
An Observational Study in the Real Clinical Practice of the Treatment of Noninfectious Uveitis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of Patients with Noninfectious Uveitis (NIU)
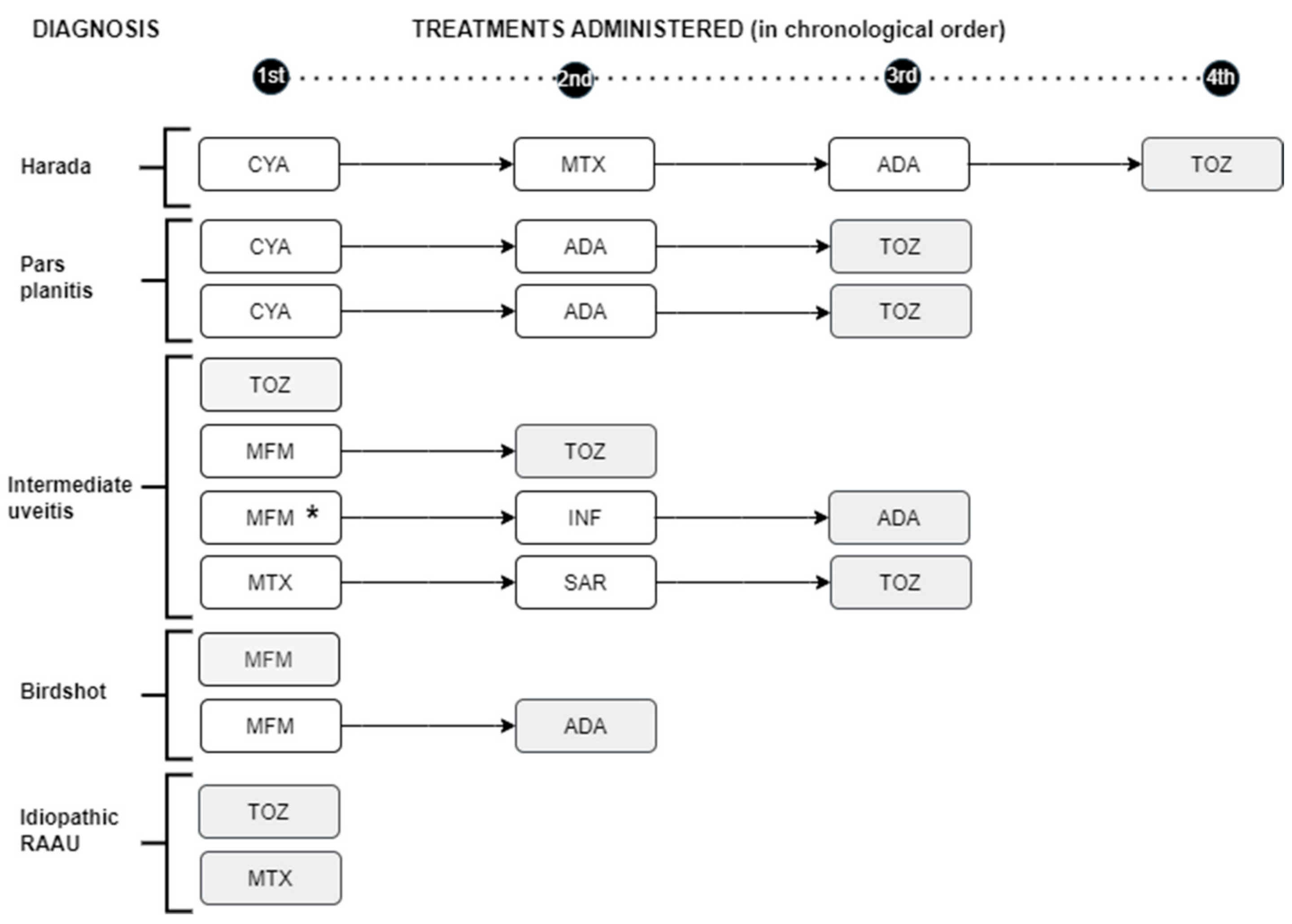
3.2. Need for IS Treatment and/or BT
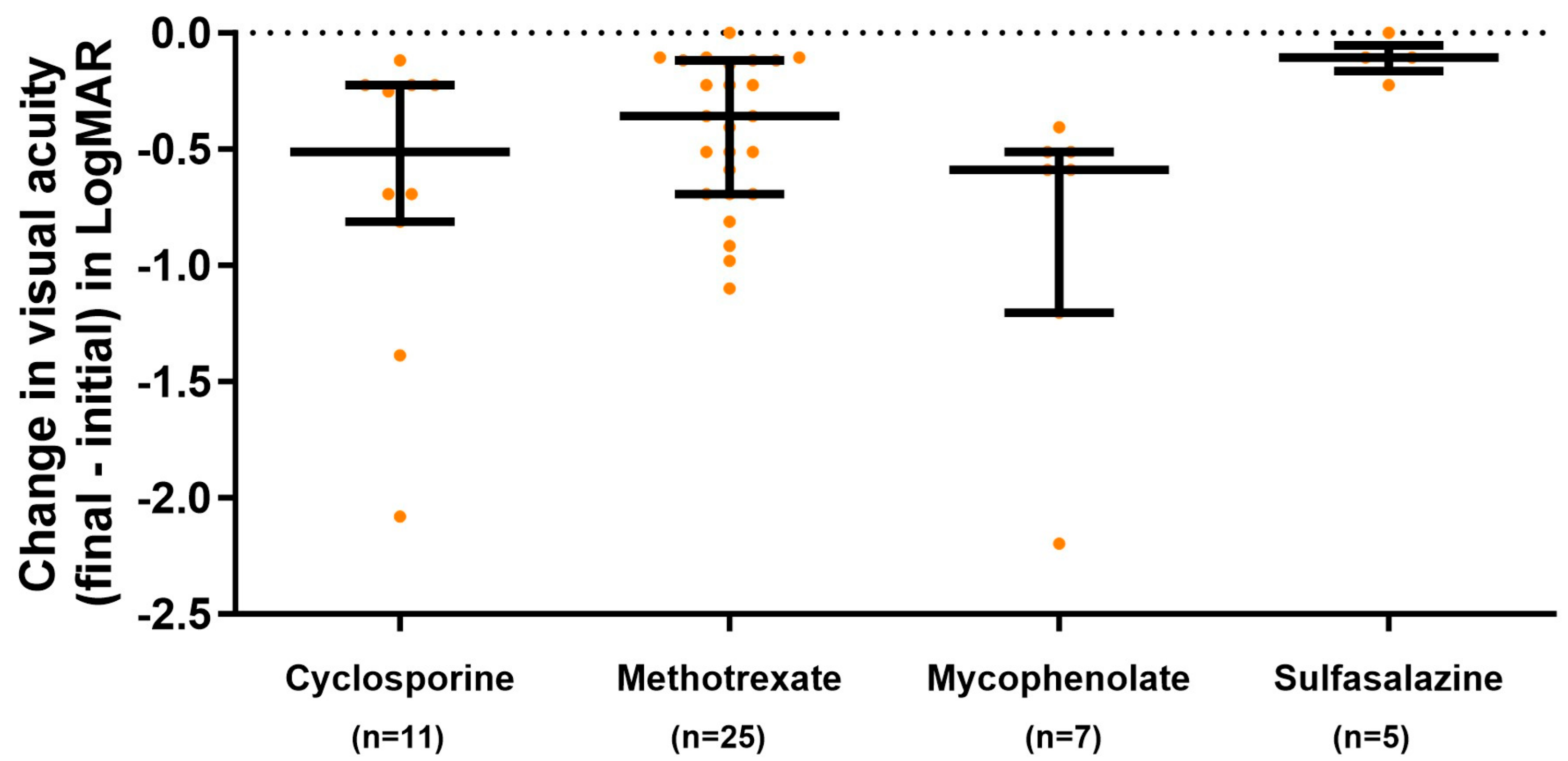
3.3. Response to Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunningham, E.T.E.; Zierhut, M. Vision Loss in Uveitis. Ocul. Immunol. Inflamm. 2021, 29, 1037–1039. [Google Scholar] [CrossRef]
- Tomkins-Netzer, O.; Talat, L.; Bar, A.; Lula, A.; Taylor, S.R.J.; Joshi, L.; Lightman, S. Long-term clinical outcome and causes of vision loss in patients with uveitis. Ophthalmology 2014, 121, 2387–2392. [Google Scholar] [CrossRef]
- Rosenbaum, J.T.; Bodaghi, B.; Couto, C.; Zierhut, M.; Acharya, N.; Pavesio, C.; Tay-Kearney, M.-L.; Neri, P.; Douglas, K.; Pathai, S.; et al. New observations and emerging ideas in diagnosis and management of non-infectious uveitis: A review. Semin. Arthritis Rheum. 2019, 49, 438–445. [Google Scholar] [CrossRef] [PubMed]
- de Smet, M.D.; Taylor, S.R.J.; Bodaghi, B.; Miserocchi, E.; Murray, P.I.; Pleyer, U.; Zierhut, M.; Barisani-Asenbauer, T.; LeHoang, P.; Lightman, S. Understanding uveitis: The impact of research on visual outcomes. Prog. Retin. Eye Res. 2011, 30, 452–470. [Google Scholar] [CrossRef]
- van Laar, J.A.M.; Rothova, A.; Missotten, T.; Kuijpers, R.W.A.M.; van Hagen, P.M.; van Velthoven, M.E.J. Diagnosis and treatment of uveitis; not restricted to the ophthalmologist. J. Clin. Transl. Res. 2015, 1, 94–99. [Google Scholar]
- Lowder, C.; Belfort, R.; Lightman, S.; Foster, C.S.; Robinson, M.R.; Schiffman, R.M.; Li, X.-Y.; Cui, H.; Whitcup, S.M. Ozurdex HURON Study Group Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch. Ophthalmol. 2011, 129, 545–553. [Google Scholar] [CrossRef]
- Callanan, D.G.; Jaffe, G.J.; Martin, D.F.; Pearson, P.A.; Comstock, T.L. Treatment of posterior uveitis with a fluocinolone acetonide implant: Three-year clinical trial results. Arch. Ophthalmol. 2008, 126, 1191–1201. [Google Scholar] [CrossRef] [PubMed]
