
Hidden Blood Loss and Its Risk Factors for Oblique Lumbar Interbody Fusion



Abstract
1. Introduction
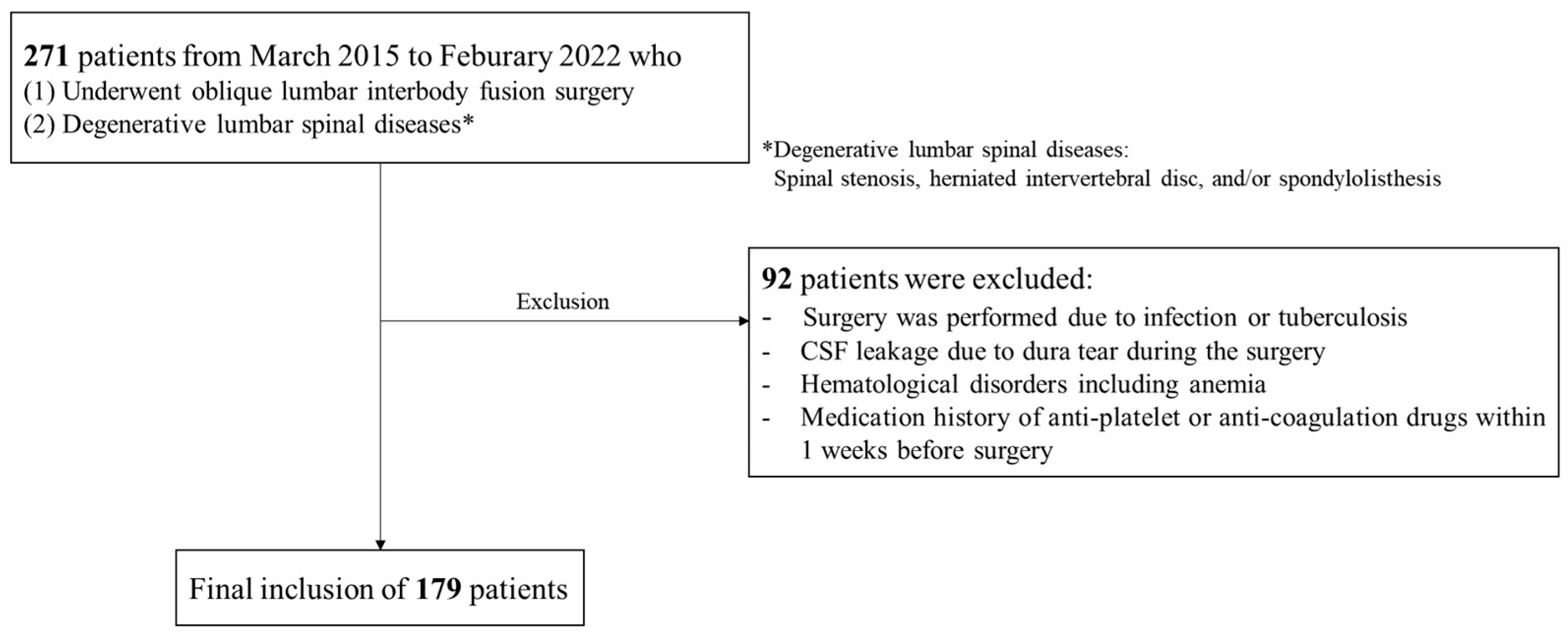
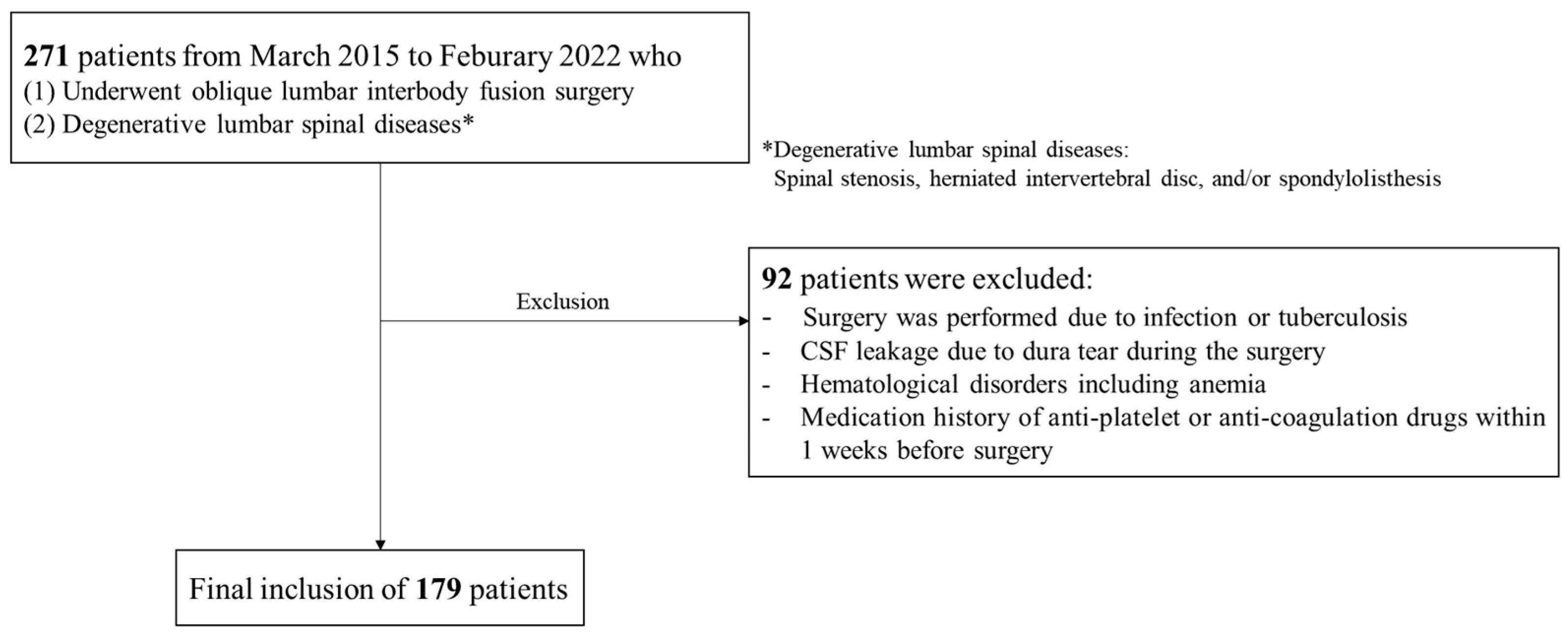
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
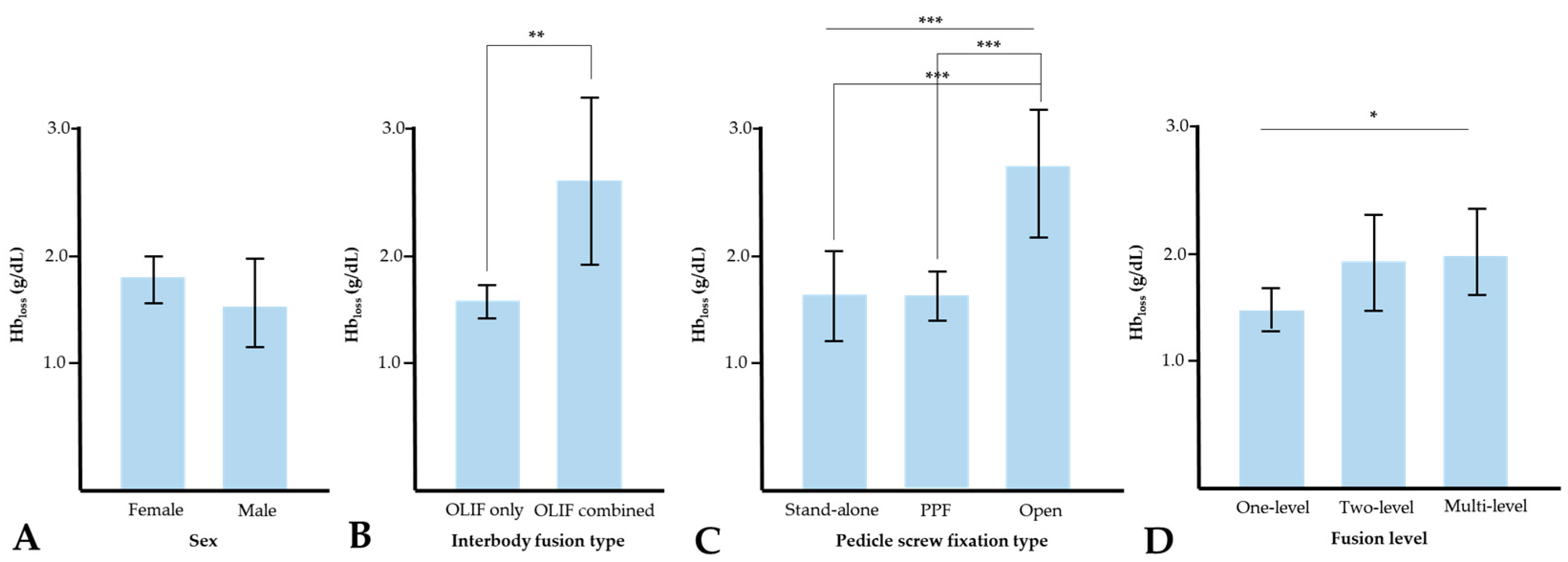
3.2. Blood Loss
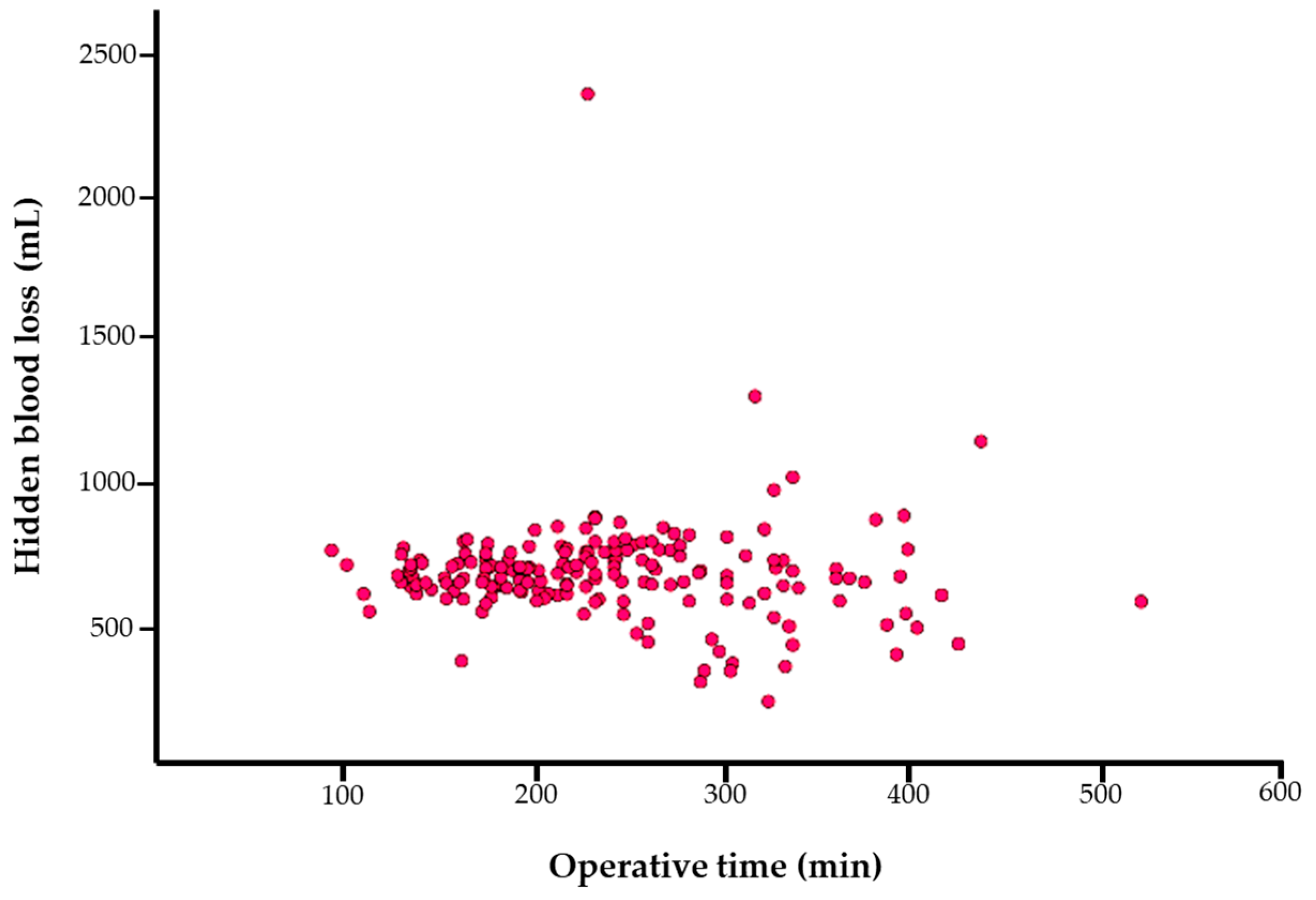
3.3. Correlation Analysis and Multivariate Linear Regression Analysis for HBL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bible, J.E.; Mirza, M.; Knaub, M.A. Blood-loss Management in Spine Surgery. J. Am. Acad. Orthop. Surg. 2018, 26, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yang, J.H.; Chang, D.G.; Lenke, L.G.; Suh, S.W.; Nam, Y.; Park, S.C.; Suk, S.I. Adult Spinal Deformity: A Comprehensive Review of Current Advances and Future Directions. Asian Spine J. 2022, 16, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Yang, J.H.; Chang, D.G.; Suk, S.I.; Suh, S.W.; Kim, S.I.; Song, K.S.; Park, J.B.; Cho, W. Proximal Junctional Kyphosis in Adult Spinal Deformity: Definition, Classification, Risk Factors, and Prevention Strategies. Asian Spine J. 2022, 16, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lenke, L.G.; Pizones, J.; Castelein, R.; Trobisch, P.D.; Yagi, M.; Kelly, M.P.; Chang, D.G. Adolescent Idiopathic Scoliosis: Is the Feasible Option of Minimally Invasive Surgery using Posterior Approach? Asian Spine J. 2023. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Ou, C.Y. Significant Blood Loss in Lumbar Fusion Surgery for Degenerative Spine. World Neurosurg. 2015, 84, 780–785. [Google Scholar] [CrossRef]
