
Impact of the Timing of Mechanical Circulatory Support on the Outcomes in Myocardial Infarction-Related Cardiogenic Shock: Subanalysis of the PREPARE CS Registry

 , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tehrani, B.N.; Truesdell, A.G.; Psotka, M.A.; Rosner, C.; Singh, R.; Sinha, S.S.; Damluji, A.A.; Batchelor, W.B. A Standardized and Comprehensive Approach to the Management of Cardiogenic Shock. JACC Heart Fail. 2020, 8, 879–891. [Google Scholar] [CrossRef]
- Thiele, H.; Ohman, E.M.; Desch, S.; Eitel, I.; de Waha, S. Management of cardiogenic shock. Eur. Heart J. 2015, 36, 1223–1230. [Google Scholar] [CrossRef]
- Thiele, H.; Ohman, E.M.; de Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Bastien, O.; Bendjelid, K.; Cariou, A.; Chouihed, T.; Combes, A.; Mebazaa, A.; Megarbane, B.; Plaisance, P.; Ouattara, A.; et al. Experts’ recommendations for the management of adult patients with cardiogenic shock. Ann. Intensive Care 2015, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Akin, I.; Behnes, M.; Rassaf, T.; Mahabadi, A.A.; Lehmann, R.; Eitel, I.; Graf, T.; Seidler, T.; et al. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. N. Engl. J. Med. 2023, 389, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.P.; Spertus, J.A.; Curtis, J.P.; Desai, N.; Masoudi, F.A.; Bach, R.G.; McNeely, C.; Al-Badarin, F.; House, J.A.; Kulkarni, H.; et al. The Evolving Landscape of Impella Use in the United States among Patients Undergoing Percutaneous Coronary Intervention with Mechanical Circulatory Support. Circulation 2020, 141, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Dhruva, S.S.; Ross, J.S.; Mortazavi, B.J.; Hurley, N.C.; Krumholz, H.M.; Curtis, J.P.; Berkowitz, A.; Masoudi, F.A.; Messenger, J.C.; Parzynski, C.S.; et al. Association of Use of an Intravascular Microaxial Left Ventricular Assist Device vs Intra-aortic Balloon Pump with In-Hospital Mortality and Major Bleeding among Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock. JAMA 2020, 323, 734. