
The Diagnostic Accuracy of Transcranial Color-Coded Doppler Ultrasound Technique in Stratifying Intracranial Cerebral Artery Stenoses in Cerebrovascular Disease Patients: A Systematic Review and Meta-Analysis

 , and
, and
Abstract

1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Study Characteristics
3.3. Studies’ Methodological Quality Assessment Based on QUADAS 2 Tool
3.4. Diagnostic Accuracy of TCCD Technique for the Detection of Steno-Occlusive Disease
3.4.1. (DSA, MRA, CTA) as Reference Standards
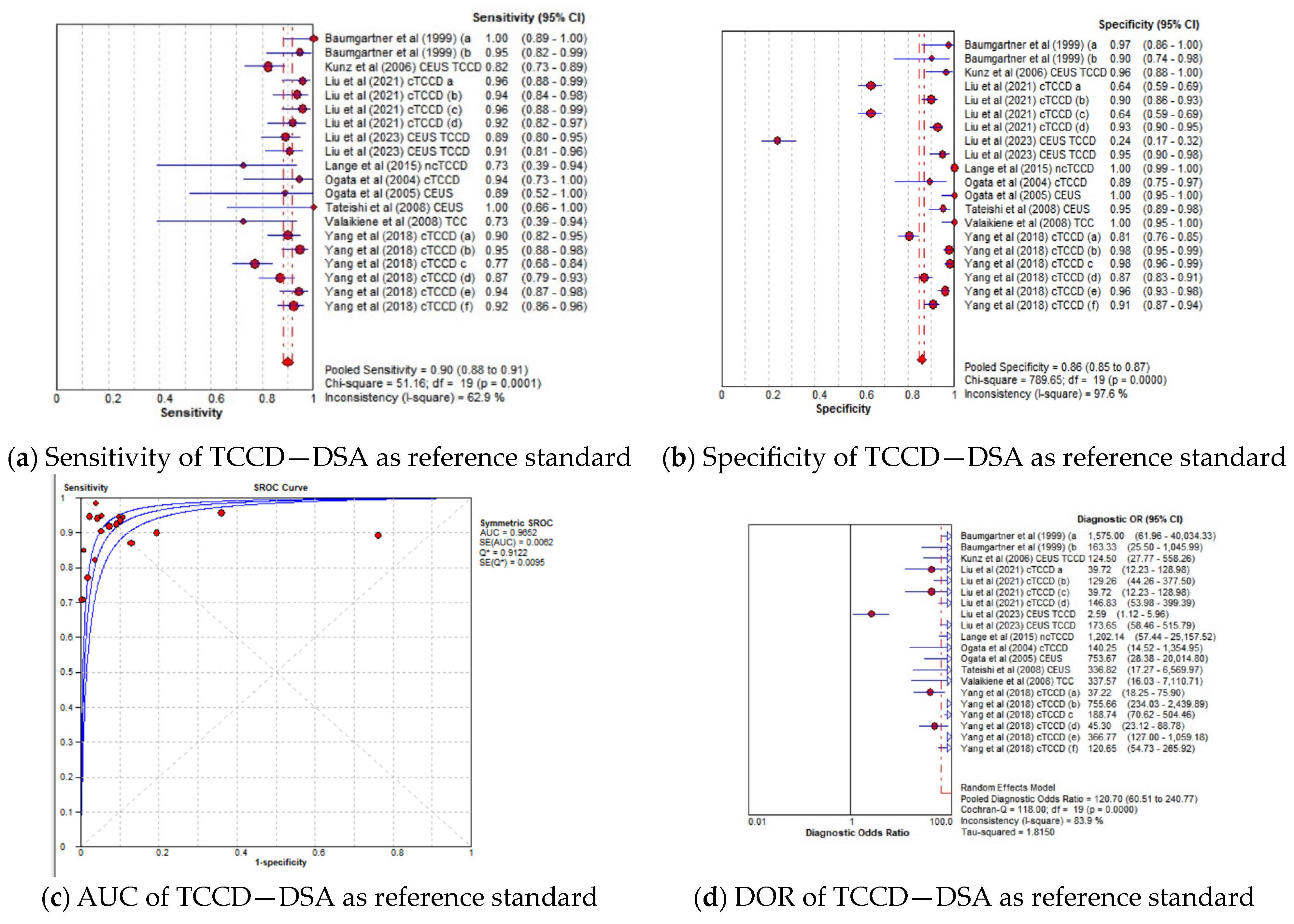
3.4.2. TCCD Compared to Only DSA as Reference Standard
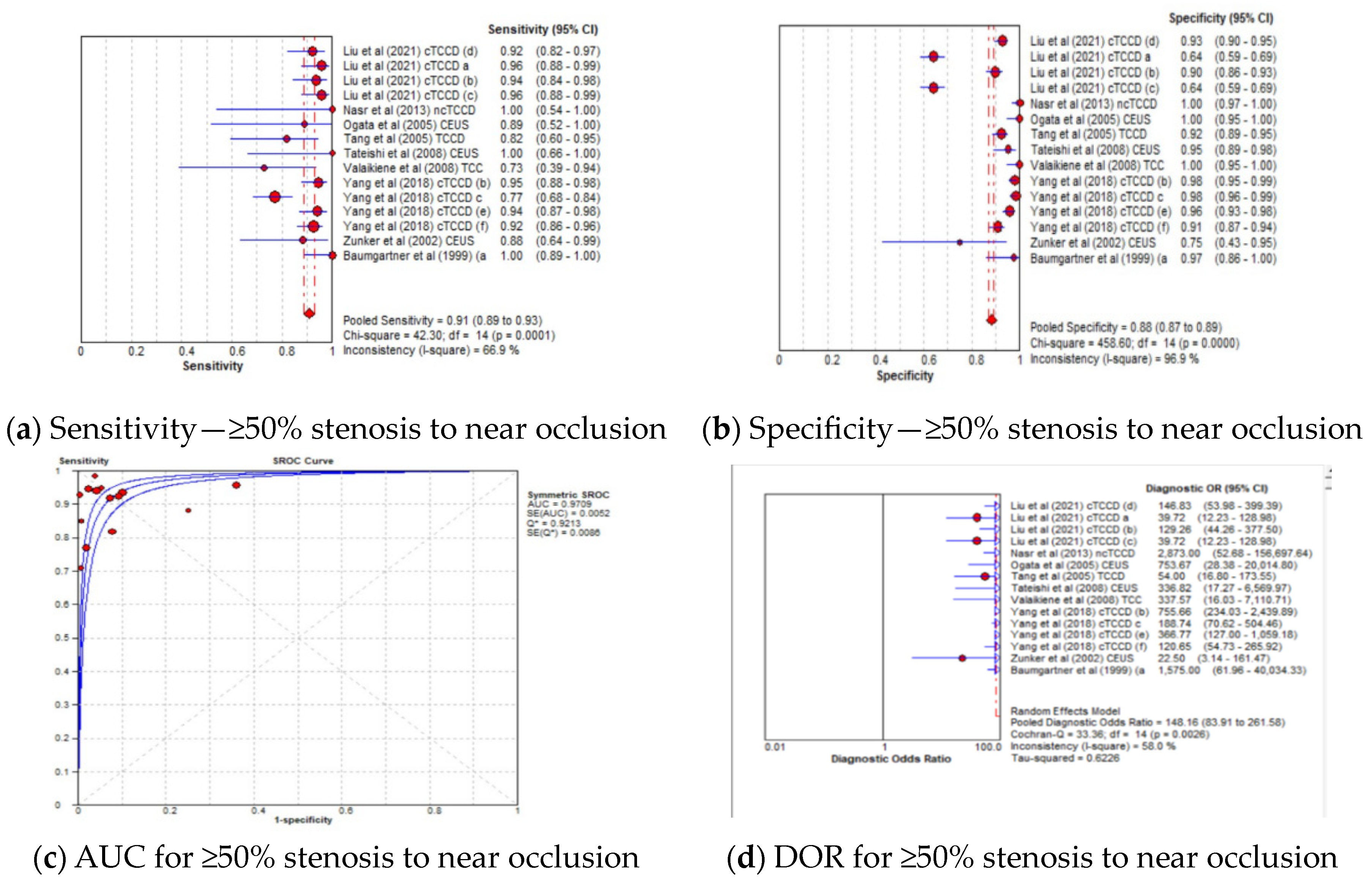
3.4.3. Diagnostic Accuracy of TCCD Technique According to Stenosis Categories
3.4.4. Diagnostic Accuracy of TCCD Technique According to Ultrasound Parameters
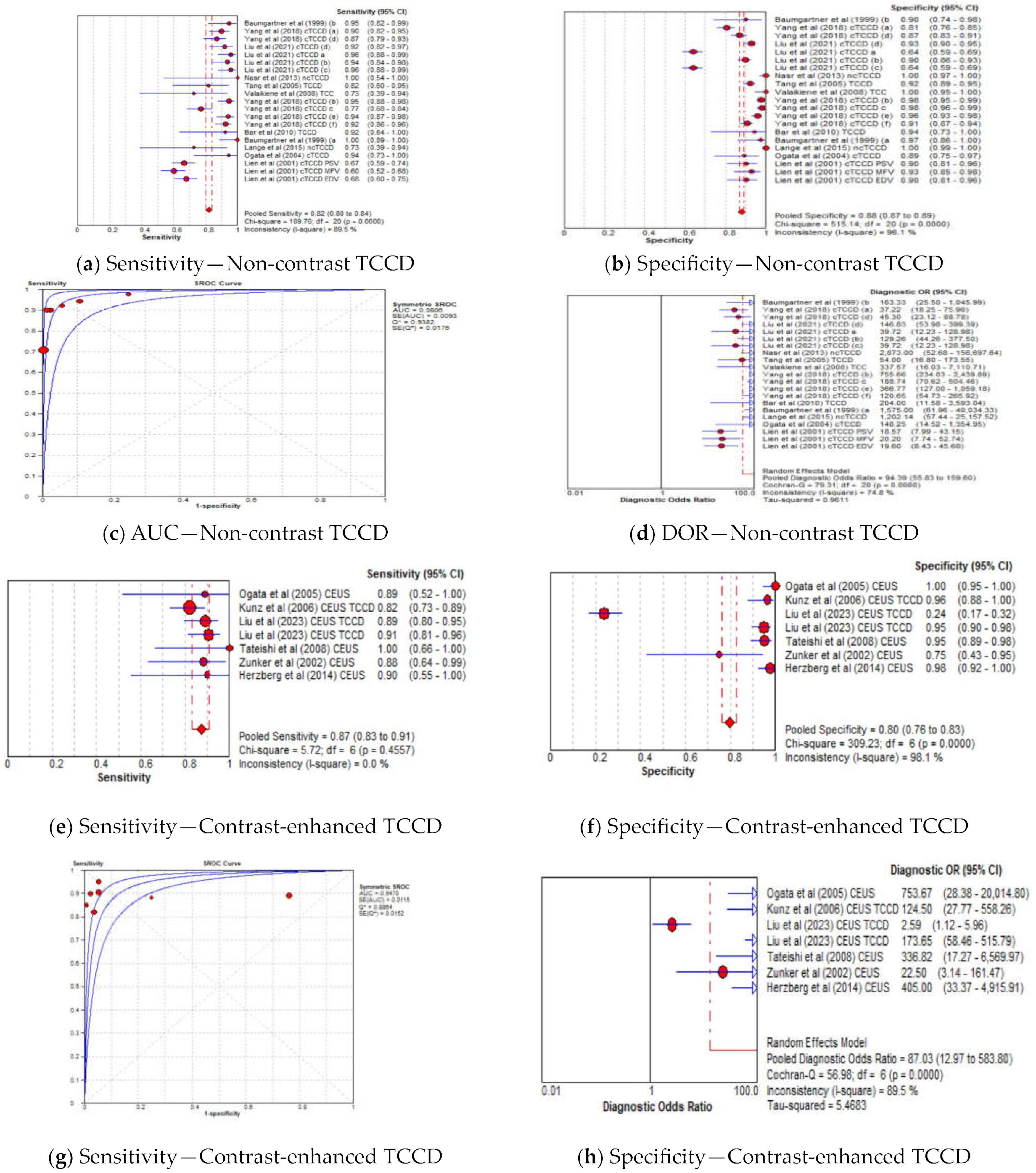
3.4.5. Diagnostic Accuracy of TCCD Based on Contrast-Enhanced and Non-Contrast TCCD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Díez-Tejedor, E.; del Brutto, O.H.; Álvarez-Sabín, J.; Muñoz-Collazos, M.; Abiusi, G.R.P. Clasificación de las enfermedades cerebrovasculares. Sociedad Iberoamericana de ECV. Rev. Neurol. 2001, 33, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Luo, H.; Zhou, J.; Yu, M.; Chen, X.; Tan, L.; Wei, W.; Li, J. Prevalence of stroke and stroke related risk factors: A population based cross sectional survey in southwestern China. BMC Neurol. 2020, 20, 5. [Google Scholar] [CrossRef]
- Esposito, L.; Sievers, M.; Sander, D.; Heider, P.; Wolf, O.; Greil, O.; Zimmer, C.; Poppert, H. Detection of unstable carotid artery stenosis using MRI. J. Neurol. 2007, 254, 1714–1722. [Google Scholar] [CrossRef] [PubMed]
- Brinjikji, W.; Huston, J.; Rabinstein, A.A.; Kim, G.-M.; Lerman, A.; Lanzino, G. Contemporary carotid imaging: From degree of stenosis to plaque vulnerability. J. Neurosurg. 2016, 124, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Neira, J.A.; Connolly, E.S. Indications for Carotid Endarterectomy in Patients with Asymptomatic and Symptomatic Carotid Stenosis. In Stroke, 7th ed.; Grotta, J.C., Albers, G.W., Broderick, J.P., Kasner, S.E., Lo, E.H., Sacco, R.L., Wong, L.K., Day, A.L., Eds.; Elsevier: Philadelphia, PA, USA, 2022; pp. 1084–1090.e2. [Google Scholar]
- Nicolaides, A.N.; Kakkos, S.K.; Kyriacou, E.; Griffin, M.; Sabetai, M.; Thomas, D.J.; Tegos, T.; Geroulakos, G.; Labropoulos, N.; Doré, C.J.; et al. Asymptomatic internal carotid artery stenosis and cerebrovascular risk stratification. J. Vasc. Surg. 2010, 52, 1486–1496.e5. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, M.L.; Kissela, B.; Khoury, J.C.; Alwell, K.; Moomaw, C.J.; Woo, D.; Khatri, P.; Ferioli, S.; Adeoye, O.; Broderick, J.P.; et al. Carotid Artery Stenosis as a Cause of Stroke. Neuroepidemiology 2013, 40, 36–41. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, X.; Liu, L.; Soo, Y.O.; Pu, Y.; Pan, Y.; Wang, Y.; Zou, X.; Leung, T.W.; Cai, Y.; et al. Prevalence and Outcomes of Symptomatic Intracranial Large Artery Stenoses and Occlusions in China. Stroke 2014, 45, 663–669. [Google Scholar] [CrossRef]
- Nguyen-Huynh, M.N.; Wintermark, M.; English, J.; Lam, J.; Vittinghoff, E.; Smith, W.S.; Johnston, S.C. How Accurate Is CT Angiography in Evaluating Intracranial Atherosclerotic Disease? Stroke 2008, 39, 1184–1188. [Google Scholar] [CrossRef]
- Mattioni, A.; Brazzelli, M.; Cenciarelli, S.; Mazzoli, T.; Del Sette, M.; Gandolfo, C.; Marinoni, M.; Finocchi, C.; Saia, V.; Eusebi, P.; et al. Transcranial Doppler sonography for detecting stenosis or occlusion of intracranial arteries in people with acute ischaemic stroke. Cochrane Database Syst. Rev. 2020, 2, Cd010722. [Google Scholar] [CrossRef]