- Li, J.X.; Phan, K.; Mobbs, R. Oblique Lumbar Interbody Fusion: Technical Aspects, Operative Outcomes, and Complications. World Neurosurg. 2017, 98, 113–123. [Google Scholar] [CrossRef]
- Xie, T.; Wang, C.; Yang, Z.; Xiu, P.; Yang, X.; Wang, X.; Wang, D.; Song, Y.; Zeng, J. Minimally Invasive Oblique Lateral Lumbar Interbody Fusion Combined with Anterolateral Screw Fixation for Lumbar Degenerative Disc Disease. World Neurosurg. 2020, 135, e671–e678. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, K.; Jian, F.; Wu, H. Efficacy of Oblique Lateral Interbody Fusion in Treatment of Degenerative Lumbar Disease. World Neurosurg. 2018, 17, e17–e24. [Google Scholar] [CrossRef]
- Liu, A.F.; Guo, T.C.; Chen, J.X.; Yu, W.J.; Feng, H.C.; Niu, P.Y.; Zhai, J.B. Efficacy and Safety of Oblique Lumbar Interbody Fusion Versus Transforaminal Lumbar Interbody Fusion for Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta-Analysis. World Neurosurg. 2022, 158, e964–e974. [Google Scholar] [CrossRef]
- Ouyang, P.; Tan, Q.; He, X.; Zhao, B. Computational comparison of anterior lumbar interbody fusion and oblique lumbar interbody fusion with various supplementary fixation systems: A finite element analysis. J. Orthop. Surg. Res. 2023, 18, 4. [Google Scholar] [CrossRef]
- Cao, S.; Fan, B.; Song, X.; Wang, Y.; Yin, W. Oblique lateral interbody fusion (OLIF) compared with unilateral biportal endoscopic lumbar interbody fusion (ULIF) for degenerative lumbar spondylolisthesis: A 2-year follow-up study. J. Orthop. Surg. Res. 2023, 18, 621. [Google Scholar] [CrossRef]