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Desch, S.; de Waha, S. Mechanical circulatory support: The last resort in cardiogenic shock? EuroIntervention 2018, 13, 2099–2101. [Google Scholar] [CrossRef] [PubMed]
- Taleb, I.; Koliopoulou, A.G.; Tandar, A.; McKellar, S.H.; Tonna, J.E.; Nativi-Nicolau, J.; Villela, M.A.; Welt, F.; Stehlik, J.; Gilbert, E.M.; et al. Shock Team Approach in Refractory Cardiogenic Shock Requiring Short-Term Mechanical Circulatory Support. Circulation 2019, 140, 98–100. [Google Scholar] [CrossRef]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement from the American Heart Association. Circulation 2017, 136, E232–E268. [Google Scholar] [CrossRef] [PubMed]
- von Lewinski, D.; Herold, L.; Stoffel, C.; Pätzold, S.; Fruhwald, F.; Altmanninger-Sock, S.; Kolesnik, E.; Wallner, M.; Rainer, P.; Bugger, H.; et al. PRospective REgistry of PAtients in REfractory cardiogenic shock—The PREPARE CardShock registry. Catheter. Cardiovasc. Interv. 2022, 100, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Helgestad, O.K.L.; Josiassen, J.; Hassager, C.; Jensen, L.O.; Holmvang, L.; Udesen, N.L.J.; Schmidt, H.; Ravn, H.B.; Moller, J.E. Contemporary trends in use of mechanical circulatory support in patients with acute MI and cardiogenic shock. Open Heart 2020, 7, e001214. [Google Scholar] [CrossRef]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary. J. Am. Coll. Cardiol. 2013, 61, 485–510. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Fröhlich, G.; Bott-Flügel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schömig, A. A Randomized Clinical Trial to Evaluate the Safety and Efficacy of a Percutaneous Left Ventricular Assist Device Versus Intra-Aortic Balloon Pumping for Treatment of Cardiogenic Shock Caused by Myocardial Infarction. J. Am. Coll. Cardiol. 