- Naylor, A.R.; Ricco, J.B.; De Borst, G.J.; Debus, S.; De Haro, J.; Halliday, A.; Hamilton, G.; Kakisis, J.; Kakkos, S.; Lepidi, S.; et al. Editor’s Choice—Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 3–81. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.B.; Wong, J.C. A novel method to quantify carotid artery stenosis by Doppler ultrasound: Using the continuity principle. Int. J. Angiol. 2010, 19, e86–e90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saba, L.; Yuan, C.; Hatsukami, T.; Balu, N.; Qiao, Y.; DeMarco, J.; Saam, T.; Moody, A.; Li, D.; Matouk, C.; et al. Carotid Artery Wall Imaging: Perspective and Guidelines from the ASNR Vessel Wall Imaging Study Group and Expert Consensus Recommendations of the American Society of Neuroradiology. Am. J. Neuroradiol. 2018, 39, E9–E31. [Google Scholar] [CrossRef] [PubMed]
- Lovett, M.E.; O’Brien, N.F. Transcranial Doppler Ultrasound, a Review for the Pediatric Intensivist. Children 2022, 9, 727. [Google Scholar] [CrossRef] [PubMed]
- Bartels, E. Transcranial color-coded duplex ultrasonography in routine cerebrovascular diagnostics. Perspect. Med. 2012, 1, 325–330. [Google Scholar] [CrossRef][Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.R.; Bashmail, F.T.; Alzahrani, N.A.; Alharbi, S.I.; Anbar, R.; Alkharaiji, M. Contrast-enhanced ultrasound for the evaluation of symptomatic and asymptomatic carotid plaques: A systematic review and meta-analysis. Echocardiography 2022, 39, 1032–1043. [Google Scholar] [CrossRef]
- Baumgartner, R.W.; Mattle, H.P.; Schroth, G. Assessment of ≥50% and <50% Intracranial Stenoses by Transcranial Color-Coded Duplex Sonography. Stroke 1999, 30, 87–92. [Google Scholar]
- Bar, M.; Školoudík, D.; Roubec, M.; Hradílek, P.; Chmelová, J.; Czerný, D.; Procházka, V.; Langová, K.; Herzig, R. Transcranial duplex sonography and CT angiography in acute stroke patients. J. Neuroimaging 2010, 20, 240–245. [Google Scholar] [CrossRef]
- Nasr, N.; Ssi-Yan-Kai, G.; Guidolin, B.; Bonneville, F.; Larrue, V. Transcranial color-coded sonography to predict recurrent transient ischaemic attack/stroke. Eur. J. Neurol. 2013, 20, 1212–1217. [Google Scholar] [CrossRef]
- Schlachetzki, F.; Herzberg, M.; Hölscher, T.; Ertl, M.; Zimmermann, M.; Ittner, K.P.; Pels, H.; Bogdahn, U.; Boy, S. Transcranial ultrasound from diagnosis to early stroke treatment—Part 2: Prehospital neurosonography in patients with acute stroke—The regensburg stroke mobile project. Cerebrovasc. Dis. 2012, 33, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.C.; Bruch, T.P.; Pedrozo, J.C.; Maranha, L.; Sakae, T.M.; Pacheco, R.; Souza, P.C.; Zétola, V.F. The use of neurovascular ultrasound versus digital subtraction angiography in acute ischemic stroke. Arq. Neuro-Psiquiatr. 2015, 73, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Zunker, P.; Wilms, H.; Brossmann, J.; Georgiadis, D.; Weber, S.; Deuschl, G. Echo contrast-enhanced transcranial ultrasound: Frequency of use, diagnostic benefit, and validity of results compared with MRA. Stroke 2002, 33, 2600–2603. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, J.; Hua, Y.; Li, X.; Gao, M.; Li, Q.; Liu, B.; Jiao, L. The Assessment of Diagnostic Accuracy for Basilar Artery Stenosis by Transcranial Color-Coded Sonography. Ultrasound Med. Biol. 2018, 44, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, Y.; Iguchi, Y.; Kimura, K.; Inoue, T.; Shibazaki, K.; Eguchi, K. Contrast-enhanced transcranial color-coded duplex sonography criteria for basilar artery stenosis. J. Neuroimaging 2008, 18, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Valaikiene, J.; Schuierer, G.; Ziemus, B.; Dietrich, J.; Bogdahn, U.; Schlachetzki, F. Transcranial color-coded duplex sonography for detection of distal internal carotid artery stenosis. Am. J. Neuroradiol. 