- Jabs, D.A.; Rosenbaum, J.T.; Foster, C.S.; Holland, G.N.; Jaffe, G.J.; Louie, J.S.; Nussenblatt, R.B.; Stiehm, E.R.; Tessler, H.; Van Gelder, R.N.; et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: Recommendations of an expert panel. Am. J. Ophthalmol. 2000, 130, 492–513. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Hatef, E.; Kayen, B.; Macahilig, C.P.; Ibrahim, M.; Wang, J.; Shaikh, O.; Bodaghi, B. A cross-sectional study of the current treatment patterns in noninfectious uveitis among specialists in the United States. Ophthalmology 2011, 118, 184–190. [Google Scholar] [CrossRef]
- Dick, A.D.; Rosenbaum, J.T.; Al-Dhibi, H.A.; Belfort, R.; Brézin, A.P.; Chee, S.P.; Davis, J.L.; Ramanan, A.V.; Sonoda, K.-H.; Carreño, E.; et al. Guidance on Noncorticosteroid Systemic Immunomodulatory Therapy in Noninfectious Uveitis: Fundamentals Of Care for UveitiS (FOCUS) Initiative. Ophthalmology 2018, 125, 757–773. [Google Scholar] [CrossRef]
- Suhler, E.B.; Adán, A.; Brézin, A.P.; Fortin, E.; Goto, H.; Jaffe, G.J.; Kaburaki, T.; Kramer, M.; Lim, L.L.; Muccioli, C.; et al. Safety and Efficacy of Adalimumab in Patients with Noninfectious Uveitis in an Ongoing Open-Label Study: VISUAL III. Ophthalmology 2018, 125, 1075–1087. [Google Scholar] [CrossRef]
- Jaffe, G.J.; Dick, A.D.; Brézin, A.P.; Nguyen, Q.D.; Thorne, J.E.; Kestelyn, P.; Barisani-Asenbauer, T.; Franco, P.; Heiligenhaus, A.; Scales, D.; et al. Adalimumab in Patients with Active Noninfectious Uveitis. N. Engl. J. Med. 2016, 375, 932–943. [Google Scholar] [CrossRef]
- Takeuchi, M.; Kezuka, T.; Sugita, S.; Keino, H.; Namba, K.; Kaburaki, T.; Maruyama, K.; Nakai, K.; Hijioka, K.; Shibuya, E.; et al. Evaluation of the long-term efficacy and safety of infliximab treatment for uveitis in Behçet’s disease: A multicenter study. Ophthalmology 2014, 121, 1877–1884. [Google Scholar] [CrossRef] [PubMed]
- Levy-Clarke, G.; Jabs, D.A.; Read, R.W.; Rosenbaum, J.T.; Vitale, A.; Van Gelder, R.N. Expert panel recommendations for the use of anti-tumor necrosis factor biologic agents in patients with ocular inflammatory disorders. Ophthalmology 2014, 121, 785–796.e3. [Google Scholar] [CrossRef]
