
Evaluating the Effects of an Enhanced Strength Training Program in Remote Cardiological Rehabilitation: A Shift from Aerobic Dominance—A Pilot Randomized Controlled Trial




Abstract
1. Introduction
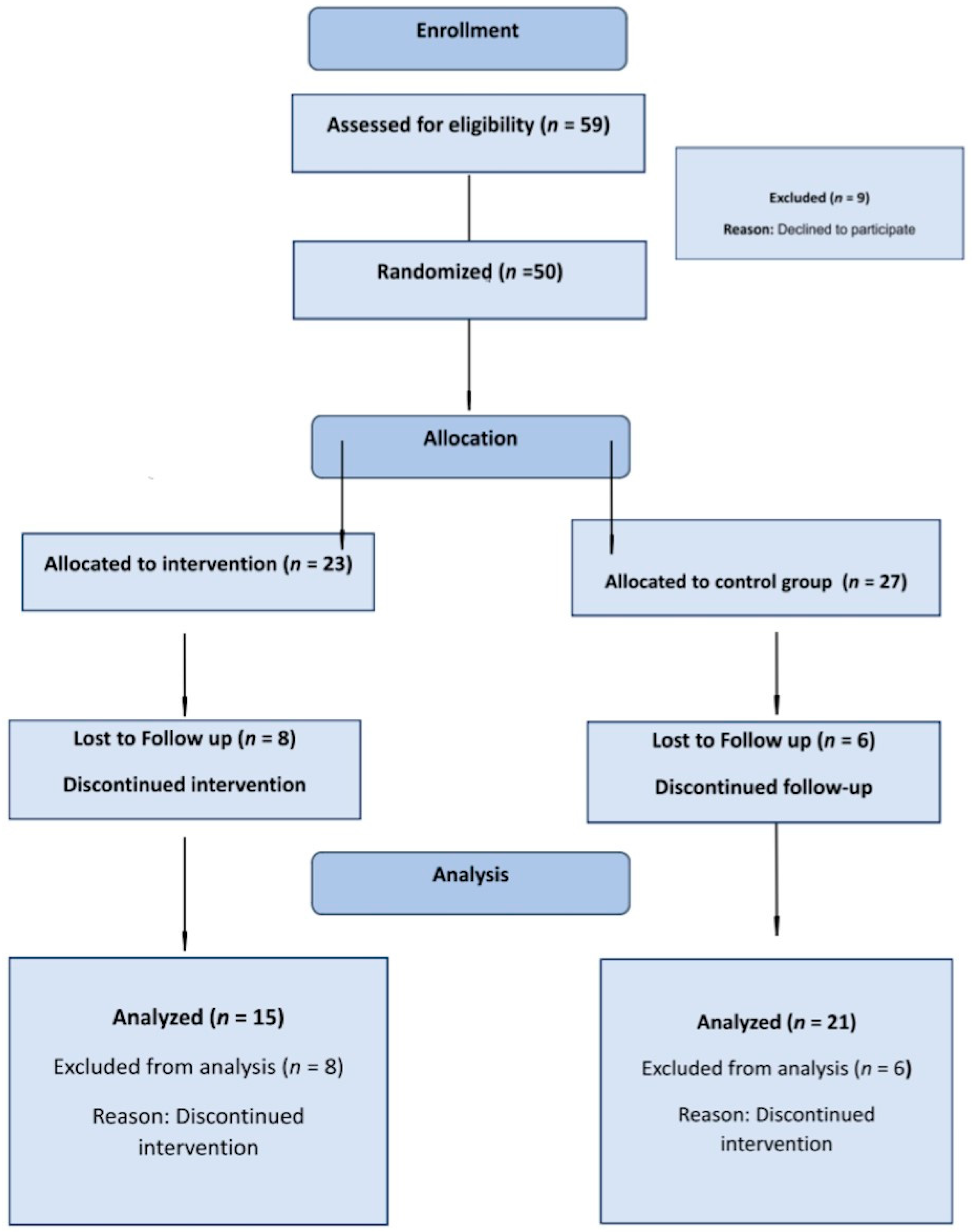
2. Materials and Methods
2.1. The Muscle Endurance Tests
2.2. The Secondary Endpoints Were
- (1)
- Functional capability changes were evaluated using functional assessments (explanation below).
- (2)
- Cardiorespiratory fitness was evaluated by defining metabolic equivalents (METs) using a stress test on treadmill with the Bruce Protocol [17]. The assessments were conducted by the patient care team at the rehabilitation center, with team members kept unaware of the participants’ affiliation with the research groups.Assessments were conducted at the commencement of the rehabilitation program and subsequently after a 4-month intervention period.
- (3)
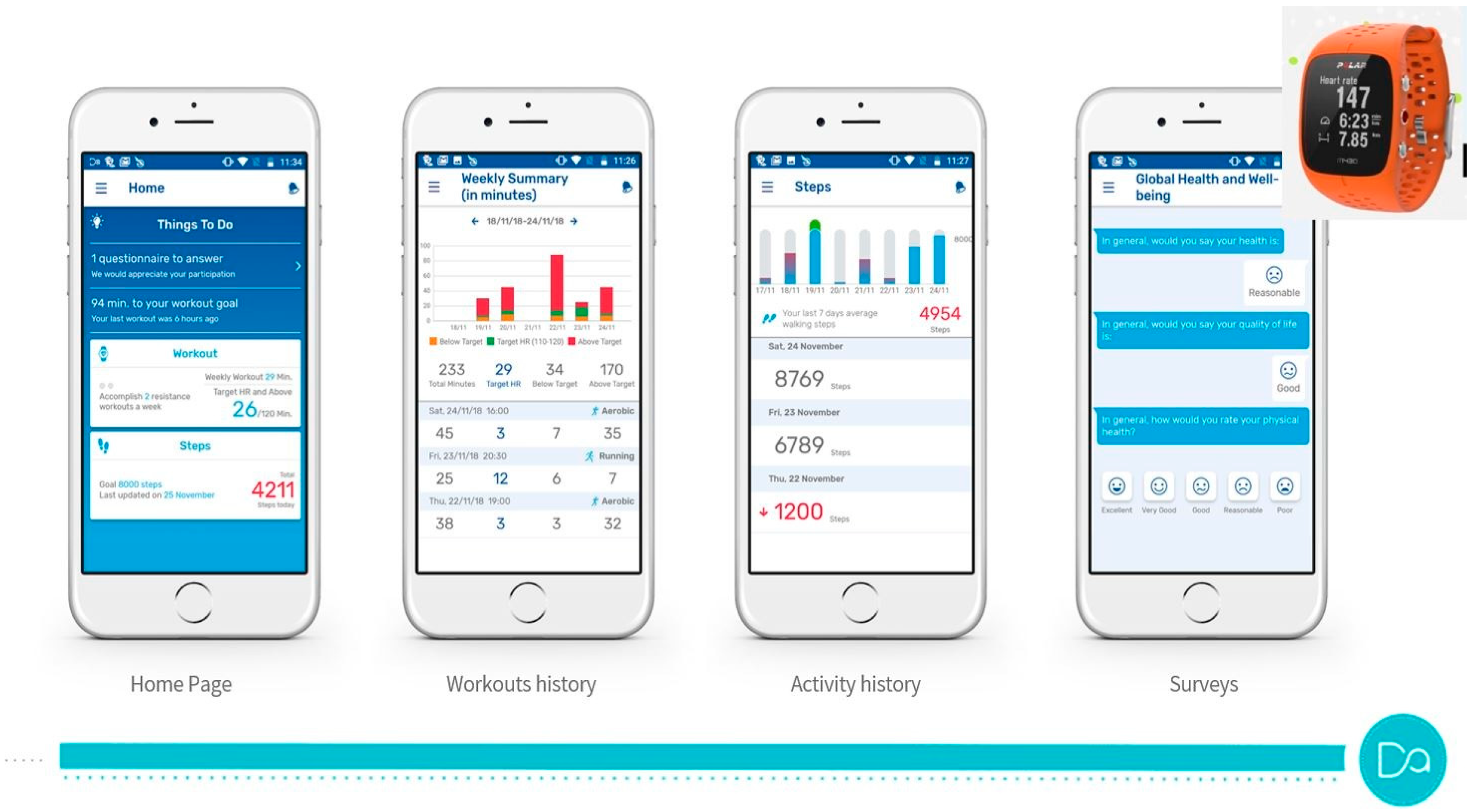
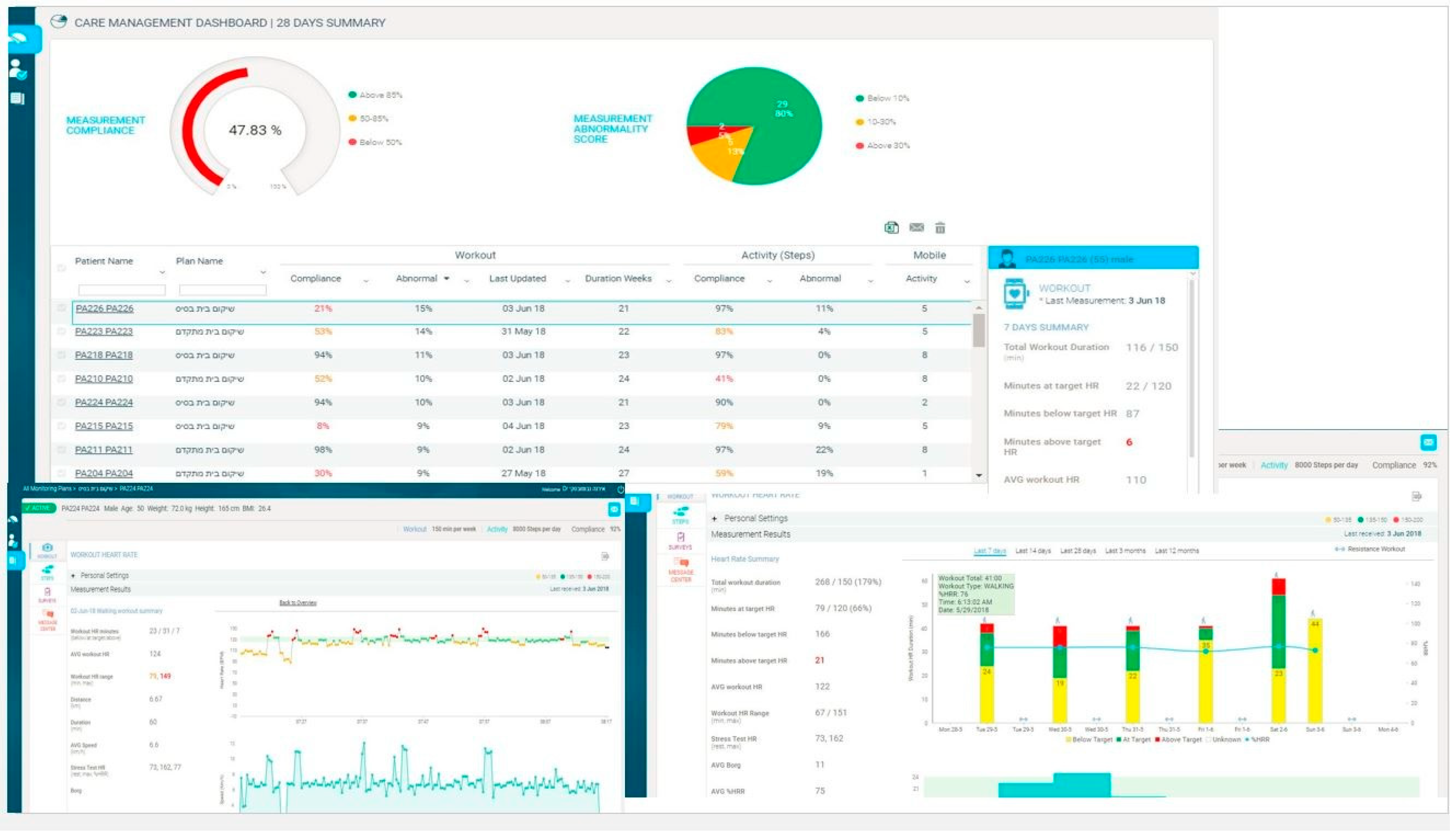
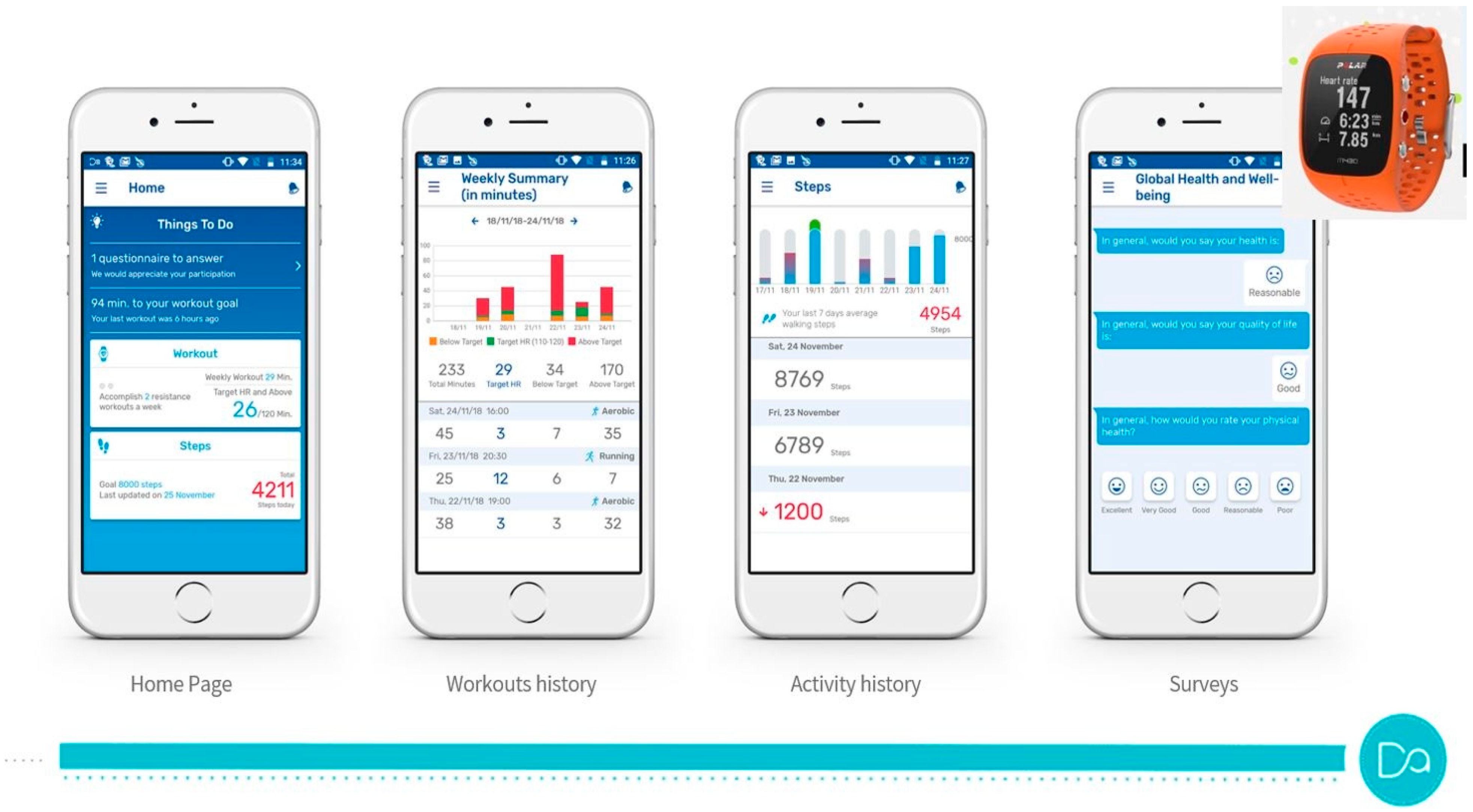