2008, 29, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Kunz, A.; Hahn, G.; Mucha, D.; Müller, A.; Barrett, K.M.; Von Kummer, R.; Gahn, G. Echo-enhanced transcranial color-coded duplex sonography in the diagnosis of cerebrovascular events: A validation study. Am. J. Neuroradiol. 2006, 27, 2122–2127. [Google Scholar]
- Herzberg, M.; Boy, S.; Hölscher, T.; Ertl, M.; Zimmermann, M.; Ittner, K.P.; Pemmerl, J.; Pels, H.; Bogdahn, U.; Schlachetzki, F. Prehospital stroke diagnostics based on neurological examination and transcranial ultrasound. Crit. Ultrasound J. 2014, 6, 3. [Google Scholar] [CrossRef]
- Tang, S.C.; Jeng, J.S.; Yip, P.K.; Lu, C.J.; Hwang, B.S.; Lin, W.H.; Liu, H.M. Transcranial color-coded sonography for the detection of middle cerebral artery stenosis. J. Ultrasound Med. 2005, 24, 451–457. [Google Scholar] [CrossRef]
- Ogata, T.; Kimura, K.; Nakajima, M.; Ikeno, K.; Naritomi, H.; Minematsu, K. Transcranial color-coded real-time sonographic criteria for occlusion of the middle cerebral artery in acute ischemic stroke. Am. J. Neuroradiol. 2004, 25, 1680–1684. [Google Scholar]
- Lien, L.M.; Chen, W.H.; Chen, J.R.; Chiu, H.C.; Tsai, Y.F.; Choi, W.M.; Reynolds, P.S.; Tegeler, C.H. Comparison of transcranial color-coded sonography and magnetic resonance angiography in acute ischemic stroke. J. Neuroimaging 2001, 11, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Klötzsch, C.; Popescu, O.; Sliwka, U.; Mull, M.; Noth, J. Detection of stenoses in the anterior circulation using frequency-based transcranial color-coded sonography. Ultrasound Med. Biol. 2000, 26, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Gerriets, T.; Seidel, G.; Fiss, I.; Modrau, B.; Kaps, M. Contrast-enhanced transcranial color-coded duplex sonography: Efficiency and validity. Neurology 1999, 52, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Brunser, A.M.; Lavados, P.M.; Hoppe, A.; Lopez, J.; Valenzuela, M.; Rivas, R. Accuracy of transcranial doppler compared with CT angiography in diagnosing arterial obstructions in acute ischemic strokes. Stroke 2009, 40, 2037–2041. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Sharma, V.K.; Hoover, S.L.; Lao, A.Y.; Ardelt, A.A.; Malkoff, M.D.; Alexandrov, A.V. Applications and advantages of power motion-mode Doppler in acute posterior circulation cerebral ischemia. Stroke 2008, 39, 1197–1204. [Google Scholar] [CrossRef]
- Liu, B.; Zhao, B.-Z.; Mu, Y.; Jiang, D. Comparative study on transcranial color-duplex sonography and contrast-enhanced ultrasound with DSA in diagnosis of cerebral arterial stenosis. Chin. J. Med. Imaging Technol. 2006, 22, 880–882. [Google Scholar]
- Ogata, T.; Kimura, K.; Nakajima, M.; Naritomi, H.; Minematsu, K. Diagnosis of middle cerebral artery occlusive lesions with contrast-enhanced transcranial color-coded real-time sonography in acute stroke. Neuroradiology 2005, 47, 256–262. [Google Scholar] [CrossRef]
- Liu, S.; Huang, Z.L.; Sun, Y.R.; Liu, L.; Qi, H.; Wei, L.Y. Application value of transcranial contrast-enhanced ultrasonography in evaluating middle cerebral artery stenosis. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 224–232. [Google Scholar]
