abdominal adiposity and premenopausal breast cancer risk among Hispanic women: The Breast Cancer Health Disparities study. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 138–147. [Google Scholar] [CrossRef]
- Moses, H.; Barcellos-Hoff, M.H. TGF-β Biology in Mammary Development and Breast Cancer. Cold Spring Harb. Perspect. Biol. 2011, 3, a003277. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Baba, T.; Nishimura, T.; Hayakawa, Y.; Hashimoto, S.; Gotoh, N.; Mukaida, N. Essential roles of the interaction between cancer cell-derived chemokine, CCL4, and intra-bone CCR5-expressing fibroblasts in breast cancer bone metastasis. Cancer Lett. 2016, 378, 23–32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total = 570 |
|---|---|
| n (%) | |
| Ethnicity | |
| African American | 182 (31.9) |
| Latin American | 388 (68.1) |
| Age | |
| 30–40 | 117 (20.5) |
| 41–50 | 208 (36.5) |
| 51–60 | 180 (31.6) |
| >60 | 65 (11.4) |
| Cancer | |
| Breast cancer | 261 (45.8) |
| Non-Cancers | 309 (54.2) |
| Body Mass Index (BMI) | |
| Obese (≥30) | 261 (45.8) |
| Overweight (>25 and <30) | 210 (36.8) |
| Normal Weight (≤25) | 99 (17.4) |
| Type-2 Diabetes (T2D) | |
| Yes | 160 (28.1) |
| No | 410 (71.9) |
| Hypertension (HTN) | |
| Yes | 192 (33.7) |
| No | 378 (66.3) |
| Cytokines | Median Level (pg/mL) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ethnicity | BMI | Breast Cancer | T2D | HTN | ||||||||
| Total | AA a | LA aa | ≥30 | 25–29 | <25 | Cases | Control b | Yes | No | Yes | No | |
| EGF | 86.9 | 119.8 ^ | 79.4 | 95.2 ^^ | 72.5 | 86.8 | 102.6 ^^ | 77.4 | 73.7 | 87.3 | 92.8 | 78.8 |
| FGF2 | 44.1 | 38.9 | 47.0 | 41.0 | 47.4 | 44.2 | 42.8 | 45.1 | 41.1 | 43.8 | 37.8 | 47.4 |
| G-CSF | 24.8 | 25.3 | 24.5 | 24.0 | 24.6 | 26.8 | 27.2 ^ | 22.4 | 26.1 | 23.8 | 25.3 | 24.2 |
| GM-CSF | 11.2 | 12.7 | 11.0 | 12.0 | 11.0 | 11.5 | 9.1 | 12.8 | 10.3 | 11.7 | 9.1 | 12.3 |
| Fractalkine | 48.3 | 45.7 | 49.4 | 47.3 | 49.2 | 49.1 | 44.9 | 51.1 | 44.7 | 49.2 | 47.6 | 45.9 |
| INFα2 | 15.6 | 14.0 | 17.1 | 16.0 | 13.5 | 18.3 | 14.9 | 17.9 | 14.0 | 16.0 | 17.0 | 13.8 |
| IFNɣ | 7.4 | 7.3 | 7.4 | 6.5 | 8.0 | 7.8 | 7.4 | 7.4 | 4.8 | 7.9 | 6.8 | 7.9 |
| TNFα | 13.9 | 14.7 | 13.7 | 15.3 | 14.3 | 11.8 | 17.3 ^^ | 12.2 | 15.7 ^ | 13.2 | 16.7 ^^ | 12.4 |
| Groα | 636.1 | 682.1 ^^ | 615.7 | 644.5 ^^ | 626.5 | 618.5 | 657.1 ^^ | 610.0 | 623.5 | 642.3 | 654.6 ^ | 627.7 |
| IP10 | 248.5 | 240.4 | 254.2 | 270.0 | 248.0 | 219.2 | 300.6 ^^ | 225.1 | 259.3 | 243.6 | 261.7 | 236.8 |
| MCP1 | 428.0 | 369.0 | 448.5 | 484.3 ^^ | 377.2 | 380.1 | 447.7 | 405.0 | 467.0 ^ | 404.2 | 463.8 | 402.2 |
| MIP-1b | 34.9 | 42.0 ^^ | 32.6 | 41.0 ^^ | 32.6 | 25.5 | 41.0 ^^ | 29.3 | 40.5 | 32.3 | 44.1 ^^ | 29.5 |
| MDC | 866.9 | 1045 ^^ | 762 | 974.4 ^^ | 782.9 | 659.2 | 938.2 ^^ | 755.9 | 904.1 | 862.3 | 939.5 ^^ | 830.4 |
| IL6 | 19.2 | 16.2 | 20.3 | 14.4 | 18.5 | 28.5 | 16.2 | 23.1 | 14.0 | 22.2 | 17.1 | 19.4 |