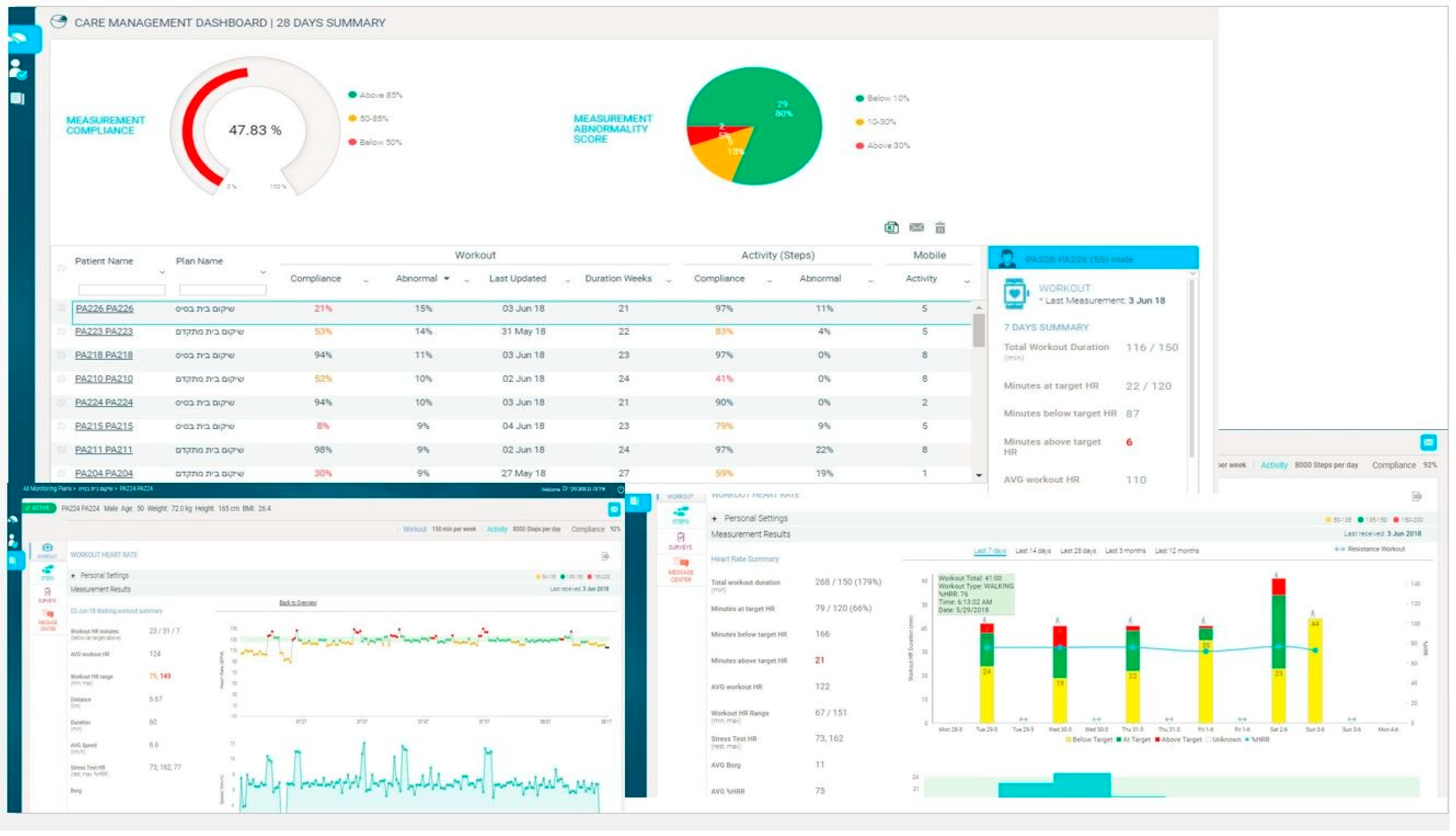
- Compliance and adherence: The following variables were evaluated longitudinally during each week of the program: the total number of minutes of aerobic exercise (aerobic minutes), the number of aerobic minutes in the target heart rate, the assessment of perceived Borg scale, the number of training sessions, the number of daily steps, the use of the RCR mobile app (number of weekly entries). The duration of participation in the CR program (number of weeks) was also noted.
- (4)
2.3. Functional Assessments
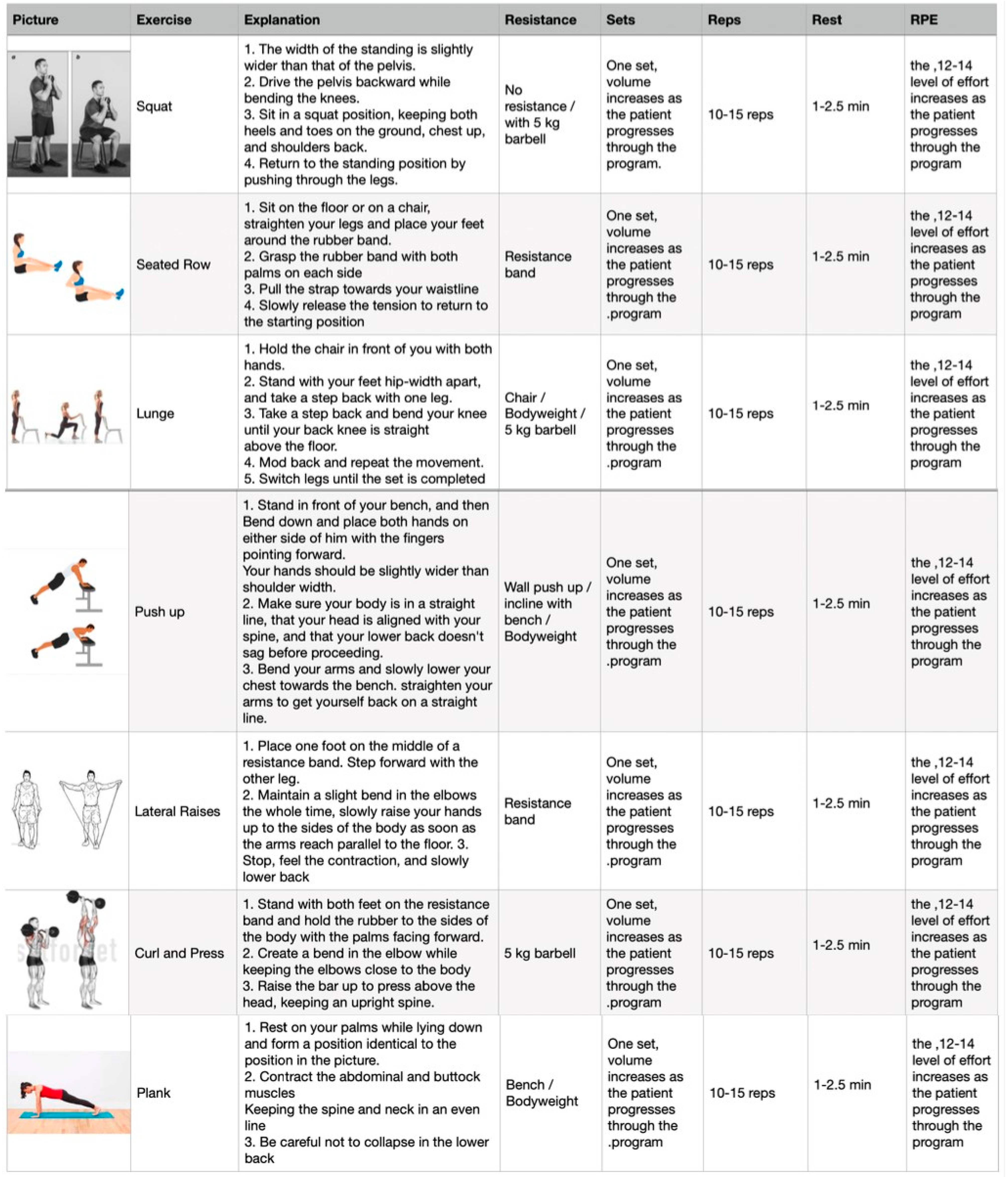
2.4. The Intervention Program
2.5. Statistical Analysis
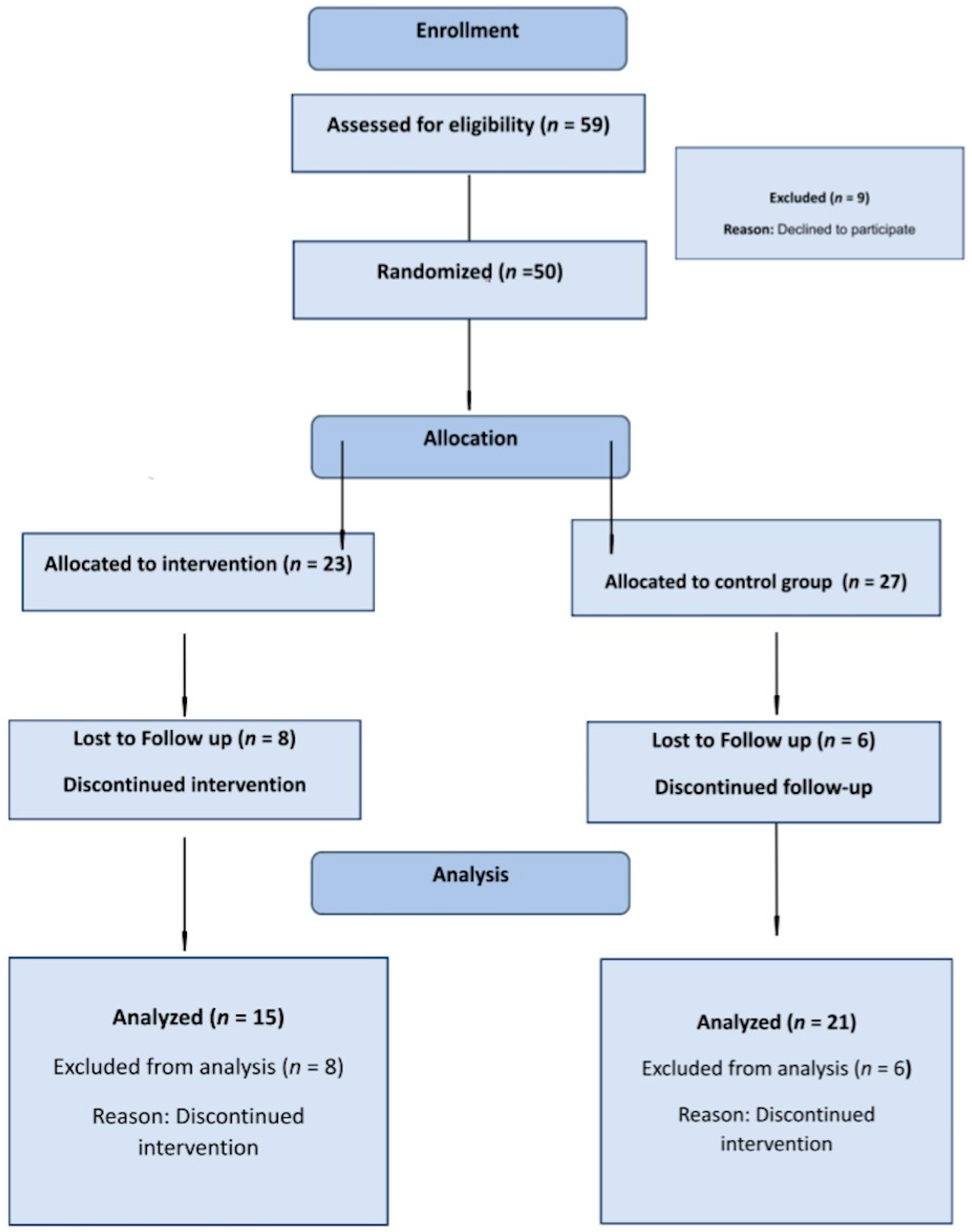
3. Results
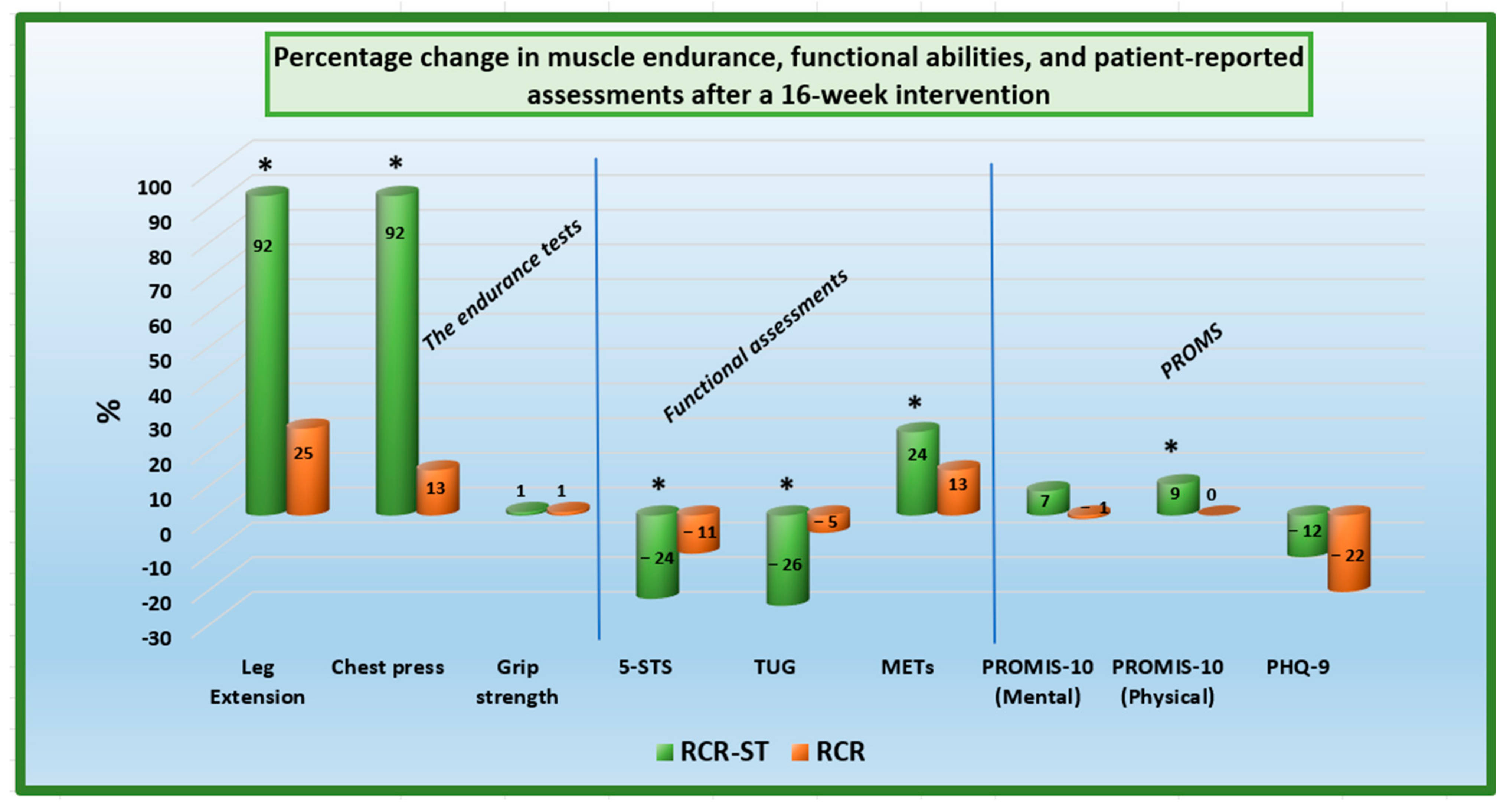
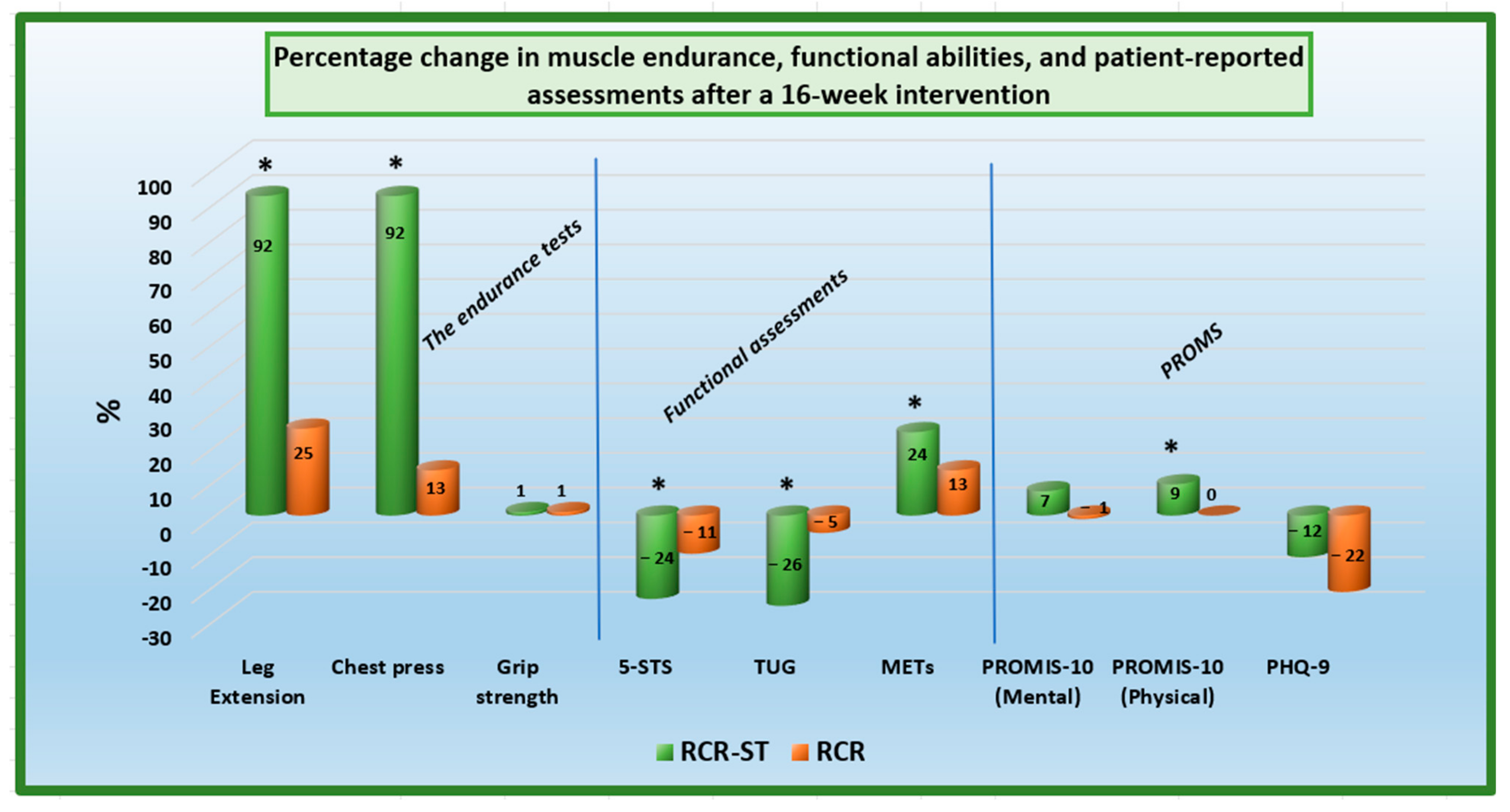
3.1. Analysis of Muscle Endurance
3.2. Analysis of the Functional Assessments
3.3. Analysis of the Secondary Outcomes
3.4. Analysis of Compliance and Adherence
4. Discussion
4.1. Effectiveness of the Enhanced Strength Training Program