- Gerriets, T.; Goertler, M.; Stolz, E.; Postert, T.; Sliwka, U.; Schlachetzki, F.; Seidel, G.; Weber, S.; Kaps, M. Feasibility and validity of transcranial duplex sonography in patients with acute stroke. J. Neurol. Neurosurg. Psychiatry 2002, 73, 17–20. [Google Scholar] [CrossRef]
- Liu, R.; Li, J.; Hua, Y.; Yang, J.; Zhao, Y.; Tian, X.; Ma, Y.; Zhao, W. Transcranial Color-Coded Sonography Criteria for Moderate and Severe Middle Cerebral Artery Stenosis. Ultrasound Med. Biol. 2021, 47, 25–32. [Google Scholar] [CrossRef]
- Baratloo, A.; Hosseini, M.; Negida, A.; El Ashal, G. Part 1: Simple Definition and Calculation of Accuracy, Sensitivity and Specificity. Emergency 2015, 3, 48–49. [Google Scholar] [PubMed]
- Samuels, O.B.; Joseph, G.J.; Lynn, M.J.; Smith, H.A.; Chimowitz, M.I. A standardized method for measuring intracranial arterial stenosis. AJNR Am. J. Neuroradiol. 2000, 21, 643–646. [Google Scholar] [PubMed]
- Stroke Outcomes and Neuroimaging of Intracranial Atherosclerosis (SONIA) Trail Investigators. Stroke Outcomes and Neuroimaging of Intracranial Atherosclerosis (SONIA): Design of a Prospective, Multicenter Trial of Diagnostic Tests. Neuroepidemiology 2004, 23, 23–32. [Google Scholar] [CrossRef]
- Jo, D. The interpretation bias and trap of multicenter clinical research. Korean J. Pain 2020, 33, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, R.; Cavaliere, C.; Soricelli, A.; Salvatore, M.; Pecchia, L.; Franzese, M. Radiomic and Genomic Machine Learning Method Performance for Prostate Cancer Diagnosis: Systematic Literature Review. J. Med. Internet Res. 2021, 23, e22394. [Google Scholar] [CrossRef] [PubMed]
- Heck, D.; Jost, A. Carotid stenosis, stroke, and carotid artery revascularization. Prog. Cardiovasc. Dis. 2021, 65, 49–54. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (s), Publication Year | Ref. | Country | Type of Patient | n—Number of Patients; * n—Number of Stenosis/Occlusions ** n—Number of Datasets According to Reference Standard, *** n—Number of Vessels | Mean Age ± SD (Years) | Gender | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n) | Index + Ref Tests (n) | Accuracy Analysis | No Stenosis | <50% Stenosis | ≥50% Stenosis Near Occlusion | 50−69% | 70−99% | Total Occlusion | ≥50% Stenosis + Total Occlusion | Male (n) | Female (n) | |||||
| Baumgartner et al. (1999) | [19] | Switzerland | CVD–ischemic events | 310 | n/a | * 69 | n/a | * 38 | * 31 | n/a | n/a | 20 | 51 | 56 ± 16 | 208 | 102 |
| Bar et al. (2010) | [20] | Czech Republic | CVD–AIS | 45 | 31 | 31 | n/a | 9 | 0 | n/a | n/a | 22 | 22 | 64.5 ± 13.8 (18–80) | 17 | 14 |
| Lange et al. (2015) | [23] | Brazil | CVD–AIS (21), TIA(3) | 265 | 65 | 24 | n/a | n/a | * 6 | n/a | n/a | * 5 | * 11 | 59.25 ± 14.7 | 14 | 10 |
| Nasr et al. (2013) | [21] | France | CVD–TIA, AIS | 159 | 116 | 116 | n/a | 110 | n/a | n/a | n/a | n/a | 6 | 63.4 ± 16.2 | 86 | 73 |
| Schlachetzki et al. (2012) | [22] | Germany | CVD–AIS | 113 | 102 | 86 | n/a | 76 | 0 | n/a | n/a | 10 | 10 | 80.6 ± 13.52 | 50 | 63 |
| Zunker et al. (2002) | [24] | Germany | CVD | 687 | 29 | 29 | n/a | 14 | 15 | n/a | n/a | n/a | 15 | 64 ± 9 | 419 | 268 |
| Yang et al. (2018) | [25] | China | CVD–(TIA = 298; Stroke = 105) | 403 | 403 | 403 | 93 | 100 | 210 | 92 | 118 | 0 | 210 | 62.7 ± 8.8 | 327 | 76 |
| Tateishi et al. (2008) | [26] | Japan | CVD–(IS = 82, TIA = 7, ICH = 14 | 120 | 120 | 111 | n/a | n/a | 9 | n/a | n/a | 3 | 12 | 65.5 ± 12.3 | 69 | 42 |
| Valaikiene et al. (2008) | [27] | Germany | CVD–IS | 40 | 40 | 40 | * 59 | * 5 | * 8 | * 1 | * 7 | * 4 | * 12 | 58.9 ± 13.8 | 26 | 14 |