- Sepah, Y.J.; Sadiq, M.A.; Chu, D.S.; Dacey, M.; Gallemore, R.; Dayani, P.; Hanout, M.; Hassan, M.; Afridi, R.; Agarwal, A.; et al. Primary (Month-6) Outcomes of the STOP-Uveitis Study: Evaluating the Safety, Tolerability, and Efficacy of Tocilizumab in Patients With Noninfectious Uveitis. Am. J. Ophthalmol. 2017, 183, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, M.; Andrillon, A.; Maalouf, G.; Sève, P.; Bielefeld, P.; Gueudry, J.; Sené, T.; Moulinet, T.; Rouvière, B.; Sène, D.; et al. Anti-Tumor Necrosis Factor α versus Tocilizumab in the Treatment of Refractory Uveitic Macular Edema: A Multicenter Study from the French Uveitis Network. Ophthalmology 2022, 129, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Deschenes, J.; Murray, P.I.; Rao, N.A.; Nussenblatt, R.B. International Uveitis Study Group International Uveitis Study Group (IUSG): Clinical classification of uveitis. Ocul. Immunol. Inflamm. 2008, 16, 1–2. [Google Scholar] [CrossRef]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T. Standardization of Uveitis Nomenclature (SUN) Working Group Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef]
- Pistilli, M.; Joffe, M.M.; Gangaputra, S.S.; Pujari, S.S.; Jabs, D.A.; Levy-Clarke, G.A.; Nussenblatt, R.B.; Rosenbaum, J.T.; Sen, H.N.; Suhler, E.B.; et al. Visual Acuity Outcome over Time in Non-Infectious Uveitis. Ocul. Immunol. Inflamm. 2021, 29, 1064–1071. [Google Scholar] [CrossRef]
- Hunter, R.S.; Skondra, D.; Papaliodis, G.; Sobrin, L. Role of OCT in the diagnosis and management of macular edema from uveitis. Semin. Ophthalmol. 2012, 27, 236–241. [Google Scholar] [CrossRef]
- Espinosa, G.; Muñoz-Fernández, S.; García Ruiz de Morales, J.M.; Herreras, J.M.; Cordero-Coma, M. Treatment recommendations for non-infectious anterior uveitis. Med. Clin. 2017, 149, 552.e1–552.e12. [Google Scholar] [CrossRef]
- Espinosa, G.; Herreras, J.M.; Muñoz-Fernández, S.; García Ruiz de Morales, J.M.; Cordero-Coma, M. Recommendations statement on the immunosuppressive treatment of non-infectious, non-neoplastic, non-anterior uveitis. Med. Clín. Engl. 2020, 155, 220.e1–220.e12. [Google Scholar] [CrossRef]