4.2. Patient-Reported Outcomes
4.3. Patient Compliance and Adherence
4.4. Implications for Cardiological Rehabilitation
4.5. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention Group (n = 15) | Control Group (n = 21) | p Value |
|---|---|---|---|
| Age, years | 56.9 ± 11.7 | 62.4 ± 8.4 | 0.132 |
| Sex, male | 11 (73.3) | 20 (95.2) | 0.061 |
| Body metrics | |||
| Weight, kg | 83.2 ± 11.2 | 85.0 ± 16.1 | 0.710 |
| Height, cm | 174.8 ± 10.5 | 177.0 ± 9.0 | 0.504 |
| BMI, kg/m2 | 27.2 ± 3.0 | 27.0 ± 4.5 | 0.890 |
| Current Smoker | 3 (20.0) | 1 (4.8) | 0.151 |
| Past Smoker | 3 (20.0) | 2 (9.5) | 0.370 |
| Comorbidities | |||
| HTN | 5 (33.3) | 5 (23.8) | 0.529 |
| Dyslipidemia | 3 (20.0) | 9 (42.9) | 0.151 |
| DM | 3 (20.0) | 3 (14.3) | 0.650 |
| CVA | 1 (6.7) | 1 (4.8) | 0.806 |
| Main Indication for CR | |||
| IHD | 9 (60.0) | 17 (81.0) | 0.166 |
| MI-ACS | 8 (53.3) | 11 (52.4) | 0.955 |
| PCI | 7 (46.7) | 11 (52.4) | 0.735 |
| Valve Surgery | 4 (26.7) | 3 (14.3) | 0.355 |