2008, 52, 1584–1588. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; Eriksen, E.; Sjauw, K.D.; van Dongen, I.M.; Hirsch, A.; Packer, E.J.S.; Vis, M.M.; Wykrzykowska, J.J.; Koch, K.T.; Baan, J.; et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock after Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 69, 278–287. [Google Scholar] [CrossRef]
- Kapur, N.K.; Paruchuri, V.; Urbano-Morales, J.A.; Mackey, E.E.; Daly, G.H.; Qiao, X.; Pandian, N.; Perides, G.; Karas, R.H. Mechanically Unloading the Left Ventricle before Coronary Reperfusion Reduces Left Ventricular Wall Stress and Myocardial Infarct Size. Circulation 2013, 128, 328–336. [Google Scholar] [CrossRef]
- Meyns, B.; Stolinski, J.; Leunens, V.; Verbeken, E.; Flameng, W. Left ventricular support by Catheter-Mountedaxial flow pump reduces infarct size. J. Am. Coll. Cardiol. 2003, 41, 1087–1095. [Google Scholar] [CrossRef]
- O’Neill, W.W.; Grines, C.; Schreiber, T.; Moses, J.; Maini, B.; Dixon, S.R.; Ohman, E.M. Analysis of outcomes for 15,259 US patients with acute myocardial infarction cardiogenic shock (AMICS) supported with the Impella device. Am. Heart J. 2018, 202, 33–38. [Google Scholar] [CrossRef]
- Basir, M.B.; Schreiber, T.L.; Grines, C.L.; Dixon, S.R.; Moses, J.W.; Maini, B.S.; Khandelwal, A.K.; Ohman, E.M.; O’Neill, W.W. Effect of Early Initiation of Mechanical Circulatory Support on Survival in Cardiogenic Shock. Am. J. Cardiol. 2017, 119, 845–851. [Google Scholar] [CrossRef]
- Basir, M.B.; Lemor, A.; Gorgis, S.; Patel, K.C.; Kolski, B.C.; Bharadwaj, A.S.; Todd, J.W.; Tehrani, B.N.; Truesdell, A.G.; Lasorda, D.M.; et al. Early Utilization of Mechanical Circulatory Support in Acute Myocardial Infarction Complicated by Cardiogenic Shock: The National Cardiogenic Shock Initiative. J. Am. Heart Assoc. 2023, 12, e031401. [Google Scholar] [CrossRef]