- Gómez-Gómez, A.; Loza, E.; Rosario, M.P.; Espinosa, G.; de Morales, J.M.G.R.; Herreras, J.M.; Muñoz-Fernández, S.; Cordero-Coma, M. Efficacy and safety of immunomodulatory drugs in patients with anterior uveitis: A systematic literature review. Medicine 2017, 96, e8045. [Google Scholar] [CrossRef]
- Gómez-Gómez, A.; Loza, E.; Rosario, M.P.; Espinosa, G.; de Morales, J.M.G.R.; Herrera, J.M.; Muñoz-Fernández, S.; Rodríguez-Rodríguez, L.; Cordero-Coma, M. Spanish Society of Ocular Inflammation (SEIOC) Efficacy and safety of immunomodulatory drugs in patients with non-infectious intermediate and posterior uveitis, panuveitis and macular edema: A systematic literature review. Semin. Arthritis Rheum. 2020, 50, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- García-Aparicio, A.; Alonso Martín, L.; López Lancho, R.; Quirós Zamorano, R.; Del Olmo Perez, L.; Sánchez Fernández, S.; Otón, T.; Jiménez Escribano, R.; González Del Valle, F.; Muñoz-Fernández, S. Epidemiology of Uveitis in a Spanish Region: Prevalence and Etiology. Ophthalmic Epidemiol. 2021, 28, 227–236. [Google Scholar] [CrossRef]
- Millán-Longo, C.; Peiteado, D.; Schlincker, A.; Hidalgo, V.; Pieren, A.; Balsa, A.; de Miguel, E. Use of Immunomodulatory Drugs at a Uveitis Clinic. Reumatol. Clin. 2019, 15, 271–276. [Google Scholar] [CrossRef]
- Chang, J.H.-M.; Wakefield, D. Uveitis: A global perspective. Ocul. Immunol. Inflamm. 2002, 10, 263–279. [Google Scholar] [CrossRef]
- Wang, L.; Guo, Z.; Zheng, Y.; Li, Q.; Yuan, X.; Hua, X. Analysis of the clinical diagnosis and treatment of uveitis. Ann. Palliat. Med. 2021, 10, 12782–12788. [Google Scholar] [CrossRef]
- Muñoz-Fernández, S.; García-Aparicio, A.M.; Hidalgo, M.V.; Platero, M.; Schlincker, A.; Bascones, M.L.; Pombo, M.; Morente, P.; Sanpedro, J.; Martín-Mola, E. Methotrexate: An option for preventing the recurrence of acute anterior uveitis. Eye Lond. Engl. 2009, 23, 1130–1133. [Google Scholar] [CrossRef]