| CABG | 1 (6.7) | 2 (9.5) | 0.760 |
| AFib | 0 | 2 (9.5) | 0.219 |
| Chest Pain | 4 (26.7) | 7 (33.3) | 0.669 |
| Atrial Arrhythmias | 1 (6.7) | 3 (14.3) | 0.473 |
| STEMI | 2 (13.3) | 0 | 0.085 |
| NSTEMI | 4 (26.7) | 7 (33.3) | 0.669 |

References
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2021, 19, 180–194. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8445013/ (accessed on 27 December 2023). [CrossRef]
- Halasz, G.; Piepoli, M.F. Focus on cardiovascular rehabilitation and exercise training. Eur. J. Prev. Cardiol. 2020, 27, 1683–1687. [Google Scholar] [CrossRef]
- Kirkman, D.L.; Lee, D.-C.; Carbone, S. Resistance exercise for cardiac rehabilitation. Prog. Cardiovasc. Dis. 2022, 70, 66–72. [Google Scholar] [CrossRef]
- Hilu, R.; Haskiah, F.; Khaskia, A.; Assali, A.; Baron, I.; Gabarin, M.; Chen, J.; Pereg, D. Effectiveness and Safety of Remote Cardiac Rehabilitation for Patients After Acute Coronary Syndrome. Am. J. Cardiol. 2023, 207, 54–58. Available online: https://www.sciencedirect.com/science/article/pii/S0002914923009487 (accessed on 27 December 2023). [CrossRef]
- Giggins, O.M.; Doyle, J.; Smith, S.; Vavasour, G.; Moran, O.; Gavin, S.; Sojan, N.; Boyle, G. Remotely Delivered Cardiac Rehabilitation Exercise for Coronary Heart Disease: Nonrandomized Feasibility Study. JMIR Cardio 2023, 7, e40283. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9960022/ (accessed on 27 December 2023). [CrossRef] [PubMed]
- Fukuta, Y.; Arizono, S.; Tanaka, S.; Kawaguchi, T.; Tsugita, N.; Fuseya, T.; Magata, J.; Tawara, Y.; Segawa, T. Effects of real-time remote cardiac rehabilitation on exercise capacity and quality of life: A quasi-randomised controlled trial. BMC Geriatr. 2023, 23, 388. [Google Scholar] [CrossRef] [PubMed]
- Bäck, M.; Hansen, T.B. Cardiac Rehabilitation and Exercise Training Recommendations. Available online: https://www.escardio.org/Education/ESC-Prevention-of-CVD-Programme/Rehabilitation/cardiac-rehabilitation-and-exercise-training-recommendations (accessed on 27 December 2023).