| Kunz et al. (2006) | [28] | Germany | CVD | 132 | 132 | ** 164 | ** 24 | n/a | n/a | n/a | n/a | n/a | ** 140 | 58 ± 14 | 92 | 40 |
| Herzberg et al. (2014) | [29] | Germany | CVD–(IS = 73, mimics = 29 | 232 | 102 | 86 | 76 | n/a | n/a | n/a | n/a | 10 | 10 | 76.8 ± 13.4 | 48 | 54 |
| Tang et al. (2005) | [30] | Taiwan | CVD–AIS | 193 | *** 309 | *** 304 | n/a | n/a | *** 304 | n/a | n/a | 0 | *** 304 | 58.3 ± 13.6 | 158 | 35 |
| Ogata et al. (2004) | [31] | Japan | CVD—AIS | 66 | 66 | 55 | 37 | n/a | n/a | n/a | n/a | 18 | 18 | 63.8 ± 13.1 | 46 | 9 |
| Ogata et al. (2005 | [38] | Japan | CVD–AIS | 75 | 75 | 75 | 44 | 9 | 0 | n/a | n/a | 22 | 31 | 64.9 ± 13.1 | 61 | 14 |
| Liu et al. (2021) | [41] | China | CVD (AIS, TIA) | 1471 | 375 | *** 409 | *** 174 | *** 103 | *** 132 | *** 70 | *** 62 | 0 | *** 132 | 62.4 ± 9 | 318 (88.5 | 47 (12.5) |
| Liu et al. (2023) | [39] | China | CVD (MCA stenosis) | 104 | 104 | ** 208 | ** 134 | ** 31 | ** 43 | ** 29 | ** 14 | 0 | ** 43 | n/a (32–81) | 55 (53) | 49 (47) |
| Gerriets et al. (2002) | [40] | Germany and Switzerland | CVD–AIS | 58 | 32 | 32 | 18 | n/a | n/a | n/a | n/a | 10 | 3 | b 64 (38–89) | 36 (62) | 22 (38) |
| Lien et al. (2001) | [32] | Taiwan | CVD–AIS | 120 | 120 | *** 240 | *** 72 | n/a | n/a | n/a | n/a | *** 10 | n/a | 65.1 ± 11.9 | 62 (52) | 58 (48) |
| Author (s), Publication Year | Ref. | Study Design | Type of Ultrasound Machine and Contrast Media | Ultrasound Technique | Reference Standard | Index to Reference Test Mean Time ± SD |
|---|---|---|---|---|---|---|
| Baumgartner et al. (1999) | [19] | Prospective, single center, consecutive patients | Acuson 128 XP/10 equipped with a 2.0/2.5-MHz 90° sector probe | TCCD | DSA | 2 days (0–6) |
| Bar et al. (2010) | [20] | Prospective, single center, consecutive patients | Philips HDI 5000 (ATL, Bothel, WA, USA) equipped with a phased array 2–4-MHz transducer | TCCD | CTA | 12 ± 7.2 (11–20) min |
| Nasr et al. (2013) | [21] | Retrospective, consecutive | Philips IU 22 (PhilipsUltrasound, Bothell, WA, USA). | TCCD | MRA | 4 h |
| Schlachetzki et al. (2012) | [22] | Prospective, single center, consecutive patients | 1. Sonosite Micromaxx equipped with a p17 transducer (sonosite Incl., Bothell, Washington, DC, USA) 2. Philips CX50 with a P2–5 transducer (Philips Ultrasound Bothwell, Wash, USA), | 1. ncTCCD (72) and 2. CEUS ncTCCD (41) | MRA, CTA | 12 ± 7.2 (11–20) min |
| Lange et al. (2015) | [23] | Retrospective, single center, non-consecutive | A portable vascular duplex ultrasound (Vivid E1, GE) equipped with a (1.5–5) MHz phased-array probe | ncTCCD | DSA | 2 ± 1 days |
| Zunker et al. (2002) | [24] | Prospective, single center, consecutive patients | HDI 3000 device (ATL). 2–3 MHz phased-array transducer SH U 508A (Levovist, Schering, Berlin, Germany) | CEUS TCCD | MRA | <90 days |
| Yang et al. (2018) | [25] | Retrospective, single center, non-consecutive | Philips IU22 (Koninklijke Philips N.V., Amsterdam, The Netherlands) and Hitachi Ascendus (Hitachi, Tokyo, Japan) ultrasound systems with 1.0–5.0 MHz phased-array probes | TCCD | DSA | <2 weeks |
| Tateishi et al. (2008) | [26] | Prospective, single center, consecutive patients | HDI 5000 (Philips, Tokyo, Japan) equipped with a phased-array 2–3 MHz transducer C.A—Levovist, Schering, Berlin, Germany | cTCCD + CEUS cTCCD | DSA | <48 h |
| Valaikiene et al. (2008) | [27] | Prospective, single center | (Elegra, 2.5PL20, 7.5L40; Siemens, Issaquah, Wash; or Logiq 500, 2.9/2.0S222, 6.7/5.0L739; GE Healthcare, Tokyo, Japan) (2–3 MHz) phased-array transducer | TCCD-Dist ICA | DSA | 5 ± 4 days, (0–14) days |