- Bajwa, A.; Osmanzada, D.; Osmanzada, S.; Khan, I.; Patrie, J.; Xin, W.; Reddy, A.K. Epidemiology of uveitis in the mid-Atlantic United States. Clin. Ophthalmol. 2015, 9, 889–901. [Google Scholar] [CrossRef]
- Foster, C.S.; Kothari, S.; Anesi, S.D.; Vitale, A.T.; Chu, D.; Metzinger, J.L.; Cerón, O. The Ocular Immunology and Uveitis Foundation preferred practice patterns of uveitis management. Surv. Ophthalmol. 2016, 61, 1–17. [Google Scholar] [CrossRef]
- Guillot, X.; Prati, C.; Sondag, M.; Wendling, D. Etanercept for treating axial spondyloarthritis. Expert Opin. Biol. Ther. 2017, 17, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, N.-S. Etanercept therapy-associated acute uveitis: A case report and literature review. Clin. Exp. Rheumatol. 2009, 27, 838–839. [Google Scholar]
- Benitez-Del-Castillo, J.M.; Garcia-Sanchez, J.; Iradier, T.; Bañares, A. Sulfasalazine in the prevention of anterior uveitis associated with ankylosing spondylitis. Eye Lond. Engl. 2000, 14 Pt 3A, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Shen, E.; Rathinam, S.R.; Babu, M.; Kanakath, A.; Thundikandy, R.; Lee, S.M.; Browne, E.N.; Porco, T.C.; Acharya, N.R. Outcomes of Vogt-Koyanagi-Harada Disease: A Subanalysis From a Randomized Clinical Trial of Antimetabolite Therapies. Am. J. Ophthalmol. 2016, 168, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Fardeau, C.; Champion, E.; Massamba, N.; LeHoang, P. Uveitic macular edema. Eye Lond. Engl. 2016, 30, 1277–1292. [Google Scholar] [CrossRef]
- Vegas-Revenga, N.; Calvo-Río, V.; Mesquida, M.; Adán, A.; Hernández, M.V.; Beltrán, E.; Valls Pascual, E.; Díaz-Valle, D.; Díaz-Cordovés, G.; Hernandez-Garfella, M.; et al. Anti-IL6-Receptor Tocilizumab in Refractory and Noninfectious Uveitic Cystoid Macular Edema: Multicenter Study of 25 Patients. Am. J. Ophthalmol. 2019, 200, 85–94. [Google Scholar] [CrossRef]
- Deuter, C.M.E.; Zierhut, M.; Igney-Oertel, A.; Xenitidis, T.; Feidt, A.; Sobolewska, B.; Stuebiger, N.; Doycheva, D. Tocilizumab in Uveitic Macular Edema Refractory to Previous Immunomodulatory Treatment. Ocul. Immunol. Inflamm. 2017, 25, 215–220. [Google Scholar] [CrossRef]