- Saxena, A.; Garan, A.R.; Kapur, N.K.; O’Neill, W.W.; Lindenfeld, J.; Pinney, S.P.; Uriel, N.; Burkhoff, D.; Kern, M. Value of Hemodynamic Monitoring in Patients with Cardiogenic Shock Undergoing Mechanical Circulatory Support. Circulation 2020, 141, 1184–1197. [Google Scholar] [CrossRef]
- Pieri, M.; Sorrentino, T.; Oppizzi, M.; Melisurgo, G.; Lembo, R.; Colombo, A.; Zangrillo, A.; Pappalardo, F. The role of different mechanical circulatory support devices and their timing of implantation on myocardial damage and mid-term recovery in acute myocardial infarction related cardiogenic shock. J. Interv. Cardiol. 2018, 31, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Antman, E.M. Time Is Muscle: Translation into Practice. J. Am. Coll. Cardiol. 2008, 52, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Contri, R.; Winterton, D.; Montorfano, M.; Colombo, A.; Zangrillo, A.; De Bonis, M.; Pappalardo, F. The contemporary role of Impella in a comprehensive mechanical circulatory support program: A single institutional experience. BMC Cardiovasc. Disord. 2015, 15, 126. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.L.; Kapur, N.K. Acute mechanical circulatory support for cardiogenic shock: The “door to support” time. F1000Research 2017, 6, 737. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Upfront Group | n = 33 | Procedural Group | n = 38 | p | |
|---|---|---|---|---|---|
| n/Mean | % or SD | n/Mean | % or SD | ||
| Age | 67 | ±10 | 62 | ±11 | 0.05 |
| OHCA | 8 | 25 | 10 | 28 | 0.99 |
| Any CPR | 15 | 45 | 30 | 79 | <0.05 |
| Female gender | 8 | 24 | 7 | 18 | 0.57 |
| BMI | 28 | 5 | 28 | 4 | 0.75 |
| Hypertension | 19 | 58 | 16 | 42 | 0.24 |
| Dyslipidemia | 11 | 33 | 8 | 21 | 0.29 |
| Diabetes mellitus | 6 | 18 | 11 | 29 | 0.40 |
| History of PCI | 5 | 15 | 6 | 16 | 0.99 |
| History of CABG | 2 | 6 | 2 | 5 | 0.99 |