| IL8 | 11.6 | 11.3 | 11.7 | 12.8 | 10.1 | 10.9 | 13.2 ^ | 9.6 | 11.7 | 11.5 | 15.1 ^^ | 9.2 |
| VEGFα | 111.4 | 152.9 ^^ | 97.6 | 136.3 ^^ | 86.1 | 78.3 | 126.4 ^^ | 97.8 | 109.3 | 109.7 | 131.9 ^^ | 100.0 |
| TGFβ1 | 17,979.0 | 19,610.5 | 17,707.0 | 19,745.0 | 13,358.5 | 20,362.0 | 25,667.0 ^ | 9123.0 | 32,977.8 ^^ | 29,411.8 | 20,066.0 | 18,152.0 |
| TGFβ2 | 993.7 | 1219.0 | 892.8 | 958.7 | 906.2 | 1105.5 | 1508.0 ^ | 652.2 | 2063.2 ^ | 1832.2 | 1275.0 | 917.6 |
| Leptin | 91,456.0 | 92,404.0 | 90,721.0 | 110,757.0 ^^ | 85,119.0 | 74,637.0 | 96,702.0 | 84,184.0 | 185,837.5 ^^ | 141,197.2 | 94,162.0 | 110,341.0 |
| a. Association of cytokines and obesity | ||||
| Outcome | Coefficients | Expected geometric mean ratios (95% CI) by obesity (Yes vs. No) | ||
| Cytokines | B (Obesity) | Std. Error | p | |
| EGF ^ | 0.16 | 0.05 | 0.001 | 1.26 (1.0, 1.8) |
| MCP1 ^ | 0.10 | 0.03 | <0.001 | 1.17 (1.1, 1.45) |
| MIP-1b ^ | 0.07 | 0.03 | 0.04 | 1.20 (1.0, 1.38) |
| MDC ^ | 0.08 | 0.03 | 0.004 | 1.10 (1.06, 1.38) |
| Groα ^ | 0.04 | 0.01 | 0.001 | 1.45 (1.03, 1.13) |
| Leptin ^ | 0.16 | 0.05 | 0.001 | 1.45 (1.15, 1.78) |
| b. Association of cytokines and T2D | ||||
| Outcome | Coefficients | Expected geometric mean ratios (95% CI) by T2D (Yes vs. No) | ||
| Cytokines | B (T2D) | Std. Error | p | |
| TGFβ1 ^ | 0.22 | 0.08 | 0.04 | 1.66 (1.17, 2.29) |
| TGFβ2 ^ | 0.17 | 0.07 | 0.04 | 1.48 (1.10, 2.04) |
| Leptin ^ | 0.21 | 0.07 | <0.001 | 1.62 (1.26, 2.0) |
| c. Association of cytokines and HTN | ||||
| Outcome | Coefficients | Expected geometric mean ratios (95% CI) by HTN (Yes vs. No) | ||
| Cytokines | B (HTN) | Std. Error | p | |
| TNFα ^^ | 0.08 | 0.03 | 0.01 | 1.20 (1.05, 1.4) |
| MIP-1b ^^ | 0.10 | 0.04 | 0.04 | 1.26 (1.10, 1.5) |
| VEGFα ^^ | 0.12 | 0.06 | 0.02 | 1.32 (1.02, 1.7) |
| d. Association of cytokines and ethnicity | ||||
| Outcome | Coefficients | Expected geometric mean ratios (95% CI) by ethnicity (AA.* vs. LA **) | ||
| Cytokines | B (AA *) | Std. Error | p | |
| MDC ^ | 0.12 | 0.03 | <0.001 | 1.32 (1.15, 1.55) |
| IP10 ^ | −0.08 | 0.05 | 0.02 | 0.83 (0.71, 0.74) |
| MCP1 ^ | −0.08 | 0.03 | 0.01 | 0.83 (0.72, 0.96) |
| VEGFα ^ | 0.17 | 0.06 | 0.007 | 1.48 (1.12, 2.0) |
| Groα ^ | 0.06 | 0.01 | <0.001 | 1.15 (1.1, 2.2) |
| Outcome | Coefficients | Expected Geometric Mean Ratios (95% CI) by Breast Cancer (Yes vs. No) | ||
|---|---|---|---|---|
| Cytokines | B (Cancer) | Std. Error | p | |
| Groα | 0.03 | 0.01 | 0.002 | 1.08 (1.03, 1.13) |
| MIP-1b | 0.09 | 0.03 | 0.006 | 1.23 (1.06, 1.44) |
| IP10 | 0.15 | 0.03 | <0.001 | 1.40 (1.23, 1.58) |
| TNFα | 0.15 | 0.03 | <0.001 | 1.43 (1.23, 1.62) |
| TGFβ1 | 0.15 | 0.07 | 0.029 | 1.41 (1.03, 1.91) |
| TGFβ2 | 0.15 | 0.06 | 0.018 | 1.41 (1.07, 1.91) |
| Cytokines (pg/mL) | African American | Latin American | Age ≤ 50 | Age > 50 | ||||
|---|---|---|---|---|---|---|---|---|
| OR ^ (95% CI) | p | OR ^ (95% CI) | p | OR * (95% CI) | p | OR * (95% CI) | p | |