- Heissigerová, J.; Callanan, D.; de Smet, M.D.; Srivastava, S.K.; Karkanová, M.; Garcia-Garcia, O.; Kadayifcilar, S.; Ozyazgan, Y.; Vitti, R.; Erickson, K.; et al. Efficacy and Safety of Sarilumab for the Treatment of Posterior Segment Noninfectious Uveitis (SARIL-NIU): The Phase 2 SATURN Study. Ophthalmology 2019, 126, 428–437. [Google Scholar] [CrossRef]
- Karkhur, S.; Hasanreisoglu, M.; Vigil, E.; Halim, M.S.; Hassan, M.; Plaza, C.; Nguyen, N.V.; Afridi, R.; Tran, A.T.; Do, D.V.; et al. Interleukin-6 inhibition in the management of non-infectious uveitis and beyond. J. Ophthalmic Inflamm. Infect. 2019, 9, 17. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total | No TTO IS/BT | With TTO IS/BT | p-Value | |
|---|---|---|---|---|
| n = 356 | n = 290 (81.5%) | n = 66 (18.5%) | ||
| Female | 180 (50.6) | 146 (50.3) | 34 (51.5) | 0.864 |
| Male | 176 (49.4) | 144 (49.7) | 32 (48.5) | |
| Age (median [Q1Q3]) | ||||
| At diagnosis | 42.8 [31.5, 54.0] | 42.0 [32.0, 55.0] | 38.0 [30.0, 47.0] | 0.027 |
| At the start of treatment | 42.5 [34.0, 50.0] | Not applicable | ||
| Time diagnosis–initiation TTO | 2 [1, 4] | Not applicable | ||
| n. outbreaks | ||||
| 1 outbreak | 157 (44.1) | 134 (46.2) | 23 (34.9) | 0.197 |
| 2 outbreak | 35 (9.8) | 30 (10.3) | 5 (7.6) | |
| ≥3 outbreak | 164 (45.9) | 126 (43.4) | 38 (57.6) | |
| Laterality | ||||
| Unilateral | 271 (76.1) | 236 (81.4) | 31 (47.0) | <0.001 |
| Bilateral | 85 (23.9) | 54 (18.6) | 35 (53.0) | |
| Anatomic Location | ||||
| Anterior | 265 (74.4) | 233 (80.3) | 32 (48.5) | <0.001 |
| Intermedia | 34 (9.6) | 22 (7.6) | 12 (18.2) | |
| Posterior | 28 (7.9) | 18 (6.2) | 10 (15.2) | |
| Panuveitis | 29 (8.2) | 17 (5.9) | 12 (18.2) | |
| Etiology | ||||
| Idiopathic | 154 (43.3) | 133 (45.9) | 21 (31.8) | Not applicable |
| AS HLA B27+ | 76 (21.4) | 58 (20.0) | 18 (27.3) | |
| Pars planitis | 19 (5.3) | 14 (4.8) | 5 (7.6) | |
| Associated with HLA B27 | 17 (4.8) | 16 (5.5) | 1 (1.5) | |
| IBD | 13 (3.7) | 10 (3.5) | 3 (4.6) | |
| AS HLA B27- | 12 (3.4) | 11 (3.8) | 1 (1.5) | |