- Chen, H.; Zheng, G.; Bian, Z.; Hou, C.; Li, M.; Zhang, Z.; Zhu, L.; Wang, X. Comparison of minimally invasive transforaminal lumbar interbody fusion and endoscopic lumbar interbody fusion for lumbar degenerative diseases: A retrospective observational study. J. Orthop. Surg. Res. 2023, 18, 389. [Google Scholar] [CrossRef] [PubMed]
- Ogura, Y.; Dimar Ii, J.R.; Gum, J.L.; Crawford, C.H., 3rd; Djurasovic, M.; Glassman, S.D.; Carreon, L.Y. Hidden blood loss following 2- to 3-level posterior lumbar fusion. Spine J. 2019, 19, 2003–2006. [Google Scholar] [CrossRef] [PubMed]
- Ju, H.; Hart, R.A. Hidden blood loss in anterior lumbar interbody fusion (ALIF) surgery. Orthop. Traumatol. Surg. Res. 2016, 102, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Lei, F.; Li, Z.; He, W.; Tian, X.; Zheng, L.; Kang, J.; Feng, D. Total and hidden blood loss between open posterior lumbar interbody fusion and transforaminal lumbar interbody fusion by Wiltse approach. Medicine 2020, 99, e19864. [Google Scholar] [CrossRef] [PubMed]
- Lei, F.; Li, Z.; He, W.; Tian, X.; Zheng, L.; Kang, J.; Feng, D. Hidden blood loss and the risk factors after posterior lumbar fusion surgery: A retrospective study. Medicine 2020, 99, e20103. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Gu, Y. Hybrid surgery of percutaneous transforaminal endoscopic surgery (PTES) combined with OLIF and anterolateral screws rod fixation for treatment of multi-level lumbar degenerative diseases with intervertebral instability. J. Orthop. Surg. Res. 2023, 18, 117. [Google Scholar] [CrossRef]