- Nabutovsky, I.; Breitner, D.; Heller, A.; Moreno, M.; Levine, Y.; Klempfner, Y.; Scheinowitz, M.; Klempfner, R. Israel’s first national remote cardiac rehabilitation program: A retrospective analysis. Digit. Health 2023, 9, 20552076231180762. [Google Scholar] [CrossRef] [PubMed]
- Sabbahi, A.; Canada, J.M.; Babu, A.S.; Severin, R.; Arena, R.; Ozemek, C. Exercise training in cardiac rehabilitation: Setting the right intensity for optimal benefit. Prog. Cardiovasc. Dis. 2022, 70, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Kamper, R.S.; Aagaard, P.; Haddock, B.; Prescott, E.; Ara, I.; Suetta, C. Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: Validation and translation to functional performance. Sci. Rep. 2020, 10, 16337. Available online: https://www.nature.com/articles/s41598-020-73395-4 (accessed on 6 September 2022). [CrossRef] [PubMed]
- Martien, S.; Delecluse, C.; Boen, F.; Seghers, J.; Pelssers, J.; Van Hoecke, A.-S.; Van Roie, E. Is knee extension strength a better predictor of functional performance than handgrip strength among older adults in three different settings? Arch. Gerontol. Geriatr. 2015, 60, 252–258. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0167494314002222 (accessed on 6 September 2022). [CrossRef]
- Jones, A.; Sealey, R.; Crowe, M.; Gordon, S. Concurrent validity and reliability of the Simple Goniometer iPhone app compared with the Universal Goniometer. Physiother. Theory Pract. 2014, 30, 512–516. Available online: http://www.tandfonline.com/doi/full/10.3109/09593985.2014.900835 (accessed on 6 September 2022). [CrossRef]
- Padulo, J.; Mignogna, P.; Mignardi, S.; Tonni, F.; D’Ottavio, S. Effect of different pushing speeds on bench press. Int. J. Sports Med. 2012, 33, 376–380. [Google Scholar] [CrossRef]
- Buitrago, S.; Wirtz, N.; Yue, Z.; Kleinöder, H.; Mester, J. Mechanical load and physiological responses of four different resistance training methods in bench press exercise. J. Strength. Cond. Res. 2013, 27, 1091–1100. [Google Scholar] [CrossRef]
- Wong, D.P.; Ngo, K.-L.; Tse, M.A.; Smith, A.W. Using Bench Press Load to Predict Upper Body Exercise Loads in Physically Active Individuals. J. Sports Sci. Med. 2013, 12, 38–43. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3761768/ (accessed on 6 September 2022).
- Gąsior, J.S.; Pawłowski, M.; Williams, C.A.; Dąbrowski, M.J.; Rameckers, E.A. Assessment of Maximal Isometric Hand Grip Strength in School-aged Children. Open Med. 2018, 13, 22–28. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5850995/ (accessed on 27 December 2023). [CrossRef]
- Will, P.M.; Walter, J.D. Exercise testing: Improving performance with a ramped Bruce protocol. Am. Heart J. 1999, 138, 1033–1037. Available online: https://www.sciencedirect.com/science/article/pii/S0002870399700670 (accessed on 13 October 2022). [CrossRef]
- Kasturi, S.; Szymonifka, J.; Burket, J.C.; Berman, J.R.; Kirou, K.A.; Levine, A.B.; Sammaritano, L.R.; Mandl, L.A. Feasibility, Validity, and Reliability of the 10-item Patient Reported Outcomes Measurement Information System Global Health Short Form in Outpatients with Systemic Lupus Erythematosus. J. Rheumatol. 2018, 45, 397–404. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5873576/ (accessed on 6 September 2022). [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1046/j.1525-1497.2001.016009606.x (accessed on 13 October 2022). [CrossRef] [PubMed]
- Baltasar-Fernandez, I.; Alcazar, J.; Rodriguez-Lopez, C.; Losa-Reyna, J.; Alonso-Seco, M.; Ara, I.; Alegre, L.M. Sit-to-stand muscle power test: Comparison between estimated and force plate-derived mechanical power and their association with physical function in older adults. Exp. Gerontol. 2021, 145, 111213. [Google Scholar] [CrossRef] [PubMed]
- Kharabsheh, S.M.; Al-Sugair, A.; Al-Buraiki, J.; Farhan, J. Overview of Exercise Stress Testing. Ann. Saudi Med. 2006, 26, 1–6. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6078558/ (accessed on 13 October 2022). [CrossRef]
- Nabutovsky, I.; Ashr, S.; Nachshon, A.; Tesler, R.; Shapiro, Y.; Wright, E.; Vadasz, B.; Offer, A.; Grosman-Rimon, L.; Klempfner, R. Feasibility, Safety, and Effectiveness of a Mobile Application in Cardiac Rehabilitation. Isr. Med. Assoc. J. IMAJ 2020, 22, 357–363. [Google Scholar]
- Ben-Tzur, D.; Sabovich, S.; Hutzler, Y.; Rimon, J.B.; Zach, S.; Epstein, M.; Vadasz, B.; Diniz, C.V.B.; Nabutovsky, I.; Klempfner, R.; et al. Advances in Technology Promote Patient-Centered Care in Cardiac Rehabilitation. Cardiol. Rev. 2023. [Google Scholar] [CrossRef]
- Maestroni, L.; Read, P.; Bishop, C.; Papadopoulos, K.; Suchomel, T.J.; Comfort, P.; Turner, A. The Benefits of Strength Training on Musculoskeletal System Health: Practical Applications for Interdisciplinary Care. Sports Med. 2020, 50, 1431–1450. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Bellon, C.R.; Stone, M.H. The Importance of Muscular Strength: Training Considerations. Sports Med. 2018, 48, 765–785. [Google Scholar] [CrossRef]
- Taylor, J.L.; Bonikowske, A.R.; Olson, T.P. Optimizing Outcomes in Cardiac Rehabilitation: The Importance of Exercise Intensity. Front. Cardiovasc. Med. 2021, 8, 734278. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8446279/ (accessed on 27 December 2023). [CrossRef]
- Kumar, K.R.; Pina, I.L. Cardiac rehabilitation in older adults: New options. Clin. Cardiol. 2019, 43, 163–170. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7021654/ (accessed on 27 December 2023). [CrossRef]
- Seguin, R.; Nelson, M.E. The benefits of strength training for older adults. Am. J. Prev. Med. 2003, 25, 141–149. [Google Scholar] [CrossRef]
- Khadanga, S.; Savage, P.D.; Ades, P.A. Resistance Training for Older Adults in Cardiac Rehabilitation. Clin. Geriatr. Med. 2019, 35, 459–468. [Google Scholar] [CrossRef]
- Liu, C.; Shiroy, D.M.; Jones, L.Y.; Clark, D.O. Systematic review of functional training on muscle strength, physical functioning, and activities of daily living in older adults. Eur. Rev. Aging Phys. Act. 2014, 11, 95–106. Available online: https://eurapa.biomedcentral.com/articles/10.1007/s11556-014-0144-1 (accessed on 27 December 2023). [CrossRef]
- Xiao, W.; Soh, K.G.; Wazir, M.R.W.N.; Talib, O.; Bai, X.; Bu, T.; Sun, H.; Popovic, S.; Masanovic, B.; Gardasevic, J. Effect of Functional Training on Physical Fitness Among Athletes: A Systematic Review. Front. Physiol. 2021, 12, 738878. Available online: https://www.frontiersin.org/articles/10.3389/fphys.2021.738878 (accessed on 27 December 2023). [CrossRef]
- De Santana, D.A.; Castro, A.; Cavaglieri, C.R. Strength Training Volume to Increase Muscle Mass Responsiveness in Older Individuals: Weekly Sets Based Approach. Front. Physiol. 2021, 12, 759677. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8514686/ (accessed on 27 December 2023). [CrossRef]