| Behcet | 11 (3.1) | 5 (1.7) | 6 (9.1) | |
| Other white dot syndrome | 8 (2.3) | 7 (2.4) | 1 (1.52) | |
| Posner | 7 (2.0) | 7 (2.4) | 0 | |
| Sarcoidosis | 7 (2.0) | 7 (2.4) | 0 | |
| Psoriatic arthritis | 6 (1.7) | 4 (1.4) | 2 (3.0) | |
| Harada syndrome | 5 (1.4) | 3 (1.0) | 2 (3.0) | |
| Birdshot uveitis | 4 (1.1) | 0 | 4 (6.1) | |
| APPC | 4 (1.1) | 4 (1.4) | 0 | |
| For drugs | 4 (1.1) | 4 (1.4) | 0 | |
| Intermedia-associated MS | 3 (0.8) | 1 (0.3) | 2 (3.0) | |
| Associated Sjögren 1º | 2 (0.6) | 2 (0.7) | 0 | |
| Cogan’s syndrome | 1 (0.3) | 1 (0.3) | 0 | |
| Systemic lupus erythematosus | 1 (0.3) | 1 (0.3) | 0 | |
| TINU | 1 (0.3) | 1 (0.3) | 0 | |
| Undetermined | 1 (0.3) | 1 (0.3) | 0 | |
| Systemic CS treatment | 43 (12.1) | 19 (6.5) | 24 (36.4) | |
| Orals | 26 (7) | 14 (4.8) | 12 (18.2) | <0.001 |
| Intravenous | 17 (4.8) | 5 (1.7) | 12 (18.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteban-Ortega, M.; Steiner, M.; Andreu-Vázquez, C.; Thuissard-Vasallo, I.; Díaz-Rato, A.; Muñoz-Fernández, S. An Observational Study in the Real Clinical Practice of the Treatment of Noninfectious Uveitis. J. Clin. Med. 2024, 13, 1402. https://doi.org/10.3390/jcm13051402
Esteban-Ortega M, Steiner M, Andreu-Vázquez C, Thuissard-Vasallo I, Díaz-Rato A, Muñoz-Fernández S. An Observational Study in the Real Clinical Practice of the Treatment of Noninfectious Uveitis. Journal of Clinical Medicine. 2024; 13(5):1402. https://doi.org/10.3390/jcm13051402
Chicago/Turabian StyleEsteban-Ortega, Mar, Martina Steiner, Cristina Andreu-Vázquez, Israel Thuissard-Vasallo, Alvaro Díaz-Rato, and Santiago Muñoz-Fernández. 2024. "An Observational Study in the Real Clinical Practice of the Treatment of Noninfectious Uveitis" Journal of Clinical Medicine 13, no. 5: 1402. https://doi.org/10.3390/jcm13051402
APA StyleEsteban-Ortega, M., Steiner, M., Andreu-Vázquez, C., Thuissard-Vasallo, I., Díaz-Rato, A., & Muñoz-Fernández, S. (2024). An Observational Study in the Real Clinical Practice of the Treatment of Noninfectious Uveitis. Journal of Clinical Medicine, 13(5), 1402. https://doi.org/10.3390/jcm13051402