- Jiang, H.; Sheng, W.; Yuan, H.; Xu, J.; Chen, X.; Gu, X.; Li, S. Hidden blood loss between percutaneous pedicle screw fixation and the mini-open Wiltse approach with pedicle screw fixation for neurologically intact thoracolumbar fractures: A retrospective study. J. Orthop. Surg. Res. 2023, 18, 113. [Google Scholar] [CrossRef]
- Miscusi, M.; Ramieri, A.; Forcato, S.; Giuffrè, M.; Trungu, S.; Cimatti, M.; Pesce, A.; Familiari, P.; Piazza, A.; Carnevali, C.; et al. Comparison of pure lateral and oblique lateral inter-body fusion for treatment of lumbar degenerative disk disease: A multicentric cohort study. Eur. Spine J. 2018, 27, 222–228. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, L.; Shan, Y.; Feng, X.; Zhang, W. Analysis of Hidden Blood Loss and its Risk Factors in Oblique Lateral Interbody Fusion Surgery. Clin. Spine Surg. 2021, 34, E501–E505. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar]
- Gross, J.B. Estimating allowable blood loss: Corrected for dilution. Anesthesiology 1983, 58, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Feng, D.P.; Wu, K.L.; Zhu, J.Y.; Li, Z.W. Hidden blood loss of minimally invasive hybrid lumbar interbody fusion: An analysis of influencing factors. BMC Musculoskelet. Disord. 2022, 23, 1099. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Jin, D.; Xie, W.; Li, Y.; Chen, W.; Ding, J.; Xu, J.; Ren, D. Hidden Blood Loss in Posterior Lumbar Fusion Surgery: An Analysis of Risk Factors. Clin. Spine Surg. 2018, 31, 180–184. [Google Scholar] [CrossRef]