- Chen, Y.-W.; Wang, C.-Y.; Lai, Y.-H.; Liao, Y.-C.; Wen, Y.-K.; Chang, S.-T.; Huang, J.-L.; Wu, T.-J. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine 2018, 97, e9629. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5794362/ (accessed on 27 December 2023). [CrossRef]
- Horton, E.J.; Ruksenaite, J.; Mitchell, K.; Sewell, L.; Newby, C.; Singh, S.J. A Comparison of Physical Activity Between Home-Based and Centre-Based Pulmonary Rehabilitation: A Randomised Controlled Secondary Analysis. Front. Rehabil. Sci. 2021, 2, 743441. Available online: https://www.frontiersin.org/articles/10.3389/fresc.2021.743441 (accessed on 27 December 2023). [CrossRef]
- Regensteiner, J.G.; Meyer, T.J.; Krupski, W.C.; Cranford, L.S.; Hiatt, W.R. Hospital vs home-based exercise rehabilitation for patients with peripheral arterial occlusive disease. Angiology 1997, 48, 291–300. [Google Scholar] [CrossRef]
- Lundberg, T.R.; Feuerbacher, J.F.; Sünkeler, M.; Schumann, M. The Effects of Concurrent Aerobic and Strength Training on Muscle Fiber Hypertrophy: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 2391–2403. [Google Scholar] [CrossRef]
- Bai, X.; Soh, K.G.; Omar Dev, R.D.; Talib, O.; Xiao, W.; Soh, K.L.; Zhao, C.; Galeru, O.; Casaru, C. Aerobic Exercise Combination Intervention to Improve Physical Performance Among the Elderly: A Systematic Review. Front. Physiol. 2022, 12, 798068. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8764279/ (accessed on 27 December 2023). [CrossRef]
- Novaković, M.; Novak, T.; Vižintin Cuderman, T.; Krevel, B.; Tasič, J.; Rajkovič, U.; Fras, Z.; Jug, B. Exercise capacity improvement after cardiac rehabilitation following myocardial infarction and its association with long-term cardiovascular events. Eur. J. Cardiovasc. Nurs. 2022, 21, 76–84. [Google Scholar] [CrossRef]
- Hollings, M.; Mavros, Y.; Freeston, J.; Fiatarone Singh, M. The effect of progressive resistance training on aerobic fitness and strength in adults with coronary heart disease: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2017, 24, 1242–1259. [Google Scholar] [CrossRef]
- Allado, E.; Poussel, M.; Albuisson, E.; Paysant, J.; Temperelli, M.; Hily, O.; Moussu, A.; Benhajji, N.; Gauchard, G.; Chenuel, B. Physical Activity Capacity Assessment of Patients with Chronic Disease and the 1-Minute Sit to Stand Test: Is There an Interest? Front. Sports Act. Living 2022, 4, 839509. Available online: https://www.frontiersin.org/articles/10.3389/fspor.2022.839509 (accessed on 27 December 2023). [CrossRef]
- Sbardelotto, M.L.; Costa, R.R.; Malysz, K.A.; Pedroso, G.S.; Pereira, B.C.; Sorato, H.R.; Silveira, P.C.L.; Nesi, R.T.; Grande, A.J.; A Pinho, R. Improvement in muscular strength and aerobic capacities in elderly people occurs independently of physical training type or exercise model. Clinics 2019, 74, e833. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6585866/ (accessed on 27 December 2023). [CrossRef]
- Giuliano, C.; Karahalios, A.; Neil, C.; Allen, J.; Levinger, I. The effects of resistance training on muscle strength, quality of life and aerobic capacity in patients with chronic heart failure—A meta-analysis. Int. J. Cardiol. 2017, 227, 413–423. [Google Scholar] [CrossRef]
- Mahindru, A.; Patil, P.; Agrawal, V. Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus 2023, 15, e33475. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9902068/ (accessed on 27 December 2023). [CrossRef]
- Schuch, F.B.; Vancampfort, D. Physical activity, exercise, and mental disorders: It is time to move on. Trends Psychiatry Psychother. 2021, 43, 177–184. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8638711/ (accessed on 27 December 2023). [CrossRef]
- Stubbs, B.; Vancampfort, D.; Smith, L.; Rosenbaum, S.; Schuch, F.; Firth, J. Physical activity and mental health. Lancet Psychiatry 2018, 5, 873. Available online: https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(18)30343-2/fulltext (accessed on 27 December 2023). [CrossRef]
- Singh, B.; Olds, T.; Curtis, R.; Dumuid, D.; Virgara, R.; Watson, A.; Szeto, K.; O’Connor, E.; Ferguson, T.; Eglitis, E.; et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. Br. J. Sports Med. 2023, 57, 1203–1209. [Google Scholar] [CrossRef]
- Wanjau, M.N.; Möller, H.; Haigh, F.; Milat, A.; Hayek, R.; Lucas, P.; Veerman, J.L. Physical Activity and Depression and Anxiety Disorders: A Systematic Review of Reviews and Assessment of Causality. AJPM Focus 2023, 2, 100074. Available online: https://www.sciencedirect.com/science/article/pii/S2773065423000111 (accessed on 27 December 2023). [CrossRef]
- Hu, M.X.; Turner, D.; Generaal, E.; Bos, D.; Ikram, M.K.; Ikram, M.A.; Cuijpers, P.; Penninx, B.W.J.H. Exercise interventions for the prevention of depression: A systematic review of meta-analyses. BMC Public Health 2020, 20, 1255. [Google Scholar] [CrossRef]
- Murray, R.M.; Sabiston, C.M.; Coffee, P.; Kowalski, K.C. Strengthening the relationship between physical activity and physical self-concept: The moderating effect of controllable attributions. Psychol. Sport. Exerc. 2021, 52, 101828. Available online: https://www.sciencedirect.com/science/article/pii/S146902922030813X (accessed on 27 December 2023). [CrossRef]
- Iwon, K.; Skibinska, J.; Jasielska, D.; Kalwarczyk, S. Elevating Subjective Well-Being Through Physical Exercises: An Intervention Study. Front. Psychol. 2021, 12, 702678. Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.702678 (accessed on 27 December 2023). [CrossRef]
- Nabutovsky, I.; Breitner, D.; Heller, A.; Scheinowitz, M.; Klempfner, Y.; Klempfner, R. The First National Program of Remote Cardiac Rehabilitation in Israel-Goal Achievements, Adherence, and Responsiveness in Older Adult Patients: Retrospective Analysis. JMIR Cardio 2022, 6, e36947. [Google Scholar] [CrossRef]
- Nabutovsky, I.; Breitner, D.; Heller, A.; Levine, Y.; Moreno, M.; Scheinowitz, M.; Levin, C.; Klempfner, R. Home-Based Cardiac Rehabilitation Among Patients Unwilling to Participate in Hospital-Based Programs. J. Cardiopulm. Rehabil. Prev. 2024, 44, 33–39. [Google Scholar] [CrossRef]
- Marzolini, S.; Brooks, D.; Oh, P.; Jagroop, D.; MacIntosh, B.J.; Anderson, N.D.; Alter, D.; Corbett, D. Aerobic with Resistance Training or Aerobic Training Alone Poststroke: A Secondary Analysis from a Randomized Clinical Trial. Neurorehabil Neural Repair. 2018, 32, 209–222. Available online: http://journals.sagepub.com/doi/10.1177/1545968318765692 (accessed on 5 September 2022). [CrossRef]
- Krzysztofik, M.; Wilk, M.; Wojdała, G.; Gołaś, A. Maximizing Muscle Hypertrophy: A Systematic Review of Advanced Resistance Training Techniques and Methods. Int. J. Environ. Res. Public Health 2019, 16, 4897. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6950543/ (accessed on 27 December 2023). [CrossRef]