| ACS STEMI | 26 | 79 | 28 | 74 | 0.78 |
| ACS NSTEMI | 7 | 21 | 10 | 26 | 0.78 |
| Intubated before admission | 20 | 61 | 28 | 74 | 0.31 |
| Thrombolysis before admission | 0 | 0 | 2 | 5.2 | 0.49 |
| Noradrenalin (mL/h when 12.5 mg/50 mL) | 6.6 | 6.2 | 8.5 | 6.5 | 0.09 |
| Systolic blood pressure (mmHg) | 95.7 | 20 | 95.9 | 23.7 | 0.85 |
| Heart rate/minute | 74.4 | 18.5 | 78.1 | 23.2 | 0.71 |
| PaO2 (mmHg) | 106.8 | 80.6 | 92.7 | 64.1 | 0.22 |
| pH | 7.20 | 0.21 | 7.24 | 0.15 | 0.36 |
| Lactate level (mmol/L) | 5.7 | 4.9 | 6.4 | 4.6 | 0.24 |
| “Door to support” time (Minutes) | 116 | 82 | 102 | 79 | 0.56 |
| Upfront Group | n = 33 | Procedural Group | n = 38 | p | |
|---|---|---|---|---|---|
| n/Mean | % or SD | n/Mean | % or SD | ||
| Multivessel Disease | 27 | 82 | 32 | 84 | 0.99 |
| MV Disease PCI | 15 | 45 | 16 | 42 | 0.81 |
| Full Revascularization | 17 | 52 | 13 | 34 | 0.16 |
| Complex PCI Procedure | 31 | 94 | 27 | 71 | 0.02 |
| Bifurcation Lesion PCI | 16 | 48 | 10 | 26 | 0.08 |
| Relevant Coronary Calcification (with need for special lesion preparation) | 3 | 9 | 3 | 8 | 0.99 |
| Contrast Used (mL) | 246 | 98 | 252 | 121 | 0.82 |
| Procedure Duration (Minutes) | 142 | 62 | 134 | 60 | 0.59 |
| Vascular Complications or Bleeding | 0 | 0 | 1 | 3 | 0.99 |
| Ischemic Complications | 1 | 3 | 0 | 0 | 0.46 |
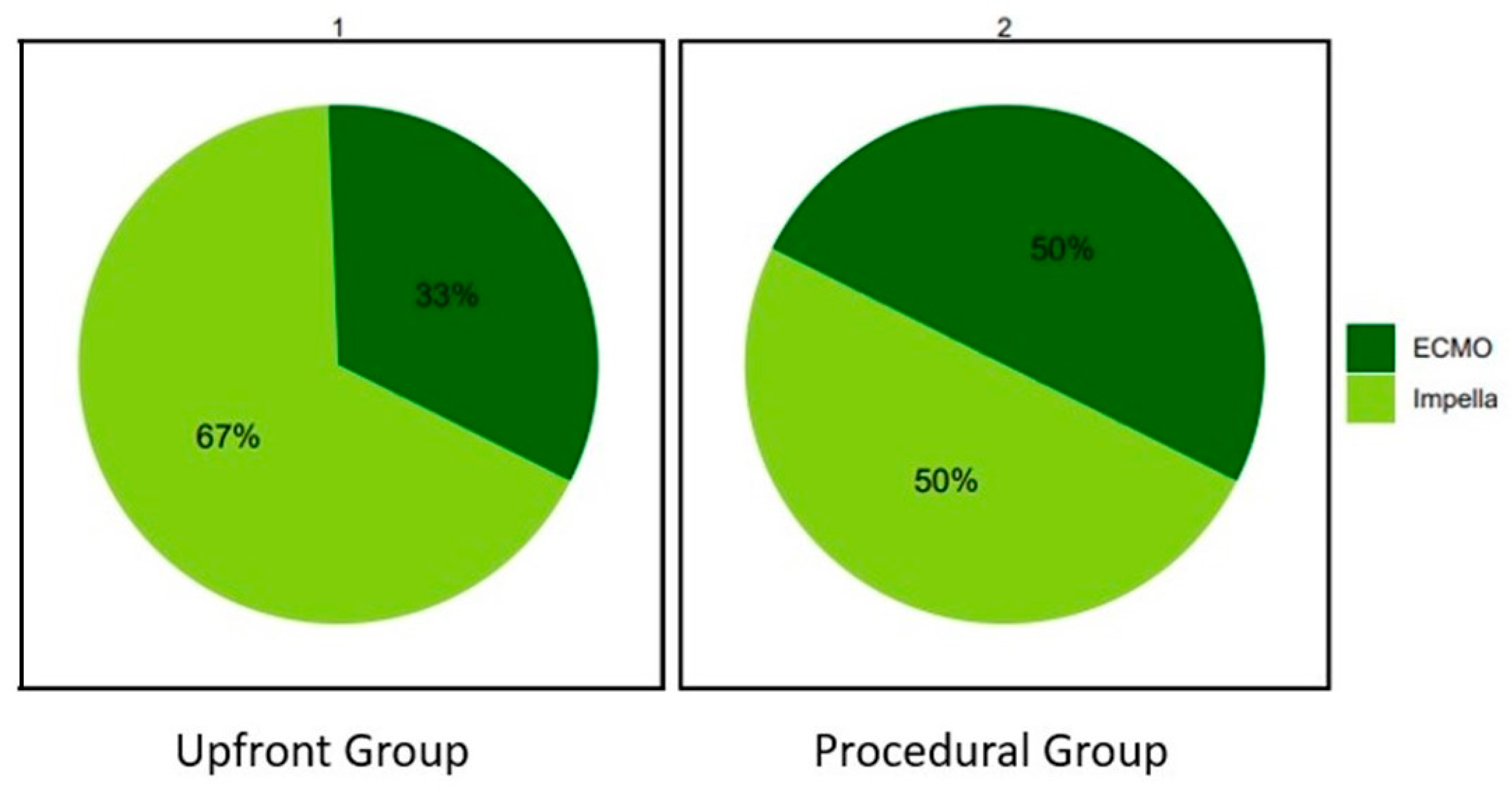
| Use of IMPELLA | 22 | 67 | 19 | 50 | |
| Use of ECMO | 11 | 33 | 19 | 50 | 0.23 |
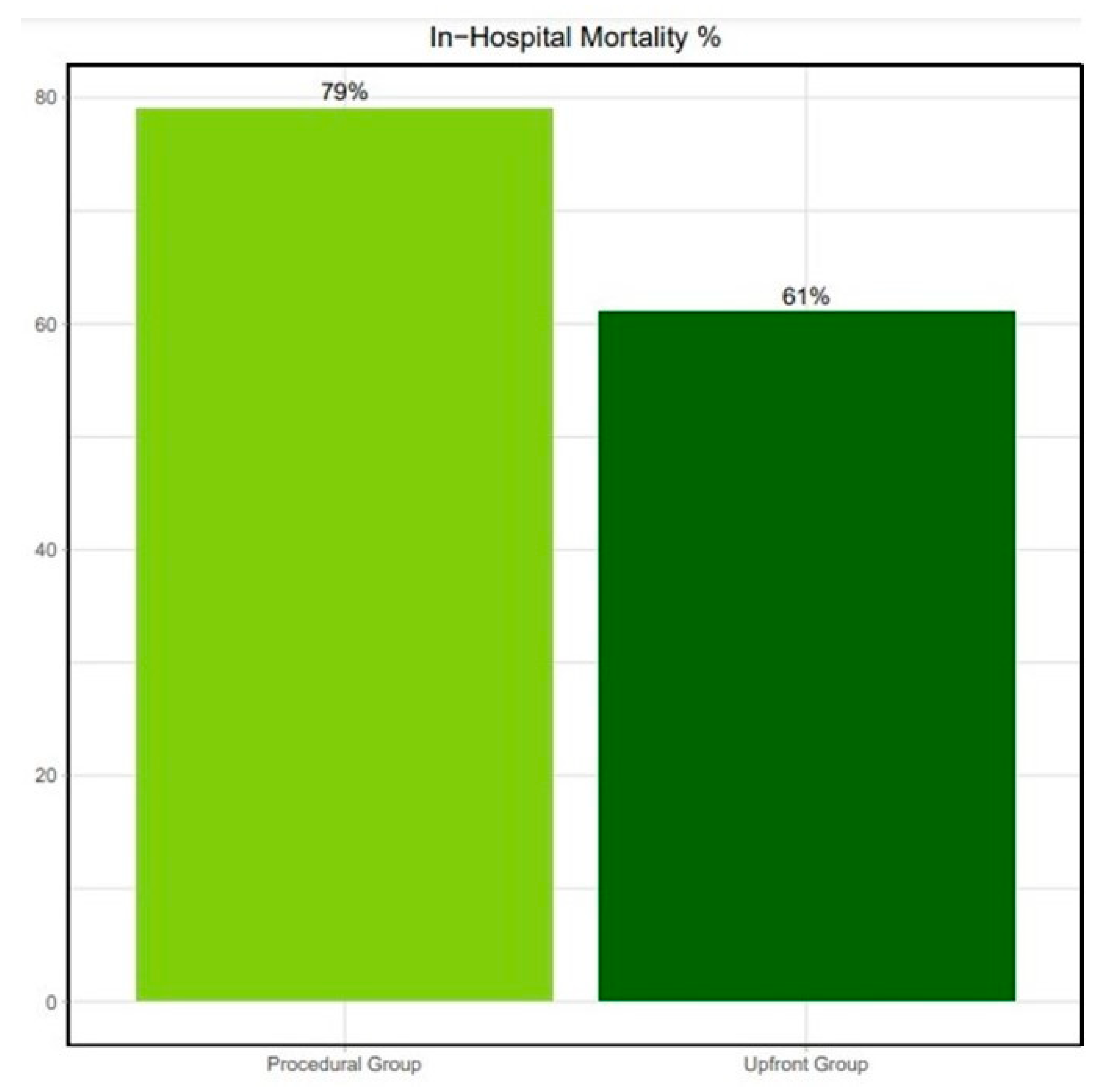
| In-Hospital Mortality | 20 | 61 | 30 | 79 | 0.12 |
| Upfront Group | n = 33 | Procedural Group | n = 38 | p | |
|---|---|---|---|---|---|
| n/Mean | % or SD | n/Mean | % or SD | ||
| CCU Stay (Days) | 9.8 | 10.2 | 8.6 | 9.8 | 0.5 |
| Total Hospital Stay (Days) | 14.5 | 14 | 13.6 | 20.4 | 0.26 |
| Days on MCS | 3.5 | 3.9 | 4.1 | 4.1 | 0.21 |