| Groα | ||||||||
| ≤636 | 1 | 1 | 1 | 1 | ||||
| 637–707 | 4.2 (1.3–13.3) | 0.015 | 1.7 (0.9–3.3) | 0.123 | 1.9 (0.9–4.2) | 0.094 | 2.3 (1.0–5.3) | 0.04 |
| ≥708 | 8.7 (2.9–25.6) | <0.001 | 5.4 (1.7–17.6) | 0.005 | 4.0 (1.4–11.0) | 0.009 | 7.0 (2.6–19.3) | <0.001 |
| MIP-1b | ||||||||
| ≤35 | 1 | 1 | 1 | 1 | ||||
| 36–57 | 1.9 (0.8–4.9) | 0.155 | 1.2 (0.7–2.1) | 0.463 | 1.4 (0.7–2.4) | 0.32 | 1.6 (0.8–3.4) | 0.194 |
| ≥58 | 1.1 (0.5–2.3) | 0.828 | 1.6 (0.9–2.9) | 0.086 | 1.8 (1.0 -3.3) | 0.04 | 1.1 (0.6–2.3) | 0.744 |
| IP10 | ||||||||
| ≤250 | 1 | 1 | 1 | 1 | ||||
| 251–388 | 1.5 (0.6–3.4) | 0.35 | 1.5 (0.9–2.6) | 0.136 | 1.1 (0.5–2.1) | 0.81 | 1.6 (0.8–3.2) | 0.21 |
| ≥389 | 5.1 (2.0–13.3) | 0.001 | 3.0 (1.7–5.1) | <0.001 | 3.6 (1.8–6.9) | <0.001 | 3.2 (1.4–7.2) | 0.004 |
| TNFα | ||||||||
| ≤14 | 1 | 1 | 1 | 1 | ||||
| 15–20 | 1.5 (0.6–2.8) | 0.533 | 1.6 (0.9–2.8) | 0.105 | 1.4 (0.7–2.4) | 0.17 | 1.4 (0.6–3.0) | 0.46 |
| ≥21 | 2.7 (1.0–6.9) | 0.041 | 3.1 (1.8–5.3) | <0.001 | 1.8 (1.0–3.3) | 0.026 | 4.1 (2.0–8.6) | <0.001 |
| TGFβ1 | ||||||||
| ≤184,55 | 1 | 1 | 1 | 1 | ||||
| 18,456–46,712 | 1.0 (0.4–2.3) | 0.944 | 1.9 (1.1–3.2) | 0.026 | 2.3 (1.3–4.3) | 0.006 | 1.0 (0.4–2.1) | 0.924 |
| ≥46,713 | 1.2 (0.5–2.9) | 0.698 | 1.7 (1.0–3.0) | 0.05 | 1.8 (1.0–3.4) | 0.047 | 1.6 (0.7–3.3) | 0.242 |
| TGFβ2 | ||||||||
| ≤1004 | 1 | 1 | 1 | 1 | ||||
| 1005–2998 | 2.0 (0.7–5.4) | 0.166 | 2.7 (1.6–4.7) | <0.001 | 2.7 (1.5–5.1) | 0.001 | 2.4 (1.1–5.2) | 0.037 |
| ≥2999 | 1.2 (0.5–2.7) | 0.733 | 1.7 (0.9–2.9) | 0.085 | 1.9 (1.0–3.5) | 0.048 | 1.5 (0.7–3.2) | 0.339 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.; Karapetyan, E.; Dutta, P.; Shaheen, M.; Vadgama, J.V. Inflammatory Cytokines Associated with Obesity, Type-2 Diabetes, and Hypertension Exacerbate Breast Cancer Risk in Underserved African American and Latin American Women. J. Clin. Med. 2024, 13, 1687. https://doi.org/10.3390/jcm13061687
Wu Y, Karapetyan E, Dutta P, Shaheen M, Vadgama JV. Inflammatory Cytokines Associated with Obesity, Type-2 Diabetes, and Hypertension Exacerbate Breast Cancer Risk in Underserved African American and Latin American Women. Journal of Clinical Medicine. 2024; 13(6):1687. https://doi.org/10.3390/jcm13061687
Chicago/Turabian StyleWu, Yanyuan, Eduard Karapetyan, Pranabananda Dutta, Magda Shaheen, and Jaydutt V. Vadgama. 2024. "Inflammatory Cytokines Associated with Obesity, Type-2 Diabetes, and Hypertension Exacerbate Breast Cancer Risk in Underserved African American and Latin American Women" Journal of Clinical Medicine 13, no. 6: 1687. https://doi.org/10.3390/jcm13061687
APA StyleWu, Y., Karapetyan, E., Dutta, P., Shaheen, M., & Vadgama, J. V. (2024). Inflammatory Cytokines Associated with Obesity, Type-2 Diabetes, and Hypertension Exacerbate Breast Cancer Risk in Underserved African American and Latin American Women. Journal of Clinical Medicine, 13(6), 1687. https://doi.org/10.3390/jcm13061687