- Yue, X.; Zhang, J.; Sun, T.; Zhang, W.; Yang, M.; Li, Z. Hidden blood loss and its influencing factors after minimally invasive percutaneous transpedicular screw fixation in thoracolumbar fracture. BMC Musculoskelet. Disord. 2022, 23, 959. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, S.; Montane-Muntane, M.; Capitan, D.; Aguilar, F.; Vilaseca, A.; Blasi, A.; Navarro-Ripoll, R. Agreement of surgical blood loss estimation methods. Transfusion 2019, 59, 508–515. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cases (n = 179) |
|---|---|
| Age (years) | 67.8 ± 8.9 * |
| Sex (n) Female Male | 129 (72.1%) 50 (27.9%) |
| Height (cm) | 156.3 ± 9.0 * |
| Weight (kg) | 61.1 ± 11.5 * |
| BMI (kg/m2) | 25.0 ± 3.7 * |
| Underlying disease (n) Hypertension Diabetic mellitus | 94 (52.5%) 44 (24.6%) |
| Disease type (n) Spinal stenosis Spondylolisthesis Mixed | 129 (70.4%) 26 (14.5%) 24 (13.4%) |
| ASA classification (n) I II III | 8 (4.5%) 124 (69.3%) 47 (26.2%) |
| Operative time (min) | 237.1 ± 78.8 * |
| Interbody fusion level (n) One-level Two-level Multi-level | 94 (52.5%) 51 (28.5%) 34 (19.0%) |
| Interbody fusion type (n) OLIF only OLIF combined (OLIF + ALIF/TLIF/PLIF) | 158 (87.2%) 23 (12.8%) |
| Pedicle screw fixation type (n) Stand-alone PPF Open pedicle screw fixation | 34 (19.0%) 121 (67.6%) 24 (13.4%) |
| Perioperative complications (n) Endplate breakage ALL rupture Blood transfusion (n) | 38 (21.0%) 21 (11.7%) 32 (17.9%) |