| Kunz et al. (2006) | [28] | Prospective, single center | Acuson 128XP/4 (Siemens, Berlin and Munich, Germany) equipped with a 2.0/2.5-MHz phased-array transducer, C.A—Levovist, Schering, Berlin, Germany | TCCD + CEUS TCCD | DSA | 3 ± 3 days (median, 1.5 days) |
| Herzberg et al. (2014) | [29] | Prospective, single center, consecutive patients | 1. Sonosite Micromaxx equipped with a p17 transducer (sonosite Incl., Bothell, WA, USA) 2. Philips CX50 with a P2–5 transducer (Philips Ultrasound Bothwell, Washington, DC, USA) C.A—UCA; SonoVue, Bracco Imaging SpA, Milan, Italy | TCCD + CEUS TCCD | CTA, MRA | n/a |
| Tang et al. (2005) | [30] | Prospective, single center, consecutive patients | Philips 4500 (Philips Medical Systems, Bothell, WA, USA) equipped with a 2.0 MHz transducer | cTCCD | MRA | <7 days |
| Ogata et al. (2004) | [31] | Prospective, single center, consecutive patients | Sonos 5500; Philips Medical Systems, Japan, Tokyo equipped with a 1.0–3.0 MHz phased-array transducer | cTCCD | DSA | 24 h |
| Ogata et al. (2005) | [38] | Prospective, single center, consecutive patients | Sonos 5500; Philips Medical Systems, Japan, Tokyo equipped with a 1.0 –3.0 MHz phased-array transducer | CEUS TCCD | DSA | 23.7 h |
| Liu et al. (2021) | [41] | Retrospective, single center, consecutive patients | Epiq 5 (Philips Medical systems, Amsterdam, The Netherlands) and Hitachi Ascendus (Hitachi, Tokyo, Japan) equipped with a 1–5 MHz phased-array transducer | TCCD | DSA | <2 weeks |
| Liu et al. (2023) | [39] | Prospective, single center, consecutive patients | PHILIPS EPIQ 7 (C) (Philips, Amsterdam, The Netherlands) equipped with a 1–5 MHz phased-array transducer C.A—SonoVue (Bracco, Milan, Italy) | CEUS TCCD | DSA | n/a |
| Gerriets et al. (2002) | [40] | Prospective, multi center, consecutive patients | HP Sonos 2000, 2500, or 5500; Acuson 128 XP/10; Toshiba SSH-140 HGor SSH-380; Siemens Elegra. C.A—Levovist, Schering, Berlin, Germany | TCCD + CEUS cTCCD | DSA (1), MRA (18), CTA (13) | <24 |
| Lien et al. (2001) | [32] | Prospective, single center, consecutive patients | HP 5500 equipped with a 2 MHz phased-array transducer | cTCCD | MRA | 24 h |
| Author (s), Publication Year | Ref. | TCCD Technique | Comparator | Site of Stenosis/Occlusion | Degree of Stenosis | Ultrasound Diagnostic Criteria | TTW Failure n or * n (%) | Sen (%) | Spec (%) | PPV (%) | NPV (%) | DA (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baumgartner et al. (1999) | [19] | TCCD | DSA | Ant + Post circulation | ≥50% | PSV ≥ 220 MCA | * 280/2741 (10) | 100 | 97.4 | 100 | 100 | 97.4 |
| Baumgartner et al. (1999) | [19] | TCCD | DSA | Ant + Post circulation | <50% | PSV ≥ 155 MCA | * 280/2741 (10) | 92.1 | 90.3 | 92.1 | 93 | 91.3 |
| Bar et al. (2010) | [20] | ncTCCD + TCCD-UCA | CTA | Ant + Post circulation | Occlusion | 1. PSV > 220 cm/s 2. absent flow signal + ant arteries visible | 5/45 (11) | 100 | 77.8 | 91.7 | 100 | 93.5 |
| Bar et al. (2010) | [20] | * TCCD | CTA | MCA main sterm | Occlusion | MCA flow signal absent + ant arteries visible | 5/45 (11) | 92.3 | 94.4 | 92.3 | 94.4 | 93.5 |
| Nasr et al. (2013) | [21] | ncTCCD | MRA | Ant + Post circulation MCA M1 (3), PCA P1 (1), VA (1), BA (1) | ≥50% stenosis (5) or occlusion (1) | 1.MCA M1 PSV = 220 cm/s, 2. ACA PSV = 155 cm/s 3. PCA P1 PSV = 145 cm/s, 4. BA PSV = 140 cm/s | 17/159 (10.7) | 100 | 100 | 100 | 100 | 100 |
| Schlachetzki et al. (2012) | [22] | ncTCCD (72) + CEUS TCCD (41) | CTA, MRA | MCA | Occlusion | MFV-asymmetric index > 21%, absent flow | 11/113 (10) | 90 | 98 | 90 | 98 | 98 |