- Marzuca-Nassr, G.N.; Alegría-Molina, A.; SanMartín-Calísto, Y.; Artigas-Arias, M.; Huard, N.; Sapunar, J.; Salazar, L.A.; Verdijk, L.B.; van Loon, L.J.C. Muscle Mass and Strength Gains Following Resistance Exercise Training in Older Adults 65–75 Years and Older Adults Above 85 Years. Int. J. Sport. Nutr. Exerc. Metab. 2023, 34, 11–19. [Google Scholar] [CrossRef]
- Caparrós-Manosalva, C.; Garrido-Muñoz, N.; Alvear-Constanzo, B.; Sanzana-Laurié, S.; Artigas-Arias, M.; Alegría-Molina, A.; Vidal-Seguel, N.; Espinoza-Araneda, J.; Huard, N.; Pagnussat, A.S.; et al. Effects of high-intensity interval training on lean mass, strength, and power of the lower limbs in healthy old and young people. Front. Physiol. 2023, 14, 1223069. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10565117/ (accessed on 27 December 2023). [CrossRef]
- Rao, A.; Zecchin, R.; Byth, K.; Denniss, A.R.; Hickman, L.D.; DiGiacomo, M.; Phillips, J.L.; Newton, P.J. The Role of Lifestyle and Cardiovascular Risk Factors in Dropout from an Australian Cardiac Rehabilitation Program. A Longitudinal Cohort Study. Heart Lung Circ. 2021, 30, 1891–1900. [Google Scholar] [CrossRef]
- Sommer, C.G.; Jørgensen, L.B.; Blume, B.; Møller, T.; Skou, S.T.; Harrison, A.; Tang, L.H. Dropout during a 12-week transitional exercise-based cardiac rehabilitation programme: A mixed-methods prospective cohort study. Eur. J. Cardiovasc. Nurs. 2022, 21, 578–586. [Google Scholar] [CrossRef]
- Resurrección, D.M.; Moreno-Peral, P.; Gómez-Herranz, M.; Rubio-Valera, M.; Pastor, L.; Caldas de Almeida, J.M.; Motrico, E. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: A systematic review of prospective cohort studies. Eur. J. Cardiovasc. Nurs. 2019, 18, 38–47. [Google Scholar] [CrossRef]
- Resurrección, D.M.; Motrico, E.; Rubio-Valera, M.; Mora-Pardo, J.A.; Moreno-Peral, P. Reasons for dropout from cardiac rehabilitation programs in women: A qualitative study. PLoS ONE 2018, 13, e0200636. [Google Scholar] [CrossRef]
| Variables | Intervention Group (n = 23) | Control Group (n = 27) | p Value |
|---|---|---|---|
| Age, years | 57.7 ± 10.3 | 61.6 ± 10.3 | 0.189 |
| Sex, male | 18 (78.3) | 26 (96.3) | 0.050 |
| Body metrics | |||
| Weight, kg | 83.2 ± 10.0 | 85.5 ± 17.8 | 0.577 |
| Height, cm | 174.2 ± 8.7 | 176.0 ± 9.6 | 0.479 |
| BMI, kg/m2 | 27.4 ± 2.9 | 27.4 ± 4.5 | 0.980 |
| Current Smoker | 4 (17.4) | 1 (3.7) | 0.108 |
| Past Smoker | 6 (26.1) | 3 (11.1) | 0.170 |
| Comorbidities | |||
| HTN | 8 (34.8) | 7 (25.9) | 0.496 |
| Dyslipidemia | 6 (26.1) | 10 (37.0) | 0.408 |
| DM | 3 (13.0) | 4 (14.8) | 0.857 |
| CVA | 1 (4.3) | 1 (3.7) | 0.908 |
| Main Indication for CR | |||
| IHD | 17 (73.9) | 23 (85.2) | 0.321 |
| MI-ACS | 14 (60.9) | 15 (55.6) | 0.704 |
| PCI | 14 (60.9) | 15 (55.6) | 0.704 |
| Valve Surgery | 4 (17.4) | 3 (11.1) | 0.524 |
| CABG | 1 (4.3) | 3 (11.1) | 0.380 |
| AFib | 0 | 3 (11.1) | 0.099 |
| Chest Pain | 6 (26.1) | 7 (25.9) | 0.990 |
| Atrial Arrhythmias | 1 (4.3) | 4 (14.8) | 0.219 |
| STEMI | 3 (13.0) | 1 (3.7) | 0.225 |
| NSTEMI | 5 (21.7) | 7 (25.9) | 0.730 |
| Intervention (n = 15) | Control (n = 21) | Time Effect | Group Effect | Time × Group Effect | |||
|---|---|---|---|---|---|---|---|
| Baseline | 16 Weeks | Baseline | 16 Weeks | P (η2) | P (η2) | P (η2) | |
| Muscle Endurance | |||||||
| Leg Extension | 15.4 ± 8.0 | 29.7 ± 14.3 | 18.6 ± 7.3 | 23.4 ± 13.0 | <0.001 (0.515) | ns | 0.005 (0.210) |
| Chest press | 10.5 ± 7.1 | 20.2 ± 10.9 | 12.4 ± 9.6 | 14.1 ± 9.8 | <0.001 (0.626) | ns | <0.001 (0.456) |
| Grip strength | 36.8 ± 10.0 | 37.3 ± 10.5 | 42.8 ± 11.6 | 43.3 ± 12.0 | ns | ns | ns |
| Functional Assessments | |||||||
| 5-STS (s) | 10.7 ± 2.9 | 8.1 ± 2.1 | 10.7 ± 2.7 | 9.5 ± 3.0 | <0.001 (0.513) | ns | 0.021 (0.148) |
| TUG (s) | 10.1 ± 2.5 | 7.4 ± 1.7 | 9.2 ± 1.6 | 8.7 ± 1.6 | <0.001 (0.267) | ns | 0.019 (0.152) |
| Cardiorespiratory fitness | |||||||
| METs | 8.5 ± 3.0 | 10.6 ± 3.4 | 9.7 ± 2.8 | 11.0 ± 2.6 | <0.001 (0.591) | ns | ns |
| Intervention (n = 15) | Control Group (n = 27) | p Value | |
|---|---|---|---|
| Total minutes of weekly aerobic exercise | 184.6 ± 113.3 | 229.1 ± 126.01 | 0.284 |
| Minutes in the target heart rate per week | 118.1 ± 100.5 | 95.9 ± 54.4 | 0.398 |
| Minutes below the target heart rate per week | 66.5 ± 39.0 | 133.2 ± 123.0 | 0.051 |
| Borg scale per week | 11.3 ± 1.8 | 10.6 ± 2.0 | 0.346 |
| Number of weekly aerobic training sessions | 5.8 ± 3.7 | 5.3 ± 2.1 | 0.614 |
| Number of weekly resistance training sessions | 2.0 ± 2.2 | 0.6 ± 0.7 | 0.009 |
| Number of daily steps | 7513.2 ± 1886.4 | 8298.6 ± 3194.0 | 0.362 |
| Number of weekly entries in the mobile app | 5.0 ± 1.1 | 3.7 ± 2.0 | 0.012 |
| Duration (weeks) of participation in the CR program | 15.1 ± 1.2 | 13.2 ± 3.9 | 0.046 |
| Scores are means between 16 weekly measures |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Leg Extension | |||||||||
| 2 | Chest press | 0.59 *** | ||||||||
| 3 | Grip strength | 0.25 | 0.32 | |||||||
| 4 | 5-STS (s) | −0.45 ** | −0.56 *** | −0.12 | ||||||
| 5 | TUG (s) | −0.39 * | −0.23 | −0.25 | 0.44 ** | |||||
| 6 | METs | 0.56 ** | 0.70 *** | 0.31 | −0.60 *** | −0.38 * | ||||
| 7 | PROMIS-10 (Mental) | 0.05 | 0.12 | 0.26 | 0.10 | −0.36 | 0.13 | |||
| 8 | PROMIS-10 (Physical) | 0.40 * | 0.60 *** | 0.21 | −0.35 | −0.39 * | 0.53 ** | 0.54 ** | ||
| 9 | PHQ9 | −0.47 * | −0.29 | 0.04 | 0.38 | 0.35 | −0.35 | −0.31 | −0.62 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nabutovsky, I.; Sabah, R.; Moreno, M.; Epstein, Y.; Klempfner, R.; Scheinowitz, M. Evaluating the Effects of an Enhanced Strength Training Program in Remote Cardiological Rehabilitation: A Shift from Aerobic Dominance—A Pilot Randomized Controlled Trial. J. Clin. Med. 2024, 13, 1445. https://doi.org/10.3390/jcm13051445
Nabutovsky I, Sabah R, Moreno M, Epstein Y, Klempfner R, Scheinowitz M. Evaluating the Effects of an Enhanced Strength Training Program in Remote Cardiological Rehabilitation: A Shift from Aerobic Dominance—A Pilot Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(5):1445. https://doi.org/10.3390/jcm13051445
Chicago/Turabian StyleNabutovsky, Irene, Roy Sabah, Merav Moreno, Yoram Epstein, Robert Klempfner, and Mickey Scheinowitz. 2024. "Evaluating the Effects of an Enhanced Strength Training Program in Remote Cardiological Rehabilitation: A Shift from Aerobic Dominance—A Pilot Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 5: 1445. https://doi.org/10.3390/jcm13051445
APA StyleNabutovsky, I., Sabah, R., Moreno, M., Epstein, Y., Klempfner, R., & Scheinowitz, M. (2024). Evaluating the Effects of an Enhanced Strength Training Program in Remote Cardiological Rehabilitation: A Shift from Aerobic Dominance—A Pilot Randomized Controlled Trial. Journal of Clinical Medicine, 13(5), 1445. https://doi.org/10.3390/jcm13051445