| Variables | Cases (n = 179) |
|---|---|
| EBL (mL) | 179.3 ± 374.0 |
| TBL (mL) | 846.7 ± 663.8 |
| HBL (mL) | 675.2 ± 741.4 |
| Drain amount (mL) | 115.2 ± 175.1 |
| Hbloss (g/dL) | 1.7 ± 1.1 |
| Variable | Preop Day | Op Day | POD 1 | POD 2 | POD 4 | POD 7 |
|---|---|---|---|---|---|---|
| Hb (g/dL) | 13.2 ± 1.3 | 12.0 ± 1.3 | 11.5 ± 1.3 | 11.0 ± 1.4 | 10.7 ± 1.4 | 11.0 ± 1.5 |
| Hct (%) | 39.7 ± 3.8 | 36.1 ± 3.8 | 36.0 ± 23.9 | 32.6 ± 4.0 | 31.4 ± 4.9 | 32.9 ± 4.2 |
| Platelet (×103/µL) | 243.7 ± 69.0 | 224.0 ± 132.4 | 196.5 ± 55.5 | 177.7 ± 49.6 | 214.1 ± 61.6 | 267.9 ± 77.8 |
| PT (s) | 12.7 ± 0.6 | 13.5 ± 0.7 | 15.4 ± 13.7 | 14.2 ± 1.6 | 13.6 ± 0.9 | 13.4 ± 0.8 |
| PT INR | 1.0 ± 0.1 | 1.0 ± 0.1 | 1.1 ± 0.1 | 1.5 ± 0.3 | 1.1 ± 0.1 | 1.0 ± 0.1 |
| aPTT (s) | 33.9 ± 5.9 | 32.8 ± 6.5 | 35.5 ± 5.3 | 42.0 ± 11.6 | 50.8 ± 14.6 | 47.4 ± 13.2 |
| Drain amount (mL) | N/A | N/A | 92.8 ± 149.1 | 42.8 ± 51.4 | 42.8 ± 51.4 | N/A |
| Variables | Correlation Coefficient | p |
|---|---|---|
| Age | −0.036 | 0.634 |
| Height | 0.234 | 0.002 |
| Weight | 0.163 | 0.030 |
| BMI | 0.015 | 0.845 |
| Operative time | −0.058 | 0.441 |
| Preoperative Hb | 0.280 | <0.001 |
| Preoperative Hct | 0.288 | <0.001 |
| Preoperative platelet | −0.108 | 0.152 |
| PT | 0.022 | 0.775 |
| PT INR | 0.046 | 0.541 |
| aPTT | −0.043 | 0.568 |
| TBL | 0.876 | <0.001 |
| EBL | −0.447 | <0.001 |
| Hbloss | 0.386 | <0.001 |
| Sex | 0.171 | 0.005 |
| Hypertension | −0.109 | 0.076 |
| Diabetic mellitus | 0.047 | 0.443 |