| Lange et al. (2015) | [23] | ncTCCD | DSA | Ant +Post circulation | ≥50−occlusion | Retrograde flow, vessel occlusion signals, or turbulent flow patterns | 11/65 (17) | 72.7 | 100 | 100 | 98.8 | 98.9 |
| Zunker et al. (2002) | [24] | CEUS TCCD | MRA | Ant +Post circulation | ≥50−occlusion | 1. MFV > 80 cm/s (MCA and ICA), 2. MFV > 75 cm/s—ACA), 3. MFV > 60 cm/s (PCA and VA), 4. MFV > 65 BA | 61 (8.8) | 83 | 82 | 83.3 | 82 | 83 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | <50% | PSV ≥ 110 | n/a | 90.3 | 80.6 | 94 | 71.4 | 88.1 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | 50−69% | PSV ≥ 150 | n/a | 94.3 | 97.9 | 98 | 94 | 96 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | 70−99% | PSV ≥ 210 | n/a | 77.1 | 98.2 | 94.5 | 91.2 | 92 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | <50% | MFV ≥ 70 | n/a | 87.4 | 87.1 | 95.8 | 67.5 | 87.3 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | 50−69% | MFV ≥ 90 | n/a | 93.8 | 95.9 | 96.1 | 93.4 | 94.8 |
| Yang et al. (2018) | [25] | cTCCD | DSA | BA | 70−99% | MFV ≥ 120 | n/a | 92.4 | 90.9 | 80.7 | 96.6 | 91.3 |
| Tateishi et al. (2008) | [26] | CEUS TCCD | DSA | BA | >50% | CEUS PSV > 120 cm/s | 6/120 (5) | 100 | 95 | 64 | 100 | 95 |
| Valaikiene et al. (2008) | [27] | TCCD | DSA | Terminal ICA | ≥70% | PSV > 200 cm/s | n/a | 71 | 100 | 100 | 95.8 | 96 |
| Kunz et al. (2006) | [28] | CEUS TCCD | DSA | Ant +Post circulation | >0% | increased MFV, retrograde flow, no signals, or turbulent flow patterns. | 7/164 (4) | 82 | 98 | 99 | 75 | 84 |
| Herzberg et al. (2014) | [29] | CEUS ncTCCD | CTA, MRA | MCA | MCA occlusion | MCA flow signal absent + ant arteries visible | 11/102 (11) | 90 | 98 | 90 | 98 | 97 |
| Tang et al. (2005) | [30] | TCCD | MRA | MCA | >50—near occlusion | PSV ≥ 140 cm/s or PSV < 40 cm/s | 17/193 (8.8) | 81.8 | 92.1 | 48.6 | 98.2 | 65.2 |
| Ogata et al. (2004) | [31] | cTCCD | DSA | MCA | MCA occlusion | EDV = 25 cm/s | n/a | 94 | 81 | 98 | 94 | |
| Ogata et al. (2005) | [38] | CEUS cTCCD | DSA | MCA | >50—MCA stenosis | PSV = 170 cm/s | n/a | 89 | 100 | 100 | 99 | 99.1 |
| Liu et al. (2021) | [41] | cTCCD | DSA | MCA | 50−69% | PSV ≥ 180 cm/s | 553/1471 (37) | 95.7 | 64 | 35.6 | 98.6 | 69.7 |
| Liu et al. (2021) | [41] | cTCCD | DSA | MCA | 70−99% | PSV ≥ 240 cm/s | 553/1471 (37) | 93.5 | 89.9 | 50.7 | 97.7 | 85.5 |
| Liu et al. (2021) | [41] | cTCCD | DSA | MCA | 50−69% | MFV ≥ 110 cm/s | 553/1471 (37) | 95.7 | 64 | 35.4 | 98.6 | 69.4 |
| Liu et al. (2021) | [41] | cTCCD | DSA | MCA | 70−99% | MFV ≥ 160 cm/s | 553/1471 (37) | 91.9 | 92.8 | 69.7 | 97.3 | 92.2 |
| Liu et al. (2023) | [39] | CEUS * TCCD | DSA | MCA | >0% | PSV ≥ 168.5 cm/s | 0/208 (0) | 89.2 | 94.7 | 39.3 | 80 | 97.7 |
| Liu et al. (2023) | [39] | CEUS * TCCD | DSA | MCA | >0% | MFV ≥ 110.5 cm/s | 0/208 (0) | 90.5 | 94.7 | 90.5 | 94.7 | 97.5 |
| Gerriets et al. (2002) | [40] | CEUS cTCCD | DSA, MRA, CTA | MCA | >0% | MFV > 120 cm/s, >21% side to side difference | 4/58 (7)—CEUS TCCD 32/58 (45)—TCCD | n/a | n/a | n/a | n/a | 97 |
| Lien et al. (2001) | [32] | cTCCD | MRA | MCA | >0% | PSV ≥ 120 cm/s | * 89/240 (37) | 66.7 | 90.5 | 93.9 | 55.1 | 78.6 |
| Lien et al. (2001) | [32] | cTCCD | MRA | MCA | >0% | MFV ≥ 85 cm/s | * 89/240 (37) | 59.9 | 92.9 | 94.8 | 50.6 | 76 |
| Lien et al. (2001) | [32] | cTCCD | MRA | MCA | >0% | EDV ≥ 85 cm/s | * 89/240 (37) | 52.7 | 90.5 | 92.5 | 46.3 | 71.6 |
| Study Author, Date | Ref. | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | ||
| Baumgartner et al. (1999) | [19] | Low | Low | Low | Low | Low | Low | Low |