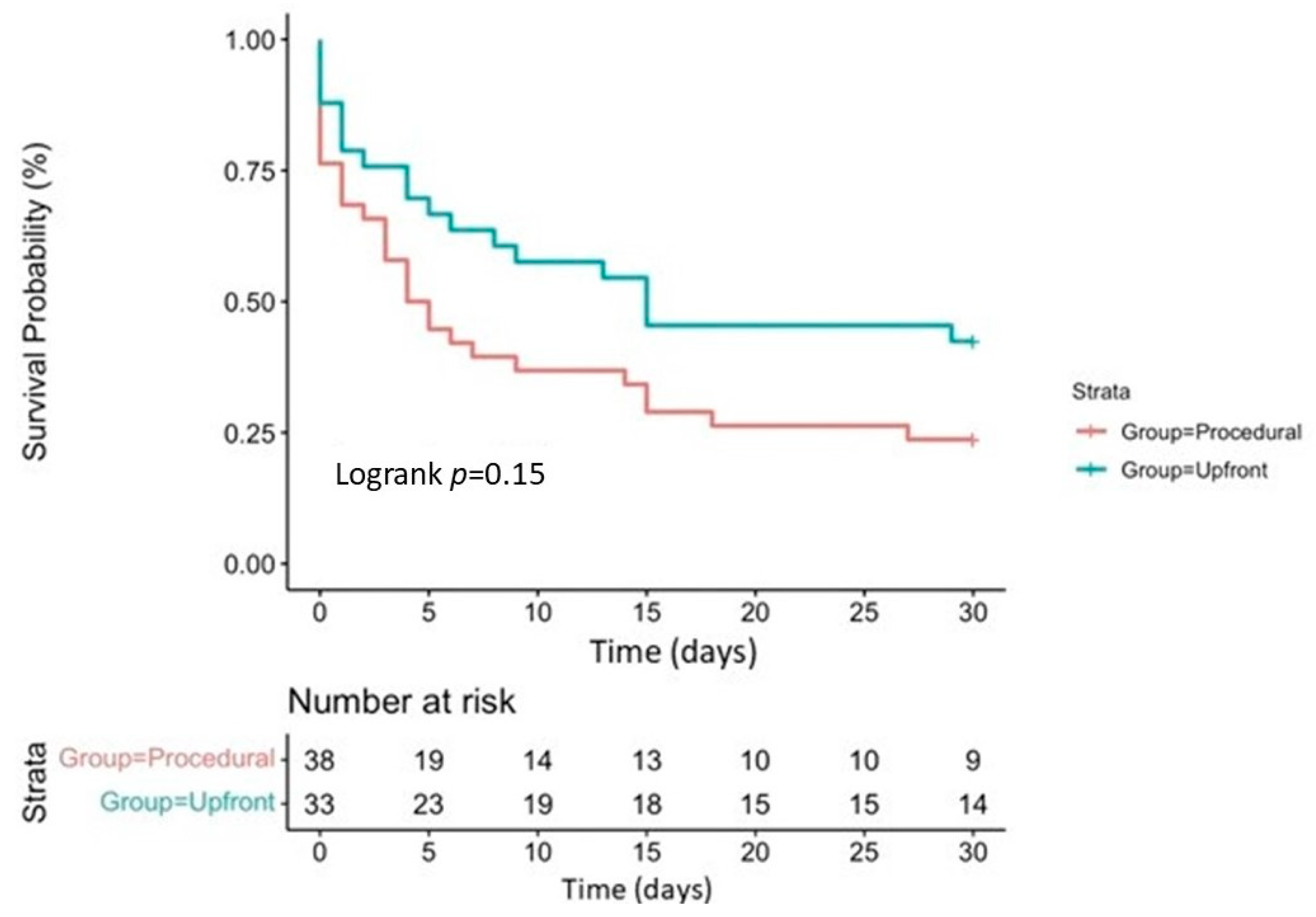
| 30-day Survival | 13 | 40 | 8 | 21 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prunea, D.M.; Bachl, E.; Herold, L.; Kanoun Schnur, S.S.; Pätzold, S.; Altmanninger-Sock, S.; Sommer, G.A.; Glantschnig, T.; Kolesnik, E.; Wallner, M.; et al. Impact of the Timing of Mechanical Circulatory Support on the Outcomes in Myocardial Infarction-Related Cardiogenic Shock: Subanalysis of the PREPARE CS Registry. J. Clin. Med. 2024, 13, 1552. https://doi.org/10.3390/jcm13061552
Prunea DM, Bachl E, Herold L, Kanoun Schnur SS, Pätzold S, Altmanninger-Sock S, Sommer GA, Glantschnig T, Kolesnik E, Wallner M, et al. Impact of the Timing of Mechanical Circulatory Support on the Outcomes in Myocardial Infarction-Related Cardiogenic Shock: Subanalysis of the PREPARE CS Registry. Journal of Clinical Medicine. 2024; 13(6):1552. https://doi.org/10.3390/jcm13061552
Chicago/Turabian StylePrunea, Dan M., Eva Bachl, Lukas Herold, Sadeek S. Kanoun Schnur, Sascha Pätzold, Siegfried Altmanninger-Sock, Gudrun A. Sommer, Theresa Glantschnig, Ewald Kolesnik, Markus Wallner, and et al. 2024. "Impact of the Timing of Mechanical Circulatory Support on the Outcomes in Myocardial Infarction-Related Cardiogenic Shock: Subanalysis of the PREPARE CS Registry" Journal of Clinical Medicine 13, no. 6: 1552. https://doi.org/10.3390/jcm13061552
APA StylePrunea, D. M., Bachl, E., Herold, L., Kanoun Schnur, S. S., Pätzold, S., Altmanninger-Sock, S., Sommer, G. A., Glantschnig, T., Kolesnik, E., Wallner, M., Ablasser, K., Bugger, H., Buschmann, E., Praschk, A., Fruhwald, F. M., Schmidt, A., von Lewinski, D., & Toth, G. G. (2024). Impact of the Timing of Mechanical Circulatory Support on the Outcomes in Myocardial Infarction-Related Cardiogenic Shock: Subanalysis of the PREPARE CS Registry. Journal of Clinical Medicine, 13(6), 1552. https://doi.org/10.3390/jcm13061552