| Disease type | −0.106 | 0.074 |
| ASA classification | −0.194 | 0.001 |
| Interbody fusion level | −0.101 | 0.084 |
| Interbody fusion type | 0.105 | 0.083 |
| Pedicle screw fixation type | 0.214 | <0.001 |
| Endplate breakage | 0.037 | 0.542 |
| ALL rupture | 0.207 | 0.001 |
| Coefficients for HBL | Unstandardized | Standardized | t | p | |
|---|---|---|---|---|---|
| Beta | SE | Beta | |||
| Constant | −16.758 | 10.765 | −1.557 | 0.121 | |
| TBL | 0.996 | 0.006 | 0.899 | 174.895 | <0.001 |
| EBL | −0.935 | 0.011 | −0.470 | −81.788 | <0.001 |
| Pedicle screw fixation type | 11.256 | 5.408 | 0.012 | 2.081 | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.H.; Kim, H.J.; An, M.; Suh, S.W.; Chang, D.G. Hidden Blood Loss and Its Risk Factors for Oblique Lumbar Interbody Fusion. J. Clin. Med. 2024, 13, 1454. https://doi.org/10.3390/jcm13051454
Yang JH, Kim HJ, An M, Suh SW, Chang DG. Hidden Blood Loss and Its Risk Factors for Oblique Lumbar Interbody Fusion. Journal of Clinical Medicine. 2024; 13(5):1454. https://doi.org/10.3390/jcm13051454
Chicago/Turabian StyleYang, Jae Hyuk, Hong Jin Kim, Minsu An, Seung Woo Suh, and Dong Gune Chang. 2024. "Hidden Blood Loss and Its Risk Factors for Oblique Lumbar Interbody Fusion" Journal of Clinical Medicine 13, no. 5: 1454. https://doi.org/10.3390/jcm13051454
APA StyleYang, J. H., Kim, H. J., An, M., Suh, S. W., & Chang, D. G. (2024). Hidden Blood Loss and Its Risk Factors for Oblique Lumbar Interbody Fusion. Journal of Clinical Medicine, 13(5), 1454. https://doi.org/10.3390/jcm13051454