| Bar et al. (2010) | [20] | Low | Low | Low | Low | Low | Low | Low |
| Nasr et al. (2013) | [21] | High | Low | Low | Low | Low | Low | Low |
| Schlachetzki et al. (2012) | [22] | Low | Low | High | Low | Low | Low | High |
| Lange et al. (2015) | [23] | High | High | Low | Low | High | High | Low |
| Zunker et al. (2002) | [24] | High | Low | Low | Low | High | Low | Low |
| Yang et al. (2018) | [25] | High | Low | Low | Low | High | Low | Low |
| Tateishi et al. (2008) | [26] | Low | Low | Low | Low | Low | Low | Low |
| Valaikiene et al. (2008) | [27] | Low | Low | Low | Unclear | Low | Low | Low |
| Kunz et al. (2006) | [28] | Low | Low | Low | Low | Low | High | Low |
| Herzberg et al. (2014) | [29] | Low | Low | High | Low | Low | Low | High |
| Tang et al. (2005) | [30] | Low | Low | Low | Low | Low | Low | Low |
| Ogata et al. (2004) | [31] | Low | Low | Low | Low | Low | Low | Low |
| Ogata et al. (2005 | [38] | Low | Low | Low | Low | Low | Low | Low |
| Liu et al. (2021) | [41] | Low | Low | Low | Low | Low | Low | Low |
| Liu et al. (2023) | [39] | Low | High | Low | Low | Low | Low | low |
| Gerriets et al. (2002) | [40] | Low | High | High | Low | Low | Low | High |
| Lien et al. (2001) | [32] | Low | Low | Low | Low | Low | Low | Low |
| Category | Sensitivity (%)—95% CI | Specificity (%)—95% CI | AUC | DOR—95% CI |
|---|---|---|---|---|
| (All angiographies—DSA, MRA, CTA) as reference standards | 83 (81–85) | 87 (86–88) | 0.96 | 98 (56–169) |
| DSA alone as reference standard | 90 (88–91) | 86 (85–87) | 0.97 | 121 (61–169) |
| Stratifying stenosis ≥50% to near occlusion (all angiographies) | 91 (89–93) | 88 (87–89) | 0.97 | 148 (84–262) |
| Total occlusions | 92 (84–97) | 98 (96–99) | 0.98 | 148 (84–262) |
| PSV as diagnostic parameter | 85 (82–87) | 85 (84–87) | 0.96 | 106 (39–288) |
| MFV as diagnostic parameter | 84 (81–87) | 87 (85–88) | 0.96 | 79 (39–157) |
| non-contrast TCCD | 82 (80–84) | 88 (87–89) | 0.98 | 94 (56–160) |
| contrast-enhanced TCCD | 87 (83–91) | 80 (76–83%) | 0.95 | 87 (13–584) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunda, S.T.; Yip, J.H.-Y.; Ng, V.T.-K.; Chen, Z.; Han, X.; Chen, X.; Pang, M.Y.-C.; Ying, M.T.-C. The Diagnostic Accuracy of Transcranial Color-Coded Doppler Ultrasound Technique in Stratifying Intracranial Cerebral Artery Stenoses in Cerebrovascular Disease Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 1507. https://doi.org/10.3390/jcm13051507
Gunda ST, Yip JH-Y, Ng VT-K, Chen Z, Han X, Chen X, Pang MY-C, Ying MT-C. The Diagnostic Accuracy of Transcranial Color-Coded Doppler Ultrasound Technique in Stratifying Intracranial Cerebral Artery Stenoses in Cerebrovascular Disease Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(5):1507. https://doi.org/10.3390/jcm13051507
Chicago/Turabian StyleGunda, Simon Takadiyi, Jerica Hiu-Yui Yip, Veronica Tsam-Kit Ng, Ziman Chen, Xinyang Han, Xiangyan Chen, Marco Yiu-Chung Pang, and Michael Tin-Cheung Ying. 2024. "The Diagnostic Accuracy of Transcranial Color-Coded Doppler Ultrasound Technique in Stratifying Intracranial Cerebral Artery Stenoses in Cerebrovascular Disease Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 5: 1507. https://doi.org/10.3390/jcm13051507
APA StyleGunda, S. T., Yip, J. H.-Y., Ng, V. T.-K., Chen, Z., Han, X., Chen, X., Pang, M. Y.-C., & Ying, M. T.-C. (2024). The Diagnostic Accuracy of Transcranial Color-Coded Doppler Ultrasound Technique in Stratifying Intracranial Cerebral Artery Stenoses in Cerebrovascular Disease Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(5), 1507. https://doi.org/10.3390